
Abstract
Introduction:
It is central for public health to answer questions related to how to change health and wellbeing in populations through interdisciplinarity and health in all policies and sectors. For a school physical activity promotion initiative to be acceptable and thus feasible, the buy-in of teachers is fundamental. Therefore, school physical activity promotion should be integrated into and support teaching activities.
Aims:
We discuss the use of education outside the classroom as a feasible pedagogical approach that integrates and promotes physical activity for school children.
Methods:
We present and discuss theoretical arguments and empirical evidence to argue and illustrate that education outside the classroom is a promising approach for promoting physical activity.
Results:
Education outside the classroom is characterised by regular curriculum-based experiential teaching activities outside the classroom with the inclusion of physical activity as a means to pedagogical ends. School subjects are taught outside the classroom drawing on problem-based learning and experiential education. Here, physical activity is integrated without compromising curriculum goals which increases teacher buy-in and thereby intervention acceptability and feasibility. Empirical evidence suggests that education outside the classroom increases boys’ moderate to vigorous physical activity and girls’ light intensity physical activity. We contend that the mechanisms are a mix of place, pedagogy and pupil motivations.
Conclusions:
Introduction
Non-communicable diseases (NCDs), such as cancer, cardiovascular diseases, diabetes and chronic obstructive lung diseases, are an enormous and increasing public health challenge. Numerous studies have shown physical activity (PA) to be a factor in reducing NCD risk [1]. Accordingly, physical inactivity has been associated with a wide range of preventable NCDs [2].
More than ever, public health needs effective and integrated strategies for promoting health and PA in whole child and youth populations in their everyday life and settings. A large narrative review of 142 studies investigating the association between PA and health indicators in children and youth revealed strong evidence of a positive relationship between PA and physical health indicators, such as body composition, physical fitness and bone health [3]. Furthermore, there is some support for a positive relationship between PA and motor skill development and psychosocial health in terms of quality of life, wellbeing and reduced psychological distress [4]. Increased PA levels can therefore be expected to have a strong impact on children’s and young people’s overall health and wellbeing.
The association between PA and learning is a widely discussed topic. There is considerable evidence suggesting that PA improves cognitive function [5]. A systematic review investigating the relationships among PA, fitness, cognitive function and academic achievement concluded that although the evidence is inconsistent, the overall evidence suggests a positive association among the concepts [6]. Accordingly, another recent systematic review concluded that cardiorespiratory fitness enhances children’s academic achievement [7]. As a consequence, the evidence supporting the utility of PA to increase academic performance or learning is growing (e.g. Have et al.) [8].
The newest (draft) World Health Organization (WHO) guidelines on PA and sedentary behaviour recommend among other things that children and adolescents (aged 5–17 years) should be active at least an average of 60 minutes per day and limit sedentary time [9]. Unfortunately, PA levels among children and youth are alarmingly low. At the European level, four out of five teenagers do not move as much as recommended [10]. The International Sports and Culture Association (ISCA) describes this trend as an ‘inactivity time bomb’, as the costs for the treatment of follow-up diseases will increase significantly over the coming years [10]. In addition, girls often have a significantly lower level of PA than boys throughout their youth, and for both sexes the PA level decreases with age [11]. Early life physical inactivity has a greater negative effect on the body, as it has not yet fully developed [12], and PA behaviours tend to persist throughout the lifespan [13]. Correspondingly, the risk of NCDs gradually accumulates during the life course [12]. Recent evidence shows the importance of a life course perspective, indicating that intervention early in life has the highest impact and therefore public health potential [12].
