
Abstract
Aim: The aim of the study is to encourage further research initiatives and collaborations based on Norwegian Armed Forces Health Registry (NAFHR) data by presenting basic information on the data contained therein. Methods: We describe how conscription board health examinations (CBHEs) are carried out, how results are recorded in the NAFHR, and the completeness of NAFHR data that are electronically available for research purposes. Results: In December 2018, the NAFHR contained data on nearly 1.5 million Norwegian citizens (95% men) who attended CBHE in 1968–2018 at the age of 17–19 years. The percentage of persons included from each birth cohort has varied as the Armed Forces’ personnel requirements and filing procedures have changed, increasing from 73% of eligible men born in 1950 to 95% of eligible men born in 1960–1991. In 2010 a preselection of candidates was implemented wherefore less than half of men born in 1992–2000 are registered in the NAFHR. Information on aerobic fitness, cognitive general ability, height and weight is registered for approximately 95% of individuals included in the NAFHR. The NAFHR contains more detailed health information for CBHEs that took place as from 1980, and information included from 2011 onwards is the most detailed. Unique, national personal identification numbers may be used to link the NAFHR to other health registries or data sources for public health research.
Keywords
Background
In Norway, all male citizens can be called upon to serve in the military; in recent years, this has changed to include women as well. Before serving, individuals must attend a conscription board health examination (CBHE) to determine their fitness for duty. The CBHE consists of tests of physical and mental health, including aerobic fitness, cognitive ability, clinical examinations and vision and hearing tests. Test results are stored in the Norwegian Armed Forces Health Registry (NAFHR), which is one of Norway’s national health registries.
Because it is a citizen’s duty to give their health information to the Armed Forces prior to military service, the NAFHR is not affected by self-selection. Therefore, the NAFHR contains physician-assessed health information from an unselected population of men spanning several decades. The NAFHR has been used as a stand-alone source for studies on national trends in aerobic fitness, cognitive ability and body mass index [1-4]. However, because every person in the NAFHR is tagged by their unique, 11-digit personal identification number, data can also be linked to other national registries and data sources on health and social welfare. NAFHR data can be used in large-sample epidemiological studies that consider a range of long-term health outcomes, such as heart conditions, dementia, or mental health problems. By pooling NAFHR data with similar data from Sweden and Denmark, even larger Nordic cohorts can be constructed [5].
NAFHR data have already been used in studies on cause-specific mortality [6,7] and disability [8,9]. Moreover, in about 20 studies, the NAFHR has provided novel insight into how factors in birth, neonatal life and family may affect the adult body and cognitive ability through individual-level linkage to the Medical Birth Registry combined with mapping of family relations [10-20]. Linkage to data from national screening programmes has contributed to explanatory models on the association between health in adolescence and adverse health outcomes in adulthood, that is, cardiovascular disorders, multiple sclerosis, alcohol consumption and obesity [7,21-23].
This article aims to encourage further research initiatives and collaborations based on NAFHR data by presenting basic information on the data.
Legislation
The NAFHR is authorised by the Health Registry Act and specific regulations; the Ministry of Defence and the Norwegian Armed Forces Joint Medical Services are responsible for its implementation and maintenance. The purpose of the NAFHR is to monitor the health of Armed Forces personnel and to identify risk factors associated with military service. The NAFHR may collaborate with research groups whenever the data analysis falls within the purposes of the registry, and the processing of data is in accordance with ethical guidelines for medical research [24,25].
Norwegian conscription law
Eligible Norwegian citizens are included in the Armed Forces’ personnel register when they reach the age of 17 years. Only those with a permanent disability that occurred before the age of 17 years are exempt from inclusion in the personnel register. Until 2009, practically all male candidates had to attend a CBHE to determine their fitness for service and were mandated to serve if selected. Women have had the opportunity to serve in the Armed Forces since 1985, although their service was voluntary. In 2007, women started receiving an invitation to attend a CBHE on a voluntarily basis. In 2010, the law and the procedure changed: every man and woman born after 1 January 1992 was obligated to submit a personal statement of skills and health to the Norwegian conscription board upon turning 17 years of age and, based on this statement, a portion of these candidates was mandated by law to attend a CBHE. However, women could choose not to serve, even if they were deemed fit and selected to do so. This changed in 2016, after which all men and women born after 1 January 1997 had to submit a personal statement of skills and health, attend at CBHE if requested, and serve in the military if selected. Since 2010, about 20,000 people attend the CBHE each year, depending on the Armed Forces’ staff requirements. While the candidates are generally examined when they are between the ages of 17 and 19 years, CBHEs can be postponed until 28 years of age upon request [25].
