
Abstract
Keywords
Introduction
The prevalence of sick leave among pregnant employees is relatively high in the Nordic countries [1–5]. In Denmark, pregnancy-related sick leave has been estimated to constitute around 4000 full-time positions per year [2]. Sick leave in pregnancy may in some cases contribute to a healthy pregnancy for the mother and child, in other cases it may have a negative impact on women’s health and socio-economic status in general [6, 7]. Being on sick leave during pregnancy increases a woman’s risk of receiving disability pension up to 8 years after childbirth [8] and employers may hesitate to employ women of childbearing age [6]. European legislation protects pregnant women from harmful work-related exposures and ensures their right for workplace adjustments, if necessary.
Nausea, vomiting, and dizziness are the most common reasons for sick leave in early pregnancy, whereas Braxton Hicks contractions, lower back pain, and pelvic girdle pain are more common in late pregnancy [3, 4, 9]. In practice, the reasons for sick leave in pregnancy are often more complex. It has been suggested that sick leave may also be related to women’s work conditions and health status. In some cases, isolated pregnancy symptoms may be a proxy for underlying causes [3, 10].
Work-related risk factors for sick leave include psychosocial work factors (e.g. high job strain and low job control) and physical work factors (e.g. heavy lifting, night or shift work, standing work) [11–13], however, workplace adjustments have been found to reduce the number of days on sick leave among pregnant employees [14]. The number of days on sick leave is highest among pregnant employees in retail, hotels, healthcare, cleaning services, and social services, and lowest in public administration [2, 15]. A high number of days on sick leave in selected occupations may be due to demanding work conditions and lack of workplace adjustments.
Health and socio-demographic factors related to sick leave are maternal age and weight, educational level, activity level, multiparity, and use of reproductive therapy [1, 3, 10, 16, 17]. Self-rated health based on a single item was found to be a strong predictor of sick leave in employees in general [18, 19]. Whether it is a predictor for pregnant employees is unknown.
As sick leave among pregnant women is a complex contribution of work factors and health status and the timing of these factors, the aim of this study was to examine associations between and timing of psychosocial and physical work factors and health status on sick leave among Danish pregnant employees.
Material and methods
Design, setting and participants
A survey was conducted in the Central Denmark Region, which is the largest of five administrative units in Denmark with 1.3 million citizens and 15,000 annual births across six public birth facilities. Healthcare in Denmark is tax financed and includes antenatal visits, intra-natal care, and post- partum care. No other public or private birth facilities were available in the Central Denmark Region during the study period.
In Denmark, pregnant women in the labour market (either as a salary earner, self-employed or unemployed and as a member of an unemployment insurance fund) are entitled to claim maternity benefit during pregnancy and after childbirth. Maternity leave begins 4 and 8 weeks before the due date for women working in the private sector and public sector, respectively. In total, parents in Denmark may apply for 1 year of paid parental leave. Pregnant employees are protected against being dismissed from work during pregnancy and maternity leave. In cases of dismission, the employer needs to prove that the reason was not pregnancy-related.
All pregnant women in the Central Denmark Region were invited to participate in the present study between 1 February and 15 May, 2018 (N = 3329). The invitation included information about the study and a login to an internet-based baseline questionnaire. The questionnaire was attached to the booking information for the first antenatal visit, a fetal ultrasound scan at the hospital in gestational week 12.
This baseline questionnaire included information on socio-economic status, psychosocial and physical work factors, health status, days on sick leave during the last year, and days on sick leave during pregnancy. A similar follow-up questionnaire was distributed in gestational week 27 to women who were employed at baseline. Gestational week 27 was chosen for practical reasons.
Variables
The outcome was days on sick leave during pregnancy dichotomized into </⩾14 days. In both questionnaires, the women were asked to report the total number of days on full-time sick leave from the start of their pregnancy. If the number of days was higher at baseline compared with follow-up, the number of days at baseline was used.
Exposure variables were psychosocial and physical work factors as well as present health status. Psychosocial work factors were measured with dimensions from the short Copenhagen Psychosocial Questionnaire II (COPSOQ II)[20]. The variables were work pace, influence, social support from supervisors, recognition, quality of leadership, job satisfaction, and conflict in work–family balance. Each variable was dichotomized into high and low with the cut-off being the mean values of a representative sample of Danish employees [21].
