
Abstract
Aims:
This study investigates how continuous exposure to psychosocial and material factors influences self-rated health (SRH) trajectories in different income groups, uniquely contrasting two mechanisms from a life course perspective: accumulation, where disadvantages intensify with longer exposure, and adaptation, where individuals adjust to adverse conditions.
Methods:
Based on the German Socio-Economic Panel (1994–2017), we analyzed data from 31,961 women and 29,149 men (18–75 years; ⩾2 observations). Psychosocial and material factors (e.g. financial/occupational worries, housing/income dissatisfaction) were measured dichotomously and as continuous exposition. Income- and sex-stratified fixed-effects regressions examined within-individual associations between exposure duration and SRH, adjusting for social environment, occupational position, and life stages. Additional specifications included continuous age and time fixed-effects.
Results:
Longer continuous exposure to disadvantageous factors was associated with declining SRH, particularly for financial worries, housing status, and income dissatisfaction, consistent with the accumulation thesis. For example, after five years of financial worries, low-income men rated their SRH ~0.2 points lower on a five-point scale compared with shorter or no continuous exposure. Adjustment for continuous age and time fixed-effects mitigated some duration effects, especially in lower income groups, indicating partly overlap of the observed patterns with age- or time-related health dynamics. Patterns indicative of adaptation were modest, with little attenuation across continuous exposure for most factors.
Conclusions:
Keywords
Background
A large body of research has documented a pronounced social gradient in the chances of achieving and maintaining good health, based on evidence from both cross-sectional [1,2] and longitudinal [3–5] studies. Regarding the different indicators of socioeconomic status, income has proven to be particularly relevant, as it reflects the resources available to purchase goods and services that determine living standards, such as housing or living environment [6]. At the same time, income might also shape how individuals experience and respond to unforeseen (financial) hardship. Individuals with higher incomes typically have greater access to resources that can buffer adverse conditions and support recovery, whereas those with lower incomes might be more vulnerable to disadvantageous exposures and less able to compensate for their effects [7]. Accordingly, exposure–health trajectories might differ across income groups, reflecting differences in vulnerability, available resources, and acquired reserves [8]. In general, psychosocial and, particularly, material factors have been identified as pivotal mechanisms for linking socioeconomic conditions to health outcomes [9,10].
From a life course epidemiology perspective, adverse circumstances, including exposure to material but also psychosocial conditions, should be examined longitudinally to capture their dynamic and cumulative associations with health [8,11], since their relevance might vary over time as health trajectories unfold [5].
Two main theoretical approaches have emerged to explain how adverse exposures affect health over time. First, the accumulation thesis assumes that the risk of adverse health increases with the time spent in disadvantageous conditions, that is, the number or frequency of exposure episodes [12,13]. In the present study, accumulation refers to increasingly adverse health trajectories with longer continuous exposure duration. Second, the adaptation thesis highlights individuals’ capacity to partially or fully adjust to adverse conditions over time, potentially allowing health to return toward its initial level after deterioration due to an adverse exposure [14]. If such reserves are insufficient, prolonged exposure might overwhelm adaptive capacity, leading to (accelerated) health declines [15,16], consistent with life course perspectives that view adaptive reserves and vulnerability as dynamic and socially patterned resources shaping responses to cumulative exposures [8]. In this study, adaptation is primarily considered in terms of attenuation of health effects while exposure persists (within-exposure adaptation). Although evidence supporting both perspectives has been found for certain exposures [17], these approaches have largely been studied independently. As a result, it remains inconclusive whether accumulation and adaptation represent mutually exclusive, complementary, or even overlapping concepts unfolding over the life course.
Despite growing longitudinal research on social determinants of health, primarily focused on conventional indicators of socioeconomic status, we still know little about how continuous exposure to psychosocial and material factors relates to processes of accumulation and/or adaptation in different income groups.
Thus, we aim to examine the effect of continuous exposure to disadvantageous psychosocial and material factors on subjective health in different income groups, examining mechanisms of accumulation and adaptation.
Accordingly, our main research question is: to what extent are psychosocial and material exposures associated with self-rated health within low-, medium-, and high-income groups, and to what extent are these associations consistent with the accumulation or adaptation thesis?
To address this question, we estimate income-stratified models, allowing associations between exposures and health to be examined separately for each income group and enabling an assessment of whether the observed patterns are indicative of accumulation or adaptation processes. Patterns consistent with the former would be reflected in increasingly negative associations with longer durations of continuous exposure, while patterns consistent with the latter would be indicated by attenuation of health associations, suggesting partial adjustment to ongoing adverse conditions.
Methods
Data source
All analyses are based on self-reported data from the German Socio-Economic Panel (SOEP), an annual longitudinal survey conducted through personal interviews with households across Germany. The SOEP maintains a representative sample of German society through high follow-up rates and regular refreshment samples [18]. The data used included all SOEP waves from 1994 to 2017 (SOEP v34), whereby individuals with less than two observations were excluded (20,065 persons) to enable the use of fixed-effects regressions. The upper age limit was 75 years to avoid bias from data thinning, selective mortality, and faster decreasing health at higher age.
