
Abstract
Background and aim:
It is generally accepted that functional somatic disorders (FSDs) are a product of biological, psychological, and social factors. Social position might be part of this complex, but the literature on this issue is currently heterogeneous and inconsistent. The aim of the present study was – in a population-based cohort – to test the hypothesis that lower social position would be associated with higher a risk of FSD.
Method:
The association between social position and FSD was examined in a cross-sectional study with various measures of social position (education as measured by vocational training; employment; cohabitation; subjective social status) and delimitations of FSD (irritable bowel syndrome, chronic fatigue syndrome, fibromyalgia, bodily distress syndrome, and symptom profiles). The associations were analyzed using logistic regressions to calculate odds ratios and 95% confidence intervals. Each social measure was analyzed independently and was adjusted for age and sex.
Results:
Lower levels of vocational training, being unemployed, and living alone were associated with higher risk of FSD, regardless of the FSD delimitation. There was also a significant negative association between subjective evaluated social status and FSD. The associations remained after multiple adjustments, and seemed to be strongest for the more severe FSD-types.
Conclusions:
Keywords
Introduction
Functional somatic disorder (FSD) is an umbrella term used to characterize various conditions with “persistent and troublesome physical symptoms that are accompanied by impairment or disability” [1]. Irritable bowel syndrome (IBS), fibromyalgia (FM), and chronic fatigue syndrome (CFS) were some of the first defined diseases now categorized as FSDs.
A large overlap between these syndromes has been found, leading to the question of whether they are distinct diseases or represent the same underlying condition [2–4]. The diagnostic construct of bodily distress syndrome (BDS) [3–5] has, therefore, been introduced as an alternative diagnostic approach. Consequently, it has been suggested to include more than just one delimitation when assessing FSD [6].
Little is known about the etiology of FSD, but it is generally accepted that its development is influenced by biological, psychological, as well as social factors [1,7,8]. Low social position might affect the risk of FSD by increasing the overall vulnerability – for example, through health-related behaviors, poor health literacy, and low adherence to health recommendations. A higher education might lead to better interaction with the healthcare system and better health behaviors. Education is often understood as an indicator of social position in early life, as it is strongly determined by the characteristics of one’s parents, and it is achieved in early adulthood [9]. Being employed brings privileges such as more material resources [9] and access to more extensive health care. Being employed also contributes to a larger social network, which has been shown to affect health through a biopsychological pathway [10].
Importantly, the etiology is also multi-directional; for example, living with FSD might result in a lower level of functionality and, therefore, affect educational level and employment status. Thus, indicators of social position can be associated with FSD in numerous ways, both as a mediator and a confounder [11].
Despite the inconsistency in terminology and measurements of social position, a number of studies have found a social gradient in FSD [12–21]. However, most studies dealing with social position and FSD are smaller studies in patients from specialized clinical settings [3,5,17,20], and are hampered by selection bias and lack of generalizability. Former studies are also hampered by the fact that usually only one parameter of social position has been taken into consideration at a time, which may be too simplistic, as social position might be associated with FSD through various mechanisms. As most studies focus on only one type of FSD, the “whole nature of FSD” is not understood [6]. Thus, the associations to IBS, CFS, and FM might vary due to differences in these diseases, and studies focusing on only one type of FSD are hampered by the heterogeneity in the definition of FSD. Similarly, the association between social position and FSD might also vary depending on the severity of FSD, as patients with severe FSD might constitute an especially vulnerable group.
Against this background, the aim of the present study was to assess whether different indicators of social position were associated with various delimitations of FSD in a population-based cohort. We hypothesized that lower social position would be associated with higher risk of FSD. We also explored whether the associations differed for the various FSD delimitations.
Methods
Study population
This cross-sectional study was based on data from the Danish Study of Functional Disorders (DanFunD). DanFunD consists of two cohorts: DanFunD part one (n = 2163) and DanFunD part two (n = 7493) [22]. The participants were all born in Denmark, were between 18 and 76 years old, and lived in 10 municipalities in the western part of greater Copenhagen. The participants were randomly selected based on the nationwide Danish Civil Registration system. A total of 9656 (33.7%) out of 28,433 invited participants were included in the DanFunD cohort (Supplemental material 1).
Written informed consent was obtained from each participant before participation, and the study was approved by the Ethical Committee of Copenhagen County (Ethics Committee: KA-2006-0011; H-3-2011-081; H-3-2012-0015) and the Danish Data Protection Agency.
Measures of social position
All participants went through general health examinations and filled in extensive questionnaires on social position and health. The questionnaires were used to define the following exposure variables.
Education was based on two questions: “Have you completed vocational training?” and “If yes, what kind of vocational training?”. The variable was categorized into four levels: skilled worker or <1 year of vocational training (e.g. trainee or skilled craftsman) (reference-group), <3 years of vocational training (e.g. social and health assistant or technician), three or four years of vocational training (e.g. teacher or nurse), and >4 years of vocational training (e.g. doctor or engineer).
