
Abstract
Aims:
To explore the prevalence and associated variables of diabetes distress in the adult Faroese type 1 diabetes (T1D) population.
Methods:
This nationwide study involved the administration of an online questionnaire to adults diagnosed with T1D. A total of 119 participants (58% of the T1D population) completed the seven-item Type 1 Diabetes Distress Scale (T1-DDS-7) in an online survey conducted from June to August 2023. Logistic regression was used to examine the association between diabetes distress and potential associated variables.
Results:
A total of 39% of the participants scored 14 or more in the T1-DDS-7, indicating diabetes distress. Multivariate logistic regressions identified five variables that were associated with diabetes distress: younger age, recent diabetes onset, being a smoker, having a lower self-estimated health, and being unsatisfied with the received information from healthcare professionals prior to start of diabetes treatment.
Conclusions:
Introduction
Diabetes distress encompasses the emotional and psychological challenges associated with the ongoing demands of managing diabetes, a chronic condition requiring constant self-care and vigilance to prevent situational as well as serious long term complications [1]. Individuals with type 1 diabetes (T1D) need to be actively engaged in their treatment, which often leads to burdens and worry that can affect their quality of life [2].
The term diabetes distress was introduced in 1995 [3], defined as the emotional stress associated with the ongoing burden and worries of managing T1D [4]. A study in 2015 identified seven significant sources of diabetes distress among adults with T1D: powerlessness, negative social perceptions, physician distress, friends/family distress, hypoglycemia distress, management distress, and eating distress. Identifying these sources led to the development of a reliable and valid assessment instrument, the Diabetes Distress Scale for Type 1 Diabetes (T1-DDS) to assess diabetes distress [5]. This scale is used to identify specific sources of diabetes distress for adults with T1D and to provide an index of overall diabetes-related emotional distress for use in clinical and research settings [6].
Research involving diabetes distress has been conducted in several countries. A 2015 systematic review found that rates of diabetes distress in T1D range from 20% to 30% [7]. Studies have linked diabetes distress in T1D to challenging life periods such as recent adult diabetes onset, adolescence, and young age [8,9], as well as to demographic factors such as being female, having low social support, and/or glycemic levels outside the recommended interval/area [6,10,11]. Although diabetes distress has been widely studied, most evidence derives from large countries and selected clinical samples. Population-based data from small-scaled healthcare systems with complete national coverage are scarce. The Faroe Islands provide a unique setting to examine diabetes distress in a well-defined, nationwide adult T1D population receiving care within a single diabetes clinic. The Faroe Islands, a self-governing part of the Kingdom of Denmark, are situated in the North Atlantic Ocean and have a population of approximately 54,500 people and an estimated T1D prevalence of 0.4% (n=242) [12]. The Faroe Islands have a Scandinavian-style welfare system, providing residents with equal access to a wide range of social and healthcare services funded through general taxes and statutory health insurance. The National Hospital of the Faroe Islands offers most specialties, including the Steno Diabetes Center Faroe Islands (SDCF), the sole endocrinology clinic in the country, serving all individuals with T1D [12]. People with T1D (PWT1D) have regular consultations with doctors, nurses, and dieticians, tailored to their individual needs. Most PWT1D are offered technological solutions such as an insulin pump and continuous glucose monitors. In 2024, a total of 140 PWT1D (58%) used an insulin pump [12]. Reimbursement for the majority of the expenses occurs through the national health insurance. Every adult member of the national health insurance pays a maximum yearly fee of DKK 2756 per year [13]. Although clinical care at the SDCF is comprehensive, diabetes distress has not yet had a specific focus, and the psychosocial dimension of living with T1D in the Faroe Islands remains unexplored. Assessing the emotional and psychological aspects of T1D management is crucial to determining whether diabetes distress is an area of concern that should be incorporated into routine clinical care. Therefore, this study aims to explore diabetes distress in the adult Faroese T1D population and to identify potential associated variables.
Materials and methods
Subjects and measures
All adult individuals 18 years and older living with T1D on the Faroe Islands (N=205) in June 2023 were invited to participate in this anonymous online cross-sectional questionnaire study. The study invitation was sent to the participants via the SDCF on 23 June 2023, through Mínboks, a personal and secure digital post box. The web-based application Research Electronic Data Capture tool was used to set up the online questionnaires and collect and manage data. In the invitation letter, the participants received a link to the questionnaire, which they completed electronically.