Procedures for conscription board health examinations
The purpose of CBHEs is to reveal and verify any physical or mental impairment that might influence the candidate’s ability to learn and perform military routines and operations. In the following, we describe the procedures for assessing the candidate’s physical and mental fitness. Some individuals may not be subjected to all these assessments if it becomes clear early in the process that he/she is not suitable for military service. However, since 2010, it has been emphasised that a full physical and mental examination should be conducted for every candidate.
Aerobic fitness and isometric muscle strength
The CBHE includes tests of aerobic fitness and, in some periods, isometric muscle strength. The methods for evaluating aerobic fitness have varied over the years. In 1968–1985, an indirect measure of maximal oxygen uptake was recorded by means of the Åstrand–Rhyming bicycle ergometer test. The test was scored according to a ‘stanine’ scale, that is, single-digit scores with values 1–9 (best), with each interval representing a given interval of maximal oxygen uptake [3]. In 1988–1993, aerobic fitness was tested by means of a treadmill. The stanine score was calculated based on lactic acid concentration in the blood (mmol/l) after a 10-minute submaximal uphill walk (12°, 80 m/min) [26]. However, only a minority of candidates were tested this way, because the treadmills were too heavy to transport between the ambulant conscription board locations. In 1994–2010, the conscription board did not conduct practical tests of aerobic fitness. Instead, a qualitative evaluation was made based on the candidate’s athletic background, using a three-category scale (A=high, B=medium, C=low). In 2011, practical tests of aerobic fitness were reintroduced. The tests were developed in a collaboration between the Norwegian School of Sports Science and the Armed Forces. The test is carried out on a treadmill; walking and running with increasing speed (4–20 km/h). The score 0–9 (best) is based on the number of minutes spent on the treadmill before yielding to exhaustion [27]. Isometric muscle strength tests (chest and leg press) were introduced in 2011/2012. Since 2017, muscle strength has been tested using pull-ups, standing long jump, and medicine ball shock throw.
Cognitive ‘general ability’
Cognitive ability, also referred to as ‘general ability’ (GA) in the CBHE, is assessed by three different, time-limited subtests: Arithmetic (25 min), Word Similarities (8 min), and Figures (20 min). The Arithmetic test is a measurement of arithmetic, algebraic, and logical reasoning ability, while the Word Similarities test is a synonym test. The Figures test is a non-verbal test of analytic intelligence. All tests were constructed to provide a linear increase in difficulty. The Arithmetic and Word Similarities tests are quite similar to those in Wechsler Adult Intelligence Scale (WAIS), and the Figures test was constructed to be very similar to the Raven’s Progressive Matrices. The tests have remained unchanged since 1954, but the Arithmetic test was changed from open-ended answers to multiple-choice with five alternatives in the mid-1990s. The scores from each of these three test are standardised into normally distributed F-scores (mean=50, standard deviation, SD=20) and summed to yield a combined measure of GA, which is reported as a stanine score. A stanine score of 5 represents an IQ score of 100 (WAIS), with an increment/decrement of 7.5 IQ units for each stanine unit deviating from 5. In 1963 and 1980, the test was calibrated to adjust for a substantial gain in GA [4]. In 1980, the mean score was lowered from around 6 to fit with a normal distribution with mean of 5.0 and standard deviation of 2. Some individuals perform poorly on the tests due to dyslexia or poor language skills. In such cases, the assessment is based on the candidate’s result on the Figures test and scored using a three-category scale (above average, average, or below average).
Clinical examination
The clinical examination in the CBHE consists of a physical health component and a mental health component. The physical health component consists of an interview, review of the candidate’s personal statements of health and any medical documentation of disease; a general clinical examination including anthropometric measurements, blood pressure, and an interview; a visual acuity test; a test of colour vision; and audiometry. Clinical examinations are conducted by medical doctors who are trained in military selection, in accordance with detailed written procedures published by the Norwegian Armed Forces Joint Medical Services [28]. During the clinical examination, the candidate is bare-footed, wearing only underwear. Anthropometric measurements are limited to height and weight, which are recorded to the nearest cm/kg. The candidate’s skin, posture and muscles are inspected, and the heart and lungs are auscultated. Blood pressure is measured at the right upper arm using an appropriately sized cuff after 5 minutes of seated rest. The candidate is screened for scoliosis, kyphosis, anisomelia, etc., by visual inspection aided by the Adam’s forward bend test. Feet are examined by palpation of the medial arch to exclude pes planus. Vision is assessed by monocular acuity with and without correction for refractive error. Visual acuity is assessed at a distance of 4 metres using an ETDRS (LogMAR) chart with two different small-scale tests for independent testing of the left and right eye. Until 2010, visual acuity was tested using a Snellen chart. Colour vision is assessed by Ishihara’s test. Hearing is assessed in a sound-insulated audiometry cabinet using an annually calibrated audiometer. Audiometry testing is carried out by personnel who have completed a training course. Initially, candidates are screened by testing each ear at 20 dB at the standard test frequencies 250, 500, 1000, 2000, 3000, 4000, 6000 and 8000 Hz. If the candidate is unable to hear all frequencies at 20 dB, a full threshold audiometry is carried out.