In relation to physical work factors, the women were asked whether their work involved standing/walking, heavy lifting, shift work or night shift. The variables were dichotomized into high (always or often) and low (sometimes, seldom, or never).
Type of occupation was assessed based on a scale from The Danish Working Environment Authority [22] and categorized into high and low risk according to national reports regarding sick leave among pregnant women [2, 15]. High-risk occupations were retail, wholesale trade, hotels, restaurants, cleaning services, day-care centres, 24-h care centres and domiciliary care.
To measure health status, data on level of burnout and stress were obtained from COPSOQ II and dichotomized according to the mean values of a representative sample of Danish employees [21]. The Edinburgh Postnatal Depression Scale (EPDS)[23] was used to assess possibility of depression and categorized as <11 (depression not likely) and ⩾11 (fairly high possibility of depression)[24]. Work ability was measured by the single item from the Work Ability Index [25]: ‘Assume that your work ability at its best has a value of 10 points. How many points would you give your current work ability?’. The item was dichotomized as low (0–6) and high (7–10). General health was measured with the single item from COPSOQ II ‘In general, how would you rate your health?’ and was categorized as fair/poor, good, excellent/very good.
Statistical methods
Baseline characteristics of the total population and according to sick leave in pregnancy were described by frequencies or means and compared using the chi-square test, Fisher’s exact test or unpaired t-test.
The associations between psychosocial and physical work factors and health status measured at baseline and sick leave ⩾14 days were estimated using logistic regression. Adjusted analyses were controlled for maternal age, gestational weight gain, physical activity during pregnancy, children <18 years living at home, and educational level, all selected a priori and obtained from the baseline questionnaire.
To provide a measure for timing and duration of exposure during pregnancy, four categories were defined: (a) low/low (not exposed in any period); (b) high/low (exposed at baseline, but not at follow-up); (c) low/high (not exposed at baseline, but at follow-up); (d) high/high (exposed in both periods). Logistic regression was used to estimate associations between these categories and sick leave (</⩾14 days) with the ‘low/low’ group used as reference.
All estimates were presented as odds ratios (ORs) with 95% confidence intervals (CIs). All reported p-values were two-sided, and the level of statistical significance was 0.05. Statistical analysis was performed using Stata, version 15.
Ethical considerations
The study was approved by The Danish Data Protection Agency (j.nr. 1-16-02-29-18). No other approval was necessary according to Danish law as the data for the study were obtained from questionnaires.
Results
The baseline questionnaire was completed by 1491 pregnant women (44.8%). A total of 1046 were employed and eligible for inclusion. However, 136 of these women did not respond to the follow-up questionnaire, resulting in a final study population of 910 women (Figure 1). Women who did not respond to the follow-up questionnaire were similar to the study population according to exposures and days on sick leave, but significantly fewer women employed in high-risk occupations completed the questionnaire.
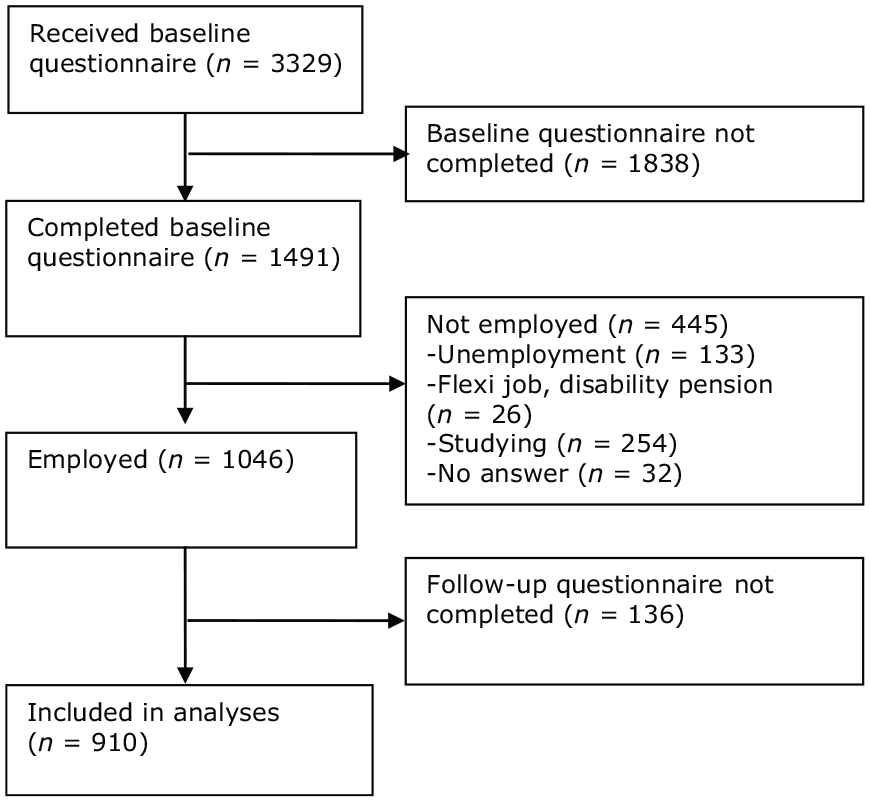
Flow chart of the study population.