The questionnaire consisted of the Type 1 Diabetes Distress Scale-7 (T1-DDS-7) [14] and a socio-demographic part including age, sex, level of education, living area, occupation, marital status/co-habitation, duration of diabetes, insulin devices, blood glucose device, height, weight, smoking, self-estimated health, self-estimated diet, WHO-5 Well-being Index, and treatment satisfaction assessed with 18-item Survey Study of Patient Experience for Patients with Diabetes [15].
T1-DDS-7
The original 28-item T1-DDS scale was translated and validated into Danish in 2023 [16] and a short form has since been developed and validated as a seven-item version by researchers in the Steno Diabetes Center Copenhagen in Denmark and researchers from the Californian research group who developed the full scale [14]. This scale represents the seven sources of T1D distress: powerlessness, negative social perceptions, physician distress, friend/family distress, hypoglycemia distress, management distress, and eating distress. The T1-DDS-7 short-form instrument was used in this study, as opposed to the 28-item full scale, to test whether it would fit as a quick screening tool in future screening of diabetes distress in PWT1D in routine care at the SDCF. When diabetes distress is detected, the 28-item full scale is then recommended to detect which of the seven sources cause distress.
The questions are answered on a Likert scale from 1 (not a problem) to 6 (a very serious problem). The lowest possible score is 7, and the highest possible score is 42. A score of <14 indicates low diabetes distress, 14–20 indicates moderate diabetes distress, and a score >20 indicates high diabetes distress [14].
The translation process
To ensure the participants’ understanding of the questionnaire, a translation from Danish into Faroese of the T1-DDS-7 was performed before, in collaboration with the SDCF and the University of the Faroe Islands. Even though the Faroe Islands is part of the Danish kingdom, the country has its own language. The Faroese language is the first native language of the Faroese people, and the Danish language is considered the second language, which is learned in public schools in second grade.
In order to maintain the content validity of the T1-DDS-7 instrument in the cross-cultural adaptation, the first author coordinated the translation, and the linguistic validation process according to the five steps of Beaton and colleagues’ Guidelines for the process of cross-cultural adaptation of self-report measures. [17]
The Faroese linguistic translation team consisted of two dualistic translators with Faroese as their first language, the Danish linguistic translation team consisted of two dualistic translators with Danish as their first language, and the expert committee consisted of diabetes healthcare professionals and researchers. The translation process was conducted between March and April 2023.
Data analysis
Data is presented as mean and standard deviation for parametric variables, median and interquartile range for non-parametric variables, and count with percentage for categorical variables. Normally distributed variables were analyzed with the independent t-test, and not normally distributed variables were analyzed with the Mann–Whitney U test. Categorical variables were analyzed with the χ2 test or Fisher’s exact test as appropriate.
Diabetes distress (outcome variable) was categorized into a dichotomous variable: a score of 0–13 indicates low diabetes distress and a score of 14 and above indicates moderate to severe diabetes distress.
Missing data was an issue for several variables. The number of missing values for each variable containing missing values did not reach high counts separately but the complete data set without any missing values resulted in a loss of too much information. Separate ‘n’ is presented when a variable is stratified, and the assumptions of the methods and results rely on the assumption that values are missing completely at random. Univariate logistic regression was used to explore the association between diabetes distress and potential predicting variables one at a time to identify potential predictors. Variables reaching statistical significance (p-value <0.05) were then tested in a multivariate logistic regression model using backward elimination based on Akaike’s Information Criterion to identify the most frequently associated variables.
Categorical variables were grouped into dichotomous groups when the stratification on diabetes distress received fewer than five responses.
Data was analyzed using Statistical Package for the Social Sciences (SPSS), IBM SPSS for Windows (version 29.0) and R (version 4.4.1) together with R Studio.
Results
Sample characteristics
A total of 205 adults with T1D were invited to participate in the study, of which 136 responded to questions about T1D and diabetes distress in the online questionnaire from June to August 2023, corresponding to a participation rate of 66.3%. Participants who reported not having T1D or did not report diabetes type were excluded. The final sample included responses from 119 individuals, corresponding to a participation rate of 58% (Figure 1).