In the absence of specific indicators, assessment of mental health and social function is based on the interview and on an evaluation of the candidate’s behaviour and reactions during the clinical examination. However, further interviews and tests are carried out if suggested by the candidate’s personal statement of skills and health or symptoms revealed during the clinical examination.
If physical or mental symptoms or conditions are present, a result of ‘functional impairment’ is recorded for one or more of 10 specific body organs/systems as defined by the Armed Forces Joint Medical Services. The medical conditions that cause functional impairment are documented using the Norwegian version of the International Statistical Classification of Diseases and Related Health Problems. Military doctors have coded medical conditions in accordance with international coding systems since the beginning of the 1970s. Prior to this, a specific list of codes developed by the Armed Forces was used.
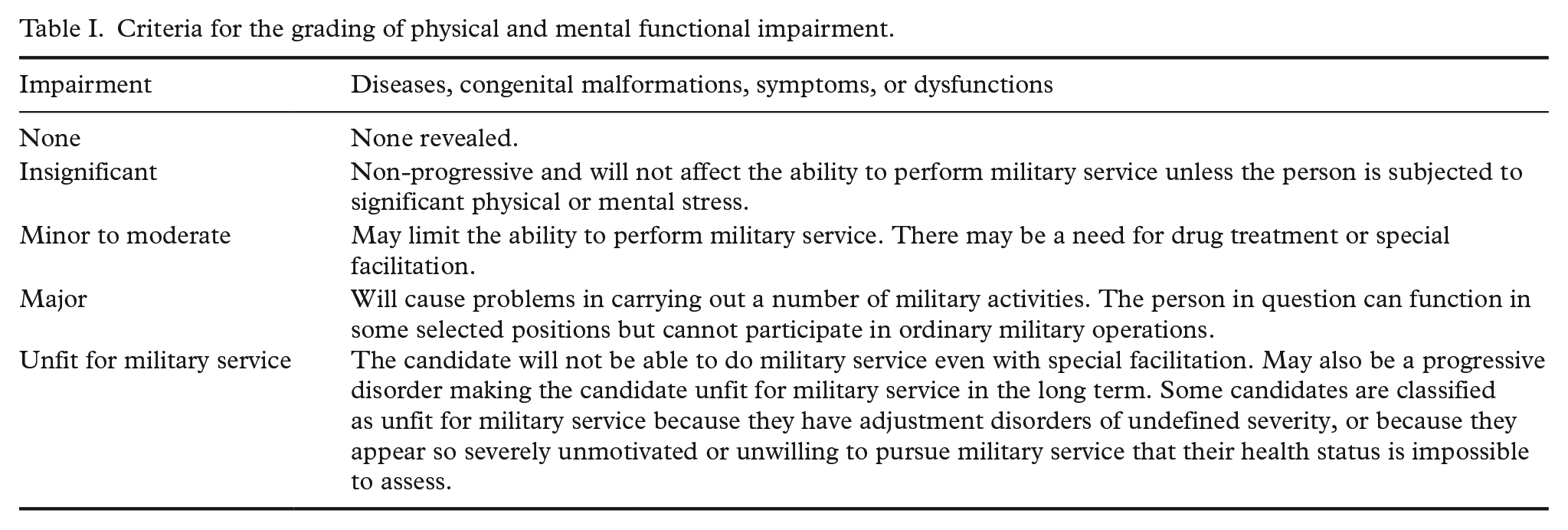
Since 1980, the severity of physical and mental functional impairment has been assessed according to specific criteria ranging from ‘insignificant’ to ‘unfit for military service’ (see Table I and previous publication by Fadum et al., 2017 [6]).
Criteria for the grading of physical and mental functional impairment.
Available data
In early 2019, we retrieved information for all candidates who attended a CBHE on or before 31 December 2018. Few persons born before 1950 are included in the NAFHR, and they are probably highly selected. Therefore, the statistics we present here are limited to candidates born after 1 January 1950.
