
Abstract
Aims: We aimed to investigate associations between mental health and sociodemographic characteristics among schoolchildren in Denmark. Methods: We performed a cross-sectional survey from January to October 2019 among 4th to 9th graders (N=1247) based on pilot data from a nationwide research project Stress-free Everyday LiFe for Children and Adolescents REsearch (SELFCARE). We assessed mental health using the five-item World Health Organization Well-Being Index and the self-report version of the Strengths and Difficulties Questionnaire. We investigated associations between mental health and sex, age in terms of grade, type of school, family setting and geographic region using regression analysis. Results: Mental health was poorer among girls in the older classes compared to girls in 4th grade, and better among boys in the older classes compared to boys in 4th grade. We found no difference in mental health among schoolchildren in municipal and private schools. Mental health was poorer among both girls and boys living alternately with their parents compared to residing with both of them. Mental health varied across geographic regions.
Keywords
Introduction
Mental health is a fundamental component of the World Health Organization’s (WHO) definition of health [1]. It is conceptualised as a state of well-being in which the individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to contribute to his or her community [2]. In this positive sense, mental health is the foundation for well-being and effective functioning for an individual and a community [1]. With respect to children, an emphasis is placed on developmental aspects such as (a) having a positive sense of identity, (b) the ability to manage thoughts and emotions and to build social relationships and (c) the aptitude to learn and to acquire an education, ultimately enabling them to become fully active individuals within society [3].
The mental health of children and young people is a global public health challenge. Most mental disorders begin during youth, although they are often first detected later in life. Mental disorders account for a large proportion of the disease burden in children and young people in all societies [4]. Up to half of mental disorders begin before the age of 15 [5]. Cross-national studies suggest that approximately one out of every four to five young people in the general population will suffer from at least one mental disorder in any given year [4]. Therefore, mental disorders have huge costs for the individuals affected as well as for society as a whole. The total costs related to mental disorders in Europe are estimated to account for more than €600 billion. Among the European countries, Denmark has the highest costs related to mental disorders in terms of percentage of GDP (5.4%) [6].
However, mental health is more than the absence of mental disorders [1]. The WHO collaborative cross-national study, Health Behaviour in School-aged Children (HBSC), has provided information about the well-being of 11- to 15-year-old schoolchildren for more than 30 years. The 2017/2018 survey report presents data from 220,000 young people in 45 countries and regions in Europe and Canada. The survey found that mental well-being has worsened in many countries during recent years. Furthermore, the results indicate consistently that boys are more likely to report better mental well-being than girls, and that these sex differences increase with age [7]. Focusing specifically on Denmark, the vast majority of Danish schoolchildren report good mental health. Despite this, the Danish HBSC survey has shown a decrease in the proportion of 15-year-olds with high life satisfaction since 2002 [8]. The potential gains from strengthening mental health among children and adolescents are therefore substantial.
According to the WHO, mental health is a public issue that requires political priority and action. This is to ensure that stigmatisation and discrimination are broken down, and that effective promotion and prevention are established [9]. In order to ensure healthy lives and to promote well-being, it is important to have accurate information about mental health within the population. It is well known that the casual mechanisms for mental disorders in young people are complex, and that biological, psychological and social risk and protective factors play a role [4]. However, adolescents are often neglected as a population group within mental health statistics in general. Little attention has been paid to inequalities related to sociodemographic characteristics among this group [7].
In addition to sex and age, mental health in children and adolescents may be associated with type of school, family setting and geographic region. In Denmark, compulsory education is 10 years (0th to 9th grade) covered by the Danish public school programme in municipal schools. Yet, it is possible for parents to enrol their children in private schools. Currently, there are 1339 (71%) municipal schools and 538 (29%) private schools in Denmark [10]. In general, children in private schools have a stronger socio-economic profile [11]. In 2018, it was estimated that 17.7% of Danish children went to a private school [12]. In most Western countries, it is estimated that about half of first marriages will be dissolved [13]. Studies have found that children with divorced or separated parents had less favourable outcomes on well-being than children living with both parents [14,15]. The National Danish Health Profile, which includes Danes aged 16 and older, indicates minor regional differences in mental health. Compared to the national average, a slightly larger proportion of Danes with poor mental health is seen in Region Zealand and the Region of Southern Denmark, and a slightly smaller proportion in Central Denmark Region [16].