Employment status was dichotomized as employed and not employed based on the question: “What is your employment status?”. Not employed included both participants who were formerly employed and participants who had never been employed due to small numbers of the latter (n = 134). We did not have information about the weekly work hours or the type of work.
Cohabitation was based on two questions: “What is your legal marital status?” and “Have you ever cohabited?”. The variable was dichotomized as cohabitating and non-cohabitating. Participants who previously had been cohabitating, but were not currently, were classified as not cohabitating.
Subjective social status, which is “referring to an individuals’ perception of his/her place in the socioeconomic structure” [23], was defined by asking the participants to rate their own social status on a scale of 1 to 10, with 1 being the lowest and 10 being the highest in society. Subjective social status was assessed as a categorical variable with four levels: lowest (1–4), low (5), high (6–7), and highest (8–10). Subjective social status was included to provide a more global and subjective picture of the individuals’ social position.
Measures of FSD
The DanFunD study included three different delimitations of FSD [4,6,24] based on self-reported symptom questionnaires: traditional FSDs (IBS, FM, CFS); BDS; and symptom profiles (SPs).
In short, the traditional FSDs (IBS, FM, and CFS) were assessed according to international published criteria [6]. The definition by Kay and Jorgensen [25] was used to define IBS. The American College of Rheumatology Criteria [26] and the definition by White et al. [27] was used to define FM, and the definition by Chalder et al. [28] was used to define CFS.
Since overlaps between the syndromes have been found, the pure syndromes (individuals with only one type of traditional FSD: IBS-pure, FM-pure, and CFS-pure) were included as well.
The BDS approach is based on clusters of symptoms: cardiopulmonary (CP), gastrointestinal (GI), musculoskeletal (MS), and general symptoms (GS). To identify BDS cases, the 25-item BDS checklist was used [5]. Single/oligo-organ BDS was assigned to participants with at least four symptoms within one or two of the four BDS symptom clusters. Multiorgan BDS was assigned to participants with at least four symptoms within at least three of the four BDS symptom clusters [4,6].
The DanFunD study also presents eight data-driven SPs identified by latent class analysis [24]: one characterized by low probability of any symptoms (“no symptoms”); three profiles characterized by few, specific symptoms (“muscle/joint”, “lower GI”, “GS”); three characterized by high probability of specific combinations of multiple symptoms from different organ systems (“MS and GS”, “MS, GI, and fatigue”, “GI, CP, and GS”); and one characterized by high probability of all symptoms (“all symptoms”). The SPs were dichotomized as single SPs (“muscle/joint”, “lower GI”, “GS”) versus no symptoms; and multiple symptoms profiles (“MS and GS”, “MS, GI, and fatigue”, “GI, CP, and GS”) versus no symptoms; and all symptoms profile versus no symptoms.
Non-responders
For all the invited participants, we extracted information on highest earned education and cohabitation status from registers in Statistics Denmark, as well as information on any prior hospital admissions since 1995 with selected FSD and common mental disorders from the Danish National Patient Registry. Diagnoses were classified according to the disease codes provided in Supplemental material 2.
Data analysis
All analyses were carried out using SAS Guide Enterprise and R Studios.
The associations between the social variables and risk of FSD were analyzed using logistic regressions to calculate odds ratios (ORs) and 95% confidence intervals (CIs). The social variables were defined as exposures and the various FSD delimitations were the outcomes. Each social variable was analyzed separately for each measure of FSD and adjusted for age and sex.
Analyses with employment as main exposures were also adjusted for education and cohabitation, whereas models with cohabitation were adjusted for education and employment. We did not mutually adjust the analyses on education and subjective social status, as employment and cohabitation were not confounders for education. We did not mutually adjust subjective social status, as this measurement provides a more global and subjective picture, hereby substantially from the other more specific, objective, and traditional measures of social position.
A total of 837 participants were excluded based on either missing data on exposure (n = 545) or outcome (n = 319), leaving 8819 participants for analysis. The participants with missing data were older (mean age 57 years) and the percentage of women was larger (57.6%) (Supplemental material 3).
Only participants aged 30–60 years were included in analyses assessing employment. This population consisted of 5530 participants (Supplemental material 4).
A non-responder analysis was performed, assessing whether any association between register-based socioeconomic variables and hospital discharge diagnosis among non-participants and participants differed. This was done by testing for interaction between study participation and social variables using likelihood ratio test.
Results
The median age of study participants was 54 years and 54% were women. The prevalence of traditional FSD was 13.4%, whereas the prevalence of BDS was 15.6%. The participants were mostly skilled workers or had less than one year of vocational training and most rated their social position as being high (Table I).
Distribution of variables stratified by sex.