In assessing the completeness of NAFHR data, we included only individuals who were evaluated at age 17–19 years. Those who attended CBHEs before age 17 (0.8%) or after age 19 years (5.2%) may have been evaluated by non-standard procedures, either because they voluntarily applied for a particular branch of the military or because they were unable to participate in a full CBHE. Among candidates evaluated at age 17–19 years, 22,058 were not assessed in person; instead they were evaluated based on medical documentation from civilian doctors or social services. Date of evaluation is normally registered in the NAFHR as the day the CBHE was conducted, or occasionally as a date a few days later. Prior to 1980, the CBHE dates were designated by year only, thus the correct age at CBHE may deviate from the registered age by up to 1 year (Supplemental Table II).
Completeness of Norwegian Armed Forces Health Registry data
By 31 December 2018, the NAFHR contained CBHE information on 1,346,165 candidates who had been assessed at age 17–19 years, 95% of whom were men, and nearly 75,000 of whom were women. With respect to the male birth cohorts from 1950 to 1960, health records were missing for approximately 10–25% of the annual birth cohorts. While 95% of Norwegian men born between 1960 and 1991 have CBHE information in the NAFHR, this is true of only half the men born since 1992 (Supplemental Table I and Figure 1).
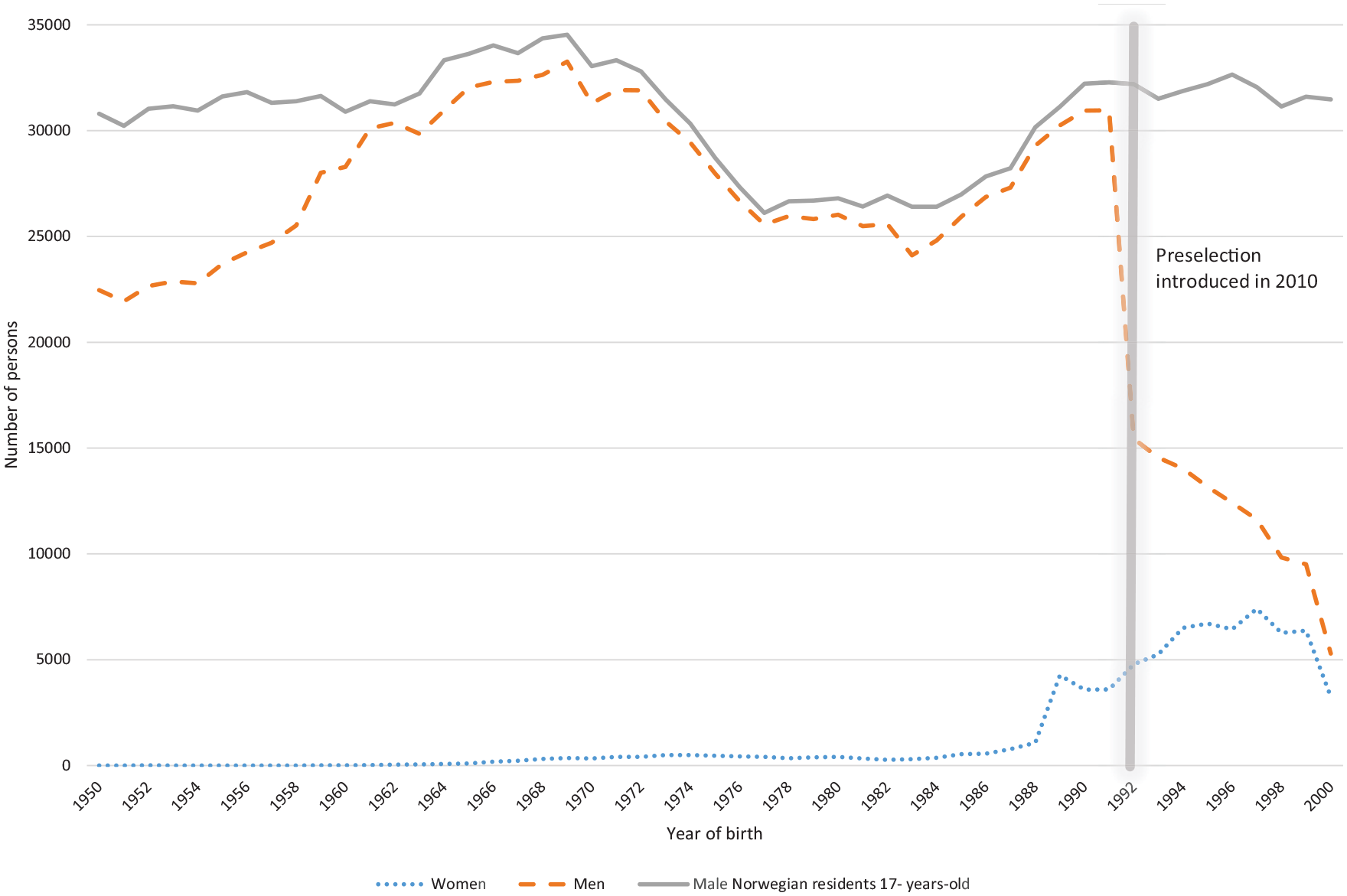
The Norwegian Armed Forces Health Registry – among men and women born in 1950–2000, the number from each birth cohort with conscription board health examination records at age 17–19 years (n=1,346,165) compared with the number of males who were Norwegian citizens and residents at age 17.
