
Abstract
Aim:
To assess the diagnostic accuracy and optimal cut-off scores of the Alcohol Use Disorder Identification Test (AUDIT) and AUDIT-Consumption (AUDIT-C) in a Danish general population.
Methods:
Questionnaire-based cross-sectional study. Data collection from 26 September to 29 October 2024, via an anonymous online test of alcohol habits among adults aged 25+ years.
Measures:
Demographics, AUDIT, self-reported International Classification of Disease Tenth Revision (ICD-10) criteria for alcohol dependence, yes/no item on harmful alcohol use. We defined hazardous use as >10 standard drinks/week (national recommendations) and possible dependence as ⩾3 ICD-10 criteria. We evaluated area under the receiver operating characteristics curve (AUC), diagnostic properties and optimal cut-offs.
Results:
Total sample: 17,959 participants, mean age 66.32 (SD=12.72) years, 51% males. Nineteen per cent reported drinking hazardously, 7.5% answered yes to harmful use and 7.8% to dependence according to ICD-10. AUDIT showed good diagnostic discrimination for hazardous use (AUC=0.89) and dependence (AUC=0.96), but not for harmful use (AUC=0.61). Internationally recommended AUDIT cut-offs for hazardous use and dependence were supported, with lower thresholds in women and the older (65+ years). AUDIT-C: hazardous use (AUC=0.92), dependence (AUC=0.92), harmful use (AUC=0.58). Optimal AUDIT-C cut-offs: hazardous 6, dependence 6, with age- and sex-specific variations. Internal consistency was high for AUDIT (α = 0.83) and low for AUDIT-C (α = 0.61).
Conclusions:
Keywords
Background
Excessive use of alcohol is one of the most important modifiable risk factors, with negative public health impacts globally attributable to an estimated 5.3% of yearly deaths [1]. Treatment-seeking for alcohol problems is generally low owing to factors such as lack of problem awareness, fear of being stigmatized, and lack of knowledge on treatment options [2–4]. Consequently, alcohol use disorders (AUDs) have a large treatment gap for patients with AUDs [5]. Trustworthy screening instruments are important for objective and accurate identification of potential risks or harmful consumption patterns, enabling both healthcare provider and patient to gain insights into the patient’s current situation and discuss suitable treatment or referral options.
The Alcohol Use Disorder Identification Test (AUDIT) is one of the most recognized and globally acknowledged screening instruments for detecting hazardous, harmful, and dependent alcohol use [6–8], where hazardous use pertains to risk of future harm, while harmful use pertains to demonstrable harm to the person’s health due to alcohol [9]. The AUDIT has been widely translated, validated, and applied in various settings worldwide [10–13]. The AUDIT score runs from 0 to 40, with current consensus around cut-off scores of 6 for women and 8 for men regarding hazardous use, 16 for both women and men regarding harmful use, and 20 indicating possible dependence [6,14].
The shorter AUDIT-Consumption (AUDIT-C) consists of the three consumption-related questions from the full AUDIT, has scores ranging from 0 to 12, and has been found a reliable instrument to identify hazardous alcohol use across various populations and settings [15–17]. Current suggested cut-off scores on the AUDIT-C for identifying hazardous use range around 3/4 for women and 4/5 for men, depending on the context and screening goals [10,17,18].
In Denmark, the AUDIT and AUDIT-C are widely used in both primary and secondary healthcare and are recommended by the Danish College of General Practitioners and the Danish Health Authorities [19]. Despite the two instruments’ widespread use in Denmark, they have so far been validated only in a hospital setting [20].
The present study aimed to investigate the diagnostic properties of the Danish version of the AUDIT and the AUDIT-C in a Danish general population sample.
Methods
Design
The cross-sectional survey study used an anonymous online questionnaire. We collected data from 26 September to 29 October 2024.
Participants and procedure
Data collection
The Danish government-supported non-governmental organization “Alkohol & Samfund” (Alcohol & Society) [21] offers an anonymous online alcohol habits test based on the Danish language version of the AUDIT questionnaire. Independent of political, religious, and economic interests, the organization has a declared goal of changing the Danish alcohol culture into a culture that is not harmful.
