
Abstract
Aim:
Refugees face many challenges that could lead to disparity in quality of care from the health-care system compared with native Danes. These challenges could be language barriers, cultural differences, mental health co-morbidities and socio-economic status (SES). The aim of this study was to compare the 30-day mortality of refugees and native Danes after visiting the emergency department (ED) at Aarhus University Hospital, Denmark.
Methods:
In this register-based cohort study linking clinical and socio-demographic data, we included all visits to a major Danish ED from 1 January 2016 to 31 December 2018. According to the predefined analysis plan, we present non-parametric Kaplan–Meier plots and propensity score-weighted analysis.
Results:
We included 29,257 eligible unique patients of whom 631 were refugees. In the 30-day time period after discharge from the ED, 11 deaths occurred in the group of refugees, resulting in a Kaplan–Meier estimate of 1.8% (95% confidence interval (CI) 0.7–2.8), and 1638 deaths occurred in the group of Danes, resulting in a Kaplan–Meier estimate of 5.9% (95% CI 5.6–6.1). The adjusted 30-day mortality risk difference was 1.6 percentage points (95% CI −2.0 to −1.2 percentage points) lower for refugees compared to native Danes. The 30-day mortality risk difference decreased from approximately 4 to 1.6 percentage points in the adjusted analysis. Thus, there were 16 fewer deaths among refugees within 30 days per 1000 discharged from the ED compared with native Danes when adjusting for age, sex, SES and co-morbidities.
Conclusions:
Keywords
Introduction
Immigration and the flow of refugees is not a new phenomenon. For thousands of years, circumstances such as danger of violence, lack of food and climate change have led to migration and continue to do so today. The health of refugees in the host country is influenced by a range of factors, such as potential infections by communicable diseases not normally present in the host country [1], mental health co-morbidity [2] and lower socioeconomic status (SES) compared with the host population [3]. Low SES is associated with poorer health outcomes and lower quality of health care [4,5]. However, all-cause mortality among refuges is found to be lower than in the general population [6,7] but higher than in other immigrant groups [6,8]. Non-Western immigrants’ encounters with the health-care system more often take place in emergency services compared with the general population in Denmark and several European countries [9,10]. The quality of health care provided during such encounters may differ depending on race and ethnicity [11–15], leading to increased risk of in-hospital adverse events [11,12], decreased probability of receiving guideline-based treatment [13,14] and increased 30-day readmission [15]. These disparities could potentially be explained by several factors, including language barriers [16,17], little knowledge of the health-care system and acculturation in the new host country [18]. This raises the question: Do refugees suffer from poorer health outcomes after visiting emergency services compared with the host population?
Aim
Here, we aim to describe and compare the 30-day mortality among refugees and native Danish patients after visiting the emergency department (ED).
Methods
Design, setting and participants
This was a register-based cohort study, linking clinical data from a major Danish ED with socio-demographic data from Statistics Denmark. The study took place at Aarhus University Hospital’s ED situated in Central Denmark Region with an uptake area of approximately 300,000 individuals, 48,000 patient contacts and 14,000 admissions annually [19]. The inclusion period was 1 January 2016–31 December 2018, and follow-up time was 30 days. During this period, 861–1013 refugees and 277,891–286,626 native Danes were resident in the uptake area [20]. Patients from all specialties are treated in the ED except for conditions assessed to be acute psychiatric, cardiological or paediatric (<18 years of age), who are seen at specialised acute clinics. Patients seen in the ED are either discharged after treatment or transferred to another department within 24 hours. In Denmark, all emergency health-care services are tax funded and free of charge for patients. For individuals who had visited the ED more than once during the three-year study period, only the last visit was included in the study cohort. Patients admitted due to injuries and poisoning (ICD-10 codes S00–T98) and ‘factors influencing health’ (ICD-10 codes Z00–Z99) were excluded.
