
Abstract
Background and aims:
Gambling problems impact not only individuals who gamble but also those closely associated with them, referred to as concerned significant others (CSOs). Many of the harms experienced by individuals who gamble also affect CSOs. These include negative economic consequences and physical and mental health problems (e.g. depression and anxiety). This study aimed to estimate the prevalence of CSOs affected by gambling at the population level in Sweden and to describe the characteristics of CSOs.
Methods:
The data were derived from a survey conducted on a nationally representative sample of the Swedish population. The initial sample comprised 27,000 individuals aged 17–84 years living in Sweden. The response rate was 36.8%, resulting in an analytical sample of 9819 respondents. The study had a cross-sectional design, and Poisson regression models with robust error variance were applied to assess associations.
Results:
A total of 5.5% of the sample reported being a CSO of an individual who gambled during the past 12 months. No significant sex differences were found. An age gradient was observed, with older adults (aged 50–84 years) being less likely to report being a CSO. CSOs had higher scores on the Problem Gambling Severity Index and were more likely to report heavy episodic drinking, daily smoking and drug use during the past year. They also reported poorer health than non-CSOs. When comparing all CSOs with those who reported negative consequences of being a CSO, we found higher risks of problem gambling, daily smoking and poor health among those reporting negative consequences.
Conclusions:
Introduction
Despite providing enjoyment for many people, existing research consistently highlights the strong association between gambling and a range of negative consequences, such as financial difficulties, increased anxiety and symptoms of depression [1–3]. Although previous studies have primarily focused on gamblers and the challenges they experience, a growing body of research is now examining the experiences of concerned significant others (CSOs). This shift in perspective, which extends the focus from individual gamblers to their immediate and broader social networks, mirrors a similar development in alcohol research [4].
The financial, social and psychological burden experienced by problem gamblers (PGs) is undoubtedly stressful for the individual. However, a growing body of literature highlights that this burden is also transferred to family members and others in close relationships with them. For instance, a widely cited study by Goodwin et al. [5] estimated that a typical PG in Australia affects six other individuals. As the authors acknowledge, a limitation of the study is that it does not clearly define which aspects or the extent to which they are affected.
First, it is important to distinguish between clinical and general population studies in research on CSOs of individuals with gambling problems. Previous research has focused on clinical populations and the harms experienced by CSOs. Clinical studies are typically conducted in treatment settings and involve participants who are actively seeking help or receiving treatment for gambling-related problems. This approach offers several advantages, including a more comprehensive understanding of the individual with gambling problems, encompassing medical history, gambling patterns, high-risk situations and related factors. It also facilitates a more nuanced characterisation of CSOs within this specific clinical context. However, as highlighted in a recent review by Tulloch et al. [6], research based on clinical samples often employs a narrow definition of CSOs, focused primarily on partners or spouses. As clinical samples predominantly exhibit a sex bias towards men, CSOs are usually women. As noted by Dowling et al. [3], this sex bias reflects cultural views of gambling as a masculine activity. Several authors have argued that there is a need for large-scale population-based studies of CSOs of gamblers to further understanding of gambling-related problems [3,6]. In addition, few individuals with gambling problems seek help, making the clinical population a non-representative minority, which may introduce bias [7].
Previous population-based studies of CSOs of individuals with gambling problems have reported prevalence rates ranging from 2% to 18% [6]. This variability can largely be attributed to methodological differences between studies. Some investigations have adopted a more restrictive definition of CSOs, limited to family relationships and ‘close friends’ [9], whereas others have employed a broader operationalisation, encompassing individuals described as ‘someone close’ [8,9]. In addition to the type of relationship, the timeframe used is also important. Lifetime estimates are generally higher than current estimates [3]. Some studies have examined the stability of CSO prevalence over time. Salonen et al. [10] estimated prevalence over a four-year period and found that it remained relatively stable over time. However, the proportion of affected family members increased. Svensson et al. [9] found that close to half of the sample (47%) were no longer affected one year later. These studies indicate that the population of CSOs might not be stable over time. A potential limitation of both studies is their reliance on lifetime exposure to problem gambling.
With regard to the harms experienced by CSOs, most studies have found that they are more likely than non-CSOs (i.e. those who do not report having a significant other who gambles excessively) to experience a range of adverse outcomes. These include financial hardship, relationship problems, poorer psychological and physical well-being, higher rates of smoking and higher levels of hazardous alcohol consumption [6,8,9,11–13]. In addition, Salonen et al. [14] found that psychological and relational-related harms were particularly common among female CSOs. Most studies also indicate that females are at greater risk of being CSOs of gamblers, reflecting the fact that individuals with gambling problems are more often male (see, e.g., Salonen et al. [8]). Other studies have focused on the children of individuals with gambling problems. However, the findings do not indicate a clear association. Some studies suggests that children of individuals with gambling problems may be more likely to developing gambling problems themselves [15,16]. Conversely, a qualitative study found that adult children who had been exposed to a parent with gambling problems during childhood were less likely to engage in gambling [17].