Sample
Eligible participants included all respondents ⩾ 25 years of age on the “Alkohol & Samfund” online survey from 26 September to 29 October 2024. The questionnaire automatically redirects participants younger than 25 years to a separate questionnaire for young adults. The questionnaire required the participants to be proficient in written Danish, but we set no formal exclusion criteria.
Questionnaires
The online questionnaire comprised the following:
Demographic data on sex (female, male, other), years of age (25–34, 35–44, 45–54, 55–64, 65+), and region of residence (Region of Northern, Central, or Southern Denmark, Region of Zealand, or The Capital Region).
The Alcohol Use Disorders Identification Test (AUDIT) [6]: participants completed the Danish version of the AUDIT, a 10-item instrument measuring alcohol consumption, dependence, and related harm (score range 0–40). Items 1–8 use a five-point Likert scale (0–4), while items 9 and 10 offer three response options (scored 0, 2, or 4). This version was obtained from the Danish Health Authority and the Danish College of General Practitioners [19]. Notably, a formally validated Danish translation of the AUDIT has not yet been established.
Alcohol dependence criteria: we included self-report items corresponding to the six diagnostic criteria for alcohol dependence syndrome (F10.2) as defined in The International Classification of Diseases, 10th Revision (ICD-10) [22]. According to ICD-10, a diagnosis of alcohol dependence syndrome requires at least three of six symptoms to be present for one month or to have recurred over a 12-month period. The included items were non-diagnostic as they were self-reported and were phrased as questions, for example: “Within the past twelve months, have you consumed more and more alcohol to achieve the same effect as before?”.
Harmful use: this was assessed with one item adapted from ICD-10 F10.1 (harmful use): “Within the past year, have you, for at least a month or on several occasions, experienced physical or psychological harm from alcohol use, or noticed that your drinking has negatively affected your judgment?”, provided dependence is not considered present.
One question on the participant’s alcohol consumption in standard drinks (a Danish standard drink contains 12 g of alcohol) within the past week. Answer categories were: “None,” “1–10,” “11–20,” “21–30,” “31–40,” “41–50”, “51–60,” “61–70,” “70+.”
No additional alcohol-related items were included beyond those described above. Owing to the online format, all items required completion before submission, and therefore no item-level missing data were present.
Statistics
We described the study sample using descriptive statistics. We collapsed the age groups into three (25–44, 45–64, and 65+) and then conducted receiver operating characteristics (ROC) curve analysis of the AUDIT and AUDIT-C for the entire sample and stratified by sex and age groups. We used the Danish national recommendations for maximum weekly alcohol consumption as reference standard for hazardous use: >10 standard drinks per week (one standard drink = 12 g of alcohol) and the yes/no question on harmful use as indicator for harmful consumption. We defined possible dependence as ⩾3 self-reported ICD-10 criteria for alcohol dependence syndrome. The three outcomes were analyzed separately as independent reference standards and were not constructed as mutually exclusive hierarchical categories.
We assessed the area under the ROC curve (AUC) and diagnostic properties (sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and agreement) of the AUDIT and AUDIT-C according to hazardous use, harmful use, and possible dependence for the full sample and stratified by sex and age groups. Using Youden’s Index [23], we estimated optimal cut-off scores for AUDIT and the AUDIT-C in relation to harmful use, hazardous use, and possible dependence. Youden Index is sensitivity + (specificity-1) and takes values from 0 to 1. The maximal index denotes the optimal cut-off. Youden values of 50 and above are considered acceptable. We chose the Youden Index because it directly maximizes the sum of sensitivity and specificity, without requiring assumptions about the relative consequences of false positives and false negatives. While alternative approaches exist, such as cost-weighted optimization or minimizing the distance to the upper-left corner of the ROC curve, we did not apply them because our study did not define explicit weighting for misclassification error.
We conducted analyses in STATA [24] version 18.
Results
The sample consisted of 17,959 participants, mean age 66.32 (SD=12.72) years, with 51% males. Of the total sample, 3503 (19.5%) self-reported hazardous use (>10 standard drinks/week), 719 (4.0%) self-reported having harmful use but not three or more symptoms of dependence, and 1402 (7.8%) self-reported ⩾3 ICD-10 criteria for alcohol dependence syndrome indicative of dependence. The proportion of participants exceeding 10 standard drinks the previous week was highest in the age group 65+, while the average AUDIT and AUDIT-C scores were highest in the youngest age group (25–44 years) (Table I).