Variables and data source
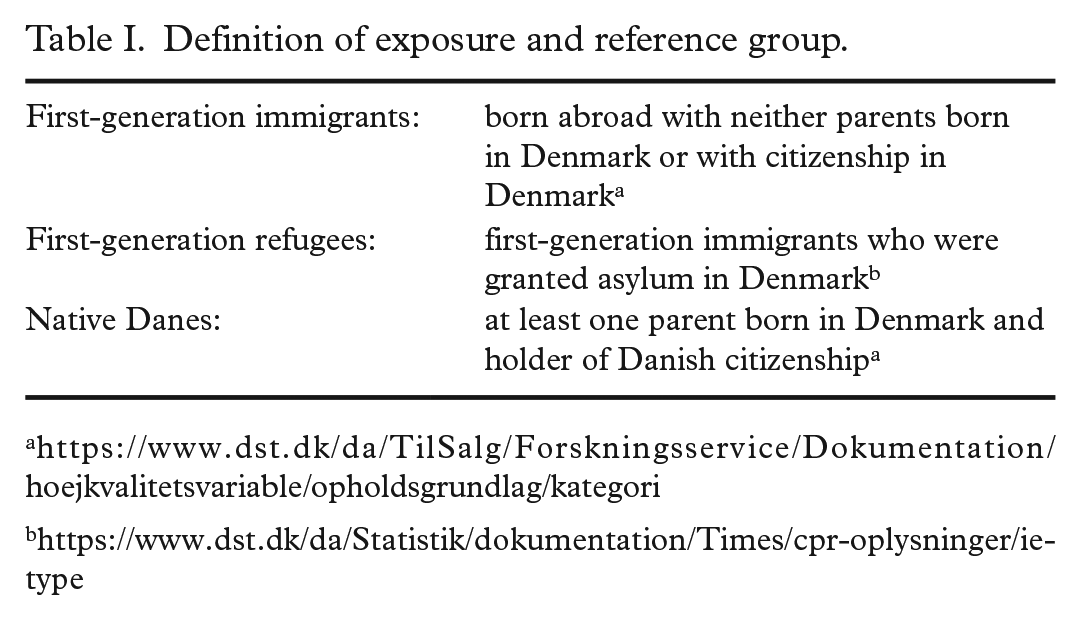
The exposure variable, first-generation refugee, was obtained from the Danish Immigration Service through Statistics Denmark. Distinguishing between first-generation refugees and native Danes was based on Statistics Denmark’s definition (Table I).
Definition of exposure and reference group.
The outcome variable, 30-day mortality after discharge from the ED, was computed from data on date of death retrieved from the Danish civil registration system; date of discharge was retrieved from the electronic medical record system.
Socio-demographic covariates were retrieved from the civil registration system and included age, sex, date of emigration, country of origin, SES and immigration date, the latter three through Statistics Denmark. Clinical data were retrieved from the electronic medical record system and included chronic diseases, discharge diagnosis, triage score, date of contact and discharge from the ED. Age-adjusted Charlson Comorbidity Index (CCIa) [21] was used to score patients’ co-morbidity using 17 diagnoses, giving a maximum index score of 29 (indicating a very large burden of co-morbidity) [22–24]; one additional point was added to the index score for each decade over 40 years [21]. To account for chronic psychiatric diseases (a mental, behavioural or emotional disorder resulting in serious functional impairment) [25], we defined a Serious Mental Illness (SMI) scale by including one point for any of the following ICD diagnoses: F10–19 substance abuse, F20 schizophrenia, F21–29 schizophrenia-like psychoses, F30–39 mood/affective disorder, F43.1 PTSD and F50 anorexia nervosa. The diagnoses were selected based on other studies [26,27]. For both CCIa and SMI, the diagnosis on discharge and any registered chronic diagnosis were used. The triage score was composed of patients’ vital parameters, with 0 indicating normal vital parameters and >5 indicating critical vital parameters [28]. In the exploratory analysis, countries were grouped geographical by World Health Organization regions (Supplemental Table SI). Statistics Denmark classifies SES into 22 groups, primarily based on source of income and/or occupation [29]. To avoid groups with very few individuals, SES was grouped into three categories: in labour market, outside labour market and in education (Supplemental Table SII). For refugees, time at risk was equal to the time in Denmark from immigration date to discharge from the ED, and for native Danes, it was equal to time from turning 18 years of age until discharge from the ED. If a person immigrated more than once, the first immigration date was used. All variables were linked using the civil registration number assigned to all Danish citizens.