Most studies on CSOs of gamblers have been conducted in English-speaking Western countries, with relatively limited attention paid to family-oriented cultures [3]. This is also important when making comparisons between countries. The present study focuses on the Swedish context. To our knowledge, only one study has been conducted in Sweden on CSOs in the general population, and it was based on data collected in 2008–2009 [9]. That study found that both male and female CSOs had poorer mental health and more hazardous alcohol consumption than the general population. With regard to problem gambling, male CSOs had an increased risk, whereas no such association was found among females. Furthermore, most associations remained one year later. It should be acknowledged that these findings are based on a broad definition of CSOs – namely, whether respondents reported having someone close to them who had, or had previously had, problems with gambling. Additionally, the Swedish Public Health Agency published a compilation of prevalence tables from the Swedish Longitudinal Gambling Study (SWELOGS) [18]. In that study, 11% reported having someone close to them who had experienced a gambling problem during the past year. Of these, 3.8% reported that the person was a family member or member of their immediate family, 5.4% reported a friend and 3.0% reported someone from their workplace, school or a similar setting.
One interpretation of these results, given the definition of CSOs, is that the observed outcomes may not be caused by being a CSO per se. Alternatively, the findings may reflect persistent consequences of being a CSO. It should also be noted that socio-economic status (SES) has rarely been accounted for in studies of CSOs of gamblers, including the present study. The observed associations may be influenced by SES, as less advantaged groups consistently exhibit higher rates of unhealthy behaviours and disease [19,20].
Since the publication of the previous Swedish study, several legislative changes have altered the Swedish gambling market. The most significant change was the transition from a monopoly system to a licence-based system in 2019 [21]. The Swedish Gambling Authority issues approximately 50–60 licenses annually to companies operating in the Swedish gambling market. Several legislative changes have also been introduced regarding the treatment of gambling-related problems.
As Sweden has undergone a re-regulation of its gambling market, it is important to examine whether this has influenced the prevalence of CSOs and other risk factors previously associated with this group. In addition, the gambling landscape is highly dynamic, with new forms of gambling continuously emerging. This necessitates ongoing monitoring and population-level investigations of gambling behaviour and affected populations. Against this background, there is a need to examine the association between CSO status and health and lifestyle factors in the Swedish population in order to update knowledge about CSOs in Sweden. Such knowledge is important for understanding the scope of the problem and for comparing findings from Sweden with those from other countries.
Aim
The primary objective of this study was to improve understanding of CSOs affected by gambling from a population-based perspective in Sweden. Specifically, the study aimed to estimate the prevalence of CSOs of gamblers and the proportion of CSOs who report experiencing negative consequences. Furthermore, the study examined whether CSOs of gamblers report poorer physical and psychological health, as well as more health-risk behaviours—such as their own gambling, alcohol consumption, drug use and smoking—compared with non-CSOs. These analyses were conducted while controlling for SES and age.
Methods
Data collection
The data were derived from the Swedish Habits and Consequences Survey [22], a cross-sectional population-based survey focusing on alcohol, tobacco, drug use and gambling habits. The original sample included 27,000 individuals aged 17–84 years (born 1937–2004) and registered in Sweden. The sample was drawn from the Swedish state personal address register (ref). The response rate was 36.4%, resulting in a study sample of 9819 individuals. Data were collected between March and June 2021. Respondents were contacted by mail and asked to complete either a paper-and-pencil questionnaire or an identical web questionnaire. In the final sample, 52.1% responded via the paper-and-pen questionnaire and 47.9% via the web questionnaire.
Outcome measures
Three study-specific questions were used to assess CSO status and related negative consequences. First, respondents were classified as CSOs if they answered ‘yes’ to the question: ‘Is there someone in your life or in your surroundings that you consider to gamble too much on games involving money, during the last 12 months?’ Second, respondents were asked about their relationship to that person (e.g. a partner, parent or child) to that person. Respondents could indicate more than one relationship type. Third, to assess whether respondents had experienced any negative consequences as a result of being a CSO, they were asked: ‘Has that person’s/those people’s gambling affected you negatively in some way, during the last 12 months?’ The response alternatives were ‘yes’ and ‘no’.
