
Abstract
Aim:
People may differ in their vaccine-related beliefs (i.e. efficacy, safety, purpose), with a host of factors influencing these differences. This can produce homogeneous groups of individuals who share certain beliefs, attitudes and opinions not only towards vaccines but science and medicine in general. This study aims to characterise distinct subgroups and identify ideal targets for tailored public health interventions to reinforce favourable vaccine beliefs.
Methods:
Latent class analysis was used to derive unique profiles using the 2019 Gallup survey of 140 countries. We modelled a composite of vaccine beliefs and regressed this on class membership and relevant covariates.
Results:
Patterns of item endorsement indicated a well-fitting five-class model, with classes distinguished based on whether individuals sought personal knowledge about science, medicine and health; trusted science and scientists; and reported confidence in the health care system. The lowest levels of vaccine beliefs were reported by a class lacking trust and confidence and the highest levels were reported by a class endorsing trust, confidence and desiring medical and scientific knowledge. Country-level income was moderately related to class membership, and vaccine beliefs were higher in lower-income countries.
Conclusions:
Keywords
Introduction
The development and dissemination of vaccines is considered one of the greatest public health achievements in history, saving countless lives and contributing to a marked improvement in health outcomes worldwide [1]. When properly administered, vaccines can prevent negative outcomes in the wider community, stabilise health systems, promote health equity and benefit local and national economies [2]. The advent of vaccines and vaccination campaigns has become even more evident in light of the SARS-CoV-2 pandemic, responsible for an enormous loss of lives [3,4]. Despite strong evidence regarding the efficacy of COVID-19 vaccines, one of the biggest challenges of the international COVID-19 vaccination campaign has been the presence of a relevant share of the population in many countries who did not receive the vaccine (worldwide, only 62.6% of the population has received at least one dose of a COVID-19 vaccine) [5]. No matter the amount of scientific evidence, other than supply issues [6], vaccine hesitancy is a relevant phenomenon that undermines efforts to reduce global health disparities [7,8].
Vaccine beliefs
Vaccine hesitancy or the reluctance to be vaccinated depends on many factors. Demographic and socio-economic factors include income, education and occupation [9,10]. Trust in science, scientists, biomedical research and health care providers has also been linked with vaccine hesitancy. Individuals with high trust and who view science as beneficial may value vaccines more than individuals with less favorable convictions about science. [11,12]. The quality of scientific and health information is also significantly associated with a higher vaccine uptake [13]. Trust in government is also important because studies have shown that low confidence in government authorities can be dissuasive to being vaccinated [14].
Macro-level characteristics
In addition to individual-level factors, contextual factors such as national wealth may also influence vaccine beliefs. Lane et al. reported a striking contrast in reported reasons for vaccine hesitancy among countries belonging to different income classes [15]. Lack of access to medical care can mitigate knowledge of vaccine benefits and dampen enthusiasm for obtaining advice from medical or health care providers.
Importance of the present study
Despite efforts to identify factors related to vaccine beliefs, there is a lack of consensus regarding which variables to emphasise. To date, most studies have relied on variable-centred approaches, attempting to identify at best one or two predictors that can become the focus of public health campaigns. This search for optimal predictors may be unfortunate because a person’s vaccine beliefs may involve multiple and quite different reasons, suggesting the population consists of individuals who form very unique profiles based on a multitude of factors. Such variability may create distinct ‘subgroups’ of individuals who differ, for instance, in their beliefs towards science, confidence in health care or trust in medical advice. These naturally forming and qualitatively distinct subgroups may also have different vaccine beliefs.
Aims
This study aimed to characterise distinct subgroups of individuals who may be responsive to tailored public health interventions reinforcing favourable vaccine beliefs.
Methods
Data
The 2018 Wellcome Global Monitor consists of a nationally representative survey conducted in 144 countries that involves more than 140,000 individuals. Further details on the survey’s methodology and design can be found in the Gallup technical report [16] and in the Supplemental Material. We excluded surveys from countries not included in the World Bank (WB) database and surveys where respondents reported ‘no’ to having ever heard of a vaccine. Missing data treatment is also addressed in the Supplemental Material.