A total of 133 (14.6%) women reported sick leave for ⩾14 days. These women were older, had a lower educational level, and had children living at home more often than women with sick leave below 14 days (Table I).
Baseline characteristics of the study population.
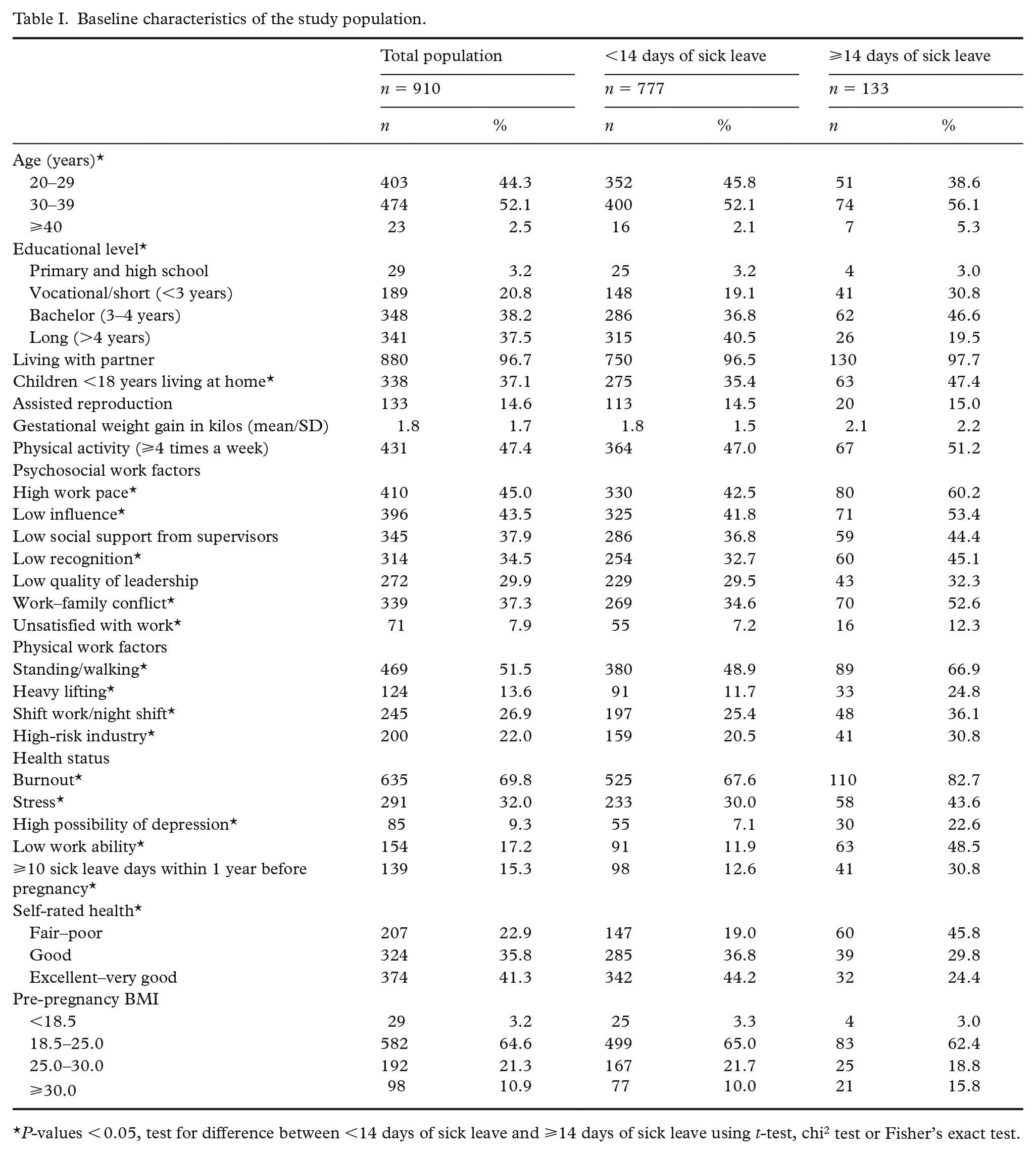
P-values < 0.05, test for difference between <14 days of sick leave and ⩾14 days of sick leave using t-test, chi2 test or Fisher’s exact test.
At baseline, a high number of women were exposed to psychosocial work-related risk factors and poor mental health compared with physical work-related risk factors (Table I). In particular, burnout, high work pace, and low influence were experienced by more than 40% of the women.
The mean duration of sick leave was 9.1 days (SD 25.0) at 27 weeks of gestation. A total of 616 women (67.7%) reported no days of sick leave during the study period.
A total of 407 (81%) of the women reported being familiar with the pregnancy policy at their workplace, and 147 (28%) had completed a workplace risk assessment. None of these factors were associated with