Statistical analysis
As defined a priori in the analysis plan (Supplemental Material), 30-day all-cause mortality after discharge from the ED was estimated using Kaplan–Meier survival analysis stratified by refugees and native Danes, with the timescale being days since discharge and the event being death. The analysis of interest was a propensity score-weighted (PS-weighted) logistic regression to estimate the risk difference of death within 30 days after discharge from the ED comparing refugees and native Danes. The PS-weights were performed with native Danes defined as the standard population (standardised mortality ratio weighting), and extreme weights were handled by truncation. Potential confounders were identified after thorough discussions, illustrated in the Directed Acyclic Graph (Supplemental Figure S1), and relevant variables were finally agreed upon by all authors. Three complexities of PS models were defined depending on the variables included (each model and its variables are stated in Table II with more details in the Supplemental Material). For each complexity, the absolute mean difference between exposure groups was plotted for each variable with truncation of extreme weights at 0 and at the 100th percentile, at the 1st and 99th percentiles and at the 5th and 95th percentiles (Supplemental Figure S2). The least complex model with the least truncation, where the absolute mean difference for all variables was ⩽10%, was used. Continuous variables were modelled with restricted cubic spline, and categorical variables were entered unchanged (see Supplemental Material for more details). To secure participants’ anonymity, this study used pseudo percentiles, pseudo median and pseudo interquartile range (IQR). Thus, we used the average of the five closest values to the percentile, median and the IQR. Likewise, strata containing values with fewer than five values for either group were replaced with the average of that variable (to maintain the anonymity of patients). A sensitivity analysis was carried out, testing the sensitivity of the results for other plausible regression models. This was done by