Participant characteristics, N=17,959.
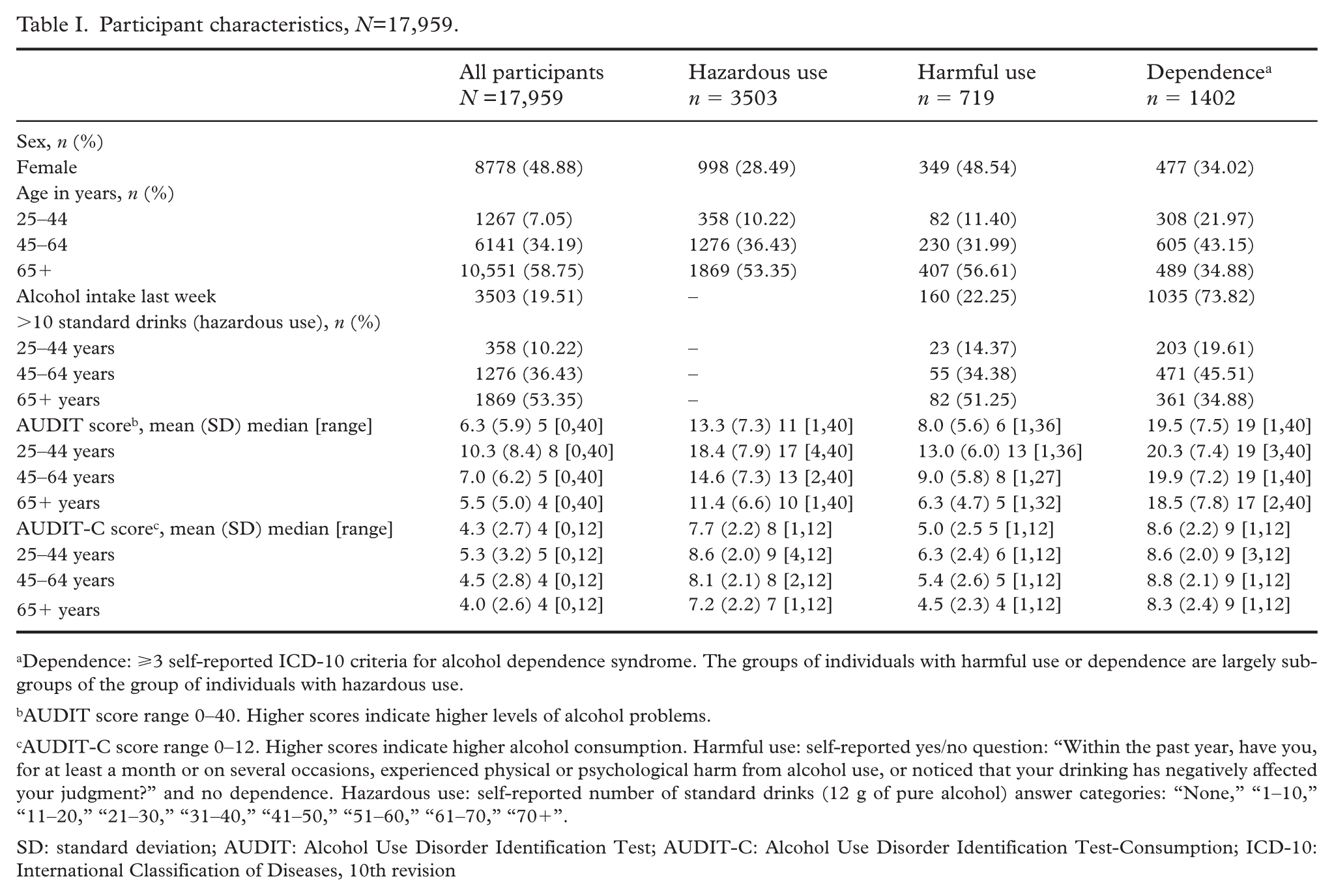
Dependence: ⩾3 self-reported ICD-10 criteria for alcohol dependence syndrome. The groups of individuals with harmful use or dependence are largely subgroups of the group of individuals with hazardous use.
AUDIT score range 0–40. Higher scores indicate higher levels of alcohol problems.