sick leave (p = 0.58 and 0.12, respectively). Moreover, 658 (73%) had consulted either their general practitioner or a midwife regarding their work environment, and this was more common among women with more than 14 days of sick leave (p < 0.001).
Psychosocial work factors generally had a considerable impact on sick leave ⩾14 days (Table II). Specifically, high work pace, low influence, low recognition, conflict in work–family balance, and being unsatisfied with one’s work increased sick leave significantly. Adjustment for potential confounders changed the estimates only marginally. Of the physical work factors, standing/walking, heavy lifting, and shift work/night shift had an impact on sick leave. Regarding health status, burnout, stress, possibility of depression, low work ability, previous sick leave, and fair/poor self-rated health were risk factors for sick leave (Table II).
Crude and adjusted odds ratios (ORs) for associations between work factors and health status at baseline and sick leave ⩾14 days among pregnant women (n = 910).
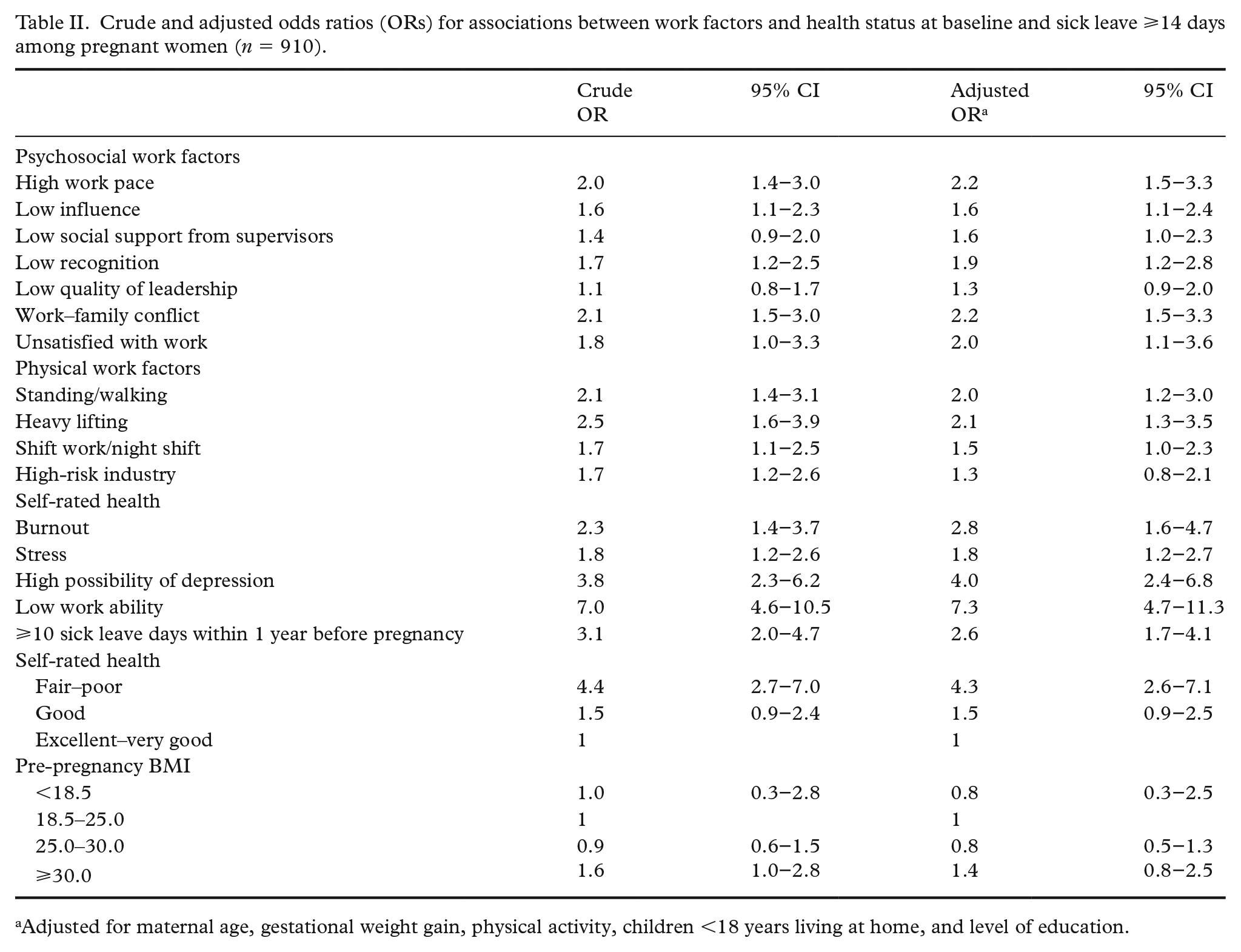
Adjusted for maternal age, gestational weight gain, physical activity, children <18 years living at home, and level of education.
Women exposed to psychosocial or physical work-related risk factors during the first 27 weeks of pregnancy or only at follow-up had a higher risk of sick leave ⩾14 days compared with women not exposed at any time during pregnancy (Table III). The risk for women only exposed at baseline was not elevated compared with women not exposed at any time. Poor health status was also a risk factor when the women were exposed in the first 27 weeks of pregnancy. Furthermore, women with a high possibility of depression at baseline were at higher risk of sick leave regardless of the duration of the exposure. Women reporting low work ability had a high risk of sick leave regardless of the period of the exposure, but women exposed in the first 27 weeks of pregnancy were especially at risk.
Crude and adjusted odds ratios (ORs) for associations between work factors and health status measured in gestational week 12 and 27, and sick leave ⩾14 days among pregnant women (n = 910).