Aims
We aimed to investigate associations between mental health and sociodemographic characteristics among Danish schoolchildren. We hypothesised (a) poorer mental health among girls compared to boys, (b) poorer mental health among children attending municipal schools compared to children attending private schools, (c) poorer mental health among children not living with both parents compared to children from intact families and (d) regional differences in mental health.
Methods
Study design and participants
From January to October 2019, we conducted a cross-sectional survey in a sample of schoolchildren (N=1247) from 63 municipal schools (n=957) and 21 private schools (n=290). The survey was a pilot test of data collection procedures in a nationwide research project Stress-free Everyday LiFe for Children and Adolescents REsearch (SELFCARE) (registered at ClinicalTrials.gov: identifier NCT04208113, December 2019). We asked the 191 teachers from the 110 schools included in the SELFCARE project to collect questionnaire data from a lower secondary education school class (4th–9th grade). Questionnaires where no parental informed consent was provided were excluded.
Procedure
In order to collect parental informed consent, we e-mailed a written statement of consent to each of the 191 teachers. The teachers printed the statements of consent, and the pupils took a copy home and asked a parent to sign it. The pupils then returned the statement of consent to their teachers, who e-mailed them back to the research group via a secure e-mail system through Aarhus University. Data were collected online in class with an electronic compilation of questionnaires, including the outcome measures and covariables mentioned below, and stored using the Research Electronic Data Capture (REDCap) tool hosted by Aarhus University [17].
Outcome measures and covariables
We assessed mental health using the five-item World Health Organization Well-Being Index (WHO-5) and the self-report version of the Strengths and Difficulties Questionnaire (SDQ).
WHO-5
The WHO-5 [18] is a short questionnaire measuring subjective well-being. It consists of five simple and positively worded statements. Participants were asked to rate how well each of the five statements applied to them when considering the last two weeks. Each item is scored on a six-point Likert scale ranging from 5 (all of the time) to 0 (none of the time). The points are added together and multiplied by four, calculating a total score ranging from 0 (absence of well-being) to 100 (maximal well-being). A total score below 50 is indicative of reduced well-being. In a Danish general population study, the mean WHO-5 score was 70 [19]. The tool was developed for adults but is used for children as young as nine [20].
SDQ
The self-report version of the SDQ [21] is a behavioural screening questionnaire measuring subjective well-being and social, emotional and behavioural functioning among children. It consists of 25 statements, some worded positively and others negatively. Participants were asked to rate each statement on a three-point Likert scale ranging from 2 (very true) to 0 (not true). The 25 items are divided between five subscales of five items each, generating scores for emotional symptoms, conduct problems, hyperactivity/inattention, peer relationship problems and prosocial behaviour. All subscales except the last one are summed to generate a total difficulties score. The subscales range from 0 to 10, with higher values indicating poorer well-being and functioning for four of the subscales (emotional symptoms, conduct problems, hyperactivity/inattention and peer relationship problems) and better well-being and functioning for the prosocial behaviour subscale. The total difficulties score ranges from 0 to 40, with higher values indicating poorer well-being and functioning. Goodman et al. have shown that the odds ratio (OR) for having a mental disorder was 1.23 (95% confidence interval (CI) 1.21–1.25) per one-point increase in the total difficulties score and that the OR for developing a mental disorder within a three-year period was 1.16 (95% CI 1.13–1.18) per one-point increase in the total difficulties score [22]. In 2019, Danish SDQ norms were published [23].
Participants had to tick the appropriate box for each covariable: sex – girl or boy; grade – 4th grade, 5th grade, 6th grade, 7th grade, 8th grade or 9th grade; type of school – municipal school or private school; family setting – lives with mom and dad who live together, lives alternately with mom and dad equally with both, lives alternately with mom and dad mostly with one of them, lives only with one parent, lives mostly with foster family or other family or other; geographic region – the Capital Region of Denmark, Region Zealand, Central Denmark Region, the Region of Southern Denmark or the North Denmark Region. We used grade as an indicator of age group, since grade, in addition to representing a uniform age group, also expresses a number of common conditions in children’s and adolescents’ daily lives.