Intervention studies have shown that addressing health determinants through socio-ecological interventions is an effective approach to increase PA levels in children (e.g. Rhodes et al.) [14]. The literature shows that prevention interventions should take into account the entire ‘life ecosystem’ of children and youth [15]. Therefore, the everyday settings and their influence on the PA of child and youth populations should be considered. This so-called settings approach is based on insights that the context affects the intervention and is in itself an influential health determinant [16]. Schools are considered an essential setting for the promotion of PA among children [17], as children spend approximately one-third of their time in school for 9 months per year and a broad demography may be obtained through schools [18]. Ambitious holistic frameworks and whole-school approaches such as health-promoting schools – based on a reciprocal relationship between health and education – have been considered best practice for the past three decades [19]. Often, such whole-school approaches build on values such as empowerment, equity, democracy and participation addressing all areas of school life and beyond with the aim of tackling the complexities of health, wellbeing and social justice within socio-ecological models. Recently, more attention has been given to policy initiatives integrating health-promoting activities into school curriculum time [20, 21].
While the health-promoting potential of schools is increasingly recognised, it is necessary to keep in mind the primary purpose of schools, namely knowledge acquisition, learning and personal growth [20]. Schools’ success is primarily evaluated by comparisons of pupils’ educational attainment and academic performance, which generates an incentive for school leaders and teachers to focus on activities that are oriented towards these goals. For a school-based PA promotion initiative to be acceptable and thus implementable, school leader and teacher buy-in is fundamental. In other words, PA interventions should at least not interfere with the primary purpose of school, and at best it should be viewed as an asset to this purpose. Further, school-based PA promotion should be considered an ‘add-in’ to teaching activities rather than an ‘add-on’ by teachers [22]. We use the term ‘add-in’ to denote health-promoting activities that become part of curriculum-based educational activities without taking time away from core curriculum obligations and time. In contrast, ‘add-on’ is used to describe activities applied on top of the core curriculum obligations as something extra during both classroom teaching and school management.
Methods
In this commentary, we discuss opportunities in the field of public health and school-based PA promotion for child and youth populations. We draw on theoretical and empirical evidence and practical experience and examples to debate and illustrate the potential for and the challenges of school-based PA promotion through the use of education outside the classroom (EOtC). We argue that EOtC is a promising approach to promote and integrate PA aimed at child and youth populations in schools in a teacher-integrated ‘add-in’ fashion at a low cost.
Our argument is divided into five parts. Firstly, we characterise EOtC and how EOtC differs from other similar school PA promotion approaches. Secondly, we describe the evidence base concerning EOtC and PA promotion and, thirdly, possible mechanisms between the practice of EOtC and PA. We then go on to discuss the practical and political implications of EOtC as school-based PA promotion. Finally, barriers and challenges for EOtC as PA promotion are discussed.
EOtC as upstream school health promotion
What is EOtC?
The concept of EOtC, or udeskole, stems from Norway but has recently gained more international attention (e.g. O’Brien and Murray) [23]. In EOtC, school subjects are taught outside the classroom in a pupil-led, teacher-facilitated way based on experiential education, in which PA is an integral part of teaching and learning activities [24]. EOtC aims to provide children with the opportunity to obtain personal and concrete learning experiences by using their bodies and senses in ‘real’ natural settings; for example, parks, or cultural settings such as museums. EOtC can take place in a variety of locations; for example, a school yard, graveyard, museum, factory, park or forest, although it is often practised in natural environments [25]. While the idea of excursions and experiential learning is not new, EOtC implies regular activities; for example, on a weekly or biweekly basis [26], and is integrated into everyday life and curriculum in practising schools.
In short, EOtC is characterised by the following:
curriculum-based teaching and learning activities outside the classroom but in school hours
setting-sensitive, problem-based, experiential education
pupil-led, teacher-facilitated learning
inclusion of PA not as a goal but as a means to pedagogical and didactical ends
regular activities on a weekly or biweekly basis.
In practice, this approach might involve mathematics lessons in which algebra and geometrical concepts are seen, felt and tested using the features of the particular setting. For younger children, this might involve counting and measuring tree trunks, and for older children perhaps weighing objects of varying densities to explore dynamics of gravity. In language or history lessons, the pupils might write poems or stories about a statue seen during a city walk. A biology class could involve looking for signs of spring in an urban park or investigating the optimal growth conditions for algae using water samples from a local pond.