AUDIT-C score range 0–12. Higher scores indicate higher alcohol consumption. Harmful use: self-reported yes/no question: “Within the past year, have you, for at least a month or on several occasions, experienced physical or psychological harm from alcohol use, or noticed that your drinking has negatively affected your judgment?” and no dependence. Hazardous use: self-reported number of standard drinks (12 g of pure alcohol) answer categories: “None,” “1–10,” “11–20,” “21–30,” “31–40,” “41–50,” “51–60,” “61–70,” “70+”.
SD: standard deviation; AUDIT: Alcohol Use Disorder Identification Test; AUDIT-C: Alcohol Use Disorder Identification Test-Consumption; ICD-10: International Classification of Diseases, 10th revision
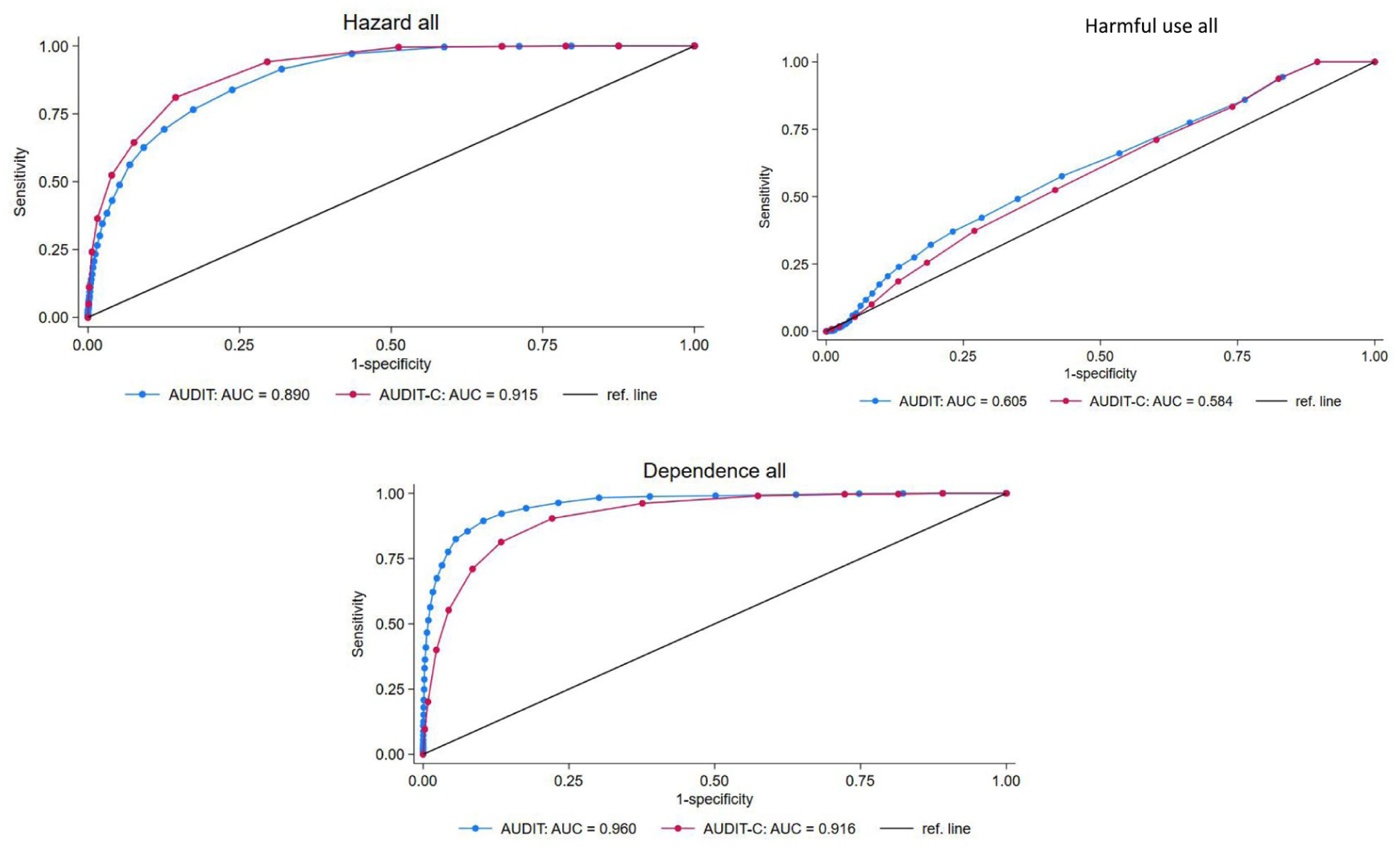
While the AUDIT showed good diagnostic performance for identifying hazardous use and possible dependence (AUC for hazardous = 0.89, AUC for dependence = 0.96), it was not able to reliably detect harmful use (AUC = 0.61); see Figure 1 and Supplemental material Table I online. Highest Youden’s J values on the AUDIT on the whole sample were estimated at 7 for hazardous use (Youden’s J=60, sensitivity 83.8 (95% confidence interval (CI) 82.6–85), specificity 76.2 (95% CI 75.5–76.9); PPV=46.1 (95% CI 44.8–47.3), NPV=95.1 (95% CI 94.7–95.5)), and 11 for dependence (Youden’s J=79.1, sensitivity 89.4 (95% CI 87.8–91), specificity 89.7 (95% CI 89.2–90.1); PPV=42.3 (95% CI 40.5–44.1), NPV=99.0 (95% CI 98.8–99.2)) (Figure 1 and Supplemental Table I).
Diagnostic properties of the Alcohol Use Disorder Identification Test (AUDIT) and the Alcohol Use Disorder Identification Test-Consumption (AUDIT-C) for hazardous use, harmful use, and possible dependence. N=17,959.
