
Abstract
Aims: Rates of parental separation have increased dramatically in recent decades. We evaluated the association of individuals’ childhood family structure with their somatic health over 46 years of follow-up. Methods: Data were drawn from the Northern Finland Birth Cohort, an ongoing project in which 12,058 participants born in 1966 have been followed from their 24th gestational week. Based on information supplied at age 14 years, family structure was categorised as ‘single-parent family’ and ‘two-parent family’. The anthropometric information, data from blood samples and medical history were collected from postal questionnaires and clinical examinations routinely performed at the ages of 31 and 46 years. Results: The study population comprised a total of 10,895 individuals; 85% (n=9253) were offspring of two-parent families and 15% (n=1642) of single-parent families. Type 2 diabetes (P=0.032) or prediabetes (P=0.007), psychoactive drug problems (P<0.001) and sexually transmitted diseases (P<0.001) were more common in the single-parent family group than in the participants from two-parent families. In addition, among men back diseases (P=0.002), and among women hypertension (P=0.003) and ovary infection (P=0.024) were more frequent in individuals affected by parental death than in those from two-parent families.
Background and aims
An individual’s family structure is important for the development of their emotional and physical health [1]. It has been observed that the two-parent family model (with both parents living in the same household as the offspring) is better for the offspring’s development than the single-parent family [2]. Divorce rates have increased significantly in the European countries since the 1960s [3]. Among families with children the proportion of single-parent families make up approximately 14% of all families in Europe [4]. More than half of all divorces happen when the offspring is under the age of 18 years [5].
All types of parental separations are associated with deficits in the offspring’s health and wellbeing from childhood to adulthood [6]. Even when parental separation occurs during the prenatal period, it can affect some subsequent health conditions in the offspring [7]. One study found that children affected by parental divorce were 50% more likely to develop health problems than children from a two-parent family [8]. Other studies have observed that the offspring from divorced families have more somatic health problems and diseases, such as overweight and obesity [7, 9] and asthma [9] than those who live with both parents. However, some studies have found that the offspring’s cardiometabolic health is unaffected by parental separation [10, 11].
Associations between parental separation and mental health problems in the offspring have been reported [6, 8, 12]. Children living in a single-parent family are twice as likely to exhibit stress [5] and lower levels of wellbeing [5, 6] than those who live with both parents. In addition, parental separation may have an impact on the offspring’s drug, tobacco and alcohol use [10, 11, 13]. Parental death has also been shown to associate with lower levels of wellbeing and an increased number of psychiatric diagnoses in the offspring [6, 14]. Young adults who have suffered parental bereavement often exhibit problems similar to those who have experienced parental divorce, such as poor mental and physical health and health risk behaviour [15].
Although previous studies have examined the associations between parental separation and the mental and somatic health of the offspring, to our knowledge, there is a lack of large-scale comprehensive studies investigating the long-term association of parental separation with the somatic health of the offspring. In the present descriptive study, we therefore examined the association between individuals’ family structure at the age of 14 years (two-parent vs. single-parent family with subgroups) and their morbidity over a 46-year follow-up period in the context of a large birth cohort study. Our hypothesis was that lifetime morbidity is more common among offspring of single-parent families compared to offspring of two-parent families.
Methods
Study design
This retrospective study examined data gathered as part of the Northern Finland Birth Cohort 1966 (NFBC1966) project. Based in the two northernmost former provinces of Finland (Oulu and Lapland), the NFBC1966 is a large, ongoing prospective, general population-based longitudinal birth cohort that comprises 96.3% of all live births in the regions with expected delivery date between 1 January 1966 and 31 December 1966 (initially a total of 12,231 individuals) [16]. Data on all members of the cohort were first collected during the 24th gestational week and subsequently at predetermined time points (birth and at ages 1, 14, 31 and 46 years). Postal questionnaires were sent to participants at the ages of 14, 31 and 46 years and clinical examinations were performed at the ages of 31 and 46 years [17]. All participants provided written consent, and the research plan was approved by the ethics committee of the Northern Ostrobothnia Hospital, Oulu, Finland.
Study protocol
Based on information supplied by the cohort members at age 14 years, the family structure of each was categorised as being from a two-parent family or a single-parent family. The single-parent families were further subdivided as follows: ‘one parent not living at home’; ‘father or mother deceased’ and ‘no information on father’.