A variety of school-based PA promotion initiatives exist, including PA breaks during the school day, supplementary physical education (PE) lessons, and the support of active play during recess through the provision of equipment, PA homework, or special events on weekends. EOtC has notable similarities to so-called movement integration (MI) (for a review, see Webster et al.) [21]. MI aims to infuse PA at any level of intensity into general classroom education during normal classroom time. As such, EOtC could be framed as a programme used for MI, comparable to other guides or programmes with activities integrated into academic lessons that use PA to reinforce academic content by directly linking the core curriculum and subject content to the activities. While the main goals of EOtC include embodied learning, knowledge acquisition and maintenance of school motivation, and thus not PA promotion in itself, EOtC may involve (and in practice often does involve) both active breaks, PA-intensive academic lessons and/or PA during transition periods (e.g. active transport). In other words, while MI programmes and EOtC may seem to be built on similar principles, the primary aims and modus operandi of EOtC and MI are different (please see Table I).
Education outside the classroom illustrated by contrasting aim, initiation, mechanisms, modalities and delivery with movement integration.
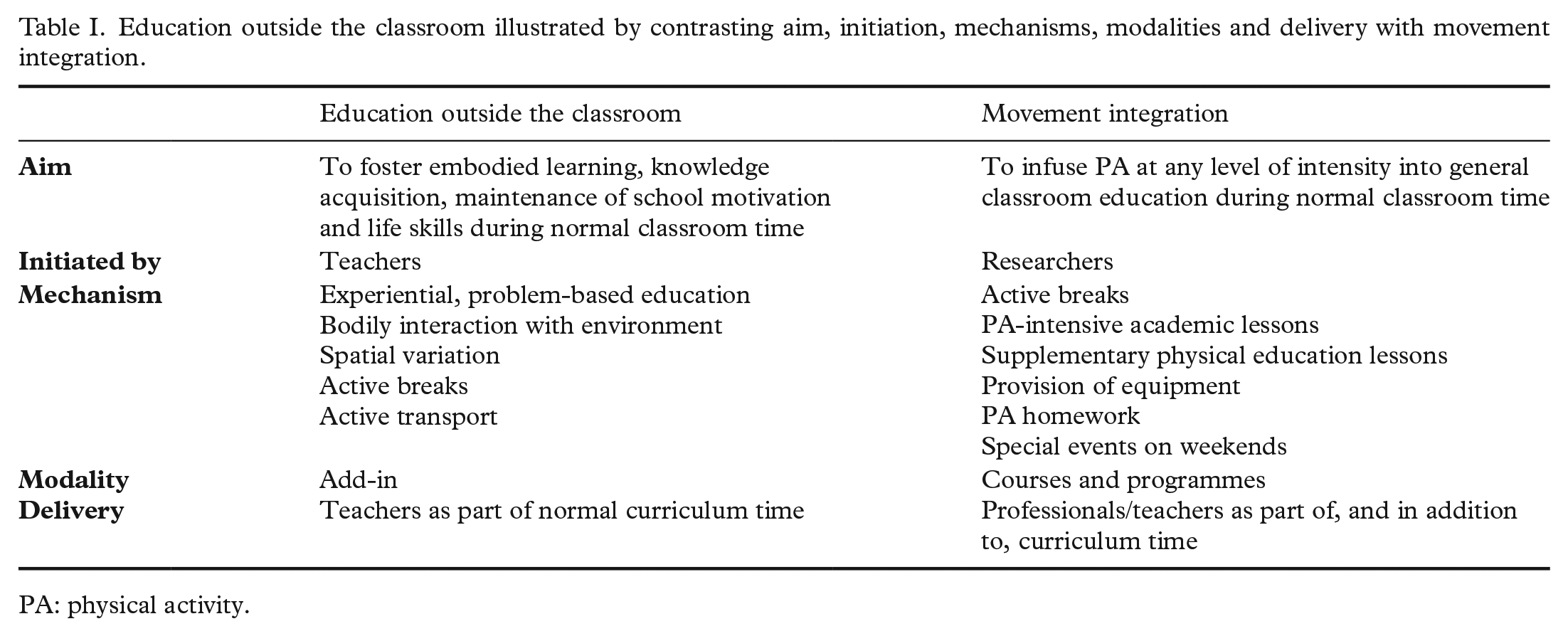
PA: physical activity.