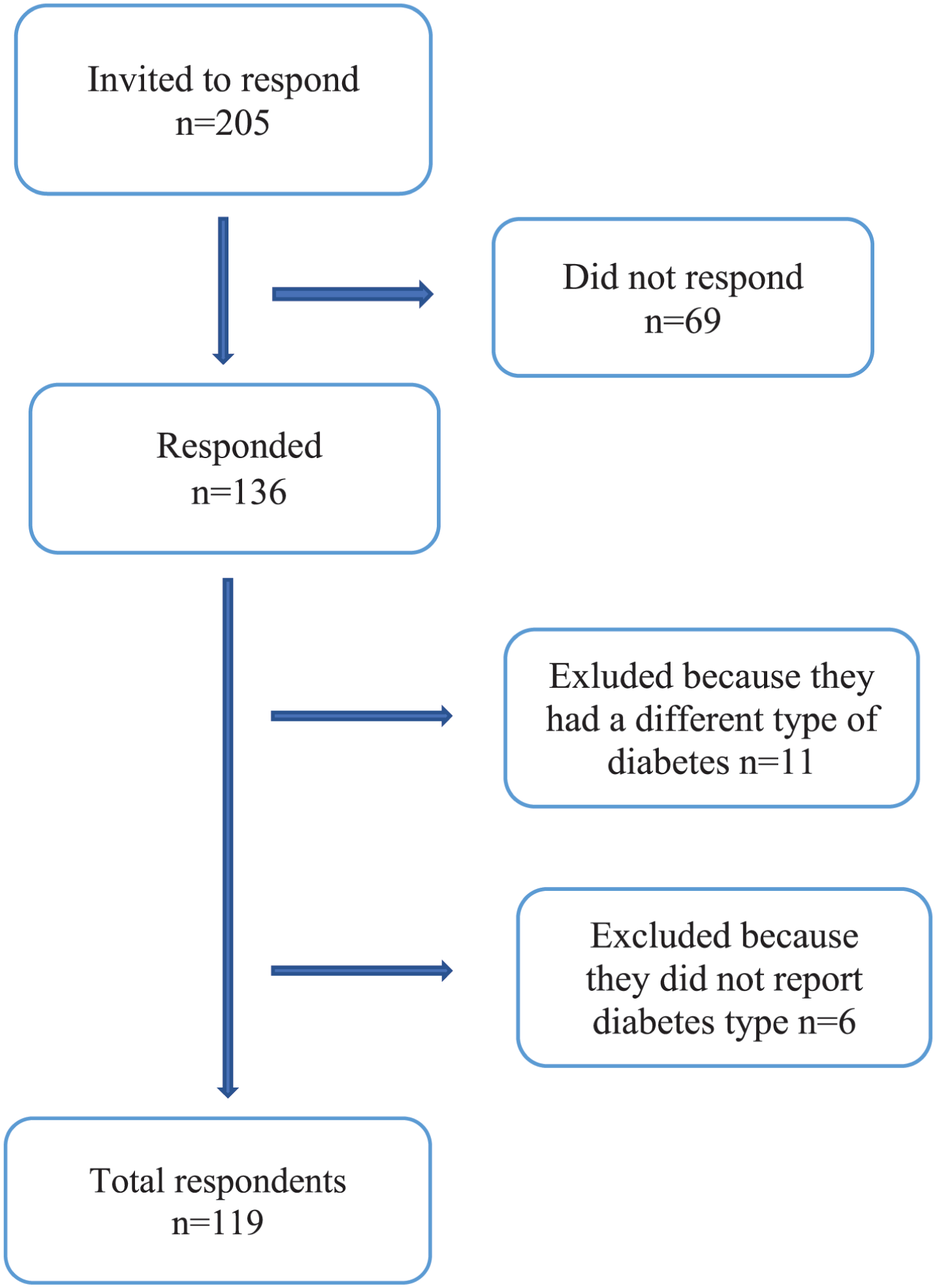
Study flowchart.