The prevalence of diseases was based on information from the NFBC questionnaires at the ages of 31 and 46 years. For the purposes of the present study, an individual was classified as having any particular disease if they reported having received a diagnosis at either 31 or 46 years of age, or both. The participants’ diagnosed conditions were grouped into 24 classifications, which in turn were placed into seven categories (Supplemental Table I). The postal questionnaires at the ages of 31 and 46 years differed in terms of how they asked about diabetes and thyroid diseases. At age 31 years, the relevant questions were general ‘diabetes’ and ‘thyroid diseases’, whereas the questions at age 46 yearsspecifically asked for information on type 1 diabetes, type 2 diabetes, hypothyroidism and hyperthyroidism. Multimorbidity was defined as the presence of at least two chronic diseases.
Data on the following variables were recorded by a nurse or physician at the clinical examinations at the age of 46 years: Weight (to an accuracy of 0.1 kg), height (to an accuracy of 0.1 cm) and waist circumference (WC) (cm) were measured in light clothing [17]. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of the height in metres. In accordance with the classification provided by the World Health Organization, BMI (kg/m2) was categorised as underweight (BMI <18.5 kg/m2), normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25–29.9 kg/m2) or obese (BMI ⩾30 kg/m2). WC and BMI were additionally examined according to gender. Systolic and diastolic blood pressure levels (mmHg) were measured in a seated position after 15 minutes of rest using an automated device (Omron digital automatic blood pressure monitor model M10-IT; Omron Kyoto, Japan) and an appropriately sized cuff on the right arm. The measurements were performed twice at age of 31 years and three times at age 46 years and thereafter the mean of blood pressure values was calculated [17].
At age 46 years blood samples were collected after an overnight fasting period. They were centrifuged and analysed immediately in NordLab Oulu, a testing laboratory (T113) accredited by the Finnish Accreditation Service (FINAS) (EN ISO 15189). Fasting plasma glucose (FPG) (mmol/l) was analysed as previously described [18]. Plasma total cholesterol (mmol/l), high-density lipoprotein (HDL) cholesterol (mmol/l), low-density lipoprotein (LDL) cholesterol (mmol/l) and triglycerides (mmol/l) were determined using an enzymatic assay method. The concentration of haemoglobin A1c (HbA1c) and the concentration of total haemoglobin were measured by the immunochemical assay method. The ratio is reported as percentage HbA1c (NGSP) (all methods by Advia 1800; Siemens Healthcare Diagnostics Inc., Tarrytown, NY, USA).
Metabolic syndrome was defined according to the International Diabetes Federation criteria as follows: abdominal obesity (WC ⩾94 cm in men or ⩾80 cm in women) and at least two of the following: blood pressure 130/85 mmHg or greater or previously diagnosed hypertension; HDL cholesterol less than 1.03 mmol/l in men or less than 1.29 in women; triglycerides greater than 1.7 mmol/l; FPG level 5.6 mmol/l or greater or previously diagnosed type 2 diabetes [19]. The present study did not take information on diabetes treatment into account when making the classifications. Participants who did not report a diagnosis of diabetes in the questionnaire at the age of 46 years were screened retrospectively for prediabetes and diabetes by examination of their FPG and HbA1c.
We examined disease prevalence and anthropometrics in the before-mentioned categories of family unit to determine any impact of family structure on later clinical outcomes. To get a better overview of the present study sample, we included sociodemographic variables in our analyses.
Statistical methods
Continuous clinical outcome measures are presented as mean and standard deviation (SD), and categorical questionnaire variables as proportions. Analysis of variance (ANOVA) was used to evaluate the associations between study groups and clinical outcome measures, while associations between study groups and categorical variables were examined using contingency tables with the χ2 test, or Fisher’s exact test when appropriate. Differences between study groups among continuous variables were evaluated with Tukey’s honest significant difference test or Games–Howell post hoc tests. The Benjamini–Hochberg (B–H) false discovery rate procedure was used to control for type I error caused by multiple comparisons in the contingency tables. All P values (P and B–Hp) were two-tailed and a P value less than 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics, version 25 (IBM Corporation and its licensors 1989, 2017). Because of the large study size (also after omitting the missing data) and numerous of non-continuous variables, missing data were omitted from the analysis rather than being imputed.