What does the empirical body of knowledge say about EOtC and PA?
A change in location from classrooms to outside the school buildings and the use of different pedagogies may theoretically lead to more accumulation of PA in EOtC than in classroom teaching.
Case studies have indicated that Danish pupils’ mean activity levels were more than twice as high on forest days as on traditional school days, and were equal to mean activity levels on school days with two PE lessons [27]. Similar findings were observed in subsequent Norwegian and Danish studies (see Becker et al. for a review) [28].
Becker et al. [28] identified a need for studies with quasi-experimental or longitudinal designs and with a greater number of participants to confirm these tendencies further. Correspondingly, a large-scale quasi-experimental Danish study, TEACHOUT, investigated PA, wellbeing, social interaction and learning among pupils in 28 EOtC classes who participated weekly in EOtC over the course of a year and compared outcomes with 20 parallel (control) classes [26]. One sub-study by Schneller and colleagues [29] found that boys in EOtC classes spent more time each week in moderate to vigorous physical activity (MVPA) than did their comparison class counterparts, while no difference was found for girls.For girls, EOtC days were associated with more light physical activity (LPA) than were typical school days with and without PE. Boys and girls spent a higher proportion of time in MVPA and LPA, respectively, in the EOtC domain than in the classroom domain. In general, children spent lower proportions of time being inactive on EOtC days than on all other day types [29].
What are the possible mechanisms between EOtC and PA promotion?
There are many possible reasons why EOtC is associated with increased PA compared to traditional classroom-based education. The location, the pedagogy, the learning approach and the social interaction are all different. These differences may all affect both the possibilities and the motivation for PA (please see Figure 1).
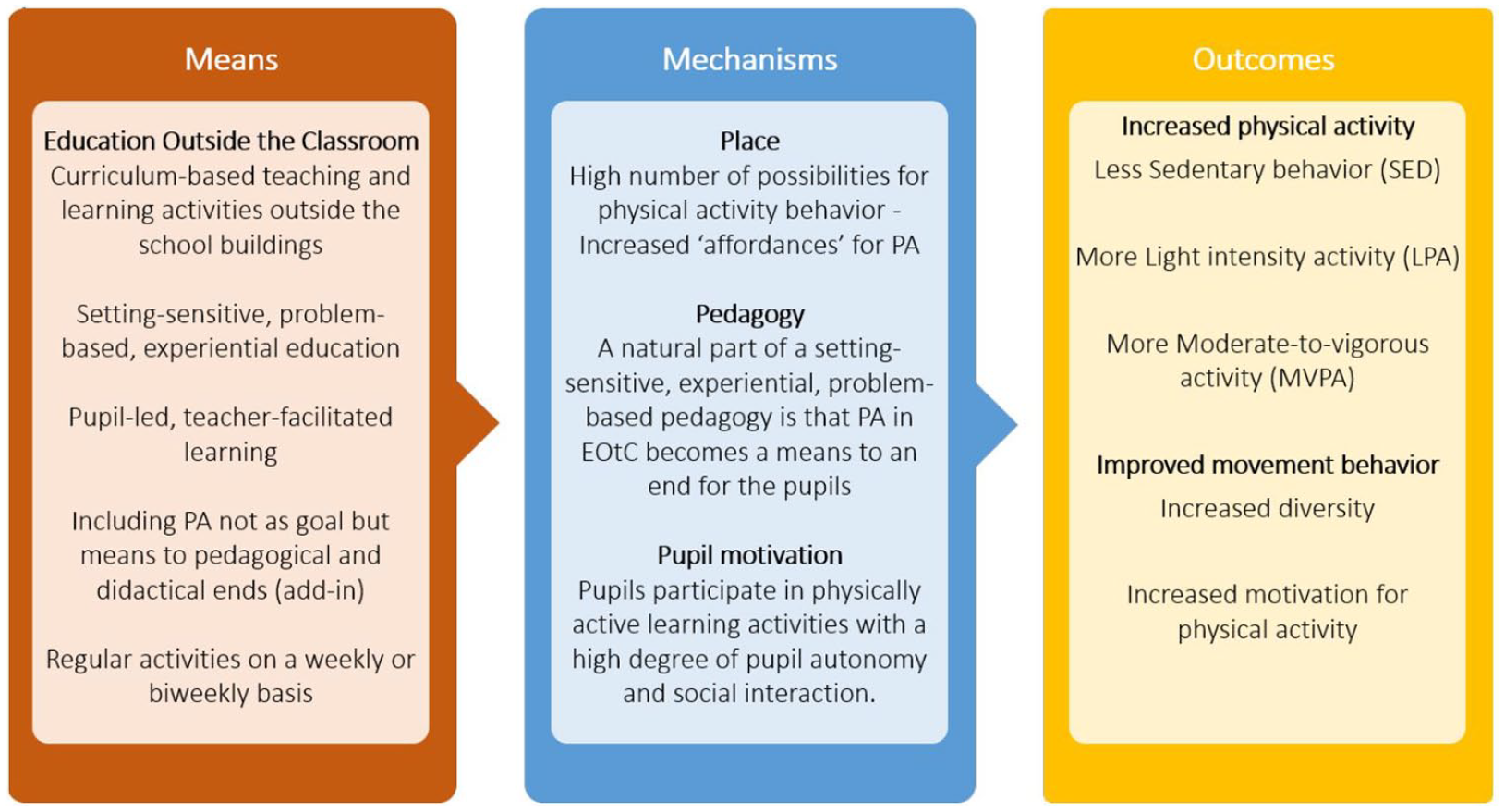
Model illustrating how education outside the classroom facilitates increased and improved movement behaviour by mediation of place, pedagogy and pupil motivation within teaching sessions in school.