Similar to the full AUDIT, the AUDIT-C could not reliably detect harmful use (AUC=0.58) but showed good performance for identifying hazardous use (AUC=0.92) and dependence (AUC=0.92), although it was not able to distinguish between the two (see Figure 1 and Supplemental Table II). The cut-offs on the AUDIT-C for highest Youden’s J were estimated for the total sample at 6 for hazardous use (Youden’s J=66.5, sensitivity 81.02 (95% CI 79.71–82.3), specificity 85.54 (95% CI 84.97–86.11); PPV=57.6 (95% CI 56.2–59.0), NPV=94.9 (95% CI 94.5–95.3)), and also 6 for dependence (Youden’s J=68.3, sensitivity 90.37 (95% CI 88.78–91.86), specificity 77.89 (95% CI 77.25–78.52); PPV=25.7 (95% CI 24.5–27.0), NPV=99.0 (95% CI 98.8–99.1)) (Figure 1 and Supplemental Table II).
The AUDIT demonstrated strong internal consistency (Cronbach’s α = 0.83), while the AUDIT-C demonstrated moderate to low (Cronbach’s α = 0.61).
Stratified analyses
Stratified on sex and age, we observed similar patterns for both scales, with good to excellent diagnostic discrimination for hazardous use and possible dependence but none to poor discrimination for harmful use. In the sex-stratified analyses for the full AUDIT, highest Youden’s J scores were seen at cut-off scores of 6/8 (women/men) for detecting hazardous use and 10/13 for dependence (Supplemental Table III). For the AUDIT-C, highest Youden’s J scores in sex-stratified analysis were found at cut-offs of 5/6 (women/men) for hazardous use and 6/7 for dependence (Supplemental Table IV).
For the age stratified analyses, the highest Youden’s J scores for the full AUDIT for detecting hazardous use were found at cut-off score 11 among 25–44-year-olds, 9 among 45–64-year-olds, and 6 among 65+-year-olds. For dependence, the highest Youden’s J scores optimal were found at cut-off 12/13 in the youngest group, 12 in the middle-aged, and 10 in the oldest (Supplemental Table V). In the youngest group, the highest Youden’s J scores for the AUDIT-C were found at a cut-off score of 7 for both hazardous use and dependence. Among 45–64-year-olds, the highest Youden’s J scores were found at cut-off 6 for hazardous use and 7 for dependence. In the 65+ group, the highest Youden’s J scores were found at cut-offs 5 and 6, respectively (Supplemental Table VI).