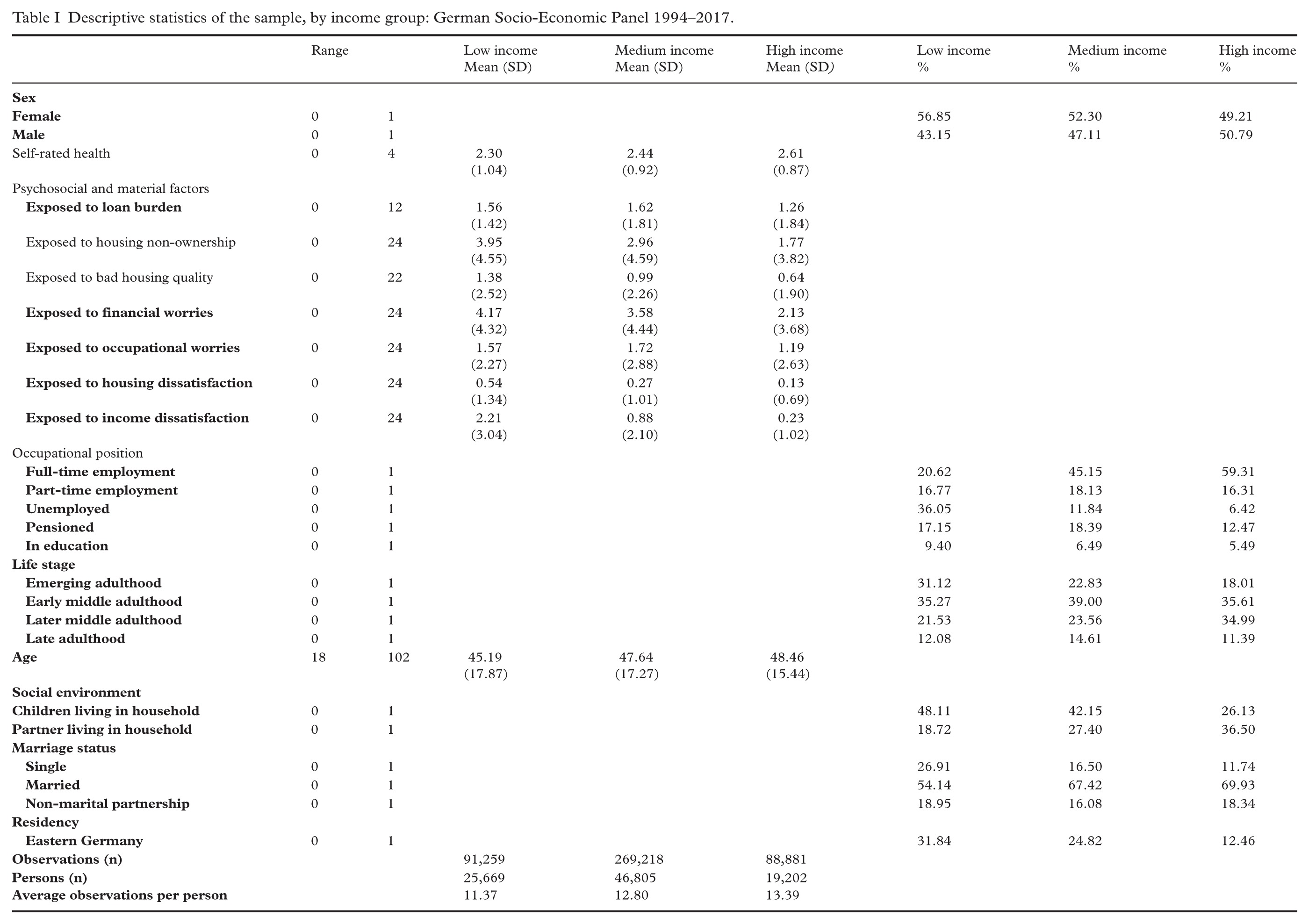
Descriptive sample statistics (including all observations across time) are shown in Table I. Since we involved only secondary analysis of anonymized data, ethical approval was not required. The data have been collected in accordance with German data protection laws.
Descriptive statistics of the sample, by income group: German Socio-Economic Panel 1994–2017.
Outcome variable
Self-rated health (SRH) is considered an accurate and reliable measure of general health, particularly mortality and morbidity [19], and has been collected annually in the SOEP since 1994. The original variable was inverted to a (continuous-treated) five-point scale spanning from 0 “poor” to 4 “very good” to ensure that higher values indicate better SRH.
Income
Among the different indicators of socioeconomic status (SES), income was chosen as the most appropriate. Unlike education, which primarily represents knowledge and intangible resources, income is more sensitive to social and individual changes over time and is therefore particularly suitable for longitudinal analyses. Furthermore, it directly reflects respondents’ current available financial resources and economic constraints [6] and might capture different associations between continuous exposure to psychosocial and material factors especially well. In the analyses, income was used as a stratification variable rather than as an explanatory variable, grouping participants according to their income group each year. It was calculated using income quintiles, with the top quintile representing a high, the bottom quintile a low, and the middle three a medium income. This approach reflects the broad middle-class segment within German society while also preventing potential bias due to small cell sizes, as suggested by Lampert et al. (2012) for health monitoring in Germany [20].
Psychosocial and material factors
All psychosocial and material factors were dichotomized, with 0 indicating non-exposure and 1 indicating exposure to the respective factor in the given survey year.
Psychosocial factors
Economic insecurities were measured through questions on financial and occupational worries, with the response categories: “not concerned at all,” “somewhat concerned,” “very concerned.” The latter two were coded as 1, the first category as 0. Income and housing dissatisfaction were assessed using 10-point scales, with higher scores indicating higher levels of satisfaction. Median splits were used to determine exposure. Scores below the median (7 for income, 8 for housing) were classified as below-average satisfaction and assigned to the code 1. Values at or above the median were categorized as average or above average satisfaction and coded 0.
Material factors
To assess loan burden, the code 0 was assigned to observations where individuals reported loan repayments as manageable (“no exposure to burdening loan repayment”). Conversely, for observations where respondents perceived loan repayment as either a major or minor burden, code 1 (“exposure to burdening loan repayment”) was assigned.
Housing status was determined based on respondents’ residential ownership status. Ownership, regardless of property type, was designated as code 0, while non-ownership, including all forms of tenancy, was assigned to the code 1.
Housing quality was operationalized by the extent of renovation need, categorizing values as “good condition,” “partial renovation,” “full renovation,” and “dilapidated.” The first category was assigned to code 0, the subsequent three indicating exposure to poor housing quality (code 1).
Exposure duration
Exposure duration was modeled as a categorical, time-varying variable considering only continuous years of exposure. If respondents experienced non-exposure for at least one year or if no information was available, the exposure duration count was reset to 0 and restarted at 1 for a new exposure observation period. For instance, if an individual reported dissatisfaction with their income for two consecutive survey waves, the exposure-duration variable took the values 1 and 2 during this first exposure spell. If this was followed by four consecutive waves without dissatisfaction, the variable is coded as 0 in each of these years. If the respondent subsequently reported dissatisfaction again for three consecutive waves, this defines a new exposure spell, and the duration count restarted at 1 and taking the values 1, 2, and 3.