Latent class analysis indicators
Latent class analysis (LCA) is a categorical analogue to factor analysis that clusters individuals into discrete ‘classes’ based on homogeneous patterning in their response profiles. These response profiles are based on ‘observed’ indicators (e.g. questions in a survey). Supplemental Table SI shows the 12 items and their response formats that were used as indicators in the LCA models. Ordinal-categorical responses were recoded so that ‘a lot’ and ‘some’ were assigned ‘1’ and the remaining response formats (‘not much’ and ‘not at all’) were assigned ‘0’. Although there are known limitations to dichotomisation when used with traditional variable-centred approaches (i.e. restricted variance and loss of power), this approach has less severe repercussions when the goal is to indicate whether an individual agrees or disagrees with a particular item.
Covariates and external markers
With the exception of age (continuous), demographic covariates were coded with the reference class ‘1’, including sex (female=1), employment status (employed=1), educational level (lower education=1), income sufficiency (sufficient=1) and urbanicity (urban=1). The WB economic classification of country-level wealth using the Gross National Income per capita index [17] was also used as a covariate.
Model testing strategy
The LCA models were tested using a three-step integrated approach with a random sample. We extracted the sample using ‘sampling without replacement’. This sampling strategy was chosen to avoid being overpowered, albeit to ensure that we had sufficient numbers to avoid sparse cells in the LCA. The precise size of the random sample (n=20,000) was based on a Monte Carlo simulation to ensure accurate parameter estimates with small standard errors and minimal bias. Data were weighted to adjust for population size differences.
In the first step, we ran a two- to eight-class model using standard inferential model fit indices to select the best fitting model. Model fit indices included the Akaike information criterion (AIC) and Bayesian information criterion (BIC), as well as changes in the log likelihood (L2) statistical fit index and entropy. We also considered evidence of latent class separation to indicate the superiority of one model over another. We used a cut-off of 0.6 for response thresholds to indicate endorsement of an indicator.
The second step involved characterising each class based on the selected covariates using univariate analysis and a multinomial logistic regression (MLR) using the most populous or distinctive class as the reference. We implemented the MLR procedure using the R3STEP procedure available in Mplus [18]. More details on these procedures are included in the supplemental material.
In the third step and using a social-psychological framework to conceptualise vaccine beliefs [19], we created a three-item composite measuring whether respondents felt vaccines were in general safe (belief), effective (belief) and important for children (attitude). Response formats ranging from 1 (‘strongly disagree’) to 5 (‘strongly agree’). We then modelled mean differences in the three-item composite based on pairwise comparisons for the obtained classes, with and without the addition of covariates and interaction terms in the model. This procedure used a weighted analysis of covariance (ANCOVA) procedure available in Stata v17 (StataCorp, College Station, TX).
Results
Sample description
A total of 131,584 survey responses were available for analysis after dropping surveys from countries not included in the WB database and eliminating surveys where respondents reported ‘No’ to having ever heard about a vaccine (n=14,338). Table I summarises characteristics of the analysis sample.
Sample characteristics.