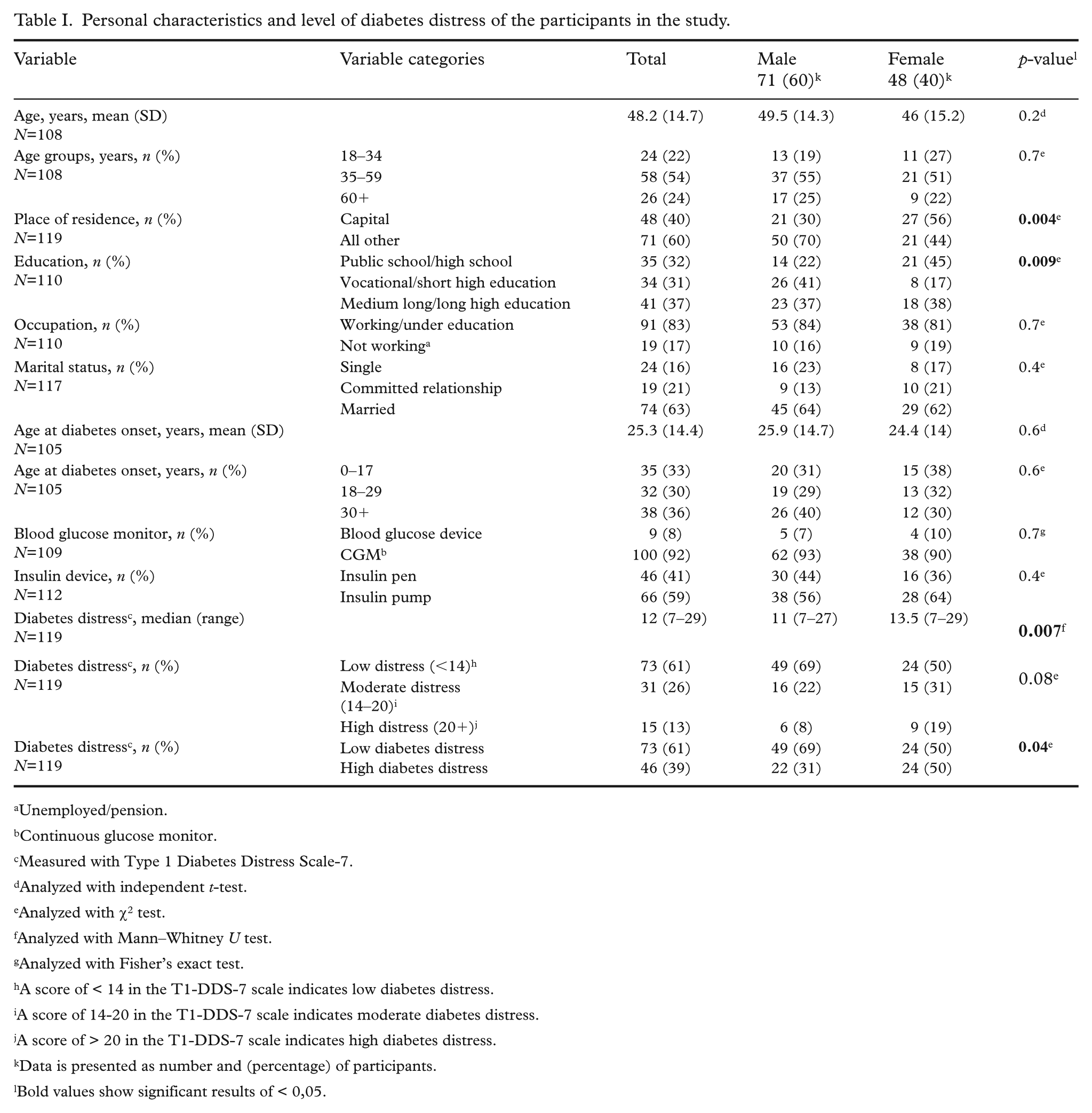
Participant characteristics are presented in Table I. The average age of participants was 48.2 (range 18–67 years); 60% were male, the average age at diabetes onset was 25.3 years; 92% used a continuous glucose monitor, and 59% used an insulin pump (Table I).
Personal characteristics and level of diabetes distress of the participants in the study.
Unemployed/pension.
Continuous glucose monitor.
Measured with Type 1 Diabetes Distress Scale-7.
Analyzed with independent t-test.
Analyzed with χ2 test.
Analyzed with Mann–Whitney U test.
Analyzed with Fisher’s exact test.
A score of < 14 in the T1-DDS-7 scale indicates low diabetes distress.
A score of 14-20 in the T1-DDS-7 scale indicates moderate diabetes distress.
A score of > 20 in the T1-DDS-7 scale indicates high diabetes distress.
Data is presented as number and (percentage) of participants.
Bold values show significant results of < 0,05.
Prevalence of diabetes distress
A total of 39% (n=46) scored 14 or more in the T1-DDS-7, indicating moderate to severe diabetes distress. Moderate diabetes distress was observed in 26% and severe diabetes distress in 13% of the participants (Table I).