By focusing exclusively on continuous exposure, this specification allows duration-based accumulation processes to be examined more directly and facilitates the identification of attenuation patterns that might be consistent with within-exposure adaptation. Intermittent exposure, by contrast, might blur this distinction, as cumulative effects might not manifest in the same way under interrupted exposure [21] and health improvements during non-exposed periods could reflect recovery rather than attenuation [22]. Therefore, exposure durations spanning the entire observation period were scarce, making valid conclusions beyond a continuous exposure duration of 15 years largely unachievable for most factors.
Consequently, we decided to limit the associations between exposure duration and SRH shown in the plots (Figure 1) to a minimum of one and a maximum of 15 years.
Covariates
To mitigate confounding bias, adjustments for potential covariates were made in all models, such as marital status (single, cohabiting, married) and the presence of partners or small children in the household as measures of respondents’ social environments. We further controlled for regional residency (eastern versus western Germany) and indicators of occupational position (full-time employment, part-time employment, unemployed, pensioned, in education). Since both the duration of exposure (time) as well as the specific point in life at which a disadvantage was experienced (timing) are relevant [13], we also adjusted for the respective life stages, including emerging (18–32), early middle (33–49), and later middle adulthood (50–64) as well as late adulthood (65–75 years) [23]. In additional specifications, we further adjusted for continuous age and survey-year dummies (time fixed-effects).
Statistical analyses
Linear fixed-effects (FE) models were considered the best method for the statistical analyses, as they inherently control for any time-invariant confounders. Therefore, exposure towards all disadvantageous factors as well as all covariates described above in the previous section were treated as time-varying and included in the respective models accordingly, to enable reliable statements about the relationships under investigation [24]. To also account for more fine-grained ageing processes and potential period-specific influences affecting all respondents (e.g. secular trends or policy reforms), we additionally re-estimated all models, including continuous age and time fixed-effects (survey-year dummies). The extended specifications are presented alongside the initial models to facilitate direct comparisons of the estimated duration effects. We ran a separate model for each of the factors (see Supplementary material Tables I–XXVIII online). Average marginal effects (FE-AME models) were used, to determine whether and to what extent the findings vary with continuous exposure duration, providing information on the average change in SRH. All models were stratified by sex and income group to identify potential trajectory disparities within the respective groups (within-estimator). Panel-robust standard errors were used in all estimated models, to adjust for clustering of observations within respondents. All analyses were conducted using Stata version 18.
Results
Sample characteristics
On average, participants were 45.19 years old in the low-, 47.64 years in the medium-, and 48.46 years in the high-income group and reported intermediate levels of SRH (medium. income: 2.44), with the low-income group slightly below (2.30) and the high-income group slightly above average (2.61). Sex distribution was fairly balanced, with a female majority in the low- (56.85%) and medium- (52.30%) but fewer women in the high-income group (49.21%). The high-income group had the shortest exposures across all factors. Low-income respondents showed higher average exposure durations for financial worries (4.17 years vs. 3.58 vs. 2.13), housing status (3.95 vs. 2.96 vs. 1.77), housing quality (1.38 vs. 0.99 vs. 0.64), and income dissatisfaction (2.21 vs. 0.88 vs. 0.23). Medium-income participants faced longer exposure durations to loan burdens (1.62 vs. 1.56 and 1.26 years) and occupational worries (1.72 vs. 1.57 vs. 1.19).