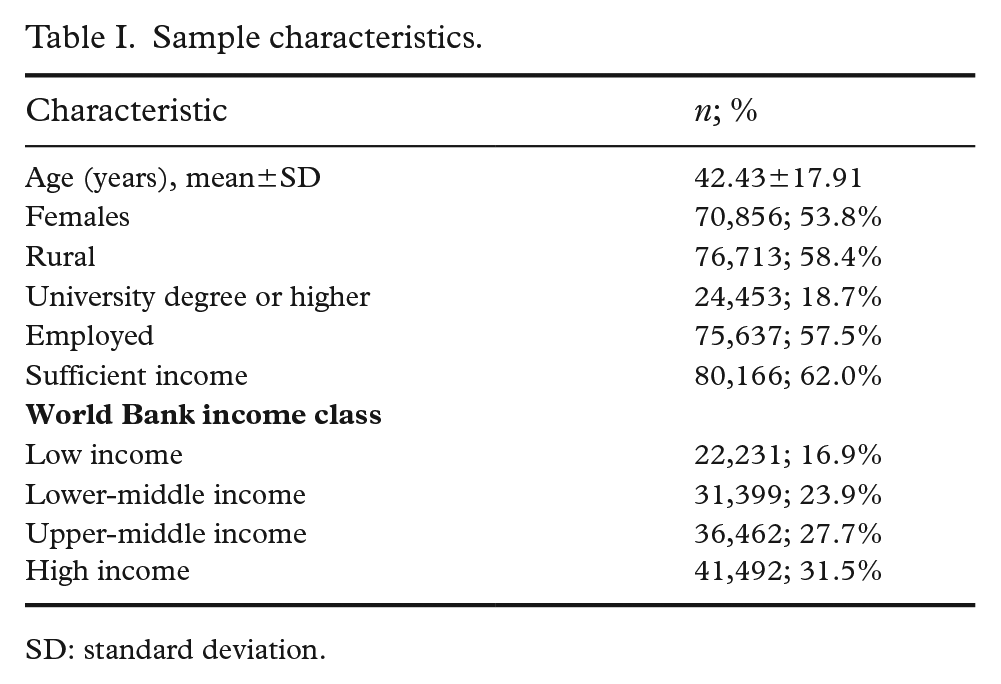
SD: standard deviation.
LCA models
Supplemental Table SII summarises the model fit indices for the two- to eight-class models. Overall, there was good fit for the five-class model. This evaluation is based on entropy (0.803; lower numbers mean poor classification), the AIC and BIC, both of which penalise models for more parameters, and substantive interpretation of the classes.
Supplemental Table SIII contains the item response probabilities for the five-class model and should be read in conjunction with Figure 1, which graphically displays a plot of the class membership profiles. Members of the first class were labelled ‘knowledge seekers, high confidence and high trust’ (latent class prevalence 19.37%, avg. ρ=0.741). Members of class 2 were labelled ‘low knowledge and information, knowledge seekers, low confidence and moderate trust’ (latent class prevalence 16.67%, avg. ρ=0.563 and 0.533 for the trust items). Members of class 3 were unlikely to endorse any of the 12 indicators above the threshold and were labelled the ‘low endorsement’ class (latent class prevalence 5.99%, avg. ρ=0.309). Members of class 4 were labelled ‘high confidence and trust in science and medical advice’ (latent class prevalence 12.92%, avg. ρ=0.579). Members of class 5 endorsed all of the indicators above the threshold and were labelled the ‘high endorsement’ class (latent class prevalence 45.06%, avg. ρ=0.904).
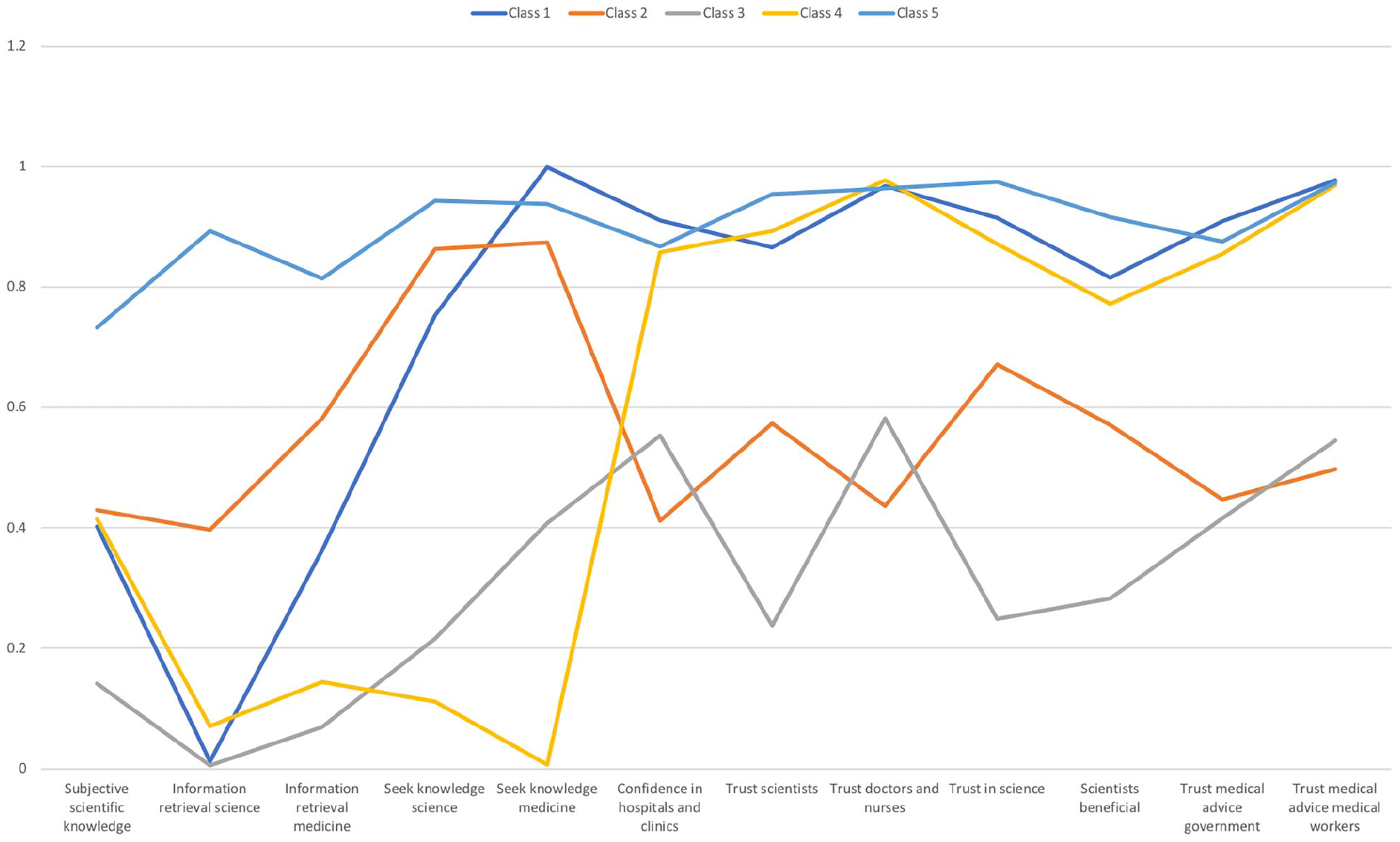
Graphical plot of the item response probabilities for the five latent classes. Unconditional item endorsement responses range from 0 to 1, with higher numbers indicating that members of a particular class were more likely to endorse the item. The pattern of item endorsement indicates the ‘composition’ of the class.