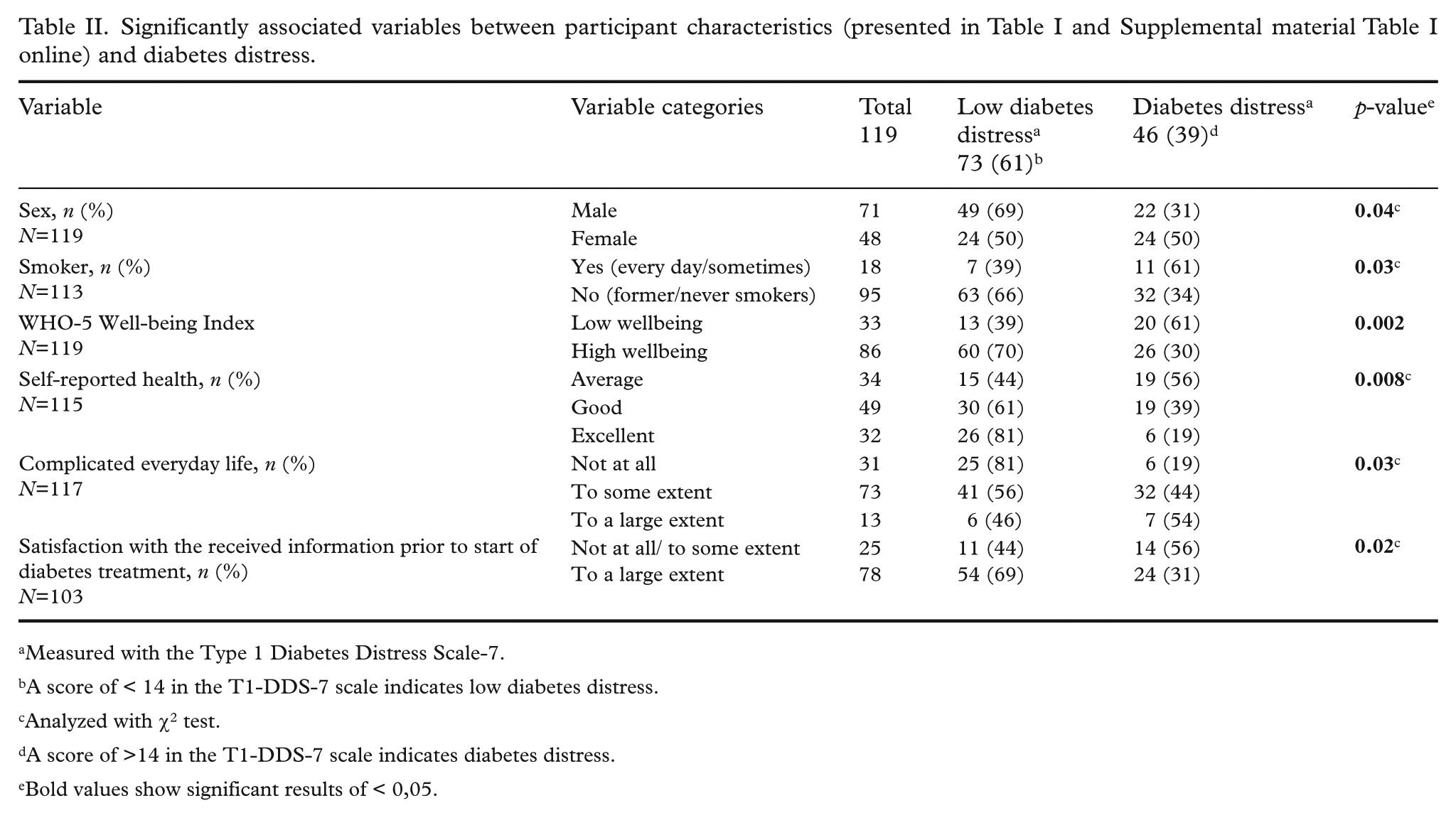
Participant characteristics, grouped according to diabetes distress categories, are presented in Table II. A significant difference in diabetes distress was identified between sexes, with 50% of females and 31% of males experiencing diabetes distress (p=0.04). Participants who experienced diabetes distress were more likely to report that everyday life was complicated to a large extent (p=0.03), were less satisfied with the information they received from healthcare professionals before start of diabetes treatment (p=0.02), had low wellbeing (p=0.002) and low self-estimated health (p=0.008), and were more likely to be smokers (p=0.03) (Table II).