Aerobic fitness and isometric muscle strength
Measures for aerobic fitness are registered for nearly 95% of the men and almost 90% of the women who had a CBHE recorded between 1968 and 2018 (Table II and Figure 2). Scores for isometric muscle strength are available from 2011 to 2018, and are recorded for 80% of candidates examined in this period.
The Norwegian Armed Forces Health Registry – completeness of data for the different variables from men and women born in 1950–2000 who attended the conscription board health examination at age 17–19 years, in total 1,346,165 persons.
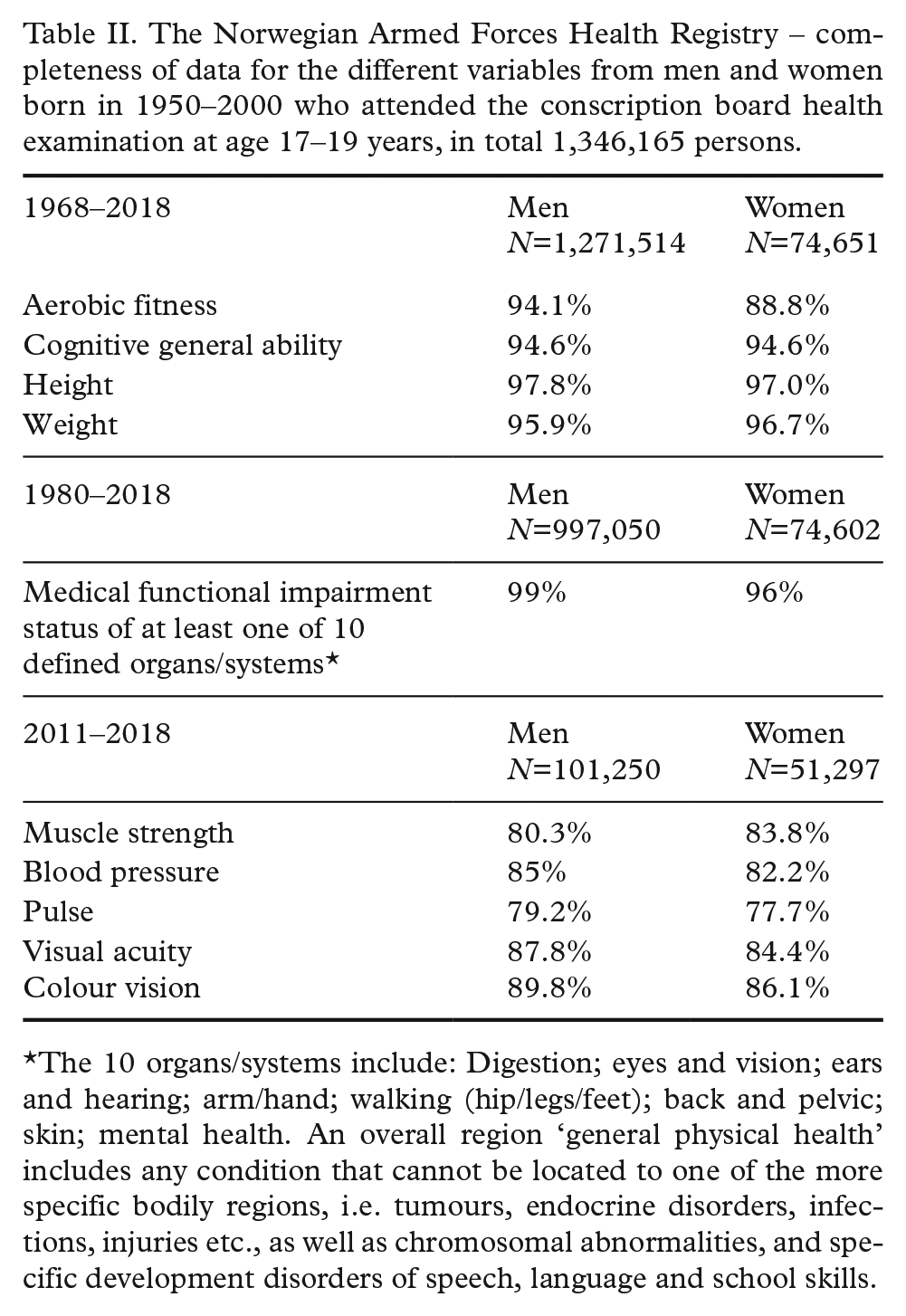
The 10 organs/systems include: Digestion; eyes and vision; ears and hearing; arm/hand; walking (hip/legs/feet); back and pelvic; skin; mental health. An overall region ‘general physical health’ includes any condition that cannot be located to one of the more specific bodily regions, i.e. tumours, endocrine disorders, infections, injuries etc., as well as chromosomal abnormalities, and specific development disorders of speech, language and school skills.