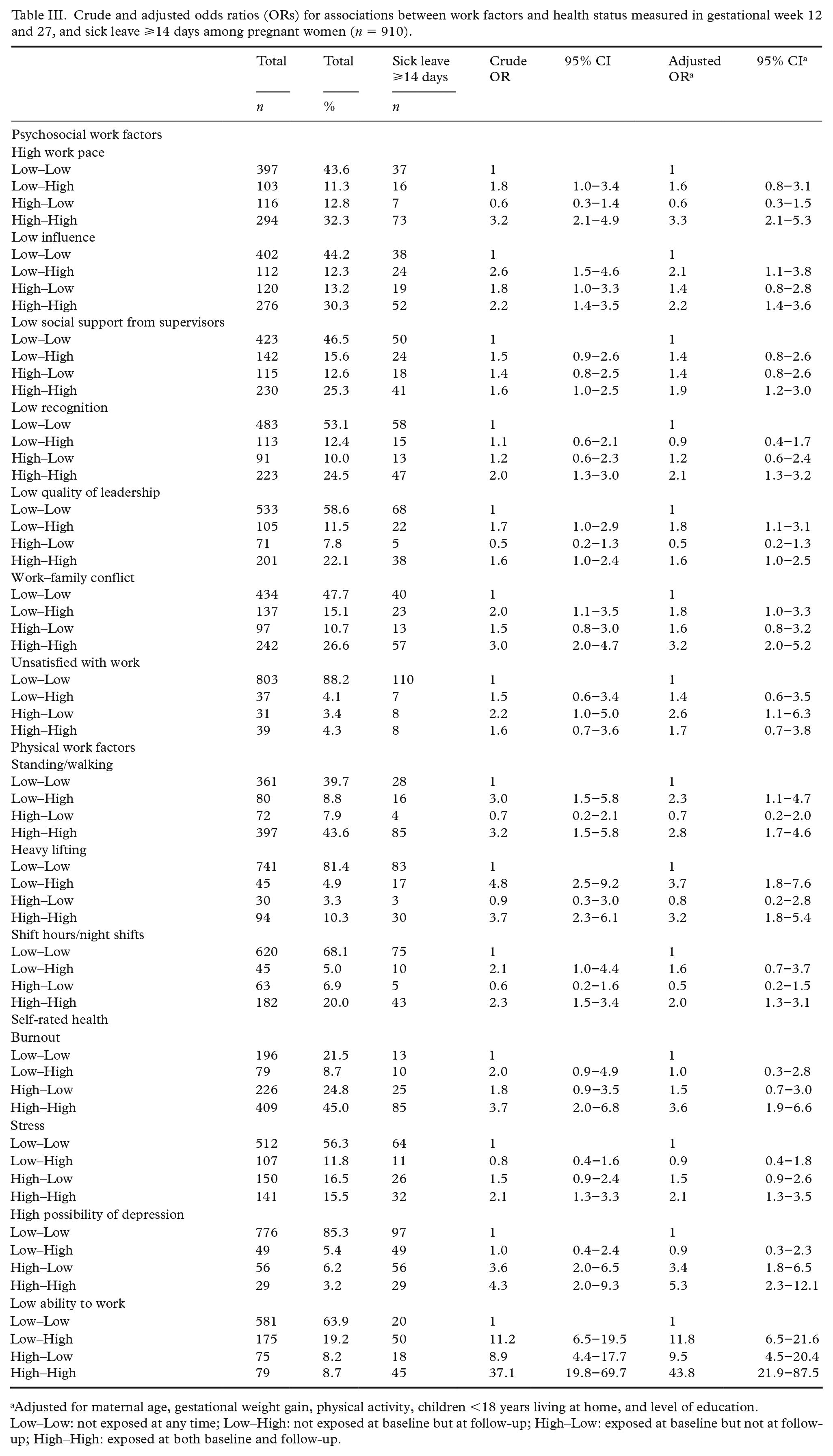
Adjusted for maternal age, gestational weight gain, physical activity, children <18 years living at home, and level of education.
Low–Low: not exposed at any time; Low–High: not exposed at baseline but at follow-up; High–Low: exposed at baseline but not at follow-up; High–High: exposed at both baseline and follow-up.
A total of 483 (53.8%) women reported a need for workplace adjustments at either baseline or follow-up, and 363 (75%) of these were offered adjustments (Table IV). Compared with women who did not report a need for adjustments, both women who needed and received adjustments and women who needed but did not receive any adjustments had a higher risk of sick leave.
Crude and adjusted odds ratios (ORs) for associations between need and receipt of workplace adjustments and sick leave ⩾14 days.