Significantly associated variables between participant characteristics (presented in Table I and Supplemental material Table I online) and diabetes distress.
Measured with the Type 1 Diabetes Distress Scale-7.
A score of < 14 in the T1-DDS-7 scale indicates low diabetes distress.
Analyzed with χ2 test.
A score of >14 in the T1-DDS-7 scale indicates diabetes distress.
Bold values show significant results of < 0,05.
Predictors of diabetes distress
We identified five risk factors that were associated with diabetes distress using multivariate logistic regressions where we included variables found to be statistically significant (p<0.05) in the univariate logistic regressions after backward elimination (Supplemental material Table I online): being of younger age (18–34 years), recent diabetes debut, being a smoker, having bad self-reported health, and being less satisfied with the received information from healthcare professionals before start of diabetes treatment started (Table III).
Associated variables for diabetes distress in the multivariate logistic regression analysis after stepwise backward elimination using variables that were statistically significant in a univariate logistic regression model (Supplemental material Table I online) (N=82).
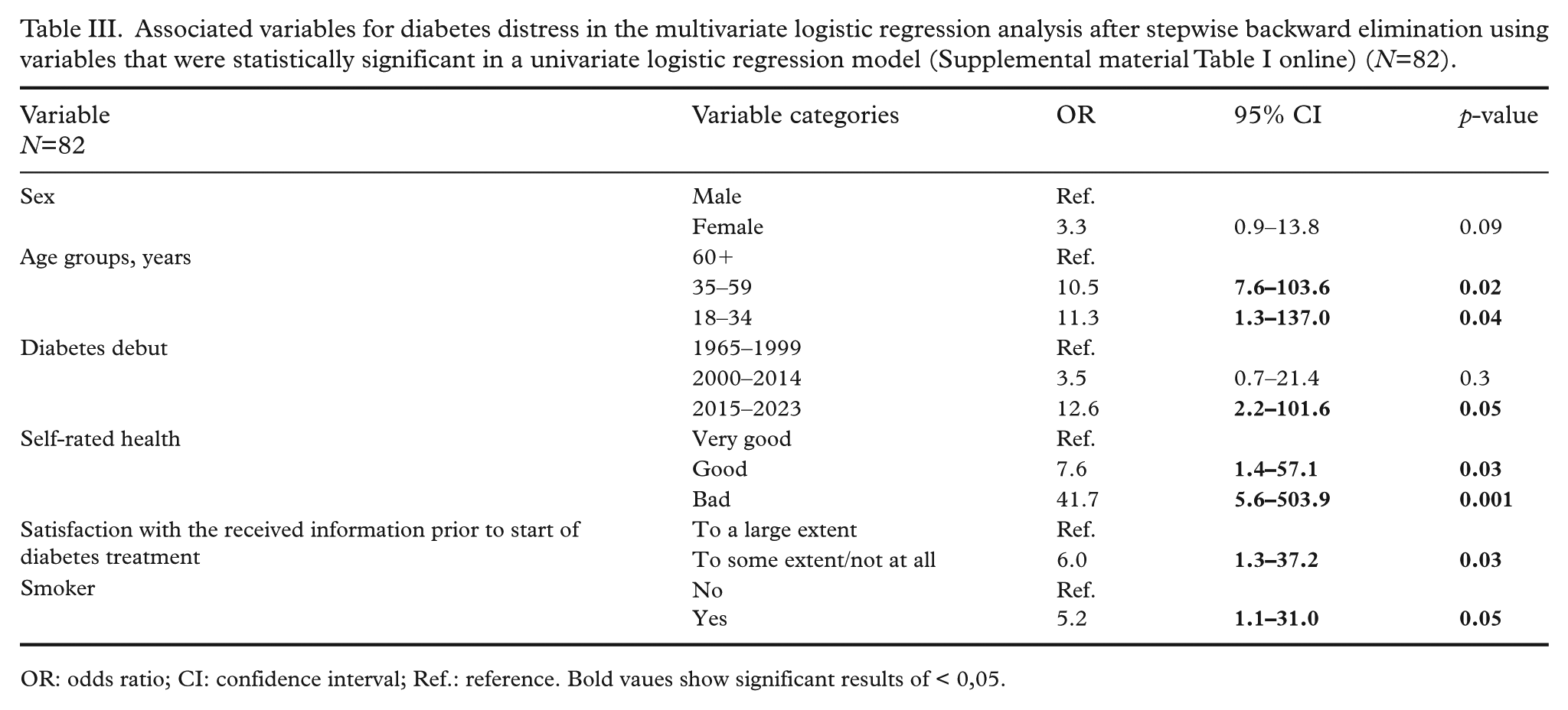
OR: odds ratio; CI: confidence interval; Ref.: reference. Bold vaues show significant results of < 0,05.