using a PS-weighted logistic regression analysis that only included age and sex. The statistical software program R was used for data analysis (The R Foundation for Statistical Computing, Version 3.6.3-4.1.1, Vienna, Austria). The R packages survival and survminer were used to create a Kaplan–Meier plot, and the WeightIt R package was used for estimating the PS-weights. The R package tidyverse was used for data wrangling. The R code is available from GitHub [30].
Propensity score weighting models.
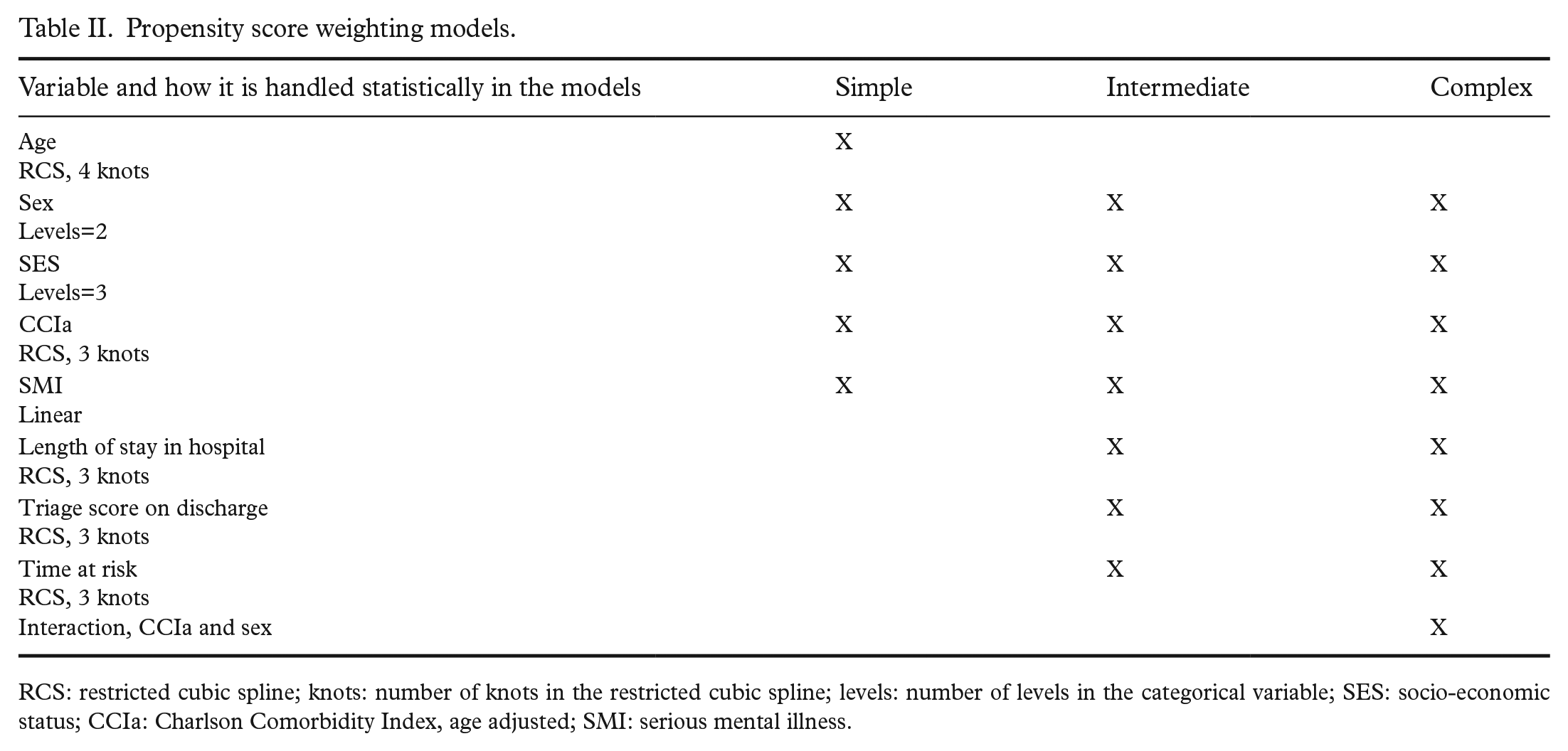
RCS: restricted cubic spline; knots: number of knots in the restricted cubic spline; levels: number of levels in the categorical variable; SES: socio-economic status; CCIa: Charlson Comorbidity Index, age adjusted; SMI: serious mental illness.
Results
A total of 173,719 patients visited the ED in the study period. Of these, 29,257 unique patients met the inclusion criteria, of whom 631 (2%) were refugees and 28,626 (98%) were native Danes (Figure 1). Table III shows the characteristics of the cohort. Further details on the distribution of country of origin (Supplemental Table SI) and SES (Supplemental Table SII) are given in the Supplemental Material. The median time in Denmark was 14 years (IQR 4–18 years). Refugees were much younger than native Danes (refugees 40 years of age, IQR 30–55 years; native Danes 61 years of age, IQR 40–75 years), which also contributed in the CCIa distribution (refugees: 11.9%; native Danes: 37.4%), and the sex distribution was almost similar. Refugees were overrepresented in the SES category ‘outside labour market’ (78%) compared with native Danes (57%; Table III). Within the study period, 11 refugees and 1638 native Danes died during the 30 days after discharge from the ED, and the Kaplan–Meier estimate was 1.8% (95% confidence interval (CI) 0.7–2.8) for refugees and 5.9% (95% CI 5.6–6.1) for native Danes (Figure 2). No refugees were censored during the follow-up period; 37 native Danes were censored, recorded as emigrated in the 30-day time period after visiting the ED. The 11 refugees who died were from the Eastern Mediterranean region.