Exposure measures: detrimental lifestyle habits
The following variables were used to measure the respondents’ own alcohol, drug and gambling behaviours during the past 12 months: gambling during the past year (yes/no), alcohol consumption during the past year (yes/no), drug use during the past year (yes/no) and non-medical use of prescription drugs during the past year (yes/no). Drug use was defined as the use of at least one of the following substances: cannabis, amphetamine, opiates, hallucinogens, ecstasy and cocaine. Non-medical use of prescription drugs was defined as the use of at least one medicine classified as a narcotic (painkillers, sedatives, tranquillisers or stimulants) without a prescription or at a higher dose or greater frequency than prescribed. Daily smoking (yes/no) was also included. In addition, monthly heavy episodic drinking (HED; yes/no) was assessed and defined as consuming at least one bottle of wine, or an equivalent amount of alcohol, on at least one occasion per month.
Problem gambling was assessed using the nine-item Problem Gambling Severity Index (PGSI) [23]. The nine items assess gambling behaviour during the past 12 months. Each item is scored from 0 to 3, resulting in a total score ranging from 0 to 27. PGSI scores were categorised into four levels of gambling severity: non-PG (score 0), low-risk gambler (score 1–2), moderate-risk gambler (score 3–7) and PG (score 8 or more). Respondents with missing information on any of the nine items were coded as non-PG.
Exposure measures: health status
Health status was assessed using three self-rated questions capturing general health, mental well-being and physical well-being. Respondents were asked: ‘How do you rate your general health / mental well-being / physical well-being?’ Response options were ‘very good’, ‘good’, ‘fair’, ‘bad/poor’ and ‘very bad / poor’. The response options ‘good’ and ‘very good’ were combined into a single category (‘good’), whereas the remaining options were combined into a second category (‘not good’).
Covariates
To account for potential confounding, the following covariates were included in the analyses: sex (men/women), age group (17–29, 30–49, 50–64, 65–84 years), educational level (compulsory education or no formal education, upper secondary education, tertiary education), country of birth (Sweden, another Nordic country, another European country, country outside Europe) and monthly income before tax, measured in thousands of SEK and categorised into quintiles, with approximately 20% of the sample in each quintile.
Statistical analyses
Descriptive statistics (percentages and means) were used to describe the study sample and the distribution of CSO status and CSO-related negative consequences. In all analyses, respondents with missing values on relevant variables were excluded. Poisson regression models with robust error variance [24] were used to assess the associations between CSO status, CSO-related negative consequences, detrimental lifestyle habits and health status. In analyses of CSOs experiencing negative consequences, the reference category comprised non-CSOs and CSO who did not report negative consequences. Results are presented as relative risks (RRs) with corresponding 95% confidence intervals (95% CIs). Model 1 presents crude estimates, whereas Model 2 was adjusted for socio-demographic variables. For analyses of health status, Model 3 was additionally adjusted for respondents’ lifestyle risk factors. A sample weighting procedure based on sex and age group was used to account for the probability of selection and to adjust for potential non-response bias. All analyses were performed in Stata version 16.
Ethical considerations
The Habits and Consequences (VoK) study received ethical approval from the Swedish Ethical Review Authority (Etikprövningsmyndigheten; decision number 2020-06508).
Results
Descriptive statistics for the sample are presented in Table I. Regarding sociodemographic characteristics, the sample had an approximately equal sex distribution, with 50.5% women. There was an overrepresentation of respondents aged 30–49 years (33.5%) and of those with tertiary education (48.5%). Furthermore, 85.5% of the sample were born in Sweden and 8% were born outside Europe. Of particular interest is the distribution of PGSI categories in the sample. Compared with estimates from the Swedish Longitudinal Gambling Study (SWELOGS) in 2021, the sample had a slightly higher proportion of moderate-risk gamblers (1.2%), but slightly lower proportions of low-risk gamblers (2.7%) and PGs (0.3%). In the 2021 SWELOGS sample, the corresponding estimates were 3.0% for low-risk gamblers, 0.8% for moderate-risk gamblers and 0.5% for PGs [18]. Furthermore, 5% of the sample were daily smokers and 3.6% had used drugs during the past year. Both estimates were similar to those reported in the Swedish Public Health Survey, which found that 3.0% had used drugs and 6% were daily smokers.
Sample characteristics.