Financial and occupational worries
Increasing negative effects of continuous financial worries on SRH were evident for all income groups and sexes (Figure 1(a)), indicating accumulation processes. The effects were more pronounced within the medium- and low-income group, with low-income respondents showing the strongest associations. For example, after five years of continuous exposure, men in this income group rated their SRH on average about 0.2 points lower (on a five-point scale) than they would have done without these financial worries. Associations within the high-income group were less pronounced. When additionally controlling for continuous age and time fixed-effects (Figure 1(b)), the previously observed accumulation patterns were mitigated, particularly in the low- and medium-income groups. The trajectories became flatter and more uniform, suggesting that part of the initial effects reflect age- or time-related health dynamics. However, negative associations with prolonged financial worries remained visible, indicating that the overall pattern of duration-related health deterioration persisted, albeit in a moderated form.
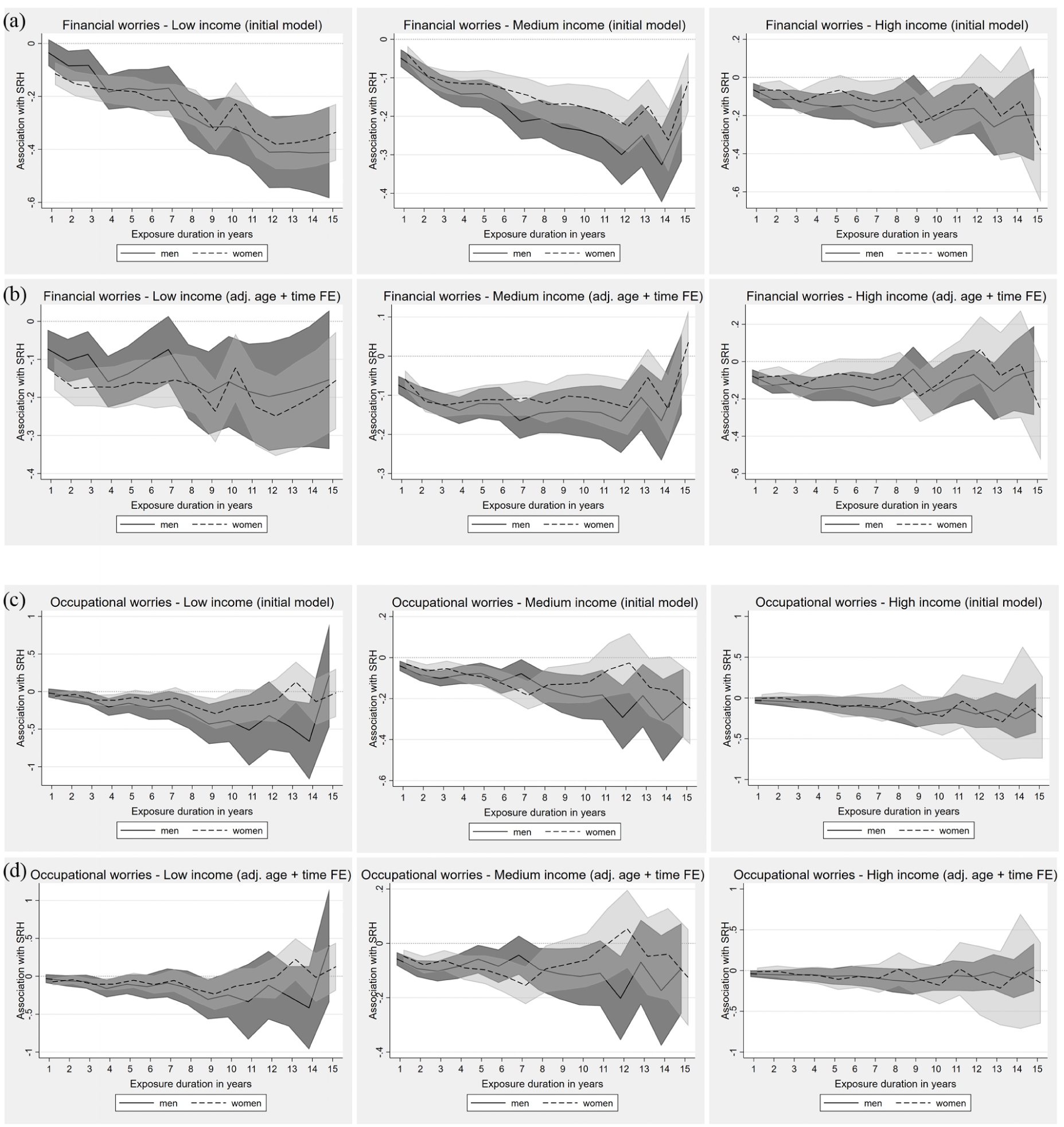
Fixed-effects (FE) models for the impact of continuous exposure to financial ((a) and (b)) and occupational ((c) and (d)) worries on self-rated health (SRH) across income groups (presented as average marginal effects).
Regarding occupational worries the results were less consistent, but also suggested accumulation processes, especially for long exposure durations (Figure 1(c)). These were most evident for men in the medium-income group. The inclusion of continuous age and time fixed-effects (Figure 1(d)) further flattened the trajectories, especially in the low- and medium-income groups. Indications of worsening SRH with longer exposure persisted, but the patterns were less clearly consistent with accumulation processes. Results in the high-income group changed only marginally.
Income and housing dissatisfaction
All models adjust for employment status, life stage, marital status, social environment, residency; Figure 1(b) and (d) additionally adjust for continuous age and time fixed-effects.
The effect of below-average income satisfaction on SRH indicated substantial and persistent accumulation effects (Figure 2(a)), increasing with longer exposure durations. Participants within the low- and medium-income groups showed a clear decline in SRH with increasing exposure to income dissatisfaction. Thus, women with a medium income rated their SRH about 0.15 points lower on average after five years of continuous income dissatisfaction, and about 0.3 points lower after 11 years, compared with no exposure. After additionally controlling for continuous age and time fixed-effects (Figure 2(b)), the previously pronounced accumulation patterns became less distinct. In the low- and medium-income groups, trajectories appeared notably flatter, suggesting persistent rather than progressively worsening effects. In the high-income group, overall patterns remained broadly comparable to the initial model.
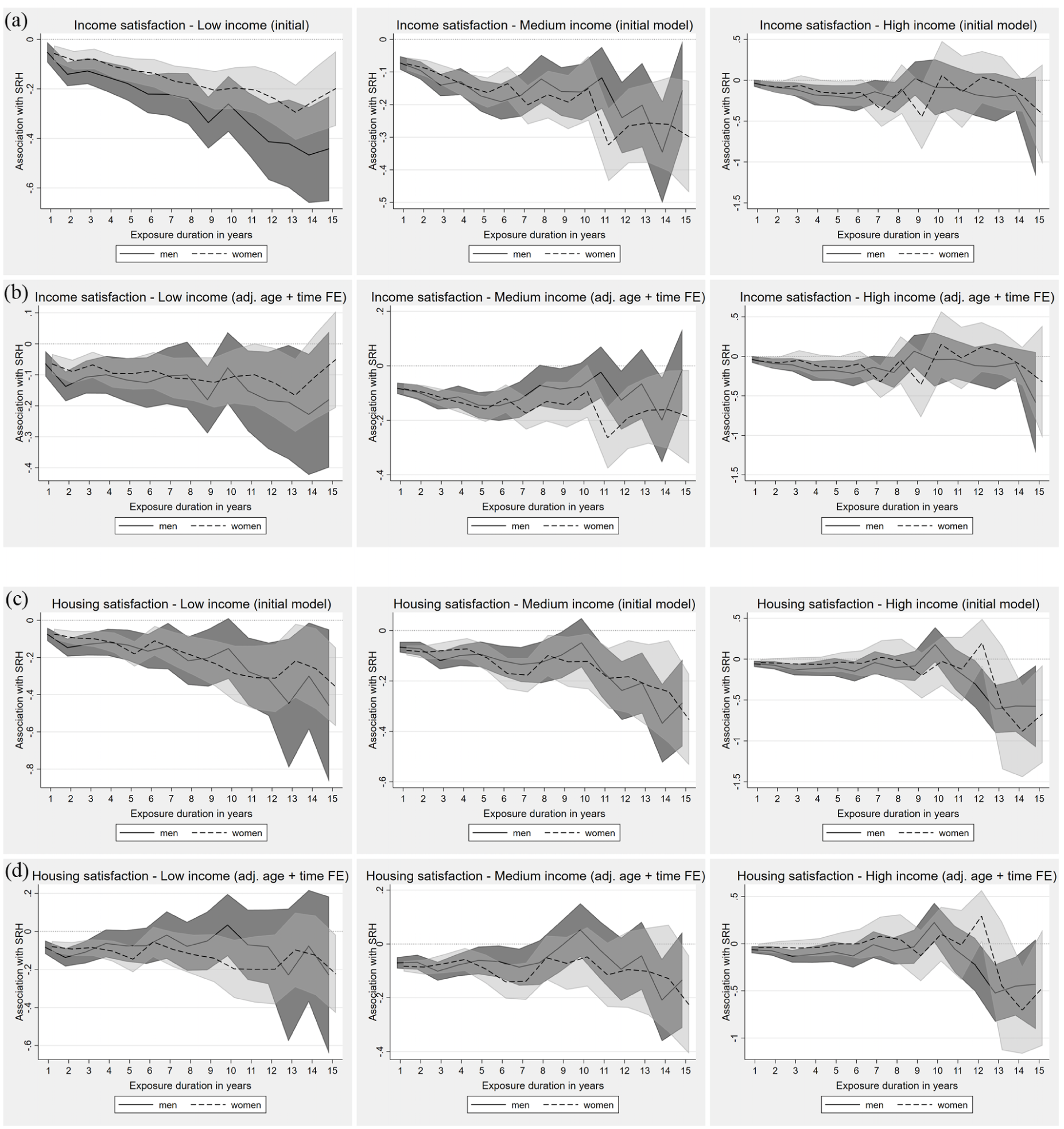
Fixed-effects (FE) models for the impact of continuous exposure to below-average income ((a) and (b)) and housing ((c) and (d)) satisfaction on self-rated health (SRH) across income groups (presented as average marginal effects).