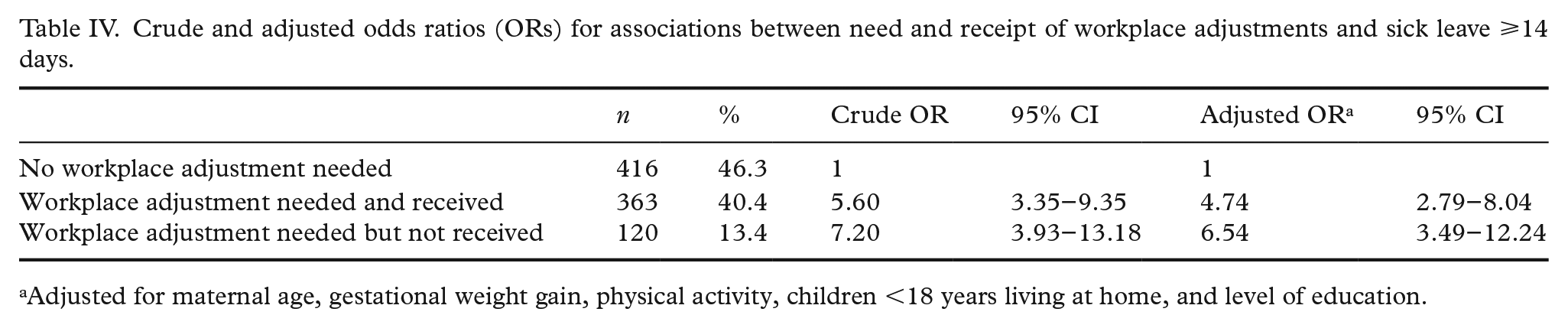
Adjusted for maternal age, gestational weight gain, physical activity, children <18 years living at home, and level of education.
Discussion
In this study of Danish pregnant women, a total of 14.6% had been on sick leave for more than 14 days at 27 weeks of gestation. Being exposed to psychosocial and physical work-related risk factors as well as reporting poor health status at baseline was associated with more sick leave days. Generally, women exposed to these risk factors during the first 27 weeks of pregnancy or only at follow-up had a higher risk of sick leave compared with those not exposed at any time or only exposed at baseline.
Physical work factors have also previously been identified as risk factors for sick leave in pregnant women [11–13]. Thus, heavy lifting, standing, walking and shift work seem to play a significant role [11, 12]. Women employed in high-risk occupations were at higher risk of sick leave, which was also found in two Danish reports based on register data [2, 15]. However, after adjusting for potential confounders, type of occupation no longer had an impact on sick leave in the present study. This may be due to methodological issues such as a generally low response rate, in particular among women from high-risk occupations, as well as a population of highly educated women. On the other hand, lack of association between occupation and sick leave may also indicate that it may be more important to look at the psychosocial and physical work environment, not only at the specific type of occupation.
In general, more women reported being exposed to risk factors related to the psychosocial work environment than to the physical work environment. Findings are in accord with previous studies showing psychosocial work factors as predictors of sick leave [12, 13]. Conflict in work–family balance was also confirmed as a risk factor for sick leave [26]. In general, women take on ‘double shifts’, as they work first a shift in paid work and then a second shift in the household [1]. The obligations of pregnant women may partly explain the high prevalence of women experiencing burnout and stress. Other explanations may be the timing of the baseline questionnaire, as nausea, vomiting and fatigue are common symptoms in gestational week 12 and are found to have a negative influence on mental health [27]. High scores in burnout and stress were associated with sick leave ⩾14 days, and the same applied to the possibility of depression. Mental disorders such as depression and anxiety have also been identified as strong risk factors for sick leave in other studies [3, 4], thus, early attention to depressive symptoms may be important in reducing sick leave. Fair or poor self-rated health was found to be associated with sick leave ⩾14 days, which is similar to findings in the general population [18, 19]. The single measure of self-reported health may be a good predictor for sick leave among pregnant women and easy to use in clinical practice. The analysis accounting for timing and duration of exposures found that women who were exposed to risk factors in the first 27 weeks of pregnancy or only at follow-up had the highest risk of sick leave. This could be seen as a lack of workplace adjustments for those in most need and may indicate a need for greater awareness of adjustment in early pregnancy.
At either baseline or follow-up, half of the women reported a need for adjustments at the workplace, and three out of four of these women were offered these adjustments. Women who did not have any workplace adjustments had a tendency toward a higher risk of sick leave compared with those who were offered adjustments. This is in line with a Norwegian study that found workplace adjustments to be beneficial, especially for employees working shifts, evenings or nights, as the risk of absence exceeding 14 days decreased by nearly 11% [14].