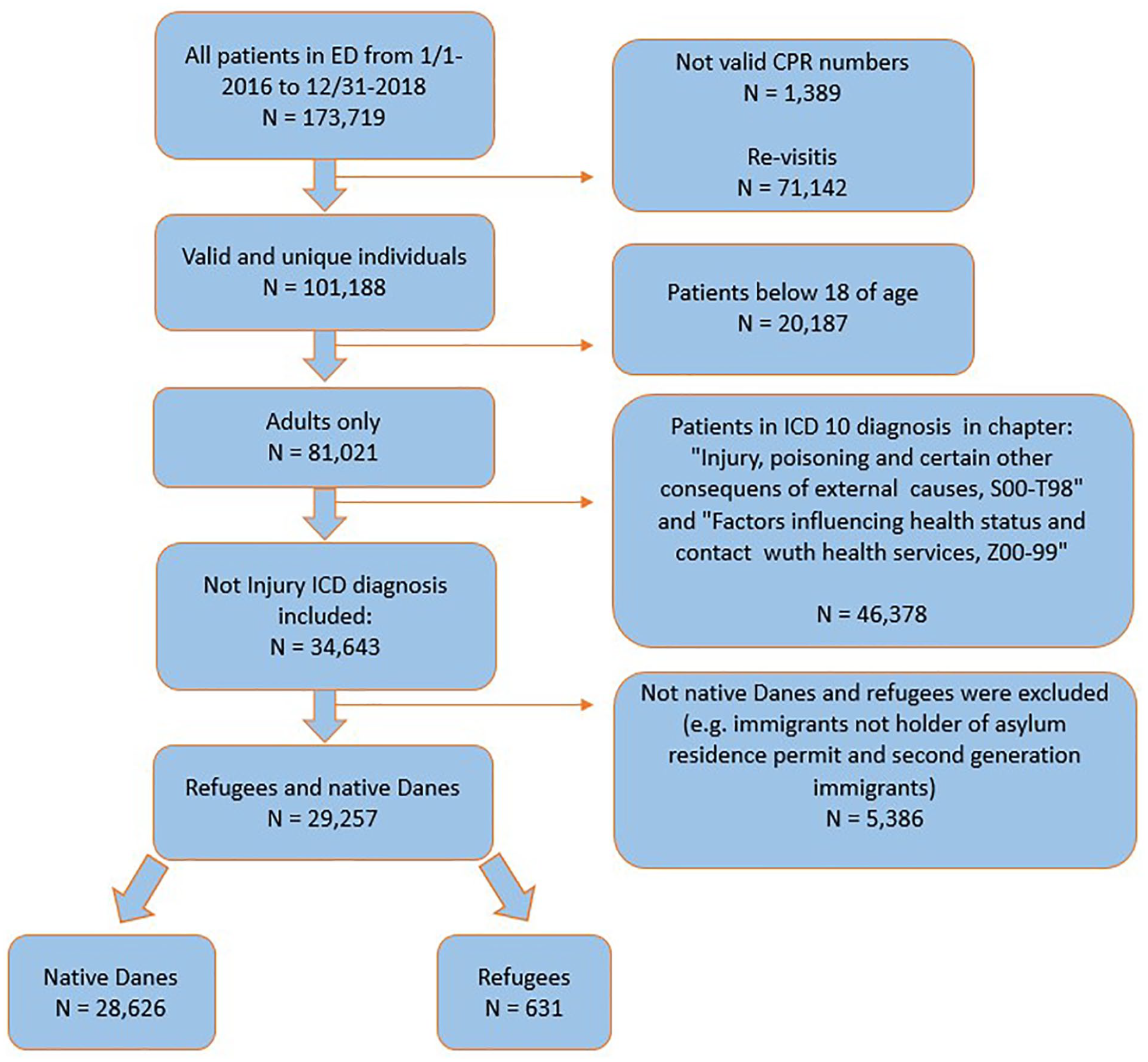
Flow chart of study population.
Characteristics of the study populations.
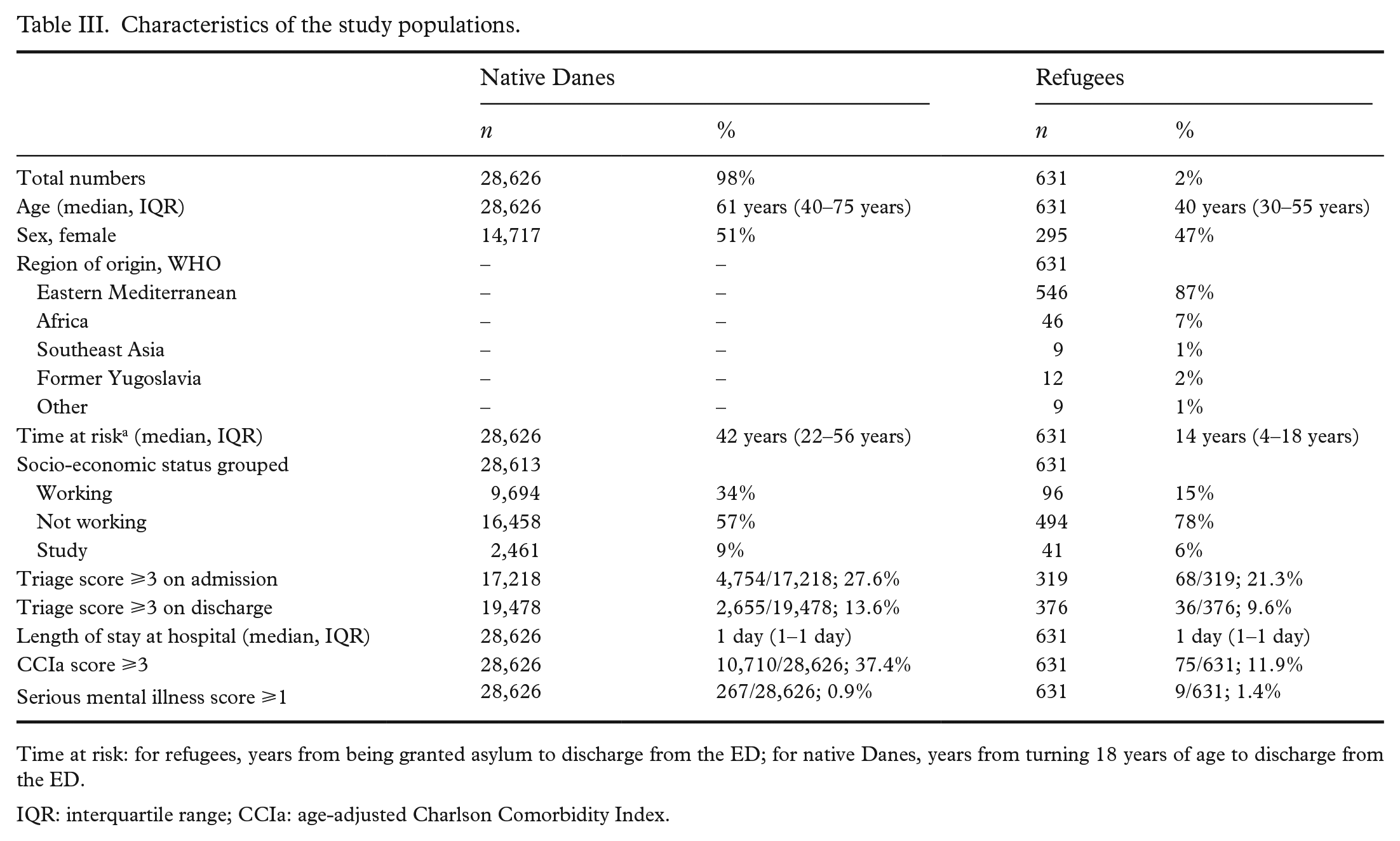
Time at risk: for refugees, years from being granted asylum to discharge from the ED; for native Danes, years from turning 18 years of age to discharge from the ED.
IQR: interquartile range; CCIa: age-adjusted Charlson Comorbidity Index.
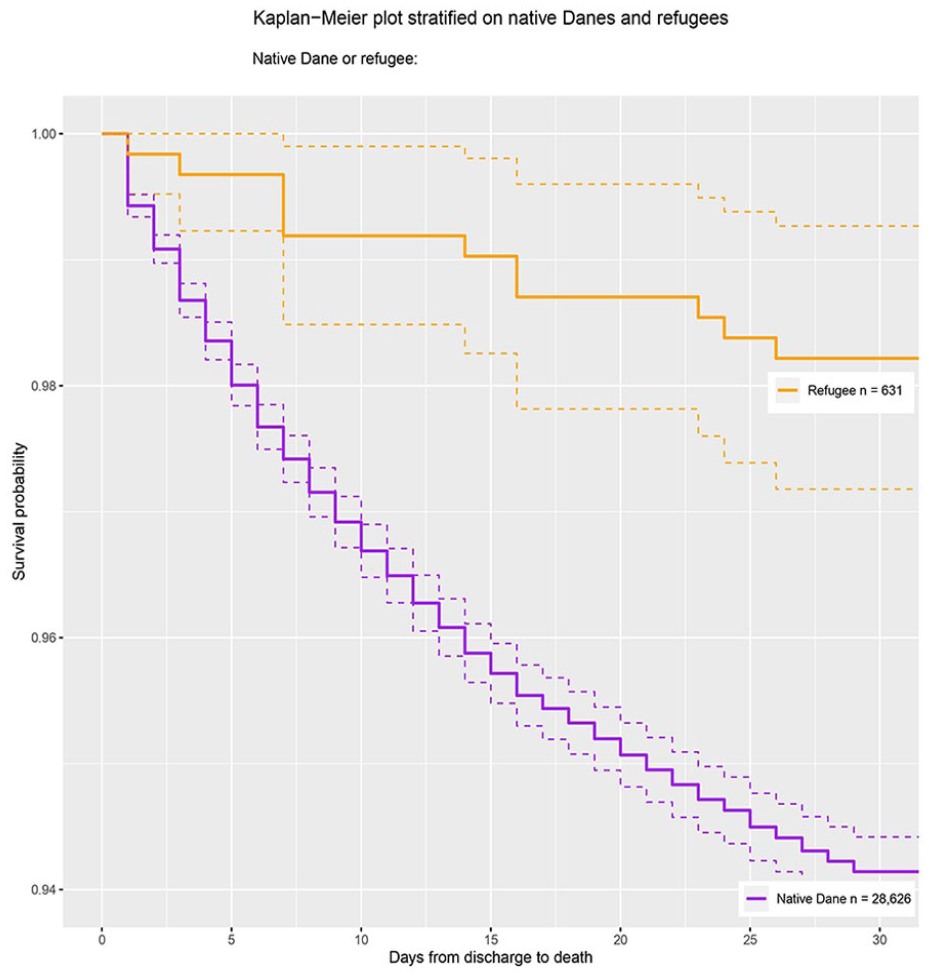
Kaplan–Meier plot showing 30-day mortality of refugees and native Dane safter discharge from Aarhus University Hospital emergency department.
The ‘simple’ PS model with 0.1 and 0.99 percentile truncation obtained balance on all variables and was chosen as the model in the logistic regression, thus including age, sex, SES, CCIa and SMI. The PS-weighted logistic regression analysis showed a 30-day mortality risk difference of −1.6 percentage points (95% CI −2.0 to −1.2 percentage points), native Danes being the standard population. In the sensitivity analysis, only including age and sex in the PS-weighted analysis increased the estimate to −1.1 percentage points (95% CI −1.4 to −0.7).
Triage score had the highest frequency of missing values, both for refugees (triage score on discharge 45%) and native Danes (triage score on discharge 37%). Missing values in all other variables varied from 0% to 2% (Supplemental Table SIII).