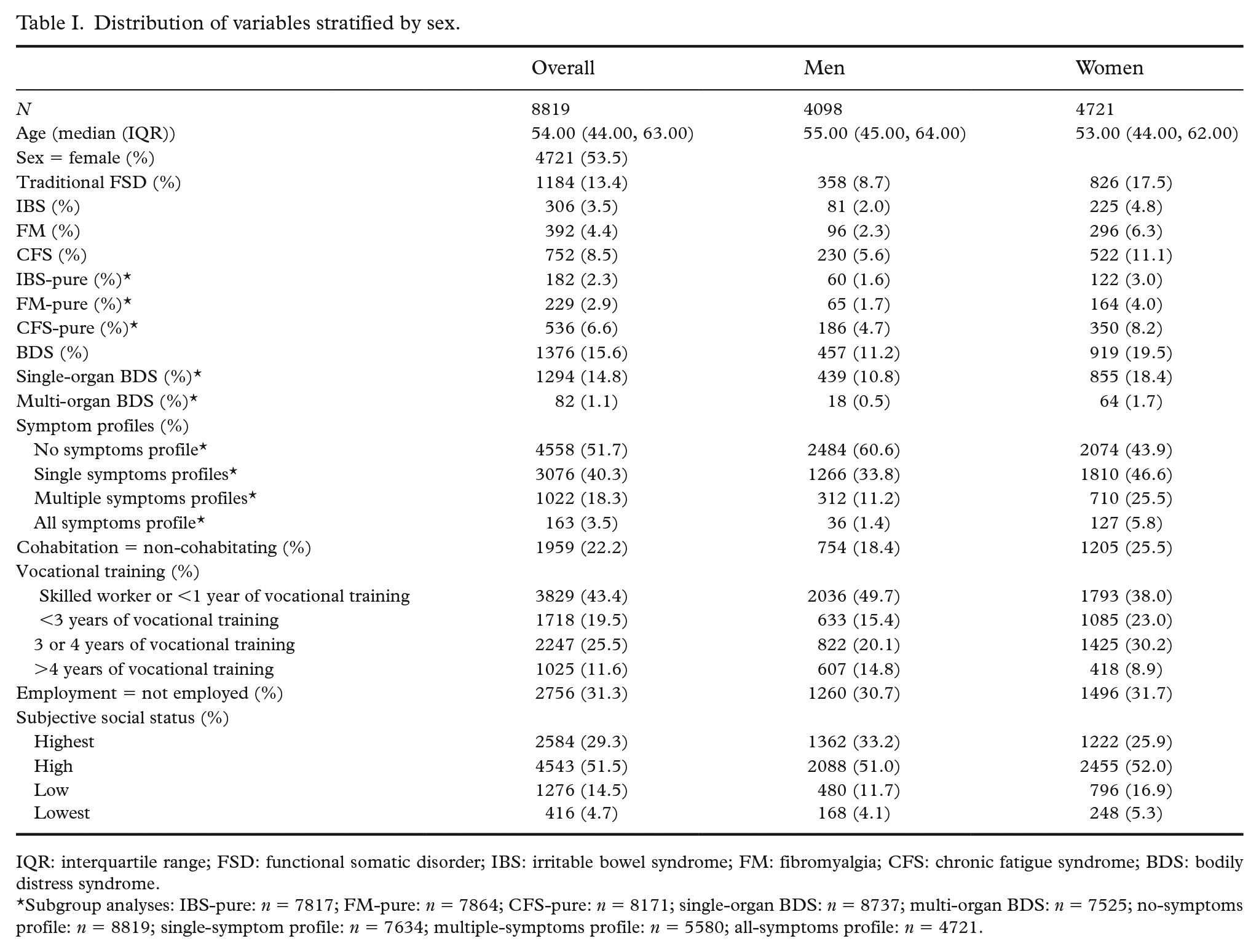
IQR: interquartile range; FSD: functional somatic disorder; IBS: irritable bowel syndrome; FM: fibromyalgia; CFS: chronic fatigue syndrome; BDS: bodily distress syndrome.
Subgroup analyses: IBS-pure: n = 7817; FM-pure: n = 7864; CFS-pure: n = 8171; single-organ BDS: n = 8737; multi-organ BDS: n = 7525; no-symptoms profile: n = 8819; single-symptom profile: n = 7634; multiple-symptoms profile: n = 5580; all-symptoms profile: n = 4721.
Traditional FSDs
Lower levels of vocational training, being unemployed, and living alone were associated with higher risk of having a traditional FSD. The associations remained after multiple adjustments (Supplemental material 5). In the associations regarding education, we used the lowest level of education as a reference and found that the strength of the associations attenuated as the education level increased. There was a negative association between subjective social status and traditional FSD (Table II).
The association (odds ratios (ORs) and 95% confidence intervals (CIs)) of social position and traditional functional somatic disorders (traditional FSS) adjusted for sex and age.