Results
There was initially a total of 12,231 individuals in NFBC and at the age of 14 years total respondents were 10,895 individuals. In the present study, two groups were formed based on information at age 14 years: (a) two-parent family (n=9253); and (b) single-parent family (n=1642). Single-parent family was additionally divided into three subgroups: (a) father or mother deceased (n=710); (b) one parent not living at home (n=882); and (c) no information on father (n=50). Subgroups ‘one parent not living at home’ and ‘no information on father’ were combined (n=932). The number of respondents in follow-ups at 31 years was 8767 (71.7% of the initial study population) and at 46 years it was 6868 (56.2% of the initial study population) from postal questionnaires, and 6033 (49.3% of the initial study population) and 5861 (47.9% of the initial study population), respectively, from clinical examinations [20]. The number of responses varied between participants.
Table I shows the cohort’s anthropometric characteristics and cardiovascular measurements at the age of 46 years. The mean levels of LDL cholesterol and triglycerides were significantly higher in individuals from a single-parent family than those from a two-parent family (P=0.044 and P=0.006, respectively). Furthermore, mean FPG was significantly higher in the ‘one parent not living at home’ subgroup (P=0.012) than in the ‘two-parent family’ group.
The characteristics of the study population at the age of 46 years. Subgroups categorised according to their childhood family structure at the age of 14 years.
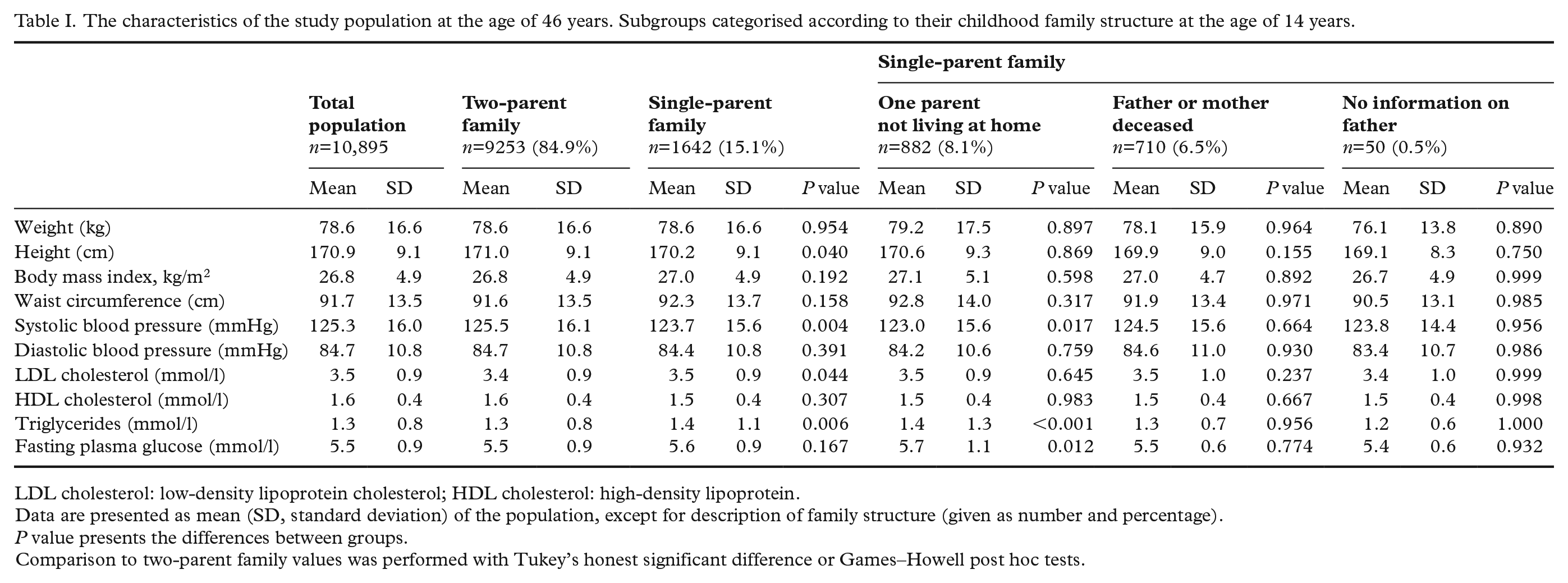
LDL cholesterol: low-density lipoprotein cholesterol; HDL cholesterol: high-density lipoprotein.
Data are presented as mean (SD, standard deviation) of the population, except for description of family structure (given as number and percentage).
P value presents the differences between groups.
Comparison to two-parent family values was performed with Tukey’s honest significant difference or Games–Howell post hoc tests.