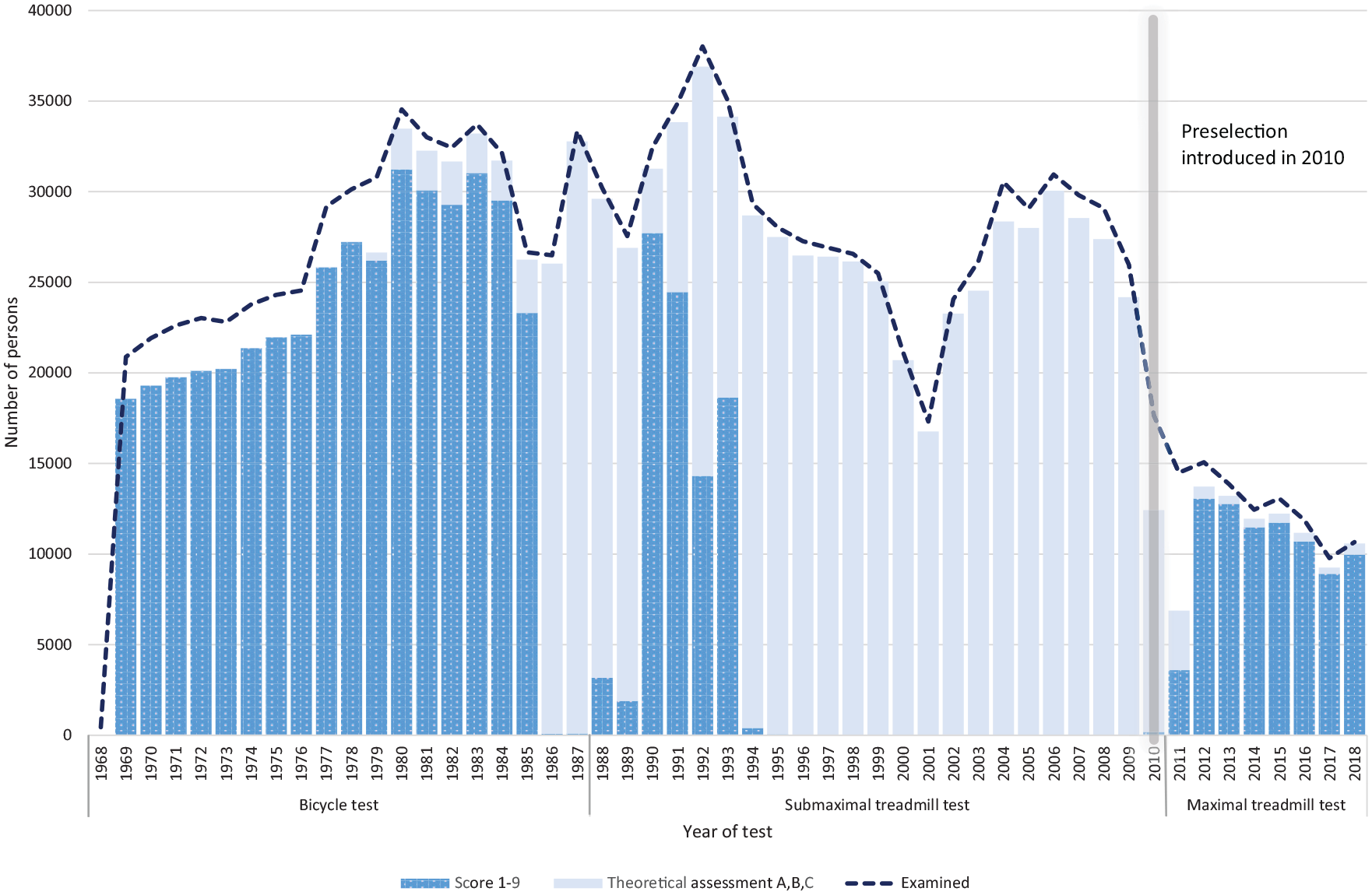
The Norwegian Armed Forces Health Registry – among men born in 1950–2000, the number tested for aerobic fitness at age 17–19 years, presented by year of examination (n=1,196,770).