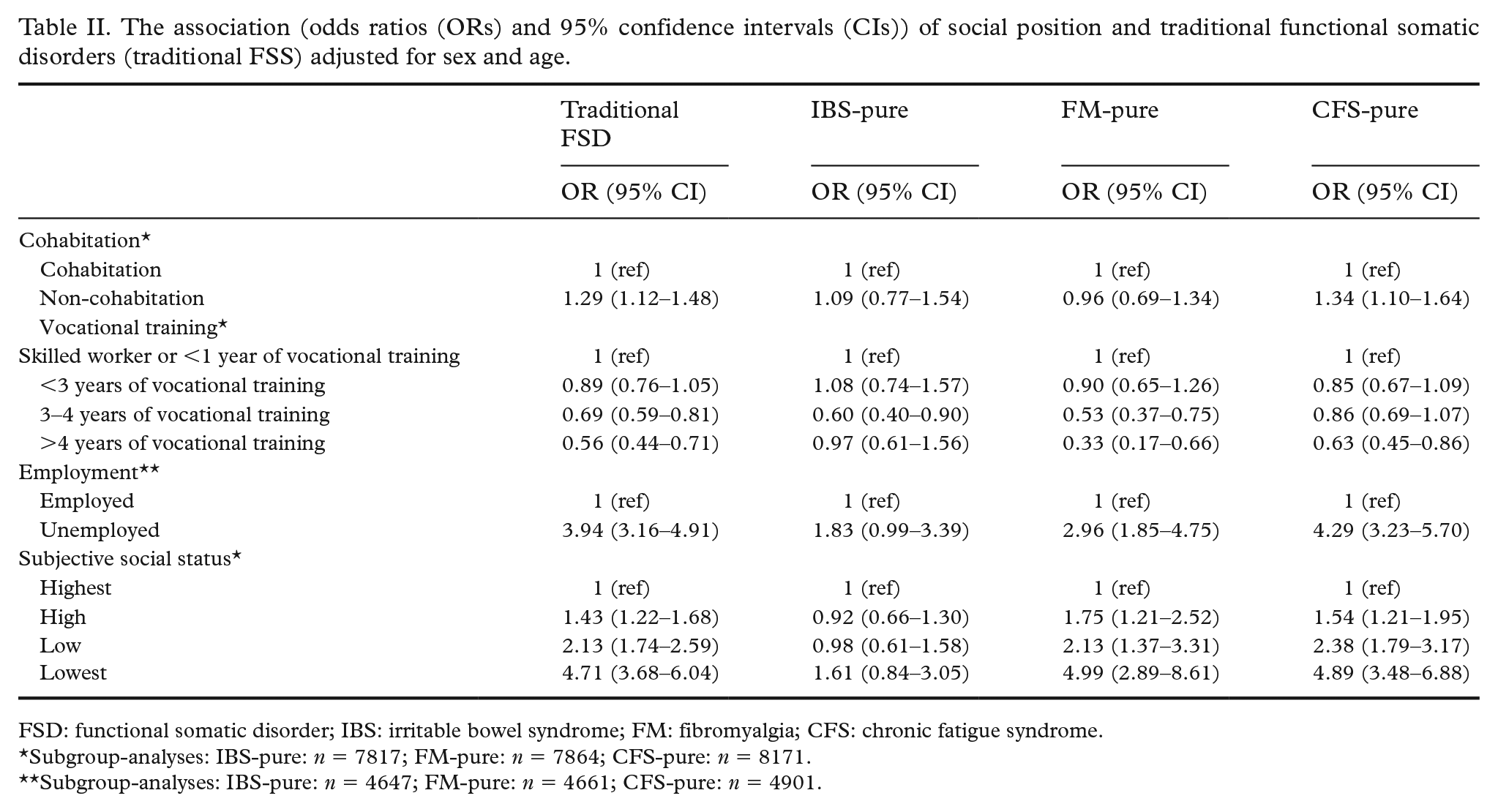
FSD: functional somatic disorder; IBS: irritable bowel syndrome; FM: fibromyalgia; CFS: chronic fatigue syndrome.
Subgroup-analyses: IBS-pure: n = 7817; FM-pure: n = 7864; CFS-pure: n = 8171.
Subgroup-analyses: IBS-pure: n = 4647; FM-pure: n = 4661; CFS-pure: n = 4901.
We saw slight differences in the associations among the FSD subtypes when looking at the ORs and CIs, with measures of social position showing a less stable association to IBS than the other subtypes. This was the case both when assessing IBS as a “pure” and a non-pure profile (Table II and Supplemental material 6).
BDS
Similar to the traditional FSD delimitation, we found lower levels of vocational training, being unemployed, and living alone to be associated with higher odds of BDS, which remained after multiple adjustment (Supplemental material 5). We also found a significant negative association between subjective social status and BDS (Table III). The associations to more severe BDS appeared stronger (Table III).
The association (odds ratios (ORs) and 95% confidence intervals (CIs)) of measures of social position with bodily distress syndrome (BDS) adjusted for sex and age.