Multinomial logistic regression
There was very little evidence of multicollinearity with regard to the covariates. Table II summarises the results of predicting class membership from the full set of covariates. The bottom portion of the table, which modelled all covariates at once, indicated that members of class 1 were more likely to be older (odds ratio (OR)=1.034, 95% confidence interval (CI) 1.025–1.041), female (OR=1.416, 95% CI 1.099–1.827) and less educated (OR=3.127, 95% CI 2.135–4.578), and to reside in countries with lower aggregate wealth based on the WB index (OR=0.440, 95% CI 0.380–0.509) compared to the reference class 5. Members of class 2 were older (OR=1.017, 95% CI 1.002–1.023), less educated (OR=2.370, 95% CI 1.520–3.698) and more likely to reside in urban locales (OR=1.493, 95% CI 1.084–2.058). They reported less satisfactory income (OR=0.327, 95% CI 0.233–0.458), and they were also more likely to be from lower-earning countries (OR=0.658, 95% CI 0.551–0.785) compared to members of the reference class 5. Members of class 3 were more likely to be older (OR=1.049, 95% CI 1.037–1.060), female (OR=1.826, 95% CI 1.273–2.617), less educated (OR=6.807, 95% CI 2.512–18.459), less satisfied with their income (OR=0.421, 95% CI 0.302–0.587) and from countries with less financial means (OR=0.378, 95% CI 0.314–0.456). With the exception of sex (female) and urban locale, members of class 4 were older (OR=1.029, 95% CI 1.020–1.040) and less educated (OR=3.815, 95% CI 2.560–5.686), reported less satisfaction with their income (OR=0.696, 95% CI 0.502–0.964), were more likely to be unemployed (OR=1.603, 95% CI 1.191–2.158) and came from countries with lower aggregate wealth (OR=0.568, 95% CI 0.473–0.682) compared to members of class 5.