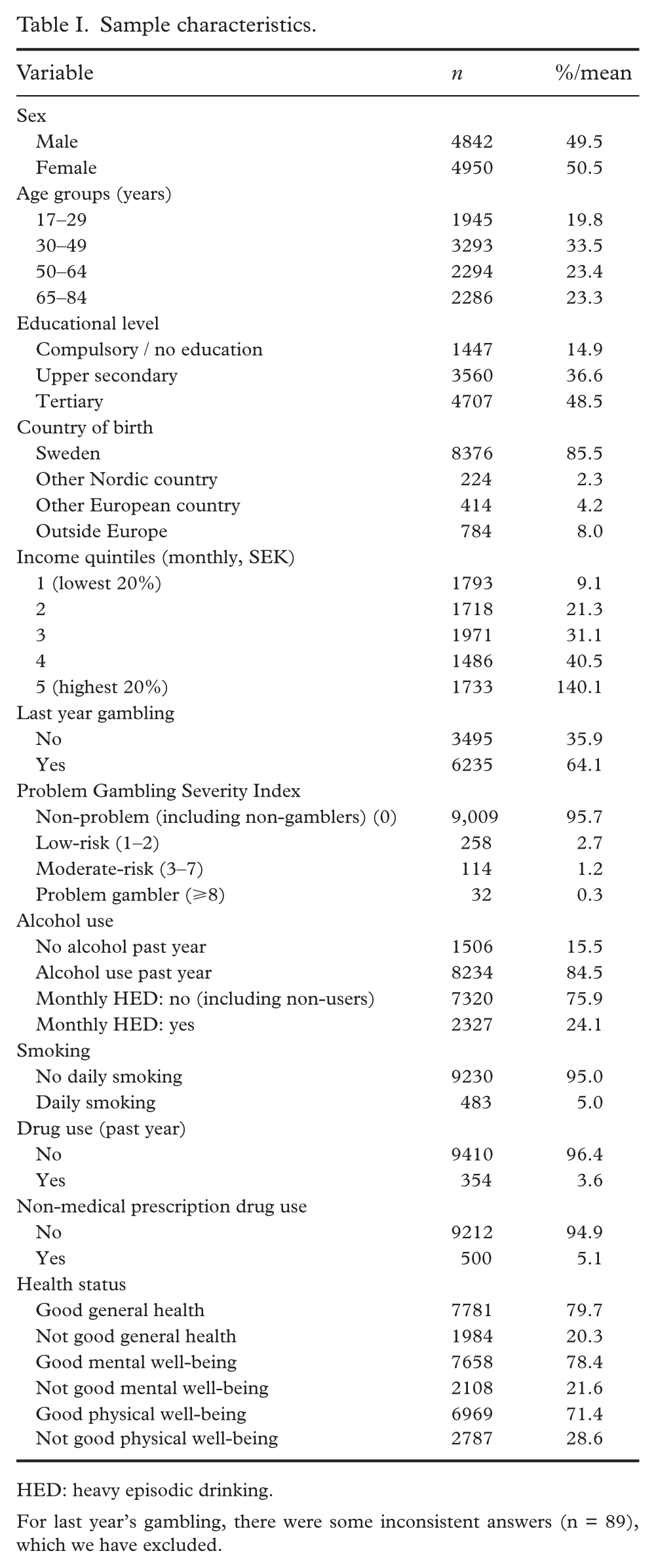
HED: heavy episodic drinking.
For last year’s gambling, there were some inconsistent answers (n = 89), which we have excluded.
Table II, presents the proportion of CSOs by relationship to the gambler and the proportion reporting negative consequences. About 5.5% reported having someone in their life or surroundings whom they consider to gamble too much, and 1.3% reported experiencing negative consequences as a result of that person’s gambling. The majority of CSOs were friends of the gambler, whereas 0.9% reported a parent, 0.8% a partner and 0.6% another family member who gambled too much.
Concerned significant others in the study sample, by relation to the gambler, and concerned significant others reporting negative consequences.
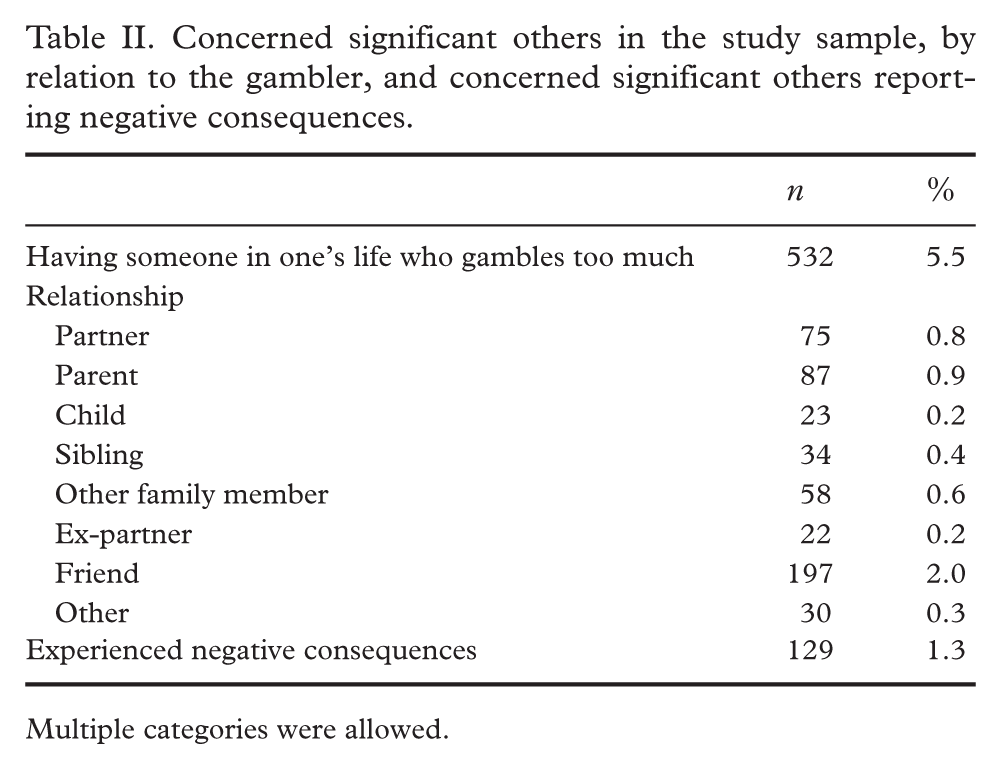
Multiple categories were allowed.