Housing dissatisfaction also showed negative effects on SRH, indicating an accumulation of disadvantages (Figure 2(c)). It also displayed stronger accumulation tendencies in the high-income group, even if they occurred only after an exposure duration of 10 years or more. Including continuous age and time fixed-effects (Figure 2(d)) mitigated the previously clearer accumulation patterns in the low- and medium-income groups, resulting in flatter and more sex-heterogeneous trajectories. Among men, duration effects largely diminished, while women displayed modest negative trends without a consistent linear accumulation pattern.
In the high-income group, a decline in SRH with prolonged exposure remained visible, although somewhat mitigated compared with the initial specification.
All models adjust for employment status, life stage,marital status, social environment, residency; Figure 2(b) and (d) additionally adjust for continuous age and time fixed-effects.
Loan burden
The effects of continuous exposure to loan burden on SRH could not be clearly attributed to either accumulation or adaptation processes (Figure 3(a)). After accounting for continuous age and time fixed-effects (Figure 3(b)), these trajectories remained largely unchanged and continued to show no consistent patterns.
All models adjust for employment status, life stage, marital status, social environment, residency; Figure 3(b) additionally adjusts for continuous age and time fixed-effects.
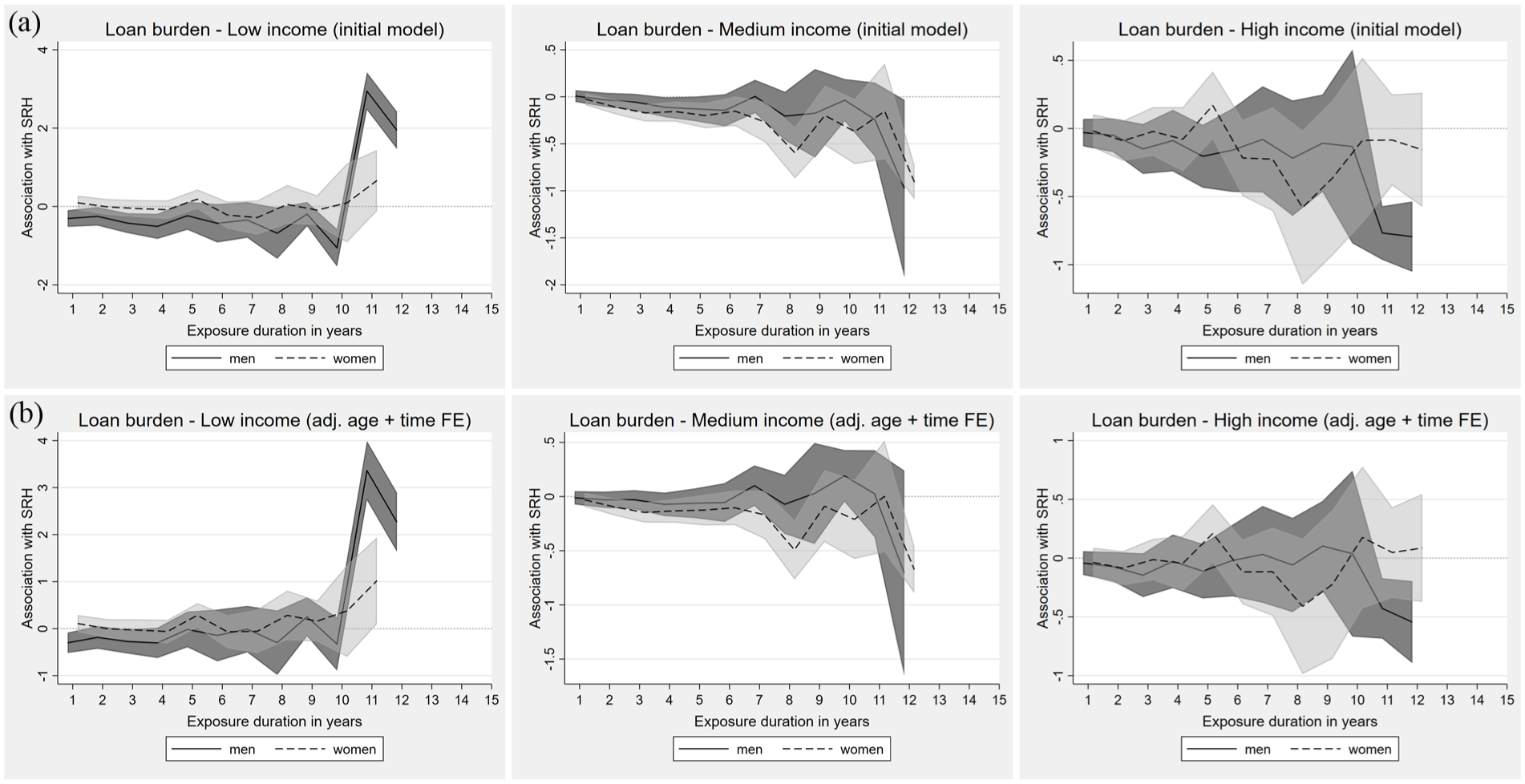
Fixed-effects (FE) models for the impact of continuous exposure to loan burden on self-rated health (SRH) across income groups (presented as average marginal effects).