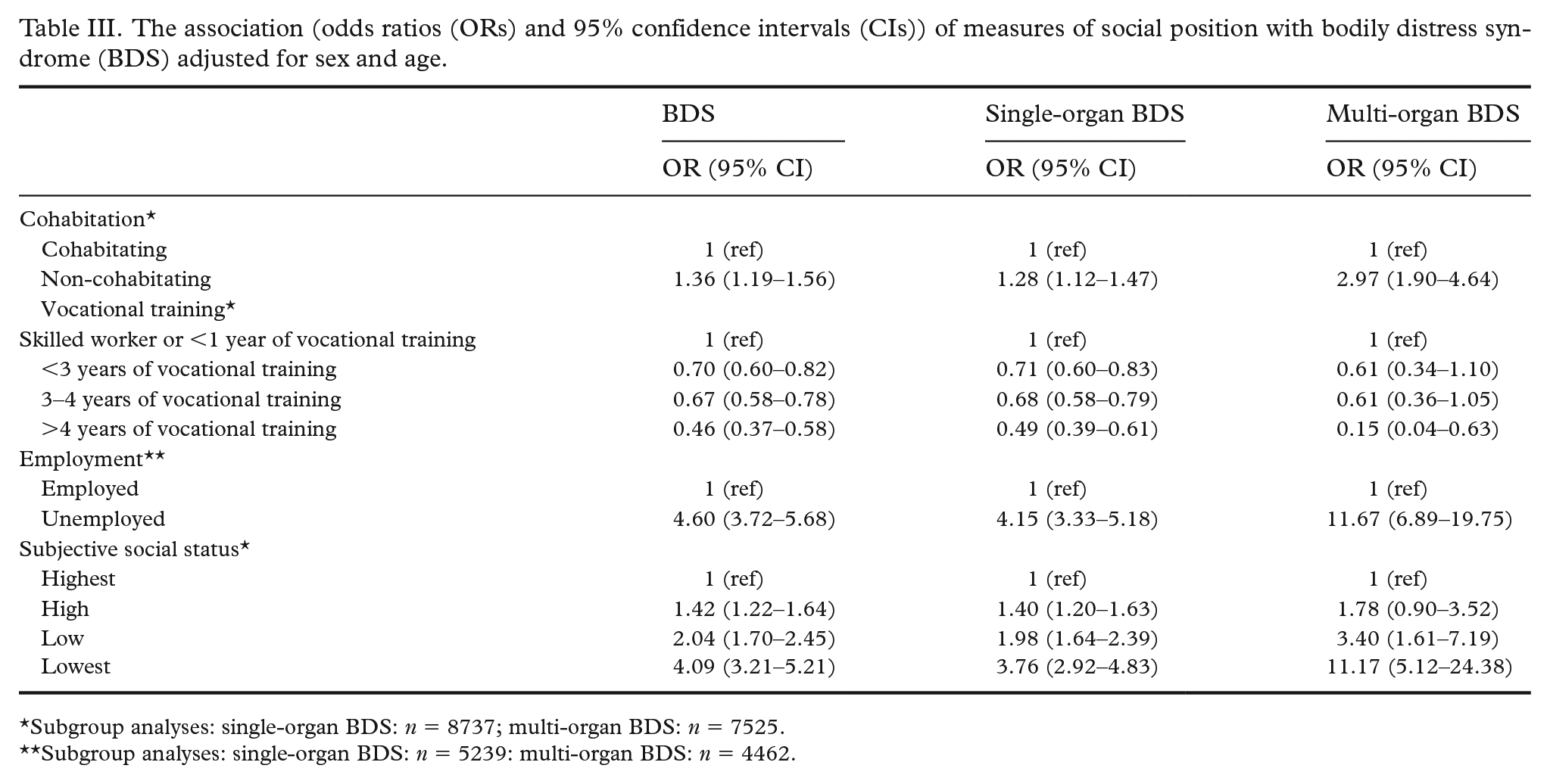
Subgroup analyses: single-organ BDS: n = 8737; multi-organ BDS: n = 7525.
Subgroup analyses: single-organ BDS: n = 5239: multi-organ BDS: n = 4462.
SPs
We found lower levels of vocational training, being unemployed, living alone, and evaluating one’s social status as lower to be associated with higher risk of SP as well (Table IV), and the associations appeared to be stronger for more severe SP.
The association (odds ratios (ORs) and 95% confidence intervals (CIs)) of social position and the symptom profiles adjusted for sex and age.