As shown in Table III, CSOs and CSOs who experienced negative consequences exhibited higher levels of detrimental lifestyle habits than non-CSOs. For instance, 2.2% of CSOs and 3.4% of CSOs who experienced negative consequences were classified as PGs, compared with 0.2% of non-CSOs. Moreover, CSOs were more likely to report monthly HED (35.1% and 23.7%, respectively, compared with 23.1%), daily smoking (7.3% and 10.2%, respectively, compared with 4.8%), drug use during the past year (9.2% and 9.8%, respectively, compared with 3.3%) and non-medical use of prescription drugs (6.6% and 9.1%, respectively, compared with 5.0%). CSO and the CSOs who experienced negative consequences also reported poorer overall health, mental well-being and physical well-being.
Distribution (%) of detrimental lifestyle habits and health status among non-CSOs, CSOs and CSOs experiencing negative consequences.
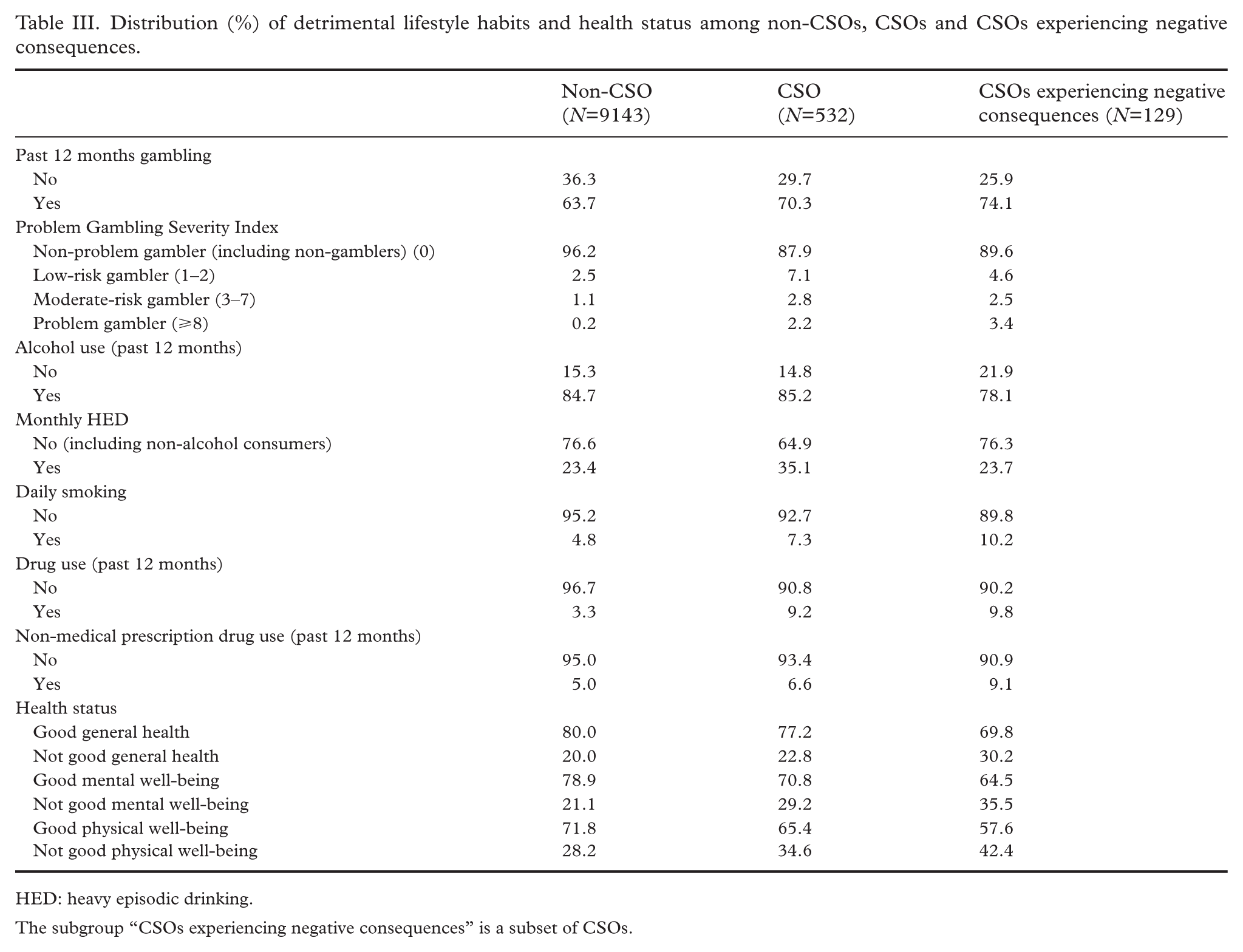
HED: heavy episodic drinking.