Cognitive general ability
GA data are available for 95% of the men and women (Table II and Figure 3).
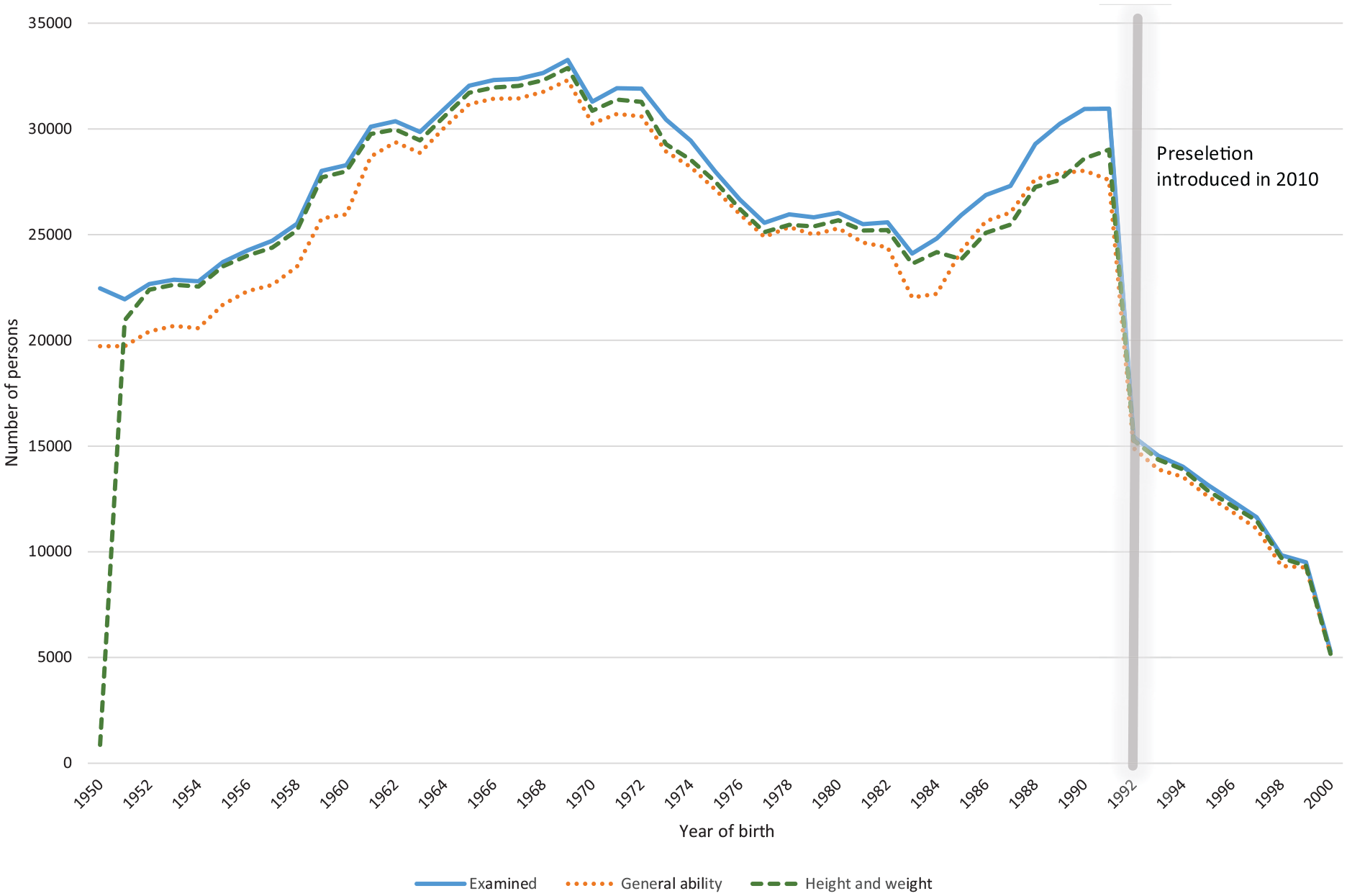
The Norwegian Armed Forces Health Registry – among men born in 1950–2000, the number from each birth cohort examined at age 17–19 years and registered with both height and weight (n=1,271,514) or with a cognitive general ability score (n=1,202,486).