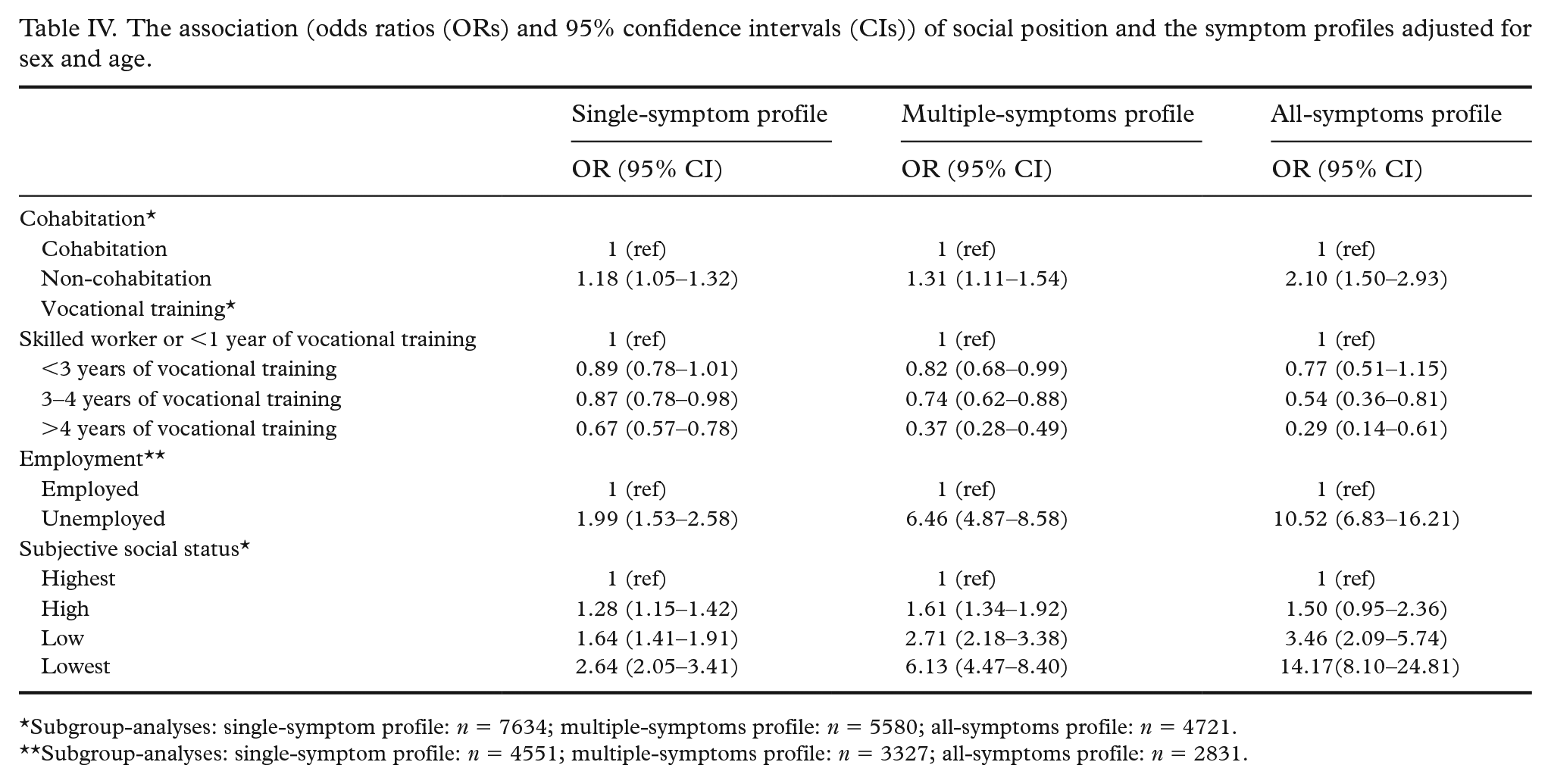
Subgroup-analyses: single-symptom profile: n = 7634; multiple-symptoms profile: n = 5580; all-symptoms profile: n = 4721.
Subgroup-analyses: single-symptom profile: n = 4551; multiple-symptoms profile: n = 3327; all-symptoms profile: n = 2831.
Non-responder analyses
The supplemental analyses comparing participants and non-participants showed that the prevalence of FSD and common mental disorders were higher among non-participants but were associated with cohabitation status and education as it were in participants (Table V). This indicates that the associations were not biased by non-participation.
The association of social position with functional somatic disorders and mental disorder in participants and non-participants.
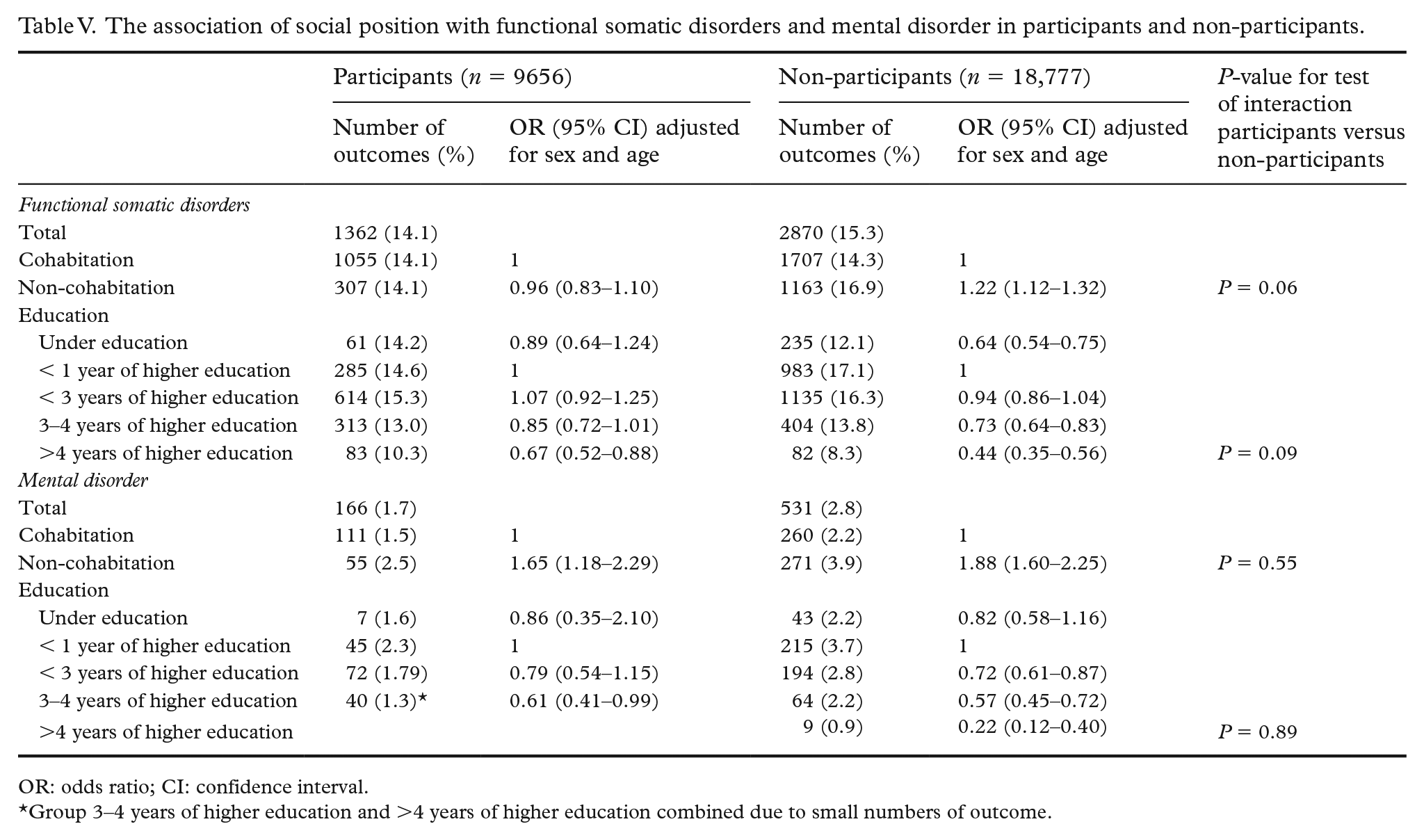
OR: odds ratio; CI: confidence interval.
Group 3–4 years of higher education and >4 years of higher education combined due to small numbers of outcome.
Discussion
In this cross-sectional study we found a consistent tendency of low social position being associated with higher risk of fulfilling criteria of FSD, regardless of the FSD delimitation.
We found lower levels of education to be associated with higher risk of FSD. Lower levels of education have also been found to predict FSD in previous studies [21], and BDS has been found to be more common in individuals having less than 10 years of education [20]. A benefit of reaching a higher level of education might be a higher ability to obtain relevant health information and engage with appropriate health services [9]. Furthermore, a higher level of education might be an indicator of growing up in a non-stressful environment. This might also decrease the vulnerability to FSD development as chronic stress has been suggested as part of the etiology in FSD [8]. Long-lasting unemployment might also result in chronic stress due to the associated financial instability. This was supported in our study, as unemployment was also independently associated with higher odds of FSD. In previous studies, individuals experiencing social strain (having financial issues and problems with housing) have been found to be 40% more likely to have CFS [18]. We also found living alone to be associated with higher risk of FSD. Cohabitation can have an impact on social position, through the increased education level and income of the household. Besides the increase in material resources, we assume that the protective effects of living together come with a higher level of social support and social network. This might result in better health behavior and coping strategies toward body symptoms.