Table II presents the descriptive statistics for the sociodemographic variables of the study population. Information from postal questionnaires was completed by the cohort mothers during pregnancy and at the offspring ages of 14 and 46 years. During pregnancy, almost the half of the two-parent families lived in an owner-occupied dwelling, while in the single-parent family subgroup ‘one parent not living at home/no information on father’ only one-third of the families occupied their own property (P<0.001). Mothers in the two-parent family group were significantly older during pregnancy than mothers in the single-parent family subgroup ‘one parent not living at home/no information on father’ (27.8 and 25.3 years, respectively; P<0.001). Occupational status during pregnancy was higher among mothers in the single-parent family subgroup ‘one parent not living at home/no information on father’ than in those from two-parent families (P<0.001). Grand multiparity was more frequent in two-parent families than in the single-parent family subgroup ‘one parent not living at home/no information on father’ (P<0.001). The offspring of two-parent families were significantly more likely to be in a relationship and less likely to be divorced or separated than those in the ‘one parent not living at home/no information on father’ single-parent family subgroup (P=0.007). These associations remained statistically significant after B–H correction.
The descriptive statistics for the sociodemographic variables of the study population. Data were gathered from postal questionnaires completed by cohort mothers during pregnancy and by the offspring at the ages of 14 and 46 years. Subgroups categorised according to childhood family structure at the age of 14 years.
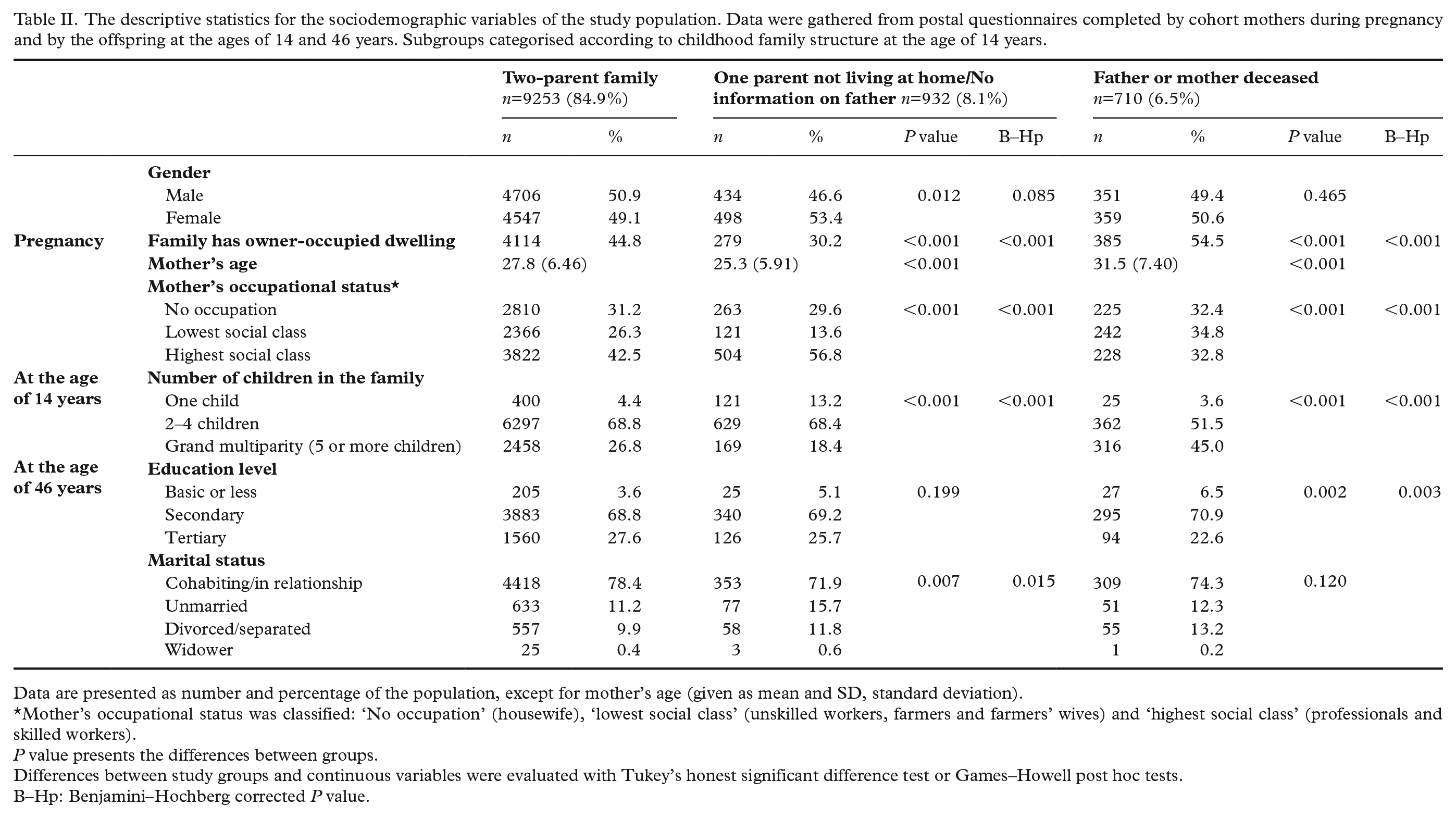
Data are presented as number and percentage of the population, except for mother’s age (given as mean and SD, standard deviation).