Housing status
Regarding housing status, accumulation processes were again evident in all income groups, although associations were weaker within the high-income group (Figure 4(a)). Interestingly, housing non-ownership was initially positively linked to SRH in all income groups but became negatively associated after a short time. After including continuous age and time fixed-effects (Figure 4(b)), these accumulation patterns were substantially mitigated.
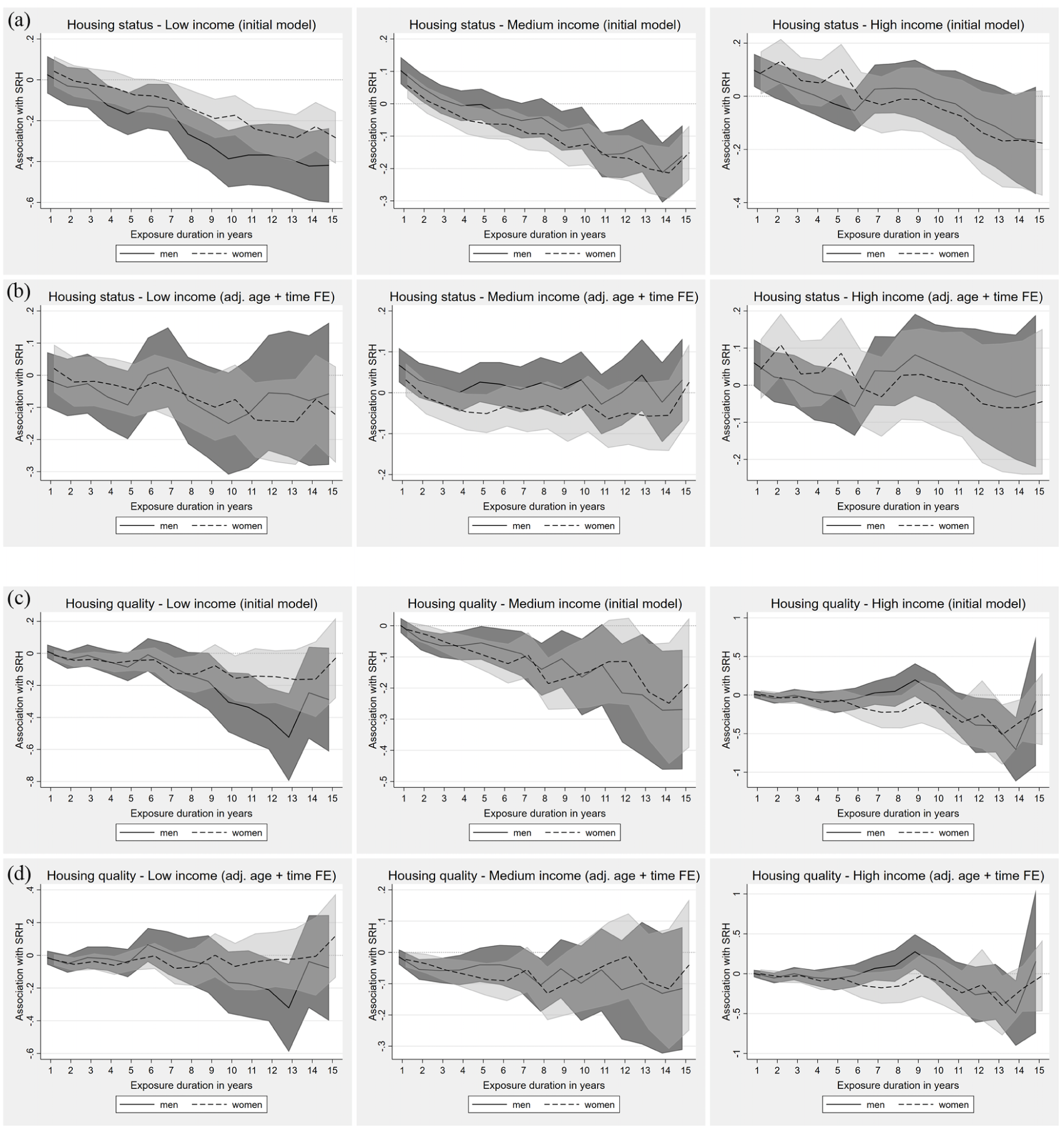
Fixed-effects (FE) models for the impact of continuous exposure to disadvantageous housing status ((a) and (b)) and quality ((c) and (d)) on self-rated health (SRH) across income groups (presented as average marginal effects).
In the low- and medium-income groups, trajectories became notably flatter and no longer consistent with clear accumulation processes. In the high-income group, patterns remained broadly similar to the initial model, though with fewer statistically significant associations across exposure durations.
Housing quality
Continuous exposure to poor housing quality showed a negative effect on SRH, again suggesting accumulation processes, particularly within the medium-income group (Figure 4(c)). Among high-income respondents, adverse associations emerged only after five or more years of continuous exposure. After adjusting for continuous age and time fixed-effects (Figure 4(d)), patterns became more heterogeneous. In the low-income group, some longer-duration declines remained visible, especially among men, but were less consistently significant. In the medium-income group, previously clearer accumulation tendencies were mitigated, with only modest early declines and wide uncertainty at longer durations. In the high-income group, longer exposures were again linked to more negative estimates, though with greater uncertainty and fewer statistically significant effects than in the initial model.
All models adjust for employment status, life stage, marital status, social environment, residency; Figure 4(b) and (d) additionally adjust for continuous age and time fixed-effects.
At a glance
Strongest accumulation effects. Financial worries (especially low/medium-income groups), housing status (all income groups), income dissatisfaction (especially low-income men);
Less pronounced effects. Housing quality (especially medium-income group; high-income group only after five years), housing dissatisfaction (especially low/medium-income groups; high-income group only after 10 years);
Heterogeneous patterns. Occupational worries (except medium-income men), loan burden (no clear accumulation or adaptation trend across model specifications);
Sex. Women generally exhibited somewhat milder trajectories in their within-effects and magnitudes;
Adjusted models. Adjustment for continuous age and time fixed-effects mitigated several duration effects, particularly in lower income groups.