A review of the existence of interventions in the healthcare sector and workplaces targeting sick leave among pregnant women found no interventions tested in workplaces [28]. These results imply the importance of testing accommodations in the workplace, for example, to reduce the degree of pregnant employees working nights and shift work, reduce heavy lifting, and providing sitting or changing work postures. Moreover, having influence on own job tasks including flexible breaks during the workday may reduce the level of sick leave. Pregnant women may also benefit from a consultation at the workplace by a physiotherapist or a midwife to talk about adjustments, exercise and mental health. Less than one-third of the participants in this study had completed the obligatory workplace risk assessment, which indicates a need to focus more on prevention in the workplace. Proactive recommendations regarding work conditions and adjustments as part of the prenatal care visits may contribute to early prediction of the need for workplace adjustment during pregnancy [4].
In the Nordic countries, the legislation states that employers’ wage costs are reimbursed when pregnant women are on sick leave. That may motivate the employer not to make adjustments, as it could be economically advantageous to replace a pregnant woman with a person fit for work, ultimately resulting in more sick leave [3, 6]. Testing workplace accommodations is therefore important to identify the effects for both the pregnant women and their employers.
Sick leave in pregnancy is not avoidable. However, for some, a reduction in the number of days on sick leave may be possible and still be reassuring for the pregnant woman. Pregnant women may in some situations continue their work and challenge their own health or the course of the pregnancy, because they are afraid of being negatively labeled by employers and colleagues [7]. However, three out of four pregnant women on sick leave evaluate their health as good or excellent, which may indicate that sick leave is not only related to medical issues [29]. The general work environment is not found to be a risk factor for pregnant women and their foetus in regard to miscarriage or low birth-weight, however, the risk is moderately elevated for high levels of exposure (e.g. ⩾2 night shift/week, >40 hours/week, lifting >100 kg/day, standing >6 h/day) [30–33]. If adjustments are not possible pregnant women are advised to be absent until adjustments are possible [34].
Strengths and limitations of the study
All pregnant women in the Central Denmark Region were invited to participate, and eligible women who only completed the baseline questionnaire, were similar to those who completed both questionnaires and participated in the study, except that few women employed in high-risk occupations participated.
Although no information on non-responders was available, some selection toward a higher educational level is likely, as more than one-third had a higher level of education (>4 years). Thus, the association between work factors and sick leave may be underestimated as women at lower educational levels have higher numbers of sick days [35], are more exposed to physical work-related risk factors, and have low influence at work [36].
Sick leave was measured using self-reported information, which has been found to be underestimated compared with register data in pregnant women [35]. Therefore, the actual frequency of sick leave may be higher than reported in this study.
In the analysis of timing and duration, exposures at gestational week 27 were measured at the same time as the outcome. This could have introduced bias if women with more sick leave tend to, for example, rate the quality of management at the workplace more poorly. If this is the case the impact of the measured risk factors on sick leave might have been overestimated at gestational week 27.
Validated scales were used to measure the psychosocial work factors, work ability, and possibility of depression. Some of the exposure groups consisted of low numbers of women resulting in uncertain estimates with wide CIs. These associations should be tested in a larger sample.
Conclusion
The study supports previous findings on associations between psychosocial and physical work-related risk factors, poor health status and sick leave among pregnant employees. Moreover, this study found the single response of self-reported health to be a strong predictor of sick leave in this population. Furthermore, pregnant women being exposed to work-related risk factors during the first 27 weeks of pregnancy or in late pregnancy had a higher risk of sick leave, which may indicate a lack of workplace adjustments. Early identification and individual adjustments of the workplace may increase welfare and retention among pregnant employees.
Footnotes
Author contributions
PP, AMM, DRA, CVN, EAN and RDM conceived and planned the study. PP wrote the first draft of the manuscript and completed the analyses. AMM, DRA and RDM significantly contributed to the interpretation of the data and writing of the paper. All authors provided critical feedback and accepted the final version of the manuscript.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by The Danish Working Environment Research Fund and Central Denmark Region.
Data accessibility statement
Research materials related to this study can be accessed by contacting Pernille Pedersen.