Results of multinomial logistic regression predicting latent class membership.
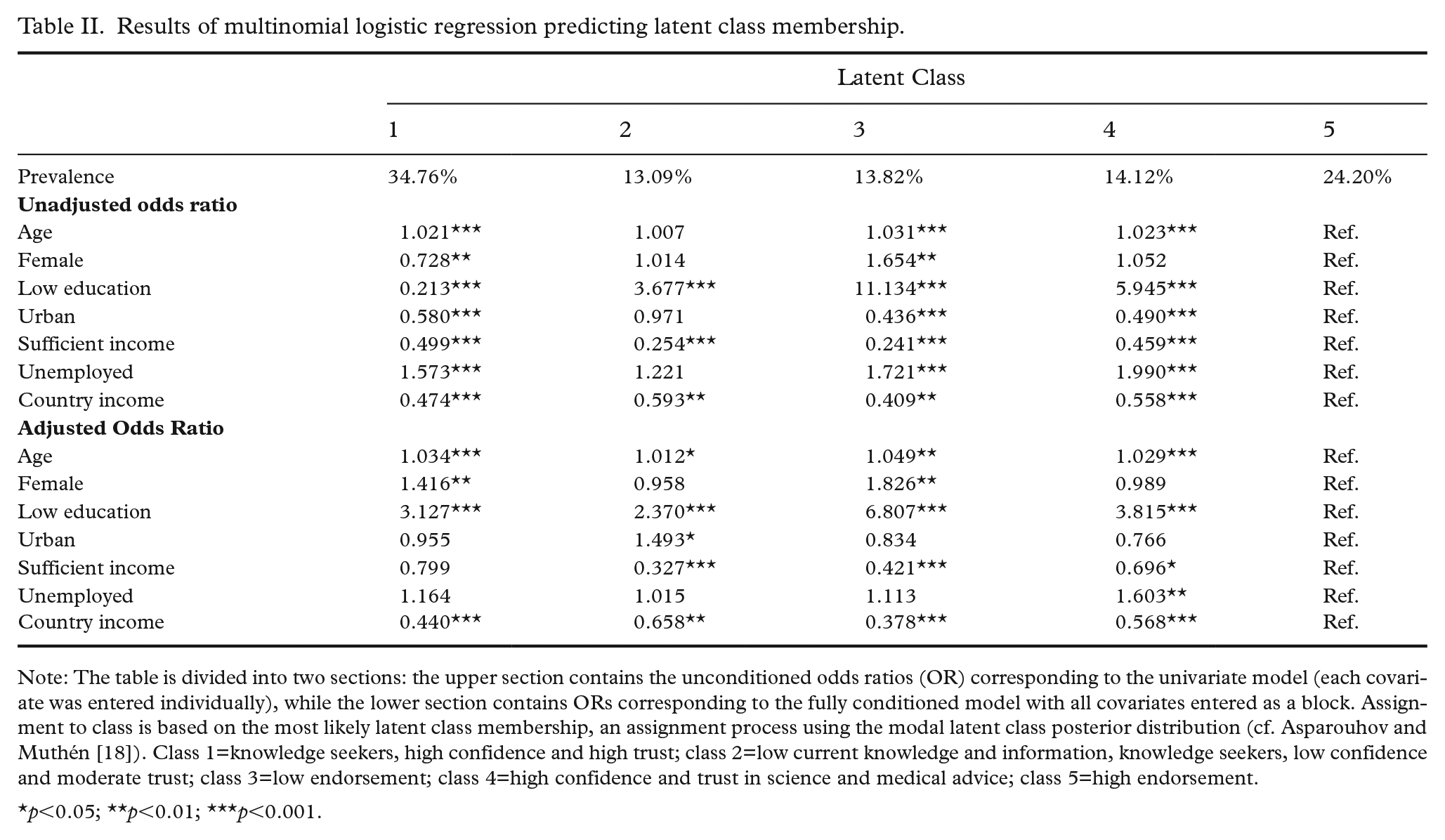
Note: The table is divided into two sections: the upper section contains the unconditioned odds ratios (OR) corresponding to the univariate model (each covariate was entered individually), while the lower section contains ORs corresponding to the fully conditioned model with all covariates entered as a block. Assignment to class is based on the most likely latent class membership, an assignment process using the modal latent class posterior distribution (cf. Asparouhov and Muthén [18]). Class 1=knowledge seekers, high confidence and high trust; class 2=low current knowledge and information, knowledge seekers, low confidence and moderate trust; class 3=low endorsement; class 4=high confidence and trust in science and medical advice; class 5=high endorsement.