The change in the physical location of the teaching activities that occur during EOtC practice results in a greatly increased number of possibilities for PA behaviour. In Scandinavia, most EOtC is practised in natural surroundings, such as parks, forests and fields, and (more infrequently) in urban and cultural settings, such as school yards, parking spaces and museums [25]. Ultimately, these are locations that are vastly more spacious and varying than the typical classroom which in itself allows, and perhaps also even stimulates, energetic (and therefore also louder) activities than would usually be feasible. Furthermore, previous studies have indicated that the actual type of location; that is, natural versus cultural environments, of the EOtC seems important for how physically active the pupils are (e.g. Mygind) [30]. In a qualitative study, Titman [31] conducted 25 focus group interviews with British children aged 5–12 years. One conclusion of the study was that children prefer nature-based settings over a built environment, and the author interpreted this preference as a consequence of increased possibilities for the children to interact with their environment [31]. Correspondingly, Fiskum and Jakobsen [32] found that outdoor education increased the variability and decreased the regulation of PA opportunities, which are the so-called ‘affordances’ for PA, as well as the opportunity to activate these affordances.
As described earlier, EOtC is characterised as a way of conducting problem-based, experiential education [24]. Central to outdoor experiential education as a pedagogical approach is the facilitation of pupils’ interaction with their physical environment and surroundings [33]. As part of a setting-sensitive, experiential, problem-based learning process, PA in EOtC often becomes a means to an end for the pupils. In other words, when practised competently by teachers, EOtC calls for bodily engagement in a way that typical classroom-based activities; for example, listening and reading and writing at a desk, do not. This might make PA meaningful, even for pupils who might dislike PA in other more sports or PE-oriented contexts.