Precision of the current consensus based cut-off scores
The currently most commonly used cut-off scores for AUDIT are 6 for women and 8 for men regarding hazardous use, 16 for both women and men regarding harmful use, and 20 indicating possible dependence [6,14]. In our sample, these cut-off scores performed as follows: hazardous use, women, cut-off 6: (Youden’s J=34.8, sensitivity 65.5 (95% CI 61.5–69.5 ), specificity 69.3 (95% CI 68.3–70.3); PPV= 12.3 (95% CI 11.2–13.6), NPV=96.8 (95% CI 96.4–97.3)). Hazardous use, men, cut-off 8: (Youden’s J=55.7, sensitivity 78.2 (95% CI 76.6–79.8), specificity 77.5 (95% CI 76.5–78.5); PPV= 56.6 (95% CI 54.9–58.2), NPV= 90.5 (95% CI 89.7–91.2)). Harmful use, all, cut-off 16: (Youden’s J=4.5, sensitivity 11.7 (95% CI 9.6–14.3), specificity 92.8 (95% CI 92.4–93.1); PPV= 6.3 (95% CI 5.1–7.7), NPV= 96.2 (95% CI 95.9–96.5)). Dependence, all, cut-off 20: Youden’s J=45.6, sensitivity 46.6 (95% CI 44.6–49.3), specificity 99.3 (95% CI 99.2–99.5); PPV= 85.7 (95% CI 83.2–88.1), NPV= 95.7 (95% CI 95.3–96)).
Discussion
The present study evaluated the diagnostic accuracy and sought to identify the optimal cut-off scores of the Danish version of the AUDIT and the AUDIT-C in a Danish general population sample of 25+-year-olds. Both instruments showed good to excellent accuracy in discriminating hazardous alcohol use and possible dependence but very poor ability to discriminate self-reported harmful use.
On the full AUDIT, results indicated a cut-off of 7 for hazardous use in general and found reasonable support for the commonly used cut-off scores 6 and 8 for women and men, respectively. Similarly, the commonly used cut-off score at 20 for detecting dependence performed well in the present study with specificity at PPV= 85.7 (95% CI 83.2–88.1) and NPV= 95.7 (95% CI 95.3–96)). It should, though, be noted that Youden’s J was only 45.6 for this cut-off point. The highest Youden’s J was seen at a cut-off as low at 11 for dependence. At this lower threshold, sensitivity increases, resulting in high NPV. This means that individuals scoring below the cut-off are unlikely to meet criteria for dependence, making the threshold useful for ruling out cases. However, the corresponding reduction in specificity leads to a lower PPV, and thus a substantial proportion of individuals scoring above the cut-off would not meet dependence criteria. It may be argued that sensitivity is more important than specificity when it comes to detecting dependence, but it might depend on the context for the screening. Importantly, PPV is dependent on the underlying prevalence of the condition in the screened population. Although the PPV for hazardous alcohol use at the recommended cut-off was 46.1%, this should be interpreted in light of the population prevalence. In a general population setting, where prevalence is moderate rather than high, a substantial proportion of individuals screening positive will not fulfill diagnostic criteria. This is an inherent property of screening instruments and does not reflect poor test performance per se. The Danish National Board of Health estimates that 5.3% of the general Danish population have a moderate alcohol problem and 0.9% have a serious alcohol problem based on another screening procedure—CAGE-C [25]. As AUDIT is intended as a screening rather than a diagnostic instrument, a moderate PPV might be acceptable if followed by clinical assessment when considered relevant. Further, the difference in time frames across consumption and diagnostic reference measures (AUDIT and ICD-10 criteria) might introduce some degree of temporal mismatch, which should be considered when interpreting screening performance.
In the literature there is less consensus about the optimal cut-off scores for AUDIT-C, and it is considered that the relevant cut-off probably is highly contextual and dependent of the aim behind the screening efforts [10,17,18]. In the present study, optimal cut-off scores on the AUDIT-C were estimated at 6 for hazardous use and 6 for possible dependence, when detecting self-reported hazardous use and dependence in a population that is curious about own alcohol habits and thus test themselves. While these thresholds suggest that the AUDIT-C can detect hazardous use/dependence but cannot distinguish between levels of alcohol use severity, its lower internal consistency (α = 0.61) compared with the full AUDIT (α = 0.83) might limit its reliability in detecting with precision and raise concerns about its use as a standalone screening tool. Although the AUDIT-C remains a practical option for time-limited settings, its lower internal consistency suggests that positive screens might warrant follow-up with the full AUDIT or additional assessments to ensure accurate identification of at-risk individuals and whether probable dependence is present or not.