There was a significant negative association between subjective social status and FSD. It has been suggested that the individuals’ own evaluations of social status “involve cognitive averaging of standard markers of socioeconomic position, while taking into account one’s assessment of current and future prospects” [23]. This measurement has already been found to be associated with health status [23,29]. As appraisal and expectations can be thought to affect the risk of FSD through health beliefs and illness behavior, the subjective social status measurement offers a telling perspective which makes it an interesting variable.
In the present study social position was more strongly associated with the more severe delimitations of FSD (multiple-symptoms profiles, all-symptoms profiles, and multi-organ BDS). Thus, unemployed had more than 10 times higher odds of multiorgan BDS (OR 11.67; 95% CI, 6.89–19.75), with similar results for the lowest subjective social status (OR 11.17; 95% CI, 5.12–24.38). Social position has previously been associated with the severity of FSD [17]. Our findings highlight that the individuals with severe FSD might be an especially vulnerable group. Contrary to our expectations, social position did not seem to be associated with IBS(-pure) – that is, those IBS cases with no comorbid FSD. This could, however, be explained by the fact that IBS symptoms are more manageable and, hence, not affecting social position. It should, on the other hand, be noted that the estimates were imprecise.
Strengths and limitations
The use of multiple indicators of social position and FSD delimitations is a strength of our study. Most importantly, it enables us to show a general tendency; regardless of how social position is measured and FSD is defined, lower social position appears to be associated with FSD, making the results robust and generalizable. Hereby, our results speak into the discussion on the nature of FSD.
Keeping the FSD delimitations separate enables us to investigate any potential differences in the associations depending on the definitions of social position and FSD, such as the severity of FSD.