p<0.05; **p<0.01; ***p<0.001.
Results of the ANCOVA with vaccine belief outcome
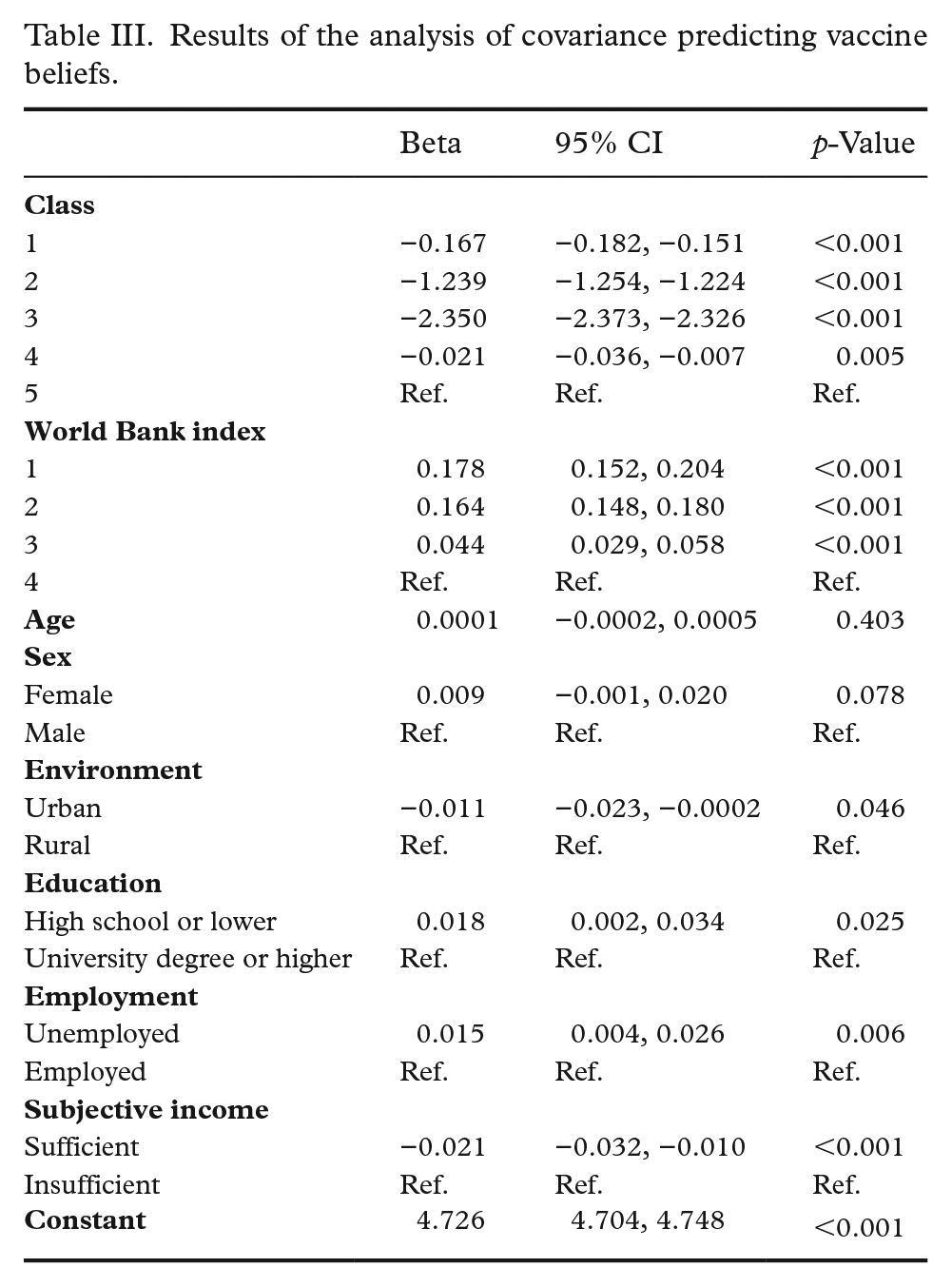
Table III shows the results of a model regressing vaccine beliefs on the full set of covariates and class membership. The regression coefficient can be interpreted as the change in vaccine beliefs for a corresponding unit change in the predictor, controlling for all other covariates in the model. Adding the covariates to the model increased the overall R2 from 76.3% to 77.2%. Levels of vaccine beliefs differed significantly between the classes (total sample mean 4.46±0.77). Class 5 (high endorsement) reported the highest levels (4.83±0.29), followed by class 4 (4.78±0.36) and class 1 (4.69±0.43). Class 3 (low endorsement) had the lowest score (2.42±0.71), with the second lowest being class 2 (3.55±0.39; p<0.001, adjusted R2=0.76). Significant mean differences in vaccine beliefs were also noted for the measure of country-level wealth (WB index). Supplemental Table SIV provides a breakdown of mean vaccine beliefs for the different WB index levels by class membership. Members of class 3 (low endorsement) consistently reporting the lowest vaccine beliefs within each WB classification, but members of the lowest income level reporting higher vaccine beliefs for all of the classes.
Results of the analysis of covariance predicting vaccine beliefs.
Discussion
In this study, using a worldwide survey, we identified five groups of individuals who could be distinguished based on whether they sought knowledge about medicine and science, had confidence in health care, trust in science and scientists and were receptive to medical and health advice from the government and health care providers. Two of the classes could be easily distinguished from the rest because they either did not endorse any of these items (low endorsement) or they endorsed all of the items (high endorsement). The remaining classes provided endorsed a mixture of the different indicators, with pronounced differences between the classes revolving around whether they endorsed seeking knowledge (class 4), having confidence in health care, feeling science is beneficial and trusting advice from medical workers and the government, all of which differentiated class 2 from the rest. The distinctions among the classes along these dimensions (particularly