One explanation for both scales’ very limited ability to detect harmful use in our sample might be the nature of the ICD-10 diagnosis of harmful use, which refers to a pattern of alcohol consumption that causes physical or mental harm to the individual but has not developed to dependence. Unlike alcohol dependence syndrome, it lacks specific criteria or examples [22]. This vagueness might make harmful use more difficult to identify reliably compared with hazardous use and possible dependence. Moreover, our data relied on a single self-reported questionnaire item to assess harmful use, whereas a structured diagnostic interview would have provided a more accurate classification. Another explanation might be that harmful use and dependence constitute a continuum with big overlap between the diagnoses—one of the reasons why the harmful use and dependence diagnoses have been combined in the fifth Diagnostic and statistical manual of mental disorders revision to the collective AUD.
Current World Health Organization (WHO) guidelines recommend considering lower thresholds in women and individuals over the age of 65 years [6]. Our findings align with these recommendations, as we observed lower optimal cut-offs across the oldest age group (65+) and for possible dependence in women. Notably, substantial cultural and contextual variability has been noted in the literature, emphasizing the need to tailor screening thresholds even more with consideration to the specific population and screening purpose [10,12,17,26]. For example, suggested cut-off for detecting possible dependence has ranged from 13 to 24 depending on the setting and study [10], challenging the feasibility of creating uniform international clinical guidelines. Compared with the WHO-recommended cut-off scores of 8, 16, and 20, we found lower threshold values for harmful use and dependence (cut-off = 11 in both cases), possibly reflecting these contextual influences. Another contributing factor might be the composition of our sample, which predominantly included older adults, who consistently demonstrated lower optimal cut-off scores, and excluded individuals younger than 25 years. Notably, previous studies have questioned the applicability of standard AUDIT thresholds in younger populations, due to the differences in drinking patterns between younger and older age groups [10,26].
Similar to the full AUDIT, recommended AUDIT-C cut-off scores vary depending on age, sex, setting, and the characteristics of the target population [17,26–29]. Overall and based on Youden’s J, we found higher cut-offs for AUDIT-C than usually recommended. It has previously been shown that cut-off scores for identification hazardous alcohol use vary with population, setting, country, and the format AUDIT-C is applied in [30]. In a setting like Denmark, with a liberal alcohol culture and where moderate daily drinking is widespread, a higher cut-off will be in better compliance with the official Danish safe limits for alcohol intake (10 drinks per week for both men and women). Importantly, national consumption recommendations and AUDIT screening cut-offs serve different purposes; the former are based on long-term epidemiological risk modeling, whereas the latter are empirically derived thresholds intended to optimize screening performance.
For the sex- and age-specific AUDIT-C cut-offs, we found slightly lower optimal thresholds in women (cut-off 5 for hazardous use and 6 for dependence) compared with men (6 for hazardous, 7 for dependence). A similar pattern was observed in the oldest age group (65+ years), which demonstrated lower optimal cut-offs across all categories (see Supplemental Table VI). These findings highlight the importance of tailoring screening thresholds with the targeted population and the purpose of the screening. Given the limited reliability of the AUDIT-C in detecting harmful use and generally low PPVs across all three categories, the instrument appears more suitable for ruling out cases rather than confirming them in a general population setting. This is consistent with its relatively high specificity and negative predictive values. Positive screens might therefore require further assessment using more comprehensive tools such as the full AUDIT. However, as the present study was conducted in a general population sample, the applicability of such a stepped approach in clinical settings requires further validation.
Limitations
Data were collected via the Danish non-governmental organization on prevention of alcohol-related harms in the society “Alkohol & Samfund” homepage. This webpage attracts primarily Danish-speaking citizens, with a concern or interest in their own drinking patterns. Consequently, the cohort is affected by selection bias and does not represent the average Danish background population. Our sample is also challenged by lack of data from younger adults, as the webpage redirects individuals younger than 25 years of age to an alternative questionnaire for young adults. The smaller sample size in the youngest age group reflects a self-selected subset of the population, limiting the generalizability of findings to younger adults. Furthermore, it is a limitation that the data are collected anonymously. We cannot rule out that some individuals might have filled in the questionnaire several times, and some might have filled in the questionnaire on behalf of, for example, a relative or friend based on assumptions.