As movement in EOtC is often characterised by being part of pupil-led problem-solving activities organised in groups, the children participate in physically active learning activities with a high degree of pupil autonomy and social interaction. As shown and described in self-determination theory and research, self-determined motivation for an activity occurs when participation in the activity produces feelings of autonomy, relatedness and competence [34]. In addition, when EOtC requires physically active transport, the level of PA undertaken by pupils in EOtC settings is, to a large degree, an autonomous choice [35]. As described, learning activities in EOtC are more often group processes than in traditional classroom teaching – a group process that might foster feelings of relatedness. Finally, it can be argued that problem-based learning may provide clear experiences of solving actual problems and hence feelings of being competent. In this way, it seems that PA taking place in an EOtC context is, to a high degree, driven by self-determined motivation, which is the kind of motivation that has been shown to be most important for the level of engagement and enjoyment of PA as well as for future engagement in PA [36]. The variety of contexts in which EOtC is practised means that the pupils engage in a wide and diverse range of movement behaviours which is beneficial for their engagement in PA activities throughout their life [37].
An additional mechanism by which EOtC affects PA is the transport that is required when travelling to the EOtC setting, which can be in close proximity to the school or further away. Transport may facilitate PA when the transportation is active (e.g. walking or cycling from the school to the place where the outdoor teaching and learning activities take place) but may also facilitate sedentary behaviour when passive forms of transport (e.g. public transportation to and from the school) are used [38].
What are the practical and political implications of EOtC as PA promotion?
When considering EOtC as PA promotion, there are several practical and political implications to consider. Here, we argue that EOtC may be effective as school-based health promotion, given the direct integration of PA with curriculum time and aims, extensive teacher acceptability, the whole-population application of EOtC and low associated costs.
Among those seeking to promote PA in education and schooling, it is becoming increasingly more accepted that integrating interventions and activities with curriculum goals and time is crucial. A key feature of EOtC is its nature of implementation in the existing educational system and teaching practices. As such, EOtC is an integrative ‘add-in’ approach: programme content and aims are delivered by the teachers as an integrated part of the existing everyday teaching practice [22]. Thus, programme outcomes can be seen as additional and simultaneous benefits to school performance and learning. For example, in EOtC, PA may not be the immediate aim of a teaching and learning session. Active transportation, walking or biking to and from the site away from the school, and the use of learning activities that require pupils to move can potentially benefit both learning and physical health. This form of ‘adding-in’ PA into children’s everyday life; that is, ‘integration within education and school systems’, is in many ways, a response to or form of the health in all policies being recommended by public health advocates globally [39].
Teachers are at the forefront of the delivery of school-based health promotion interventions, and teacher acceptability is therefore key. EOtC seems to be a particularly sustainable and effective upstream health promotion given the buy-in of teachers [40]. Historically and conceptually, EOtC differs from MI (MI aims to infuse PA at any level of intensity into general classroom education during normal classroom time; for a review see Webster et al.) [21] programmes in that EOtC is a teacher-initiated approach and is often described as a grassroots movement [24] (please see Table I). MI, on the other hand, was developed as a response to increasing sedentarism among children; it is initiated by researchers and implemented by teachers [21]. In terms of school-based interventions, teacher buy-in is central to immediate intervention feasibility and to the longer-term continuation and impact of the activities. While recent research in EOtC involves more direct researcher control to improve the quality of the evidence and implementation [26, 28], the approach remains rooted in a tradition that is teacher-generated and for which many teachers see a multitude of benefits. For example, a qualitative study found that Danish primary school teachers perceived an improvement in pupils’ academic learning and life skills through the use of EOtC [40]. These improvements were in accordance with teachers’ perceived teaching goals as well as their personal values and motivated the teachers to continue working with EOtC. In addition, there are indications from quantitative case studies that EOtC promotes children’s academic performance [28] and school motivation [41]. Furthermore, while EOtC is practised in a variety of settings, natural environments appear to be the type of location most frequently used in Denmark [25]. Exposure to natural environments is associated with improvements in cognitive measures related to academic performance, as well as a range of mental, physical and social health outcomes [42]. Correspondingly, improvements in pupils’ social and psychological wellbeing were observed in relation to EOtC [28, 43]. These added bonuses of EOtC legitimise the use of EOtC through its facilitation of the core business of the school setting, as well as holistic child wellbeing, thus bolstering the acceptability of EOtC as a school-based PA promotion approach. The influence of EOtC on academic outcomes is fundamental to the willingness of teachers, school leaders and parents to engage with EOtC. As such, these results are fundamental to the feasibility and sustainability of EOtC as a school-based PA promotion strategy.