Discussion
Accumulation processes were evident across nearly all psychosocial and material factors and their effects on SRH. Additional models including continuous age and survey-year dummies (time fixed-effects) mitigated several of the initially more pronounced duration effects, suggesting that parts of the observed accumulation patterns might overlap with age- or time-related health dynamics. At the same time, negative associations between continuous exposure and SRH remained visible across multiple domains, especially for financial and occupational worries, indicating that the identified inequalities cannot be fully attributed to ageing or time trends alone.
We found no consistent evidence supporting the adaptation perspective, unlike Clark and Georgellis, who did so for labor market and life events on well-being [14]. While some attenuation patterns emerged in the adjusted models, these were typically statistically non-significant and/or not sustained over longer exposure durations, often followed by renewed accumulation or heterogeneous patterns.
No valid effects were found for loan burden, which might be due to the lower prevalence of student and real estate loan debt in Germany, common sources of long-term financial strain [25]. Conversely, for some factors, such as housing status and financial worries, accumulation processes were evident across income groups. A decreasing relevance of material factors for SRH in repeated measurements, as observed by Groeniger et al. [5] for mortality, was therefore not apparent. Instead, housing status emerged as a substantial determinant of SRH when considered as continuous exposure, showing consistent accumulation processes across income levels in the initial models. After a phase of expenditure and effort associated with the acquisition of property, home ownership is described as a psychological anchor that could increase self-esteem, life satisfaction, and social integration, acting as a proxy for well-being, which might be lacking in its absence [26]. This is particularly noteworthy given that Germany has one the lowest housing ownership rates in Europe, due to an extensive supply of affordable long-term rental housing on the one hand and high transfer taxes and relatively limited subsidies for purchasing real estate on the other [25]. Continuous exposure to financial worries was also associated with progressively disadvantageous effects on SRH. Existing literature thereby primarily emphasizes the impact of financial worries as stressors on mental and physical health [27,28].
Individuals with limited financial resources might also face greater barriers to accessing and maintaining housing ownership and healthy lifestyles [11,26], although in Germany these challenges are partly mitigated by a welfare state that provides a wide range of protections, including nearly universal access to healthcare [29]. These findings align with previous longitudinal research which also identified housing status and financial worries as factors strongly linked to accumulation processes [30]. At the same time, more nuanced and partly divergent trajectories were observed for most of the other factors, depending on the income group considered.
Within low-income participants, nearly all psychosocial and material factors showed declining SRH effects with continuous exposure in the initial models, emphasizing the relevance of accumulation processes, which might reflect more limited reserves and higher vulnerability to persistent exposures [8] . The negative effects for persons with low income were most pronounced for housing and income dissatisfaction.
The effect for housing dissatisfaction could result from the correlation between low income and an increasing likelihood of affordability issues in the housing market, which, in turn, could lead to poorer housing [31]. Moreover, these respondents might only be able to afford fewer, if any, activities or stays outside their own homes. Furthermore, the longer low housing satisfaction persists in combination with low income, the less likely it is that the situation will improve, which is reflected in an increasing deterioration in health [32]. For income dissatisfaction, it can also be assumed that continuing discontent leads to diminishing prospects of improvements, which increasingly negatively impacts SRH.
Continuous exposure might also increase the amount of time that persons are limited or unable to participate in society owing to financial hardship, leading to social isolation and lower self-esteem, correlates of poorer (mental) health [33].
Regarding housing quality and occupational worries, some of the most pronounced impacts on SRH were evident within the medium-income group in the initial specification. Corresponding research suggests that individuals with a medium income are particularly prone to fearing a loss of status and standard of living due to negative (occupational) changes [34]. However, Germany’s extensive welfare system might help to alleviate job insecurity and related stress, which could, in turn, explain the partly ambiguous effects on SRH. The former is also consistent with the findings on housing quality, where differences in the health effects might be attributed to differing definitions of the need for renovation. Participants with high income are possibly more likely to face minor housing deficiencies that are less relevant to health, while low-income individuals are more likely to experience major defects that directly affect health, such as the risk of exposure to environmental hazards and infectious diseases [35,36].
High-income persons did not display clear accumulation or adaptation patterns for a large number of the studied factors, even though they also were continuously exposed to these disadvantages. It can therefore be assumed that respondents from the high-income group have other or more resources at their disposal to compensate the consequences of disadvantageous exposures, also beyond their mere financial advantages [7], underscoring the role of resource-based differences in shaping individuals’ capacity to buffer and adapt to such exposures over time [8]. At some point, however, even these protective mechanisms seem to be exhausted, which might explain the late, but then often more pronounced, declines in SRH after long-lasting exposures, for example, for housing quality or dissatisfaction [15,16].
Moreover, the timing of exposure also shapes health trajectories, as the same psychosocial and material factors could have different effects depending on when they occur [13]. According to existing research [4,30,37], health impacts seem to peak in early and later middle adulthood, while they appear to be less pronounced in emerging and late adulthood. Our findings indicate similar patterns, although the specific role of life stages in the health effects of disadvantageous exposures was not our primary focus. Moreover, the mitigation of some duration effects after further adjusting for continuous age and time fixed-effects suggests that cumulative disadvantage and temporal or ageing dynamics might partly overlap. Additional analyses indicated that models including only continuous age, only time fixed effects, or both specifications yielded highly comparable trajectories, as both adjustments introduce year-specific temporal variation, making it difficult to clearly disentangle these time-related processes [38]. The mitigation was more pronounced in the lower income groups, indicating that exposure duration, age-related health deterioration and contextual influences might be more closely intertwined in socioeconomically disadvantaged contexts. One possible interpretation is that health trajectories in lower socioeconomic groups are more strongly shaped by age-related decline, a pattern that has been linked to accelerated biological ageing in other research [39,40]. At the same time, period effects such as macroeconomic changes or policy reforms might have affected socioeconomic groups differently, thereby shaping exposure patterns and potentially contributing to the observed mitigation [41].
Strengths and limitations
Based on the extensive and long-running data source of the SOEP, the large sample size of this study allowed to explore the relationship between psychosocial and material factors and SRH within different income groups using a longitudinal approach. This longitudinal design enabled the observation of individual trajectories of exposure to the considered factors over time.