Statistical analysis
We calculated proportions for categorical variables, and means with standard deviations for continuous variables. We examined sociodemographic characteristics and self-reported mental health for all participants and for girls and boys separately because of the well-known systematic differences in mental health between sexes [7]. Separately for girls and boys, we examined associations between outcomes and covariables by use of linear regression models adjusting for grade, type of school, family setting and geographic region. Results are presented as differences in means with 95% CI. All statistical analyses were performed using Stata/IC v16 (StataCorp, College Station, TX).
Ethics
The study was approved by the Danish Data Protection Agency (AU-id. no.: 2016-051-000001/1145).
Results
A total of 135/191 (71%) teachers included in the SELFCARE project contributed to the survey study. The teachers were from 84/110 (76%) schools included in the project. Out of 77 municipal schools, 63 (82%) were included, and out of 33 private schools, 21 (64%) were included. A total of 1247/2746 (45%) schoolchildren had parental informed consent to participate in the study.
Background and characteristics
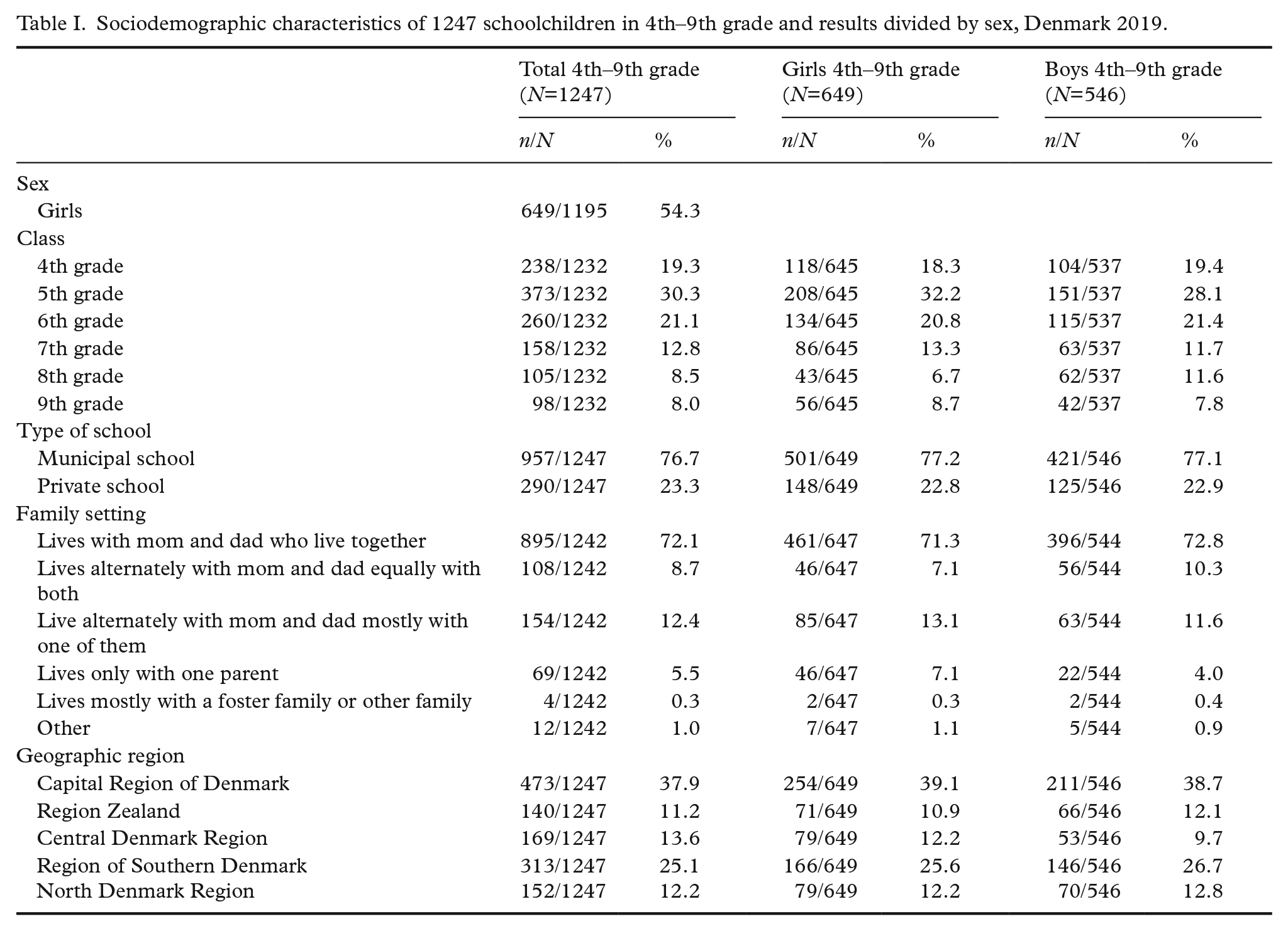
Approximately half of the 1247 participants were girls (54.3%; Table I). The largest percentage of participants were in 5th grade (30.3%). Most of the participants went to a municipal school (76.7%). Among participants, 72.1% resided with both parents. Approximately one third of the participants were from the Capital Region of Denmark (37.9%). Characteristics divided by sex are presented in Table I.