classes 2, 3 and 5) reinforces that not all people evaluate science, medicine and health care providers the same way and have different needs for knowledge about medicine and science. It is important to recognise that these differences can become part of the decision-making process when an individual is considering vaccination. Thus, efforts to increase vaccination rates must consider the role of cognitions and beliefs.
To illustrate the class differences further, the lowest mean levels of vaccine beliefs belonged to members of the low endorsement class and the highest levels belonged to the high endorsement class. This suggests that the belief that vaccines were effective, safe and important for children may vary principally along the lines of whether individuals desire knowledge about science and medicine, trust medicine and scientists and have confidence in health care providers. Clearly, members of the low endorsement class did not share these beliefs, whereas members of the high endorsement class were quite different not only in their beliefs towards vaccines but also on the basis of their implicit trust, confidence and desire for knowledge and information about medicine and science. For members of class 5, their trust and confidence reinforce for them the perceived efficacy of vaccines. Other studies also confirm that trust in science, the scientific community and biomedical research [11] is one of several factors that may influence a person’s willingness to be vaccinated [20]. The same goes for trust in scientists [21,22], health care providers [22,23] and health systems [23]. Unsurprisingly, this holds true for the COVID-19 vaccine as well [24,25].
In choosing to use a ‘person-centred’ approach with LCA, we were able to implicate a wider set of indicators to map distinguishing features of the classes. This stands in direct contrast to a regression-based approach, where there would be competition between indicators, resulting in only a handful of the indicators remaining as significant predictors of vaccine beliefs. The addition of covariates then refined the picture regarding class membership, indicating that in comparison to class 5, members of the remaining classes tended to be older and female, less educated, reported less sufficient income and were more likely to come from lower-income countries.