Discussion
In this study of diabetes distress among Faroese PWT1D explored by using T1-DDS-7, the prevalence of moderate to high diabetes distress was found to be 39%. This is comparable to the only other study using this instrument, a large Danish cohort study (N=2016), where the prevalence of diabetes distress was 38% [16], as well as in two studies using the full DDS scale [5,18] and a study using the PAID 20 scale [19]. Overall, the findings of this study provide evidence for the applicability of the T1-DDS-7 as a brief screening instrument in routine clinical care.
The finding that demographic factors including sex, age, and recent diabetes debut were associated to high diabetes distress is consistent with previous studies indicating that various subgroups of individuals with T1D, particularly being female and in specific life stages such as being of younger age and having recent T1D onset, increase the likelihood of moderate to severe diabetes distress. These PWT1D require specialized targeted interventions and individualized care to address their personal psychosocial needs [11,19]. A Norwegian study among adult university students found that having T1D was significantly associated with lower quality of life. Additionally, a high level of diabetes distress was associated with being female, failing to meet HbA1c treatment goals, and less frequent blood glucose monitoring [20]. A large multinational study found that emerging adults differed from adults over the age of 30 years in reporting better overall quality of life and social- and healthcare support. However, emerging adults experienced higher levels of diabetes distress and were less engaged in their diabetes self-management [21].
The association of emerging adulthood, short T1D duration, and high diabetes distress identified in our study is also in line with other studies that found higher rates of diabetes distress in these groups of PWT1D [9,22]. The findings of this study highlight a noteworthy prevalence of diabetes distress among emerging adults with T1D and shed light on the distinct challenges this group faces in managing their condition. This finding highlights the need for targeted interventions tailored to this particular group. Recognizing these demographic nuances is essential for developing effective strategies that address the diverse needs of people living with T1D and diabetes distress.
In this study, individuals with high diabetes distress were more likely to have lower self-reported health and were more often smokers than those with low diabetes distress levels. These results are in line with another study where high diabetes distress was associated with low quality of life, low diabetes empowerment, unhealthy diet, and not being physically active, as well as high glycemic levels [23]. Diabetes distress might play a causative role in the individuals’ diabetes management, leading to missed insulin boluses and higher HbA1c or vice versa [24]. A Danish study showed several associations between clinical and psychosocial factors and HbA1c, for example, HbA1c increased by 0.3% (3.1 mmol/mol) per one-point increase in the T1-DDS score [25]. Conversely, another study showed that targeted interventions to reduce high diabetes distress can lead to a dramatic reduction of diabetes distress and that elevated diabetes distress, when left untreated, does not necessarily resolve itself over time and can become chronic [26]. The correlation between HbA1c and diabetes distress has not been examined in this study but should be considered for investigation in future research, particularly intervention research.
In this study, individuals who reported lower satisfaction with the information received before start of diabetes treatment also experienced the highest levels of diabetes distress. This aligns with existing knowledge that a decrease in diabetes distress level may be explained by dealing the attention towards patient concerns [27]. Thus, in a systematic review, higher perceived quality of healthcare provider–patient communication was associated with improved self-management and lower diabetes distress [28].
While the associated factors identified in this study are largely consistent with previous research, the findings extend existing knowledge by demonstrating that both the prevalence and risk profile of diabetes distress observed in larger countries are also present in a small, nationwide T1D population with universal access to diabetes care and high treatment satisfaction [Olsen et al., 2026, in preparation]. This suggests that diabetes distress is not merely a function of healthcare access or system fragmentation, but a persistent psychosocial challenge even within highly organized care settings.