Our analyses used fixed-effects regressions along with several key covariates to account for time-invariant characteristics and numerous time-varying confounders, thereby enhancing the validity of the observed effects. However, residual confounding by unobserved time-varying factors cannot be ruled out. Moreover, while accounting for time-invariant unobserved heterogeneity, fixed-effects models cannot fully eliminate the possibility of reverse causality, whereby declining health might itself increase the likelihood of subsequent exposure to adverse psychosocial or material factors. In addition, while the FE-AME models captured the average change in SRH over time, allowing us to examine health trajectories separately within income groups, they do not inherently test differences between them. Consequently, although our findings are suggestive of a social gradient, we cannot conclusively confirm its presence.
This study relies on self-reported data, which, although providing valuable insights into individual (health) perceptions, might also introduce some bias owing to recall issues, social desirability, and/or subjectivity. The same applies to potential bias from the fact that the first (or last) year of observed exposure might not align with the actual exposure period, limiting the accuracy of duration as an explanatory variable.
The differences in the trajectories presented in this study appear rather modest in size at first glance. However, it should be noted that the average marginal effects are the values that result from a single change in one factor at a time, while keeping all other conditions constant. Yet, it can be assumed that simultaneous exposures to multiple factors or a relapse to the initially studied exposure could lead to heightened effects.
Additionally, attrition over time could further contribute to an underestimation of health effects, as individuals facing severe stressors or health issues might be more likely to drop out of the survey. Supplementary analyses indicated that poorer baseline SRH was modestly associated with higher dropout probabilities, whereas attrition was not disproportionately concentrated among low-income respondents. Although the magnitude of these associations was small, and explained variance negligible, some bias cannot be entirely ruled out. While the use of refreshment samples in the SOEP helps maintain representativeness, survey participants might still appear somewhat healthier than the general population [42].
In the specific context of Germany, structural factors such as the peculiarities of the German (welfare) system might also shape the observed effects by providing potential protective mechanisms. While unlikely to fully counteract all consequences of continuous exposure to disadvantageous conditions, as evidenced by factors such as housing status, this system could still shield individuals from extreme material deprivation. This might influence both the magnitude of our findings and their applicability to other countries or policy environments.
We have chosen to study continuous exposure rather than number or frequency of exposure episodes as a first step towards a more holistic view on health inequalities. While allowing a more precise examination of continuous exposures, this approach might restrict the observation of long-term exposures and individuals might be considered multiple times if they were exposed more than once. We chose this strategy to minimize the effect of improvement and deterioration of the living situation. Accordingly, our modeling approach is particularly well suited to identifying accumulation processes and attenuation patterns under continued exposure (within-exposure adaptation), reflecting adjustment to ongoing adverse conditions while exposure persists, whereas post-exposure recovery dynamics (post-exposure adaptation) might be better captured using alternative modeling approaches.
Furthermore, health effects have been studied over a relatively short period of up to 15 years, while prolonged exposures might have even longer-term effects. It remains to be investigated whether and to what extent exposure towards disadvantageous psychosocial and material factors also have an impact on health inequality over longer periods of time, for example, from youth to old age. Specifically regarding the latter, the age cutoff at 75 years might limit the generalizability of our findings to older adults.
Conclusions
While patterns indicative of (within-exposure) adaptation were limited, the initial models revealed evidence for the existence of accumulation processes, as every psychosocial and material factor examined, with the exception of loan burden, showed negative health effects of continuous exposure within at least one income group. Certain factors, such as housing status and financial worries, thereby seemed to be particularly relevant as they were apparent within each income group. Although the inclusion of continuous age and time fixed-effects mitigated several of the initially more pronounced duration effects, especially in lower income groups, certain patterns between continuous exposure and SRH remained visible, particularly regarding financial and occupational worries.
In line with previous research [5], the current study echoes the call for further longitudinal analyses to strengthen the holistic life-course perspective in understanding the associations between SES, (dis)advantageous factors, and health implications. Future research should examine longer-term health disparities, for example, whether and how the anticipation of and exposure to disadvantageous factors affect health at older ages or potentially accelerate age-related health deterioration, while lagged decay-based exposure modeling might provide a promising extension to also more explicitly capture (post-exposure) adaptation processes.
Current health policy concepts often fall short of adequately addressing socioeconomically patterned health inequalities, particularly compared with efforts towards physical health improvements [3]. Our findings highlight the need for targeted measures that focus on reducing income-related disparities.
To this end, it seems vital to identify the (non-monetary) resources that individuals with high income possess to mitigate adverse health effects, and to ensure that these resources also become increasingly accessible to individuals with both low and medium SES.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261450780 – Supplemental material for Examining accumulation and adaptation in psychosocial and material exposures and self-rated health: A fixed-effects approach within income groups using German panel data
Supplemental material, sj-docx-1-sjp-10.1177_14034948261450780 for Examining accumulation and adaptation in psychosocial and material exposures and self-rated health: A fixed-effects approach within income groups using German panel data by Anja Knöchelmann, Tobias Rähse and Matthias Richter in Scandinavian Journal of Public Health
Footnotes
Author contributions
All authors contributed to the study conception and design. Conceptualization: Anja Knöchelmann, Tobias Rähse; writing–original draft preparation: Anja Knöchelmann, Tobias Rähse; writing–review and editing: Anja Knöchelmann, Tobias Rähse, Matthias Richter; funding acquisition: Matthias Richter, Anja Knöchelmann.
Data availability statement
The raw data contained in this manuscript are not openly available owing to data protection restrictions of the German Institute for Economic Research (DIW), which collects and provides the SOEP data. SOEP data are available free of charge for scientific use from the DIW at ![]() after signing a data distribution contract. Data transformation files and codes are available upon reasonable request.
after signing a data distribution contract. Data transformation files and codes are available upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
Since we involved only secondary analysis of anonymized data, ethical approval was not required. The data have been collected in accordance with German data protection laws.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the project “Accumulation, health and health inequalities. The importance of life course processes and risk profiles,” which is funded by the German Research Foundation (DFG), with grant agreement number No. RI2467/2-2.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.