An examination of the differences in mean levels of vaccine beliefs showed that the high endorsement class had the highest levels of vaccine beliefs overall, followed by class 4, whose members endorsed all of the same indicators as class 5, with the exception of information retrieval and seeking knowledge. The lowest mean levels of vaccine beliefs were observed in the low endorsement group, and next was the class characterised as not wanting knowledge and information, having low confidence in health care and moderate trust. Covariate adjustment to the model predicting vaccine beliefs showed that aggregate country-level wealth was also a factor in determining levels of vaccine beliefs. The highest level of vaccine beliefs was observed for the low-income countries, and the observed mean differences by class remained consistent within income level. This finding is consistent with recent evidence indicating higher vaccine acceptance in lower-income countries [10,26].
Implications for public health
The information obtained from this study has several public health applications. First, public health professionals can utilise these findings to guide both the content and direction of campaigns to increase vaccination rates. For one thing, they need to be based on the beliefs that people have towards science, medicine and health care providers. In light of the different composition of the classes, there is also the consideration of targeting campaign messages so they can address not only sources of information but also building or strengthening beliefs in science and medicine. Relatedly, health care providers can work towards building greater confidence in their knowledge in an effort to build rapport with members of the communities they serve. Outreach is the first thing that comes to mind, as well as developing education programmes to build confidence in health care providers. All of these efforts can be used to forward the cause of medical providers building trust based on familiarity and exposure and through service. This can have tremendous benefits down the road, both when treating illness and in preparing individuals to make the right choices for their health and well-being.
Second, low vaccine beliefs may result from the lack of investment in health care or the lack of effort to convey the benefits of health care (and science) to the population. This would suggest that countries should invest more in dissemination, creating large-scale media campaigns that encourage greater use of health care and strengthening people’s views towards the benefits of medicine and science.
In addition, the current study provides vital support for the role of social-psychological theory in developing public health campaigns. In particular, the theory of reasoned action highlights the role of beliefs and intentions in promoting health behaviours [27]. In part, beliefs reflect the social norm (perceived prevalence), as well as the perceived behavioural ‘benefits’ of engaging in a particular behaviour. Use of this type of framework would suggest that campaigns targeting vaccines can focus on illustrating the health benefits of vaccines as well as the fact that most people do eventually get vaccinated against preventable diseases. This would then entail promoting intentions to get vaccinated, which optimally predicts the actual behaviour.
Limitations
This study has several limitations. Only 12 of the possible indicators available in the survey were used to derive class membership. Conceivably, either with a larger or even smaller pool of items, we could obtain different solutions, although using large numbers of indicators can contribute to statistical artifacts (e.g., low entropy, sparse cells and poor model fit). The class enumeration was further validated through covariate adjustments as well as significant class differences in vaccine beliefs. LCA with cross-sectional data does not permit making causal statements about ‘influence’. Rather, we can only determine associations between class membership and covariates or mean differences in vaccine beliefs.
Conclusions
The findings of this study suggest more work is needed to improve trust in science and medical providers. Such efforts can include media campaigns targeting attitudes and beliefs towards medicine and medical providers to boost confidence in the health care system. At the same time, these campaigns can reinforce the role of government and medical providers in giving medical advice and showcase how scientific research on vaccines offers protection from communicable diseases and can extend longevity. Tailored interventions grounded in community-based approaches with the collaboration of multiple stakeholders are likely to achieve greater vaccination compliance.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948221134187 – Supplemental material for Trust in science, medicine and medical providers and its relations to vaccine beliefs: A latent class analysis
Supplemental material, sj-docx-1-sjp-10.1177_14034948221134187 for Trust in science, medicine and medical providers and its relations to vaccine beliefs: A latent class analysis by Francesco Sanmarchi, Dino Gibertoni, Davide Golinelli, Davide Gori, Maria Pia Fantini and Lawrence M. Scheier in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
The authors appreciate the hard work of the Wellcome Trust to make the Gallup survey data available for public use.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.