Mother’s occupational status was classified: ‘No occupation’ (housewife), ‘lowest social class’ (unskilled workers, farmers and farmers’ wives) and ‘highest social class’ (professionals and skilled workers).
P value presents the differences between groups.
Differences between study groups and continuous variables were evaluated with Tukey’s honest significant difference test or Games–Howell post hoc tests.
B–Hp: Benjamini–Hochberg corrected P value.
The lifetime prevalence of diseases and health conditions of the study population at the age of 31 and 46 years, by childhood family structure at the age of 14 years, are shown in Table III. When compared with the two-parent family group, the following conditions were significantly more common in the subgroup ‘one parent not living at home/no information on father’ than in the two-parent family group: psychoactive drug problems (P<0.001) and sexually transmitted diseases (P<0.001). These associations remained statistically significant after B–H correction (Table III).
The lifetime prevalence of diseases and health conditions.
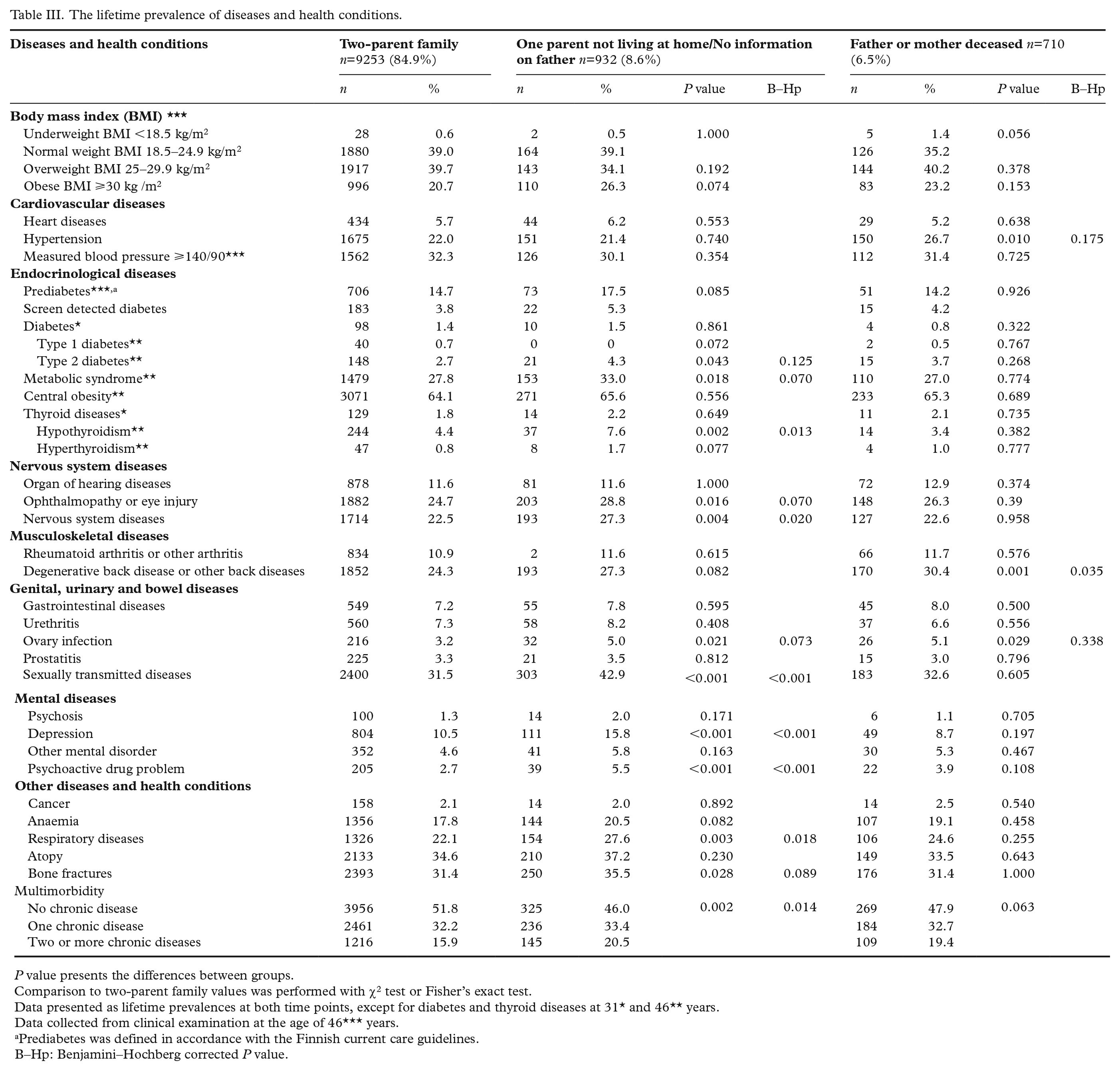
P value presents the differences between groups.
Comparison to two-parent family values was performed with χ2 test or Fisher’s exact test.
Data presented as lifetime prevalences at both time points, except for diabetes and thyroid diseases at 31* and 46** years.
Data collected from clinical examination at the age of 46*** years.
Prediabetes was defined in accordance with the Finnish current care guidelines.
B–Hp: Benjamini–Hochberg corrected P value.