The subgroup “CSOs experiencing negative consequences” is a subset of CSOs.
The associations, expressed as RRs, between lifestyle habits and health status and whether these differ between CSOs and CSOs experiencing negative consequences from others’ gambling, are presented in Table IV. In Model 1 (crude estimates), we found a significantly increased risk among CSOs of having gambled during the past year (RR=1.28, 95% CI 1.06–1.56), being classified as a low-risk gambler (RR=2.86, 95% CI 2.00–4.09), a moderate-risk gambler (RR=2.75, 95% CI 1.57–4.82) and a PG (RR=7.7, 95% CI 4.50–13.1). A significantly increased risk among CSOs was also observed for monthly HED (RR=1.68, 95% CI 1.39–2.03) and daily smoking (RR=1.57, 95% CI 1.13–2.18).
Associations (RR, 95% CI) between detrimental lifestyle habits, health status and CSOs and CSOs experiencing negative consequences from others’ gambling.
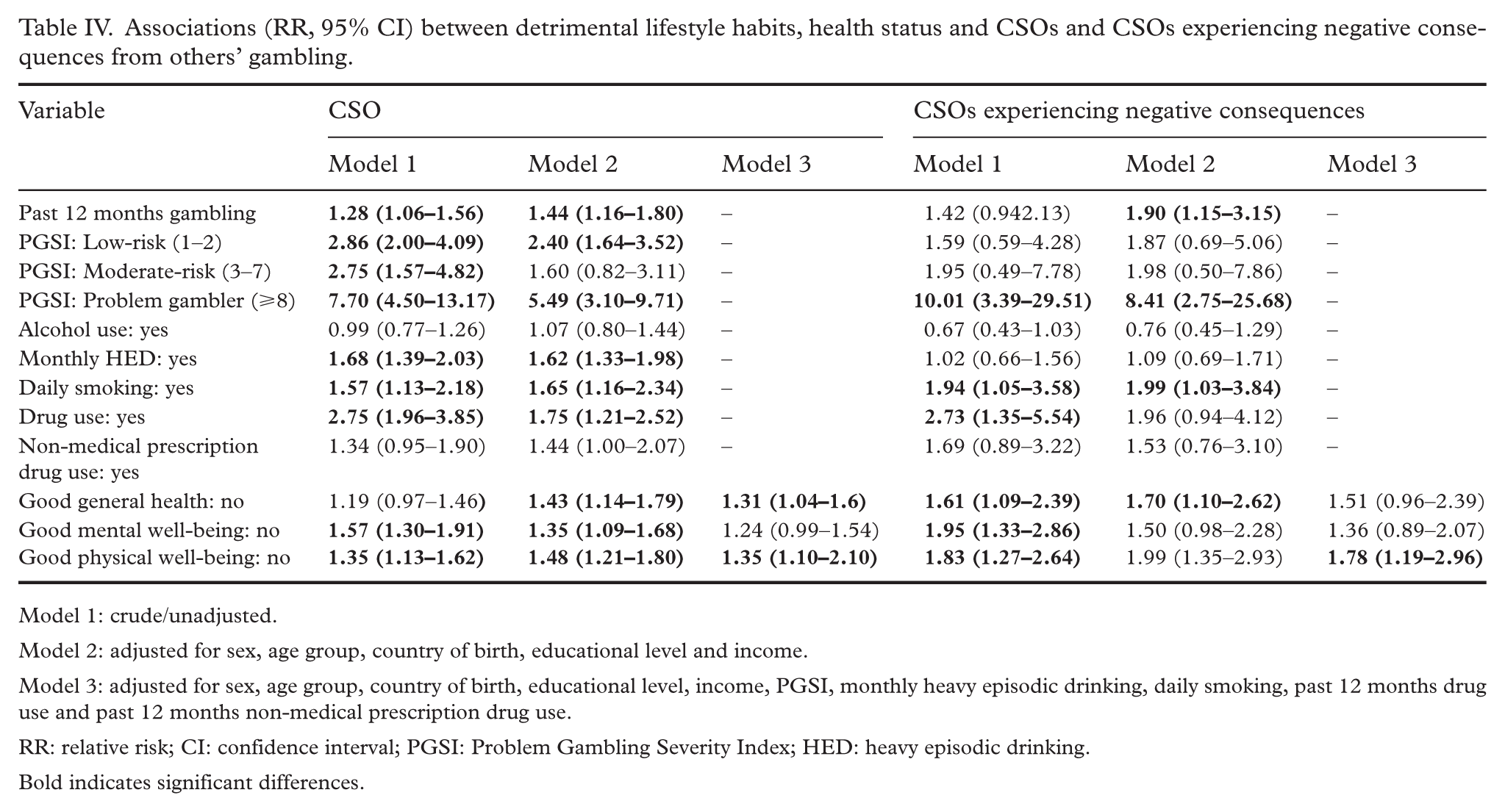
Model 1: crude/unadjusted.