Sociodemographic characteristics of 1247 schoolchildren in 4th–9th grade and results divided by sex, Denmark 2019.
Self-reported mental health
Table II presents the WHO-5 mean scores as well as the SDQ mean scores. The WHO-5 mean scores were comparable to the Danish general population mean score [19]. The SDQ mean scores were in the category ‘close to average’ compared to Danish norms [23] (Table II).
Self-reported mental health among 1247 schoolchildren in 4th–9th grade and results divided by sex, Denmark 2019.

Missing data: a<5%; b<10%.
M: mean; SD: standard deviation; WHO-5: five-item World Health Organization Well-Being Index; SDQ: Strengths and Difficulties Questionnaire.
Sociodemographic associations with mental health
Tables III and IV show that mental health was associated with sociodemographic characteristics. Mental health, measured by the WHO-5, was poorer among girls in 7th grade (–6.40 (95% CI –11.11 to –1.70)), 8th grade (–7.28 (95% CI –13.18 to –1.38)) and 9th grade (–15.06 (95% CI –20.40 to –9.72)) compared to girls in 4th grade (Table III). Mental health, measured by the SDQ total difficulties score, was better among boys in 6th grade (–2.42 (95% CI –3.90 to –0.95)), 7th grade (–1.87 (95% CI –3.62 to –0.12)), 8th grade (–3.00 (95% CI –4.79 to –1.21)) and 9th grade (–3.86 (95% CI –5.80 to –1.91)) compared to boys in 4th grade (Table IV). There was no difference in mental health among children in municipal and private schools. Mental health, measured by the WHO-5, was poorer among both girls (–4.25 (95% CI –8.24 to –0.26)) and boys (–5.35 (95% CI –9.99 to –0.71)) living alternately with their parents, mostly with one of them, compared to girls and boys residing with both parents (Table III). This was also the case when measured by the SDQ total difficulties score. Mental health was poorer among both girls (1.63 (95% CI 0.39–2.87)) and boys (1.88 (95% CI 0.43–3.33)) living alternately with their parents, mostly with one of them, compared to girls and boys residing with both parents (Table IV). Among boys, mental health measured by the WHO-5 was also poorer when living with only one parent (–8.60 (95% CI –16.04 to –1.17)) compared to boys residing with both parents (Table III). Mental health, measured by the WHO-5, was better among girls living in the North Region of Denmark (5.84 (95% CI 1.53–10.15)) compared to girls living in the Capital Region of Denmark (Table III) and better among boys living in Central Denmark Region (6.00 (95% CI 0.48–11.52)) compared to boys living in the Capital Region of Denmark (Table III). Mental health, measured by the SDQ total difficulties score, was better among girls living in Central Denmark Region (–1.66 (95% CI –3.04 to –0.27)) compared to girls living in the Capital Region of Denmark (Table IV).
Associations between mental health measured by the WHO-5 and sociodemographic characteristics among 1247 schoolchildren in 4th–9th grade divided by sex, Denmark 2019.

Crude.
Adjusted for grade, type of school, family setting and geographic region.
M: mean; SD: standard deviation; 95% CI: 95% confidence intervals.
Associations between mental health measured by the SDQ total difficulties score and sociodemographic characteristics among 1247 schoolchildren in 4th–9th grade divided by sex, Denmark 2019.

Crude.
Adjusted for grade, type of school, family setting and geographic region.M: mean; SD: standard deviation; 95% CI: 95% confidence intervals.
See online version for the SDQ subscales (Supplemental Tables SV and SVI).