It is also a limitation that the diagnoses harmful alcohol use and dependence are based on self-reported data and not based on clinical interviews. Likewise, harmful use was based on self-reports of a single yes/no items and analyzed among those that did not self-report dependence. We could not perform a time-line follow back interview [31], which is usually considered gold standard. Finally, the cross-sectional design of the study restricted our ability to examine longitudinal changes in alcohol consumption and test–retest reliability of the AUDIT and AUDIT-C measures.
Despite these limitations, the size of the dataset and the broadness of the respondents may be considered a strength.
Conclusion
In a Danish general population sample aged 25 years and older, both the AUDIT and AUDIT-C demonstrated good diagnostic accuracy for detecting hazardous alcohol use and possible dependence but limited ability for detecting harmful use. The AUDIT exhibited high internal consistency, while the AUDIT-C exhibited low. Given its brevity and high specificity, the AUDIT-C might be useful as an initial screening tool to rule out cases, while positive findings might warrant further assessment with the full AUDIT. However, the applicability of this approach in clinical settings requires further validation. Local circumstances are necessary to consider in defining appropriate cut-off points for both AUDIT and AUDIT-C.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261457731 – Supplemental material for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT)
Supplemental material, sj-docx-1-sjp-10.1177_14034948261457731 for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT) by Peter N. Schøler, Kjeld Andersen, Maja Thiele, Ulrik Becker, Erik Christiansen and Anette S. Nielsen in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-2-sjp-10.1177_14034948261457731 – Supplemental material for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT)
Supplemental material, sj-docx-2-sjp-10.1177_14034948261457731 for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT) by Peter N. Schøler, Kjeld Andersen, Maja Thiele, Ulrik Becker, Erik Christiansen and Anette S. Nielsen in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-3-sjp-10.1177_14034948261457731 – Supplemental material for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT)
Supplemental material, sj-docx-3-sjp-10.1177_14034948261457731 for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT) by Peter N. Schøler, Kjeld Andersen, Maja Thiele, Ulrik Becker, Erik Christiansen and Anette S. Nielsen in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-4-sjp-10.1177_14034948261457731 – Supplemental material for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT)
Supplemental material, sj-docx-4-sjp-10.1177_14034948261457731 for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT) by Peter N. Schøler, Kjeld Andersen, Maja Thiele, Ulrik Becker, Erik Christiansen and Anette S. Nielsen in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-5-sjp-10.1177_14034948261457731 – Supplemental material for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT)
Supplemental material, sj-docx-5-sjp-10.1177_14034948261457731 for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT) by Peter N. Schøler, Kjeld Andersen, Maja Thiele, Ulrik Becker, Erik Christiansen and Anette S. Nielsen in Scandinavian Journal of Public Health
Supplemental Material
sj-docx-6-sjp-10.1177_14034948261457731 – Supplemental material for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT)
Supplemental material, sj-docx-6-sjp-10.1177_14034948261457731 for Danish validation of the Alcohol Use Disorder Identification Test (AUDIT) by Peter N. Schøler, Kjeld Andersen, Maja Thiele, Ulrik Becker, Erik Christiansen and Anette S. Nielsen in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank The Novavi Foundation for unconditional funding.
Ethical considerations
This study was not eligible for application to the Danish National Research Ethics Committee according to national regulations Section 14;2 of the Danish Act on Research Ethics Review of Health Research Projects.
Consent for publication
Not applicable.
Author contributions
Author eligibility adheres to Vancouver recommendations. PNS: study conceptualization, study planning and design, drafting of the manuscript, draft of figures and tables. KA: study conceptualization, study planning and design, manuscript editing. UB: study conceptualization, study planning and design, manuscript editing. MT: study conceptualization, study planning and design, manuscript editing. EC: analysis, manuscript editing. ASN: funding acquisition, study conceptualization, study planning and design, manuscript editing. All authors approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an unconditional grant from the Novavi Foundation. The funder had no role in the conduct, analysis, interpretation, reporting, or presentation of the work. MT is funded by a grant from the Novo Nordisk Foundation (NNF20OC0059393).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.