Discussion
Key results
The unadjusted 30-day mortality estimates were 1.8% for refugees and 5.9% for native Danes. This approximately 4 percentage point risk difference decreased to 1.6 percentage points after adjusting for confounding. Thus, per 100 discharged patients from the ED, there would be 1.6 fewer deaths among refugees within 30 days compared with native Danes.
Strengths and limitations
One of the major strengths of this study is that it is based on the highly complete and valid registers in Denmark, which made it possible to create a large cohort and to identify refugees as a subgroup of migrants. The major benefit of subgrouping refugees is to create a less heterogeneous population compared to generalising all types of migrants. Refugees have all fled from unsafe conditions and may be assumed to have more comparable migration experiences between them compared with other migrant groups such as study migrants – factors which affect health and which are therefore relevant to keep in mind when studying migrant health. It would have been desirable to have even more subgroups (e.g. concerning country of origin, proficiency in the Danish language, usage of interpreters, religion and initial diagnosis in the ED). However, this was not possible due to relatively small number of events within 30 days and no recorded information of these categorical variables (e.g. language skills).
‘Refugee’ as exposure did not include asylum seekers or undocumented refugees, which would be relevant populations to include because their challenges are similar to those of refugees. However, data on these populations are difficult to obtain due to a lack of registration in the Danish civil registration system. Bias could have been introduced by unregistered emigration and death abroad in the 30-day period after discharge from the ED. If so, we expect this happened predominantly in the refugee population, resulting in an underestimation of the mortality risk difference. Registered emigration was low (refugees 0%; native Danes 0.1%), and we do not expect it to have affected the results.
A strength was the low fraction of missing values in the variables included in the PS-weighted logistic regression analysis (age 0%; sex 0%; SES refugees 0%, native Danes <1%; CCIa 0%; SMI 0%).
Interpretation
The decreased mortality risk of refugees in this study might seem surprising when considering refugees’ language barrier [16,17], acculturation process [18] and the existing literature on differences in quality of health care when comparing race and ethnicity [11–14,31].