Height and weight
Height and weight are registered for 96–97% of the candidates (Table II and Figure 3). For men, recorded height ranges from 100 to 215 cm with a mean of 179.7 cm (SD=6.6), while weight ranges from 30 to 195 kg with a mean of 72.2 kg (SD=11.8). In women, recorded height ranges from 100 to 200 cm with a mean of 167.4 cm (SD=6.3). Weight in women ranged from 30 to 176 kg with a mean of 64.2 kg (SD=10.2).
Medical assessments
Records of functional impairment status are available in almost all men and women who attended a CBHE in 1980 or later. Electronic medical records were introduced in the Armed Forces in 2004. The proportion of functional impairment records that are accompanied by an ICD diagnosis in the NAFHR has gradually increased since 2004, and coverage is considered complete as from 2010.
The first measurements of blood pressure and pulse were recorded in 2004. The percentage of candidates for whom blood pressure was recorded was 10% in 2008, gradually increasing to 80% of candidates examined in person in 2011–2018. Detailed information on visual acuity also increased gradually in this period (Table II).
Discussion
The NAFHR contains information on CBHE for about 1.5 million people born after 1950. Ninety-five percent of the men born in Norway from 1960 to 1991 have some CBHE information registered in the NAFHR, and missing on each of the variables is small (between 2 and 6%). Research can choose to include nearly complete birth cohorts, or focus on selected groups using prospective and retrospective cohort designs as previously discussed.
CBHE information is unavailable for about 10–25% of men born in 1950–1959. Still, the majority of men born in this period are registered in the NAFHR with personal identification number and can be linked to other registries or data sources.
Since 2010, only a subset of conscription candidates has been called to attend CBHE, thus NAFHR records for birth cohorts later than 1992 are not representative of the general population. On the other hand, due to the recent introduction of gender-neutral mandatory military service – unique in western countries – the number of females represented in the NAFHR is increasing steadily. Further, more detailed health information is available for individuals that have been assessed since 2010, and the validity of the data is improving as the Armed Forces produce more detailed protocols, more training, and more supervision of military doctors. This process of ‘tightening’ the medical selection in order to hand-pick the most fit individuals began as early as the year 2000 [29].
CBHEs have always been conducted by medical doctors and military officers trained in standardised procedures. However, it is important to bear in mind that the purpose of CBHEs has always been rooted in the Armed Forces’ need of soldiers. The assessments of the candidates’ physical and mental state are likely to vary somewhat between doctors, between conscription board districts, and over time, depending on the doctors’ clinical experience, military policies, and the candidates’ motivation to enter military service. Although the testing methods and procedures have always been chosen centrally by the Norwegian Armed Forces, little documentation is available with regard to calibration protocols, the reliability of testing equipment and the accuracy of test results. The NAFHR does not have full access to the Armed Forces databases, and cannot guarantee that every man included in the Armed Forces personnel register appears in the NAFHR.
This article focuses on CBHE information that is electronically available in the NAFHR as of 2018. Additional health-related information collected in the course of military service is available electronically, but it was impossible to provide a thorough description of these data within the framework of this article. Further data – stored on paper and in scanned documents – can be retrieved manually.
Supplemental Material
SJP920412_Supplemental_Tables – Supplemental material for The Norwegian Armed Forces Health Registry conscription board health examinations 1968–2018
Supplemental material, SJP920412_Supplemental_Tables for The Norwegian Armed Forces Health Registry conscription board health examinations 1968–2018 by Elin A. Fadum, Leif AA. Strand, Inger Rudvin, Mari L. Hæreid and Einar K. Borud in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We wish to acknowledge the following persons who critically read the manuscript: MD Kjetil Høye, The Armed Forces Personnel and Conscription Centre; MD Prof. Arne J. Norheim, The Norwegian Armed Forces Joint Medical Services; PhD Anders Aandstad, Norwegian Defence University College; and MD PhD Siri E. Håberg, The National Institute of Public Health. Further, we want to acknowledge Trudy Perdrix-Thoma of Professional Standards Editing for English language editing.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data access
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.