Model 2: adjusted for sex, age group, country of birth, educational level and income.
Model 3: adjusted for sex, age group, country of birth, educational level, income, PGSI, monthly heavy episodic drinking, daily smoking, past 12 months drug use and past 12 months non-medical prescription drug use.
RR: relative risk; CI: confidence interval; PGSI: Problem Gambling Severity Index; HED: heavy episodic drinking.
Bold indicates significant differences.
In Model 2, where estimates were adjusted for sex, age group, country of birth, educational level and income, the pattern was very similar. The only estimate that became non-significant was moderate-risk gambling.
In Model 3, we adjusted for all the above socio-demographic variables and lifestyle factors (gambling, alcohol consumption, smoking, and drug use). In this model, we still found a significant association between CSOs compared with non CSOs (general health: RR=1.61, 95% CI 1.09–2.39; physical well-being: RR=1.83, 95% CI 1.64–2.64).
When comparing CSOs with CSOs who reported experiencing negative consequences, we found an elevated and significant risk of problem gambling (RR=10.01, 95% CI 3.39–29.51), daily smoking (RR=1.94, 95% CI 1.05–3.58), drug use during the past year (RR=2.73, 95% CI 1.35–5.54) and health outcomes, including general health (RR=1.61, 95% CI 1.09–2.93), mental well-being (RR=1.95, 95% CI 1.33–2.86) and physical well-being (RR=1.83, 95% CI 1.27–2.64).
Discussion
This study aimed to increase knowledge about CSOs affected by gambling from a population perspective. More specifically, we examined whether CSOs of individuals with gambling problems report poorer physical and/or mental well-being and other related factors compared with non-CSOs. The results show that CSOs had a higher prevalence of several adverse outcomes, including poorer physical and mental well-being, higher levels of HED, daily smoking, drug use during the past year and non-medical use of prescription drugs. Furthermore, CSOs who experienced negative consequences are at higher risk of adverse outcomes themselves, including problem gambling and poorer physical and mental well-being. In the multivariate analysis, adjusting for socio-demographic factors, most associations remained. Importantly, both CSOs and CSOs experiencing negative consequences were associated with a higher risk of gambling during the past year and problem gambling (PGSI⩾8).
The results support previous reviews of CSOs, which have reported several negative consequences, including both physical and psychological harms [1]. Our findings from a population-based study partially corroborate previous research and further specify the types of problems experienced by a large cohort of CSOs both at the time of answering the questionnaire and during the previous year.
Another important finding is that CSOs of individuals with gambling problems have a lower SES than CSOs whose significant others do not experience problem gambling. One practical implication of the study is that resources are needed to support CSOs of individuals with problem gambling, as there appears to be a substantial financial strain in this group. Although this finding may appear intuitive, a more comprehensive understanding of CSOs’ SES is important when designing prevention and treatment interventions. This is consistent with the review by Irie and Kengo [3] and has been supported by more recent studies.
One way of conceptualising our findings is to view the presence and risk of adverse consequences as a continuum. At one end of this continuum are non-CSOs, who have a lower level of adverse consequences, regardless of gambling involvement or relationship type. However, when comparing CSOs without negative consequences with those who reported negative consequences, the likelihood of adverse outcomes increases substantially. This pattern also appears to be related to the nature of the relationship with the gambler, with friendship being associated with fewer negative consequences.