Another characteristic and benefit of EOtC as a form of PA promotion is that EOtC, at least in Scandinavia [25], is applied broadly to child and youth populations. EOtC is a low-cost intervention, as it is delivered by ordinary teachers as part of normal curriculum time, rather than by trained specialists or researchers. As such, EOtC presents a resource-efficient, feasible and acceptable health promotion approach delivered in a universal setting dominated by the public sector. This allows for EOtC to be used widely and for children from all geographical and socioeconomic backgrounds to be reached; for example, through regulation and legislation. As a universal approach, EOtC avoids potentially counterproductive stigmatisation of vulnerable populations and invites children, who otherwise struggle to conform to typical classroom-based rules and regulations, to unfold in a different pedagogical and didactical space. Although EOtC does not specifically target vulnerable groups who are considered at risk of performing too little PA, EOtC promotes PA at a structural level to promote the PA of all children and youth, and in this way increases the number of children reaching PA guidelines and recommendations in the whole population. As such, individual-level effects may be small, because EOtC does not directly aim to promote PA, nor does it target children and youth in specific need for enhanced PA. While EOtC may not provide large effects for individuals, the impacts of universal approaches for the wider population are considerable [44]. Furthermore, evidence suggests that childhood PA tracks into later life, suggesting long-term impacts on adult generations [13].
What are the challenges and barriers to PA promotion through EOtC?
A key criticism raised towards universal approaches involves the risk of inadvertently increasing social inequality in health [45]. For example, PA promotion initiatives might cause children and youth who are already physically active to engage in more PA, but not the populations who are not sufficiently physically active. EOtC does not explicitly aim to enhance levels of PA and is not necessarily planned towards this goal. While some teachers might purposefully plan to integrate PA into their EOtC practice, others might not. It is therefore possible that accumulated levels of PA will vary by the individual teachers, contexts and groups of pupils.
While the EOtC research is currently premature as a basis for conclusions in this regard, there are some indications that call for attention and potentially action. In the above-mentioned TEACHOUT study, a significant association between regular EOtC activities and increased MVPA was found for boys, but no difference was found for girls who only displayed increased LPA [29, 46]. In other words, both boys and girls engage in more PA, but boys engage in more MVPA than girls. Girls are consistently found to engage in less PA than boys, a trend that continues over the life course. Previous research has not been based on sufficient sample sizes to allow for further subgroup analyses to be performed. However, if the gender difference in PA is indicative of a trend towards already active children accumulating more PA during EOtC and less active children accumulating less PA, actions may be required to adapt EOtC. This indicates that, although one of our main arguments for the use of EOtC is its ‘add-in’ nature, there might be a need for teachers actively to include PA in their activities to reach the group of children who do not actively seize opportunities for PA, without compromising curriculum goals. As such, teachers might need time and guidelines to help them implement activities integrating PA and teach learning objectives simultaneously. One of the ways in which EOtC promotes PA is through active transport, and this also seems to be a PA domain that effectively levels PA differences between the sexes. However, transportation to EOtC settings is sometimes performed using inactive means of transportation, such as riding on buses, due to a lack of nearby facilities. This presents a potentially costly, time-consuming and polluting barrier to PA promotion through EOtC.
At present, Scandinavian teachers receive no specific EOtC pedagogical or didactical training unless through private courses or networks. Therefore, the quality of EOtC related to the educational value as well as the level of integrated PA depends on the competence and resources of the individual teacher. This leads to variations in both educational and PA promotion outcomes. Scandinavian countries are often seen as countries of reference with regard to EOtC [47], and we therefore consider it unlikely that EOtC teacher education and teacher professional development is more progressed elsewhere. Including EOtC pedagogy and didactics in teacher education and in-service training is a necessary step towards ensuring more homogenous and high-level education and PA outcomes. Political support for EOtC teacher networks and local support staff could also increase the confidence with which teachers use EOtC and integrate PA into learning activities.