Table IV shows the lifetime prevalence of the diseases and conditions stratified by sex. The following diseases were significantly more common in female offspring in the single-parent family subgroup ‘one parent not living at home/no information on father’ than in women from two-parent families: metabolic syndrome (P=0.014), type 2 diabetes (P=0.032), hypothyroidism (P=0.005), ophthalmopathy or eye injury (P=0.009), nervous system diseases (P=0.019) and respiratory diseases (P=0.003). Only the association with hypothyroidism and respiratory diseases remained significant after B–H correction. In addition, among women, obesity (P=0.040), hypertension (P=0.003), type 2 diabetes (P=0.030) and ovary infection (P=0.024) were more common in the ‘father or mother deceased’ subgroup than in the two-parent family group; however, none of these associations remained significant after B–H correction. Prediabetes (P=0.007), degenerative back disease or other back diseases (P=0.047), depression (P<0.001), bone fractures (P=0.005) and multimorbidity (P=0.040) were significantly more common in the male offspring from the single-parent family subgroup ‘one parent not living at home/no information on father’ than in men from two-parent families. Only the associations with prediabetes, depression and bone fractures remained significant after B–H correction. Furthermore, degenerative back disease or other back diseases (P=0.002) were more common in men from the ‘father or mother deceased’ subgroup than in men from two-parent families; however, this association did not remain significant after B–H correction (Table IV).
The lifetime prevalence of diseases and health conditions stratified by sex.