Discussion
In line with previous findings our study showed that in general, the mental health of Danish schoolchildren is good [8]. Our results substantiate the well-known phenomenon that mental health gets poorer with age among girls and better with age among boys. Mental health among both sexes was poorer if they had alternate living arrangements compared to residing with both parents. Mental health was better among girls living in the North Region of Denmark and better among both girls and boys living in Central Denmark Region compared to those living in the Capital Region of Denmark. We found no association between mental health and type of school.
It is useful to know that some sociodemographic characteristics are associated with poorer mental health among schoolchildren. Nevertheless, the solution is not necessarily to deliver differentiated initiatives promoting mental health focusing exclusively on children at high risk. The WHO recommends universally delivered psychosocial interventions to promote positive mental health and to prevent mental disorders. Based on available evidence, interventions should cover social and emotional learning, which may include components such as emotional regulation, problem solving, interpersonal skills, mindfulness, assertiveness and stress [24]. Schools are considered particularly useful for delivering interventions promoting mental health. Schools are one of the primary communities for children and adolescents, and they play a major role not only in the development of children’s and adolescents’ cognitive and academic skills, but also in their social and emotional development [25]. Universal interventions provide an opportunity to reduce a larger proportion of the total disease burden compared to high-risk interventions. The reason for this is that most cases of poor mental health occur among the many who are at low and moderate risk rather than among the few who are at high risk. Geoffrey Rose describes this as the prevention paradox [26]. In schools, universal interventions have the advantage that no children are pointed out and thus are not at risk of being stigmatised by their classmates. Implementing universal interventions still allows for the possibility of keeping an eye on those with the poorest mental health and helping to enhance their mental health.
Our study showed significant regional differences in mental health among Danish schoolchildren. The Danish SDQ norms published in 2019 were based on data from only one municipality in the Region of Southern Denmark [23]. The study sample used to establish the Danish norms may not be representative of Danish children in general. First, the sample included children with developmental difficulties attending special educational settings. Second, the sample did not include children attending private schools. Third, although not far from the national average, the municipality contributing to the data was characterised by a lower income and a shorter duration of education [23]. In the light of these limitations, we have identified a need for norms based on a study population representative of the whole country.
Strengths and limitations
This study includes schoolchildren from all five geographic regions in Denmark. This fact enhances the generalisability of the study findings with regard to associations between mental health and sociodemographic characteristics. Estimates of associations between variables are not as vulnerable to bias as prevalence estimates are [27]. However, the fact that only 45% of eligible schoolchildren in our survey had parental informed consent to participate means that selection bias affecting the mean values cannot be ruled out. General experience is that the motivation to participate in surveys is least among the socially disadvantaged in the population [27]. Furthermore, a lower socio-economic status is associated with higher SDQ problem scores [28]. Hence, we cannot rule out that our SDQ total scores are underestimated. Therefore, the exclusion of schoolchildren without parental informed consent may lead to a picture of better mental health among Danish schoolchildren compared to what it is really like. It is conceivable that the elaborate procedure for obtaining parental informed consent led to the low participation rate. A large part of the explanation for the lack of parental informed consent may be down to a simple oversight from the teachers, the schoolchildren or the parents. An option could have been to inform the parents about the survey and the possibility of withdrawing at any time instead of asking for parents to opt in. This has been done in previous surveys conducted in Danish schools [29].
Because of the cross-sectional study design, a statistical association between a sociodemographic characteristic and mental health is not synonymous with a causal correlation. However, the knowledge of the associations found, even without the causal connections, is valuable as a basis to target interventions [30].
Conclusions
In conclusion, we found associations between mental health and sex, age in terms of grade, family setting and geographic region among Danish schoolchildren. We found no association between mental health and type of school. Universal interventions in schools have the potential to improve mental health in all children as well as in high-risk and vulnerable groups without causing stigma.
Supplemental Material
sj-pdf-1-sjp-10.1177_14034948211002062 – Supplemental material for Associations between mental health and sociodemographic characteristics among schoolchildren. A cross-sectional survey in Denmark 2019
Supplemental material, sj-pdf-1-sjp-10.1177_14034948211002062 for Associations between mental health and sociodemographic characteristics among schoolchildren. A cross-sectional survey in Denmark 2019 by Michelle S. Beck, Lone O. Fjorback and Lise Juul in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
The authors wish to thank you all the participating schools, teachers and schoolchildren for their support in this survey study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.