Although the association between having a close relationship with an individual with problem or at-risk gambling and adverse outcomes may be expected, a notable finding in our study is the higher level of alcohol consumption among CSOs. The may reflect coping mechanisms in response to negative emotions arising from the relationship. This is a hypothesis that should be explored in future studies. The findings regarding HED are consistent with an Australian study in which CSOs reported more binge-drinking episodes [25].
An important consideration is the type of support CSOs may need to manage their situation and reduce or mitigate adverse consequences. In a Swedish study, CSOs generally sought help to manage their financial situation and to better understand how to encourage individuals with gambling problems to seek treatment or other forms of support [26]. When designing interventions to reduce adverse consequences for CSOs, it is important to consider addressing alcohol consumption, gambling involvement among CSOs and overall health, including smoking. However, there is a need to differentiate between types of CSOs when developing effective interventions.
The results regarding CSOs of individuals who gamble are similar to findings in alcohol research. Several studies have found that CSOs of individuals with alcohol problems are themselves alcohol dependent or heavy drinkers [27,28]. This is in line with the results of our study; however, there is one important difference. Studies focusing on CSOs of individuals with alcohol problems often report that women are more exposed to harm from a known person, whereas we did not observe the same pattern in relation to gambling.
Overall, this suggests commonalities between CSOs of individuals who gamble and CSOs of individuals with alcohol problems. One interpretation is that adverse consequences among CSOs are not solely related to a specific addictive behaviour but may instead extend beyond particular types of addiction and be shared across different addictive behaviours.
Practical implications
There are several practical implications of the findings. One important implication is that CSOs of individuals with gambling problems need access to support services to manage their own adverse outcomes. More preventive interventions targeting CSOs of individuals with gambling problems should be made available. The similarity between our findings and those from alcohol research may help to conceptualise what types of interventions may be useful. Several studies have examined interventions aimed at reducing harm among CSOs of individuals with alcohol problems [29,30], and approaches used in this area may also be applicable to CSOs of individuals with gambling problems.
Another practical implication is the need to differentiate between different groups of CSOs. The risk of adverse consequences appears to differ between friends of individuals with gambling problems and close relatives. There is therefore a need to broaden the discourse on CSOs of individuals with gambling problems and to recognise that different groups may have distinct needs and experiences rather than treating CSOs as a homogeneous population. Future studies should examine this further and clarify distinctions between different types of CSOs. However, one challenge is that the population of individuals with problem gambling is relatively small, and the CSO population is even smaller, which limits the feasibility of large-scale studies with sufficiently large CSO samples.
Limitations
One important limitation of the study concerns the definition of CSO status. This definition may have led to either an overestimation or underestimation of the number of CSOs in the sample. Consequently, the prevalence of CSOs in this study should be interpreted with caution. As multiple definitions of CSOs are used in the literature, caution is also warranted when comparing results across studies.
Another important limitation of the present paper is the cross-sectional design, which precludes casual inference. This is particularly relevant because many of the observed associations may predate CSO status. For instance, it is likely that respondents had gambled excessively, engaged in HED or were daily smokers before becoming CSOs, even though the questionnaire refers to a one-year period. We cannot rule out reverse causality; that is, respondents’ own gambling behaviour may contributed to their involvement with a person with gambling problems. A longitudinal design would be better suited to addressing causal relationships.
Another limitation is the response rate of 36.8%, which is borderline acceptable. However, in terms of representativeness, the PGSI distribution is very similar to that reported in other Swedish population studies [18]. Another potential limitation concerns recall bias. Participants were asked to report gambling and other behaviours that may be difficult to recall accurately. Previous studies have also shown that individuals who gamble may have difficulties accurately estimating gambling losses [31]. Social desirability bias may also have influenced responses. It is difficult to determine the extent to which these limitations have affected the results; however, findings should be interpreted with appropriate caution.
Future research
Future research should focus on longitudinal studies in which CSOs are followed over several years in order to understand how their level of risk changes and which factors contribute to these changes. These processes should also be examined using qualitative methods. Since prevalence and access to gambling differ across countries, there is a need for studies that map CSOs internationally in order to understand whether different jurisdictions experience different types of CSO-related problems.
Conclusions
Prevention and treatment of gambling problems should not only target individuals with gambling problems but should also include CSOs, due to the negative consequences they experience. These include a higher risk of problem gambling, HED, daily smoking, drug use and poorer overall health. The type of relationship is also important in this context. Friends of individuals with gambling problems have a lower risk than CSOs with closer relationships to the individual with gambling problems. Overall, treatment and support need to be available to CSOs in general, and there is also a need for more tailored interventions for different types of CSOs based on their relationship to the individual with gambling problems as well as their risk profile.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by Svenska Spels oberoende forskningsråd (Swedish Gambling Independent Research Council), grant FO2022-0007.