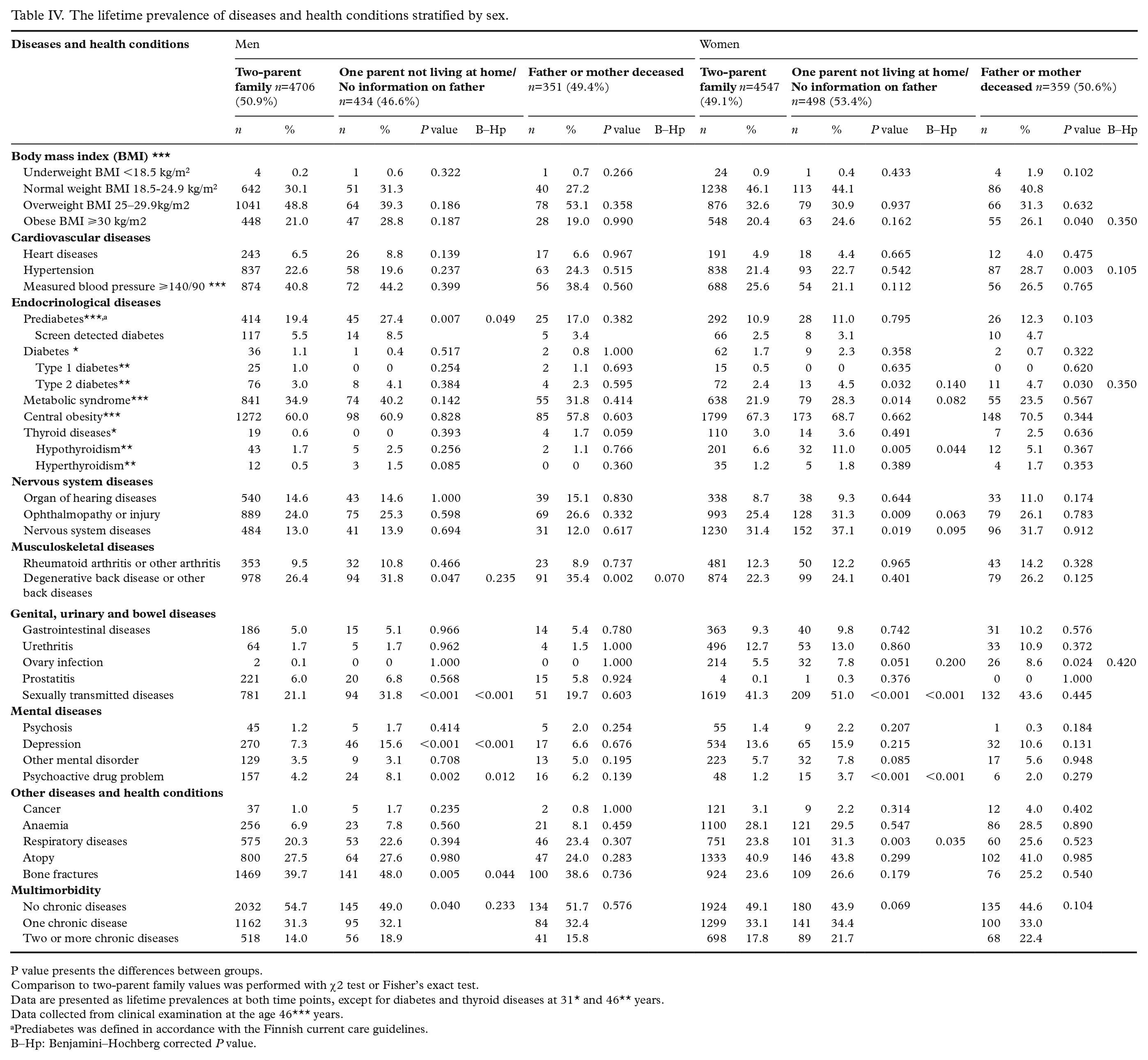
P value presents the differences between groups.
Comparison to two-parent family values was performed with χ2 test or Fisher’s exact test.
Data are presented as lifetime prevalences at both time points, except for diabetes and thyroid diseases at 31* and 46** years.
Data collected from clinical examination at the age 46*** years.
Prediabetes was defined in accordance with the Finnish current care guidelines.
B–Hp: Benjamini–Hochberg corrected P value.
Discussion
In this large prospective population-based study of 10,895 individuals, we observed that adulthood lifetime morbidity was associated with childhood family structure, being higher in the offspring of single-parent families than in the offspring of two-parent families. This pattern was particularly apparent in type 2 diabetes or prediabetes, the use of psychoactive drugs and sexually transmitted diseases. Morbidity was especially high in the combined subgroup ‘one parent not living at home/no information on father’ and among women in single-parent families. Although the significance of these effects may be considered minor at the individual level, they are relevant at the overall population level.
Metabolic syndrome, a cluster of obesity-related cardiometabolic risk factors, was more prevalent among women in the combined subgroup ‘one parent not living at home/no information on father’ than in the two-parent family group. We also observed that LDL cholesterol and triglyceride values were higher in the single-parent family group than in the two-parent family group. This aligns with a previous report that parental loss in childhood is associated with the development of metabolic syndrome in adulthood [21]; however, controversial findings have been reported [11]. An elevated prevalence of type 2 diabetes has been reported in adults that were affected in childhood by parental death [22] or separation [23], which our findings confirm. The increased cardiometabolic risk factors among single-parent family offspring might be partly explained by the higher prevalence of type 2 diabetes.