Diabetes distress has been a research target for about 30 years and, therefore, different types of interventions to reduce diabetes distress have also been conducted, showing that dealing with diabetes distress through targeted support can reduce diabetes distress [29]. Researchers in Denmark have been conducting and pilot-testing the study REDUCE [30], where PWT1D with moderate to severe diabetes distress participated in a group-based program with five bi-weekly two and a half-hour meetings. The study showed a significant reduction in diabetes distress and a significant increase in quality of life in the participants. These findings highlight the importance of dealing with diabetes distress in PWT1D by, first, using a screening instrument in routine care settings and, second, offering suitable targeted interventions to reduce moderate to severe diabetes distress.
In evaluating the methodologies utilized across studies, it becomes evident that the instruments employed in assessing diabetes distress among emerging adults exhibit levels of diabetes distress among PWT1D. Nevertheless, studies using other diabetes distress instruments also showed high diabetes distress in adults with T1D [11,19]. In a study of diabetes distress, where all individuals received care in an academic clinical practice that prioritized staff training and interventions to prevent diabetes distress, the prevalence was still 30% [31].
The T1-DDS-7 short-form instrument used in this study has recently been developed and found valid and reliable for routine screening for diabetes distress among adults with T1D [14,16]. The T1-DDS-7 short-scale instrument has now been tested in both this small group of participants and in a larger Danish cohort [16]. This study found that the prevalence and associated variables observed in the Faroe Islands were similar to those observed elsewhere. These findings suggest that implementing this short-form instrument could be helpful in diabetes clinics as a quick screening instrument for detecting diabetes distress in PWT1D. Recommendations, when elevated levels of diabetes distress are found, include using the full 28-item scale to identify which of the seven sources causes the distress and initiating open dialogue with health professionals in routine care before determining further treatment to decrease the diabetes distress [14]. The findings from this questionnaire-based study suggest that routine assessment of diabetes distress might be particularly relevant among Faroese PWT1D, especially younger adults, recently diagnosed people, and PWT1D in vulnerable life situations.
One strength of the study is the high participation rate and the nationwide design, representing 64% of the T1D population on the Faroe Islands. Owing to the limited population size in the Faroe Islands, the number of PWT1D is small. However, a small population represents an opportunity for comprehensive inclusion, where all individuals with T1D attend the same clinic, enhancing the generalizability of the results.
One of the key limitations of this study is the potential for selection bias, which might affect the representativity of the findings. Although the response rate was relatively high (58% of the total T1D population), certain demographic groups were underrepresented, particularly younger adults (18–34 years) and older individuals (60+). Additionally, males were overrepresented, which could skew the results. It is also possible that individuals experiencing higher levels of diabetes distress were less likely to participate owing to survey fatigue or disengagement from healthcare services. These findings are also consistent with previous studies showing that younger individuals and females often report higher levels of diabetes distress [11,19]. This self-selection bias might lead to an under- or over-estimation of the true prevalence of diabetes distress in the adult Faroese T1D population. Further studies should aim for strategies to engage a balanced sample and assess potential differences between respondents to improve generalizability.
Another key limitation of this study is the absence of HbA1c measurements linked to glycemic levels. Including HbA1c and other clinical data in the future research could provide deeper insight into the relationship between emotional distress and clinical diabetes management outcomes.
Conclusions
In conclusion, diabetes distress was reported by more than one-third of adult PWT1D, with emerging adults appearing particularly affected. Key factors associated with increased distress included recent diabetes onset, lower self-rated health, dissatisfaction with the information received prior to initiating diabetes treatment, and current smoking status.
These findings underscore the importance of targeted support in general and particularly during critical life transitions and for individuals in vulnerable situations. Integrating the assessment and the management of diabetes distress into routine diabetes care seems important for improving long-term health and psychosocial outcomes in PWT1D in the Faroe Islands.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261455442 – Supplemental material for Exploring diabetes distress among adults with type 1 diabetes: A nationwide cross-sectional study
Supplemental material, sj-docx-1-sjp-10.1177_14034948261455442 for Exploring diabetes distress among adults with type 1 diabetes: A nationwide cross-sectional study by Tórhalla VANJA. Klein Olsen, May-Britt Skoradal, Ingrid Willaing, Herborg Líggjasardóttir Johannesen and Maria S. Petersen in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We sincerely thank the participants in this study. Appreciation is also expressed to the healthcare team at the SDCF for assistance in the translation process, giving personal comments regarding the T1D treatment, and for assistance in sending out the study invitations.
Ethical considerations
This study complies with the principles in the Declaration of Helsinki and has been conducted in accordance with the data protection regulation in the Faroe Islands.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.