Using a large, population-based sample is another strength. However, the participation rate was relatively low for DanFunD and differences in the responders and non-responders could be an issue leading to potential bias.
Nonetheless, an analysis based on register data indicated that although rates of especially mental disorders seem to be higher among non-participants, the ORs for the exposure-risk associations were not biased by the non-participation.
The cross-sectional nature of the study also limits the interpretation of the results. Thus, it is plausible that having an FSD might be a barrier for cohabiting, entering the work force or achieving a higher education. This is especially important in relation to our findings of a stronger association for the more severe FSD types. It is interesting that we also found associations for the less severe types of FSD, as we would expect these to be more manageable. The vocational training variable is also interesting in this perspective, as it is a measure based on performance early in life, which may introduce a time dimension to our cross-sectional study. This makes the variable less vulnerable to reverse causality. However, if FSD is founded early in life, it seems plausible that individuals with FSD, especially severe cases, are less likely to achieve a higher level of education.
In addition, our data were based on questionnaires. The delimitation of FSD thereby does not take comorbidities or differential diagnosis into account.
Lastly, we used very broad classifications for our measurements of social position, and only made simple adjustments. This increases the risk of unmeasured confounding. However, adjustments had little impact on the estimates for the individual social measures. This indicates that none of the social variables alone can explain the entire association.
Our study cannot stand alone but it is a crucial step in the understanding of the interplay between social position and FSD. With FSD prevalence of around 16% in a population-based study [6], continued research is highly important to public health.
Conclusion
In conclusion, lower social position is associated with higher risk of FSD, with the strongest associations for the more severe FSD delimitations. The mechanism behind the relations, however, is yet unknown.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948211056752 – Supplemental material for Social position and functional somatic disorders: The DanFunD study
Supplemental material, sj-docx-1-sjp-10.1177_14034948211056752 for Social position and functional somatic disorders: The DanFunD study by Signe U. Schovsbo, Thomas M. Dantoft, Betina H. Thuesen, Katja B. Leth-Møller, Lene F. Eplov, Marie W. Petersen, Torben Jørgensen and Merete Osler in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-2-sjp-10.1177_14034948211056752 – Supplemental material for Social position and functional somatic disorders: The DanFunD study
Supplemental material, sj-docx-2-sjp-10.1177_14034948211056752 for Social position and functional somatic disorders: The DanFunD study by Signe U. Schovsbo, Thomas M. Dantoft, Betina H. Thuesen, Katja B. Leth-Møller, Lene F. Eplov, Marie W. Petersen, Torben Jørgensen and Merete Osler in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-3-sjp-10.1177_14034948211056752 – Supplemental material for Social position and functional somatic disorders: The DanFunD study
Supplemental material, sj-docx-3-sjp-10.1177_14034948211056752 for Social position and functional somatic disorders: The DanFunD study by Signe U. Schovsbo, Thomas M. Dantoft, Betina H. Thuesen, Katja B. Leth-Møller, Lene F. Eplov, Marie W. Petersen, Torben Jørgensen and Merete Osler in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-4-sjp-10.1177_14034948211056752 – Supplemental material for Social position and functional somatic disorders: The DanFunD study
Supplemental material, sj-docx-4-sjp-10.1177_14034948211056752 for Social position and functional somatic disorders: The DanFunD study by Signe U. Schovsbo, Thomas M. Dantoft, Betina H. Thuesen, Katja B. Leth-Møller, Lene F. Eplov, Marie W. Petersen, Torben Jørgensen and Merete Osler in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-5-sjp-10.1177_14034948211056752 – Supplemental material for Social position and functional somatic disorders: The DanFunD study
Supplemental material, sj-docx-5-sjp-10.1177_14034948211056752 for Social position and functional somatic disorders: The DanFunD study by Signe U. Schovsbo, Thomas M. Dantoft, Betina H. Thuesen, Katja B. Leth-Møller, Lene F. Eplov, Marie W. Petersen, Torben Jørgensen and Merete Osler in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-6-sjp-10.1177_14034948211056752 – Supplemental material for Social position and functional somatic disorders: The DanFunD study
Supplemental material, sj-docx-6-sjp-10.1177_14034948211056752 for Social position and functional somatic disorders: The DanFunD study by Signe U. Schovsbo, Thomas M. Dantoft, Betina H. Thuesen, Katja B. Leth-Møller, Lene F. Eplov, Marie W. Petersen, Torben Jørgensen and Merete Osler in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
The authors would like to thank the DanFunD steering committee consisting of Professor MD DMSc Torben Jørgensen (principal investigator), MD PhD Michael Eriksen Benros, Senior Consultant MD PhD Lene Falgaard Eplov, Professor MD DMSc Per Fink, MSc PhD Susanne Brix Pedersen, Professor MD PhD Allan Linneberg, and MSc Eng. PhD Thomas Dantoft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the following Danish foundations: the Lundbeck Foundation (grant number R155-2013-14070), Trygfonden (grant number 7-11-0213), and Knud og Edith Eriksens Mindefond (case number 62786). The funding sources had no role in the conduction of the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.