There are most likely multiple reasons for the decreased 30-day mortality among refugees after admission to the ED. First, it could be that refugees are less ill when admitted to the ED. Native Danes are scored as being slightly more ill on admission compared to refugees (a triage score ⩾3 on admission of 27.6% among native Danes and 21.3% among refugees). Furthermore, the triage score on admission was the variable with the highest reported missing values and the largest difference of missing between the two groups (refugees 43%; native Danes 34%). Missing a triage score may indicate that the patient’s illness was not severe enough to be scored, even though this is not in accordance with clinical guidelines. The second reason for the decreased 30-day mortality among refugees could be existing residual confounding. Refugees in the ED were around 20 years younger than native Danes. Even though age was included in the adjusted analysis, we cannot rule out that all of its effect has been removed and that it is the young age of refugees being reflected in the decreased mortality reported in our main result. Third, this study points to refugees using the health-care system differently. In accordance with the existing literature [9,10], this study indicates that refugees used emergency services more than the general population did: more than half of the refugee population situated in Aarhus in the study period sought treatment in the ED compared to around 1 in 10 native Danes. A possible explanation could be that language and cultural barriers, lack of information on refugees’ medical history and differences in health literacy might turn into fear of missing a severe health condition, leading to refugee patients being admitted more frequently than native Danes.
The adjusted model is an attempt to isolate the effect of being a refugee. This model showed a decreased risk difference in 30-day mortality, meaning that when a refugee population has the same age, sex, SES and co-morbidity distribution as the general population in the host country, the effect of being refugee on 30-day mortality decreases. However, it is doubtful if the refugee population will ever have such a distribution in the real world. This raises the question of whether the unadjusted estimate is more relevant, since the unadjusted estimate gives the 30-day mortality difference in the actual population. We acknowledge that this feat is vulnerable to residual confounding, lacking information on all parameters needed to isolate the effect of being a refugee and other limitations described above [32].
Generalisability
Due to differences in the composition of the refugee population over time and across different host countries, it can be difficult to generalise studies on refugee health. Across Denmark, there are only minor changes in the composition and origin of refugees and no major differences in structure of the EDs. Studies assessing 30-day mortality in the general population in Denmark after discharge from the ED showed similar patient age and 30-day mortality [33,34] as the native Danes in this study. Thus, we believe our results can be generalised to at least Danish EDs and countries with comparable health-care systems and population composition.
Further research
Further research is needed to explore if the slightly decreased mortality risk for refugees is also found when adjusting for diseases and the role of health-care utilisation. To study other research questions of interest such as how health is affected by migration status in general, migrant groups such as labour and study migrants and reunified families could be compared with refugees.
Conclusions
The risk of death within 30 days after visiting the ED was 1.8% for refugees and 5.9% for native Danes, suggesting that being a refugee was associated with a lower risk of 30-day mortality after visiting an ED. The estimate of the main analysis also suggests that refugees have a lower mortality than native Danes. Thus, for every 1000 refugees treated and discharged from the ED, 16 fewer will die in a 30-day time period compared with 1000 native Danes of the same age, sex, SES, CCIa and SMI distribution. In conclusion, this result supports that refugees do not suffer from decreased quality of health care compared to native Danes in the ED in terms of survival. Even though refugees potentially face many challenges in accessing the health-care system and with their general health, these challenges do not increase mortality when admitted to the ED.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948231158847 – Supplemental material for Is being a refugee associated with increased 30-day mortality after visiting the emergency department? A register-based cohort study using Danish data
Supplemental material, sj-docx-1-sjp-10.1177_14034948231158847 for Is being a refugee associated with increased 30-day mortality after visiting the emergency department? A register-based cohort study using Danish data by Signe F. Storgaard, Christian Wejse, Jane Agergaard and Andreas H. Eiset in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank the reviewers for improving this manuscript. We also thank Jacob Dvinge Redder, who was a great support and help in understanding and working with the clinical data from the ED. We also thank Joseph Lee Rodgers, who was a great help when editing the manuscript in terms of both the content and the English language.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Aarhus University Research Foundation (30714- 26101) and Tømmerhandler Johannes Fogs Fonden.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.