We observed that the drinking and other drug problems were more common in the single-parent group. This aligns with previous findings that people affected by parental separation start alcohol consumption earlier [24], and are more likely to develop problematic drinking habits in adulthood [10]. Earlier alcohol initiation is linked with a higher risk of alcohol dependence in later life [25], which might partly explain the higher prevalence of problem drinking in adults who were affected by parental separation in childhood. Our finding regarding psychoactive drug problems is supported by the previous report from the NFBC1966 cohort that overdosing by drugs resulting in hospitalisation is more common in the offspring from single-parent families [13]. We also observed a higher prevalence of sexually transmitted diseases in the single-parent family group. One previous study has also found that people who have experienced at least one childhood adversity, such as parental separation, have a higher likelihood of sexually transmitted diseases [12]. Furthermore, parental separation has been linked with sexual risk behaviour patterns such as earlier sexual debut [12, 24] and having a greater number of sexual partners [26].
Parental separation has been shown to have both short and long-term negative effects on several domains of the offspring’s societal functioning [6]. The results of the present study appear to support these findings.
This study has several strengths, including its large cohort size and its longitudinal design. The NFBC1966 cohort is a representative, unselected population-based sample of Finnish adults. A further strength is the lifetime study setting of the NFBC1966 project, which includes multiple cross-sectional clinical examinations. The participation rate remained high during the 46 years of follow-up and a large variety of diseases were taken into account in the present analysis. Blood samples were examined and measurements of other relevant components were taken by trained physicians or study nurses using identical procedures. Also, all blood samples were analysed in the same laboratory by the same method.
Family status was recorded at the time when the participants were 14 years old. However, a potential limitation of the study is presented by the fact that no subsequent parental separation was documented and therefore the number of offspring who were affected by parental separation could be higher than reported here. Similarly, no information was available regarding later reconciliation or the introduction of step-parents, any of which might have had an effect on the participants’ family dynamics. The formation of our single-parent family subgroups was hindered by small numbers of participants, which necessitated the combination of the ‘one parent not living at home’ and ‘no information on father’ groups. It must be acknowledged that the practical effect on the offspring’s daily life may have varied significantly between these subgroups; when the father is not living at home he could nevertheless be a part of the offspring’s life, even if not on a daily basis. This is very different to there being no information about the father – in this situation the father has no contact whatsoever with the offspring. A further potential weakness of the study may be that disease diagnoses (although made by a doctor) were self-reported by the participants, which may have led to inaccuracies in the data. Our study was descriptive in design, and therefore did not control for factors that may confound findings in this complex area. Therefore, the influence and possible causal roles of such factors should be explored in future studies.
Conclusions
In conclusion, to the best of our knowledge, we can state that our study was the first to investigate extensively the prevalence of somatic diseases in the offspring of single-parent families over 46 years of follow-up. The findings of our descriptive study suggest that some somatic diseases are more prevalent in individuals brought up in single-parent families than in those from two-parent families. Clinicians should be aware of the potential association between patients’ family structure and their somatic health, and consider targeted disease screening in people from single-parent families. Active research on the associations of parental separation with the offspring’s somatic health should be continued, particularly considering the influence of confounding factors. There is public and scientific concern about this issue, and therefore support from healthcare professionals and society is warranted.
Supplemental Material
sj-xlsx-1-sjp-10.1177_14034948211014296 – Supplemental material for Parental separation and offspring morbidity in adulthood: a descriptive study of the Northern Finland Birth Cohort 1966
Supplemental material, sj-xlsx-1-sjp-10.1177_14034948211014296 for Parental separation and offspring morbidity in adulthood: a descriptive study of the Northern Finland Birth Cohort 1966 by Heidi Varis, Maria Hagnäs, Ilona Mikkola, Tanja Nordström, Katri Puukka, Anja Taanila and Sirkka Keinänen-Kiukaanniemi in Scandinavian Journal of Public Health
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Northern Finland Birth Cohort 1966 was supported by the University of Oulu grant nos. 65354 and 2400069; Oulu University Hospital Grant Numbers 2/97, 8/97 and 24301140; Ministry of Health and Social Affairs grant nos. 23/251/97, 160/97, 190/97; National Institute for Health and Welfare, Helsinki grant no. 54121; Regional Institute of Occupational Health, Oulu, Finland grant nos. 50621, 54231; and ERDF European Regional Development Fund Grant Number 539/2010 A31592. Heidi Varis has received funding from the Juho Vainio Foundation and the Finnish General Practice Foundation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.