Another barrier and central stakeholder is the parents, who might be sceptical about safety or academic standards. For example, parental safety concerns have been found to restrict levels of outdoor play [48]. There is currently little research investigating if this is a barrier specifically to EOtC implementation. In a Danish case study which followed one class using EOtC over a duration of 3 years, some parents initially displayed some discomfort concerning academic standards and cold weather. These concerns were absent towards the end of the 3 years (unpublished data discussed in Mygind) [49].
Much of the evidence for EOtC as a means to promote PA discussed above stems from a high-income country context, the Scandinavian countries in particular. The Scandinavian school systems are inscribed in wealthy sociocultural contexts with strong welfare states, where almost all children attend school. In other parts of the world, where poverty and infrastructural restraints limit the opportunity for children to attend school, other issues are likely to be of greater importance for child health and education than the use of EOtC. Compared to other high-income countries, factors such as the following might contribute to important differences in EOtC implementation: the national curricula; the level of flexibility given to teachers’ choice of themes, pedagogy and methods; and the degree to which the education system is oriented towards test performance. The geographical context might likewise restrict opportunities for EOtC; for example, extreme heat or weather conditions and potentially dangerous fauna and flora in natural environments. Likewise, norms and perceptions pertaining to safety related to spending time outdoors, particularly in nature, among teachers and parents may differ across cultures and act as a barrier to implementation [50]. Hence, we acknowledge that EOtC as a form of PA promotion is currently most well established in a Scandinavian context and may provide other results in other contexts. However, we encourage exploration of the approach in other educational contexts.
Conclusion
In this paper, we have debated and argued the use of EOtC as a form of upstream PA promotion for child and youth populations in school settings. We have presented and discussed theoretical and empirical evidence for the utility of EOtC as a primarily pedagogical and didactical ‘add-in’ approach that integrates and promotes PA in schools. In EOtC, school subjects are taught outside the classroom, drawing on problem-based learning and experiential education, where PA is an integral part of teaching and learning activities. Empirical evidence suggests that EOtC increases boys’ MVPA and girls’ LPA. We contend that the mechanisms are a mix of place, pedagogy and pupil motivations; however, more research is needed to understand the pathways and mechanisms. EOtC is a promising approach to public health and PA promotion because it is integrated into children’s everyday life and settings through school curriculum time and is applied broadly to child and youth populations at a low cost. Empirical and anecdotal support for the benefits of EOtC on pupils’ school achievement, wellbeing and motivation for learning indicates acceptability in a schooling context, resulting in extensive buy-in by teachers and school leaders. Such an ‘add-in’ approach to school PA promotion provides a potential win-win approach in which both public health and education stand to gain. This intersectoral approach makes it possible to reach a wider range of schools and pupils, mobilises additional resources for PA promotion and leads to more sustainable activities. Teachers are the foundation of school-based health promotion efforts, which is a considerable advantage for EOtC as a PA promotion initiative. However, potential limitations, including how to ensure that girls are more active in the EOtC setting and how to ensure high-quality facilities for EOtC near schools, need to be addressed. Furthermore, the evidence for the effect of EOtC on school achievement, learning and wellbeing needs to be explored and confirmed by more large-scale experimental research.
Footnotes
Acknowledgements
The authors offer their warm thanks to Lawrence St Leger and Jens Aagaard-Hansen for their considered and helpful feedback on the early drafts of the manuscript. They also thank their colleagues Mikkel Bo Schneller, Mads Bølling, Camilla Roed Otte, Niels Ejbye-Ernst and Karen Barfod for collaboration on the TEACHOUT study, without which the idea and background for this debate paper would not have been conceived.
Author contributions
PB initiated the idea of a commentary. PB, LM, PE, GN and EM contributed to the content and drafted individual parts of the manuscript. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable.