
Abstract
Aims:
The climate in Europe is warming, and the population is ageing faster than on other continents. These concurrent trends present significant challenges for social, economic and ecological sustainability of health care systems. This systematic scoping review examines how non-optimal air temperatures are associated with health care utilization among older populations in Europe.
Methods:
We screened peer-reviewed articles from six databases (MEDLINE, Science Direct, Web of Science, Scopus, ProQuest and GreenFILE) published in English during 2000–2024. The key search terms were air temperature, older people, health care services and Europe. We screened 1794 articles, reviewed 144 full-texts and extracted data from 52 articles. Of the included articles, 29 (56%) focused on heat exposure, 10 (19%) on cold exposure and 13 (25%) on both.
Results:
A positive association between non-optimal air temperature and health care use was found in 43 (38%) of heat-related and 30 (48%) of cold-related analyses. Emergency hospital admissions were the most frequently examined type of health care service, with cardiovascular and respiratory conditions being the primary causes. The strongest evidence of positive associations was observed for respiratory conditions in emergency hospitalisations and for cardiovascular hospitalisations associated with cold exposure. The evidence regarding modifying effects of social vulnerabilities remains limited.
Conclusions:
Keywords
Background
Europe is experiencing both accelerated warming and population ageing at a faster rate than other continents. While the global surface air temperature has risen by 1.3°C since the pre-industrial era, Europe has seen an increase nearly 1°C higher than the global average [1]. This intensified warming trend is contributing to more frequent and prolonged heat periods, which are associated with direct health impacts such as heat strokes and dehydration [2] as well as the exacerbation of chronic conditions, including cardiovascular, metabolic and respiratory conditions and kidney disorders [3–5].
The U- or J-shaped relationship between temperature and mortality is well-established, with evidence showing that both heat and cold exposure can significantly affect health. Non-optimal air temperatures are defined as those exceeding or falling below the region-specific minimum mortality temperature. Between 2000 and 2019, non-optimal air temperatures caused over five million excess deaths globally, including approximately 835,000 in Europe alone, with 21% attributed to heat and 79% to cold exposure [6]. This indicates that, to date, the health impacts of low temperatures are more pronounced than those of heat. Projections suggest, however, that by 2100 Europe will experience an increase in heat-related deaths and a decline in cold-related deaths as a result of climate warming, accompanied by substantial regional variation [7,8]. Along with the expected increase in extreme weather events, both high and low temperatures will continue to pose a considerable public health risk.
Europe has the highest proportion of people aged 80 years and older, and this population is projected to nearly double, increasing from 40 million in 2023 to around 80 million by 2060 [9]. The prevalence of chronic conditions and multimorbidity rises and the thermoregulation deteriorates with age, making older adults more vulnerable to heat- and cold-related adverse health outcomes [4,10]. Indeed, population ageing is shown to be a key driver of the future burden of temperature-related mortality [11], suggesting that the ageing societies are becoming more susceptible to exogenous health shocks triggered by non-optimal ambient air temperatures.
Research interest in the association of non-optimal air temperatures with emergency medical service use, hospital admissions, and out-of-hospital cardiac arrests has been on the rise. However, review studies show inconsistent findings regarding health care use during non-optimal air temperatures [3,12–15]. Even though most report an increase with age and those with pre-existing chronic conditions, only one review from the year 2011, comprising six studies, has focused specifically on older people [14]. Furthermore, most studies included in the reviews originate from outside Europe and there is a scarcity in research reporting on individual- and area-based susceptibility.
Climate change, coupled with the ageing population, poses challenges for social, economic and ecological sustainability of the health care systems. For example, the global estimate for healthcare costs related to heat-related illnesses is projected to reach $7.1trillion by 2050 [16]. Consequently, there is a pressing need for a comprehensive and up-to-date overview of the association between non-optimal air temperatures and health care use. This systematic scoping review examines how non-optimal ambient air temperatures are associated with health care use in populations aged over 65 years in Europe and how medical conditions and social vulnerabilities modify the association. Our aim is to 1) describe the extent and nature of the evidence, 2) summarize the main findings from a multidisciplinary body of knowledge and 3) identify gaps in the literature to support future research planning.
Methods
Search strategy and selection criteria
This systematic scoping review was developed in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [17]. We included peer-reviewed journal articles published in English from 2000 to 2024 that examined the association between ambient air temperature and health care use among people aged over 65 years in Europe. We excluded reviews, studies in which temperature was measured in combination with other climate indicators, studies that reported results by season and studies that did not provide numerical results for individuals aged 65 and older.
Our search period (1 January 2000 to 9 August 2024) was exceptionally extensive. To comprehensively identify relevant studies, we conducted our search across six databases: MEDLINE, Scopus, ScienceDirect, ProQuest, Web of Science and GreenFILE. The search strategy was developed in consultation with a librarian and refined through discussions of the authors.
Literature was identified through searches of titles, abstracts and keywords. Of our four main concepts—1) age, 2) air temperature, 3) health care services and 4) Europe region—age was also searched for the full-texts (Supplemental material 1 online). Our screening process consisted of two steps. First, five independent researchers (LE, JT, ET, LK and JP) screened titles and abstracts. Second, four research team members (LE, ET, LK and JP) screened the full-texts. Each article was assessed independently by two researchers and if any disagreements appeared, it was resolved by involvement of a third researcher.
After the screening, we searched for relevant articles from the reference lists of review articles but did not identify any additional articles that would have fulfilled our inclusion criteria. Our search strategy is reported in Supplemental material 2.
Data extraction and synthesis
We exported the search results to the Covidence software, which automatically removed duplicates and provided a platform for the research team to collaborate systematically and transparently. In Covidence, we developed and piloted the data extraction template, and two independent researchers (LE and ET) summarized key characteristics and main findings of the included studies. Two other researchers (JP and LK) did a random check and extracted data from 12% of the studies to ensure the consistency of results. Any disagreements were resolved by a third researcher. We extracted information from the authors and publication year, country and study period, exposure (temperature) and outcome (health care use), association between air temperature and health care use, study design, method of analysis and size of the study by age group. A description of the data extraction is available in Supplemental material 3.
In synthesizing the extracted data, we first characterize the studies by year of publication, publication platform and country. Second, we describe the methodologies employed in these studies. Third, we present evidence on the association between non-optimal air temperature and health care use and explore the modifying effects of social vulnerabilities. In accordance with PRISMA-ScR guidance, a systematic critical appraisal of individual sources of evidence was not undertaken, as scoping reviews aim to map the extent and nature of the available evidence rather than assess the methodological quality or inform policy decisions.
Results
Our search strategy initially identified 2393 records. After automatic removal of 599 duplicates, 1794 records remained for title and abstract screening. Following this screening, 144 articles were selected for full-text review and, ultimately, 52 studies were included in the final review. The study selection process is illustrated in Figure 1.
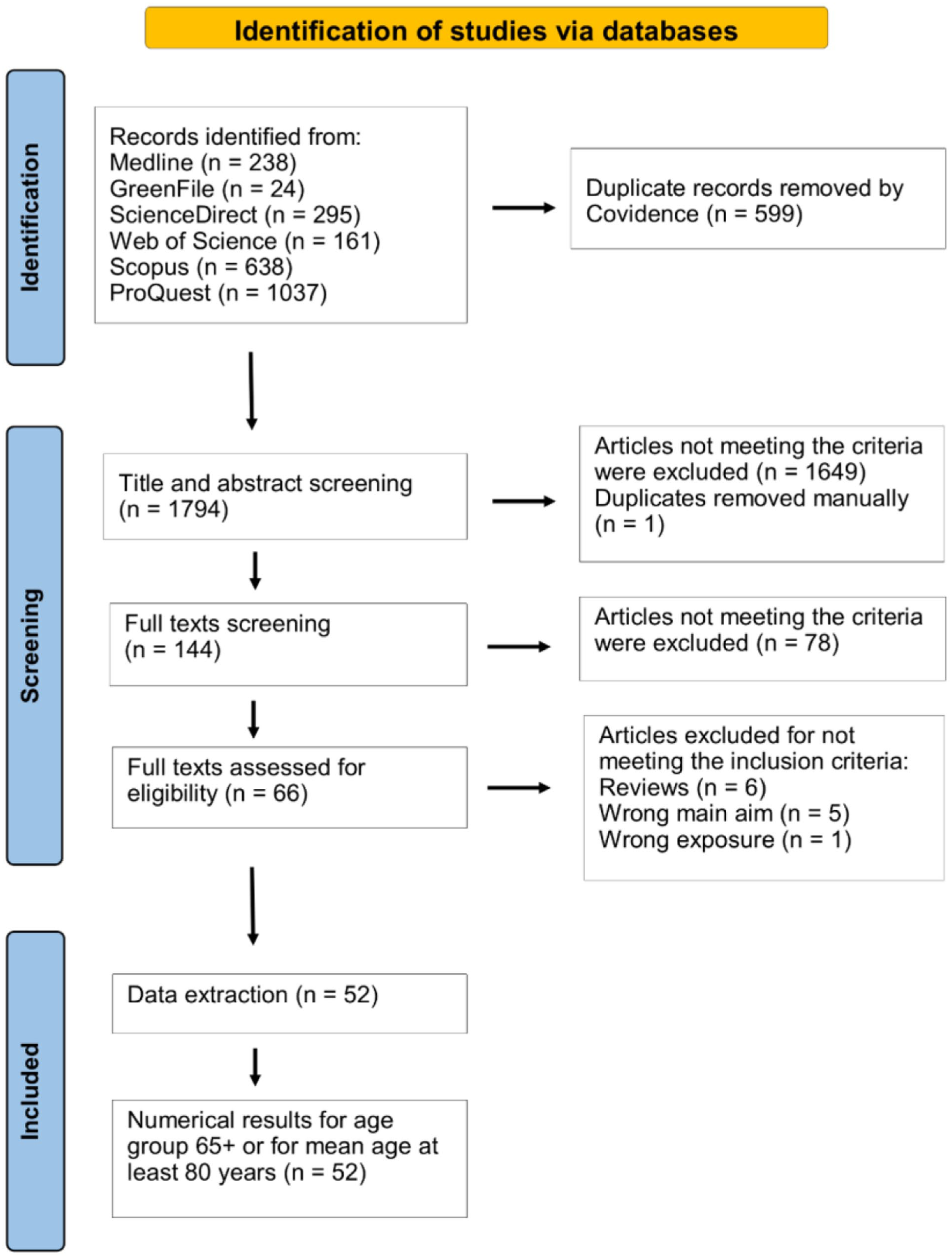
Study selection process with PRISMA flow chart.
Characteristics of the studies
Key characteristics of the studies are described in Table I [18–69]. More than half of the articles (n=28, 54%) included in this scoping review were published during the past eight years, that is, 2017 or later, indicating an increasing interest in the topic. The identified articles were published in 35 different journals, highlighting the multidisciplinary nature of the research. The most common journals were the International Journal of Environmental Research and Public Health (n=6, 12%), PLoS One (n=5, 10%), Environmental Health (n=4, 8%) and the International Journal of Biometeorology (n=3, 6%) (Supplemental material 4). The most commonly examined European regions were Spain (n=11, 21%), England or the UK (n=11, 21%) and Italy (n=8, 15%).
Description of the included studies (52) by the examined health care service.
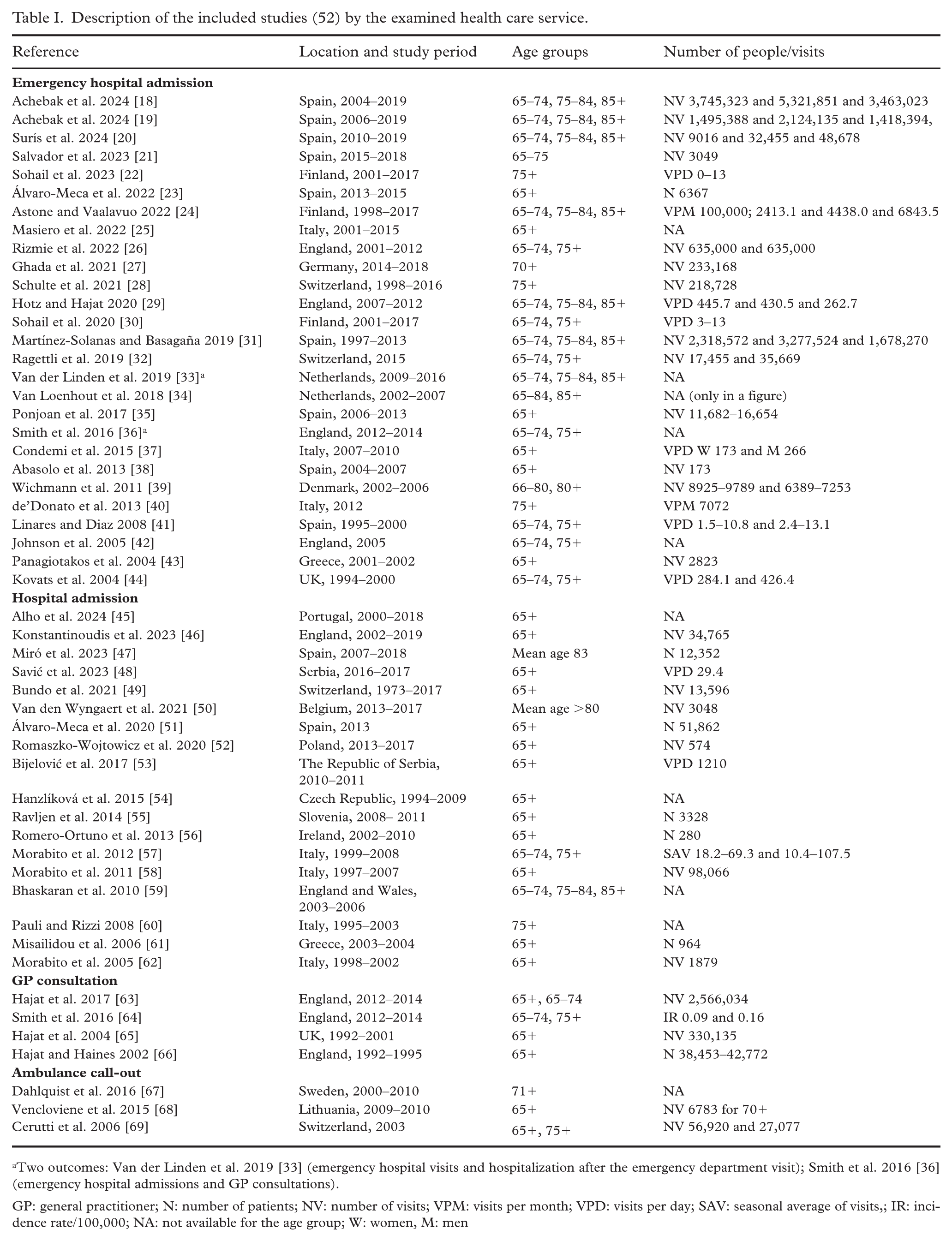
Two outcomes: Van der Linden et al. 2019 [33] (emergency hospital visits and hospitalization after the emergency department visit); Smith et al. 2016 [36] (emergency hospital admissions and GP consultations).
GP: general practitioner; N: number of patients; NV: number of visits; VPM: visits per month; VPD: visits per day; SAV: seasonal average of visits,; IR: incidence rate/100,000; NA: not available for the age group; W: women, M: men
According to prior reviews [12,13], we classified the included 52 studies into four categories based on health care service: emergency hospital admission (n=27, 52%), hospital admission (n=18, 35%), general practitioner (GP) consultation (n=4, 8%) and ambulance call-out (n=3, 6%) (Figure 2(a)). Since information on the outcome of interest, health care service use, is typically retrieved from hospital records or health care registers, all the studies were based on patient-based register data. The size of the study samples was reported in various ways, including the number of patients, the total number of admissions or the number of admissions within a specific time period. There was also substantial variation in sample sizes, ranging from 173 to over a five million health care visits during the study period (Table I).
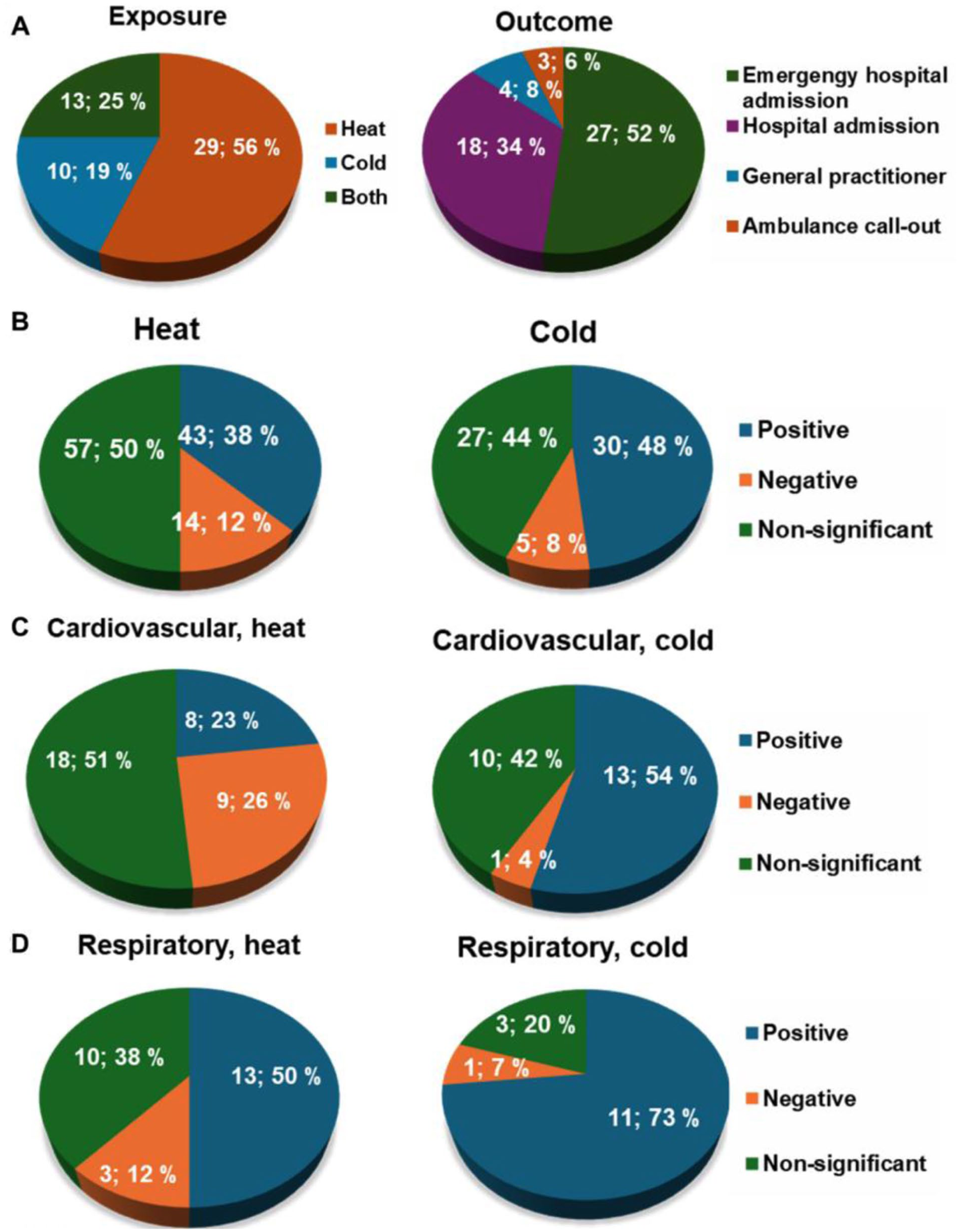
A panel figure. (a) Number and proportion of identified studies by the exposures and outcomes. (b) Number and proportion of positive, negative and non-significant associations of heat and cold exposure with health care use due to all causes. (c) Number and proportion of positive, negative and non-significant associations of heat and cold exposure with health care use by cardiovascular conditions. (d) Number and proportion of positive, negative and non-significant associations of heat and cold exposure with health care use by respiratory conditions.
We were interested in both heat and cold exposure. Most of the studies examined the association between heat and health care use (n=29, 56%), some focused solely on cold exposure (n=10, 19%) and the rest examined both (n=13, 25%) (Figure 2(a)). Temperature was most commonly measured as exceeding the 95th or 99th percentile or falling below the first or fifth percentile of the daily temperature distribution, a 1°C increase or decrease in daily mean temperature, an increase or decrease above or below the determined temperature threshold, or as a temperature range. Additionally, 11 studies examined longer exposures, defined as heat waves or cold spells. The variation in determining specific threshold values for exposures is generally related to local climatic conditions and the population’s level of adaptation in a given region. Therefore, comparability between studies is improved when exposure is presented as a deviation from the daily mean temperature (Table II).
Description of the methods of the included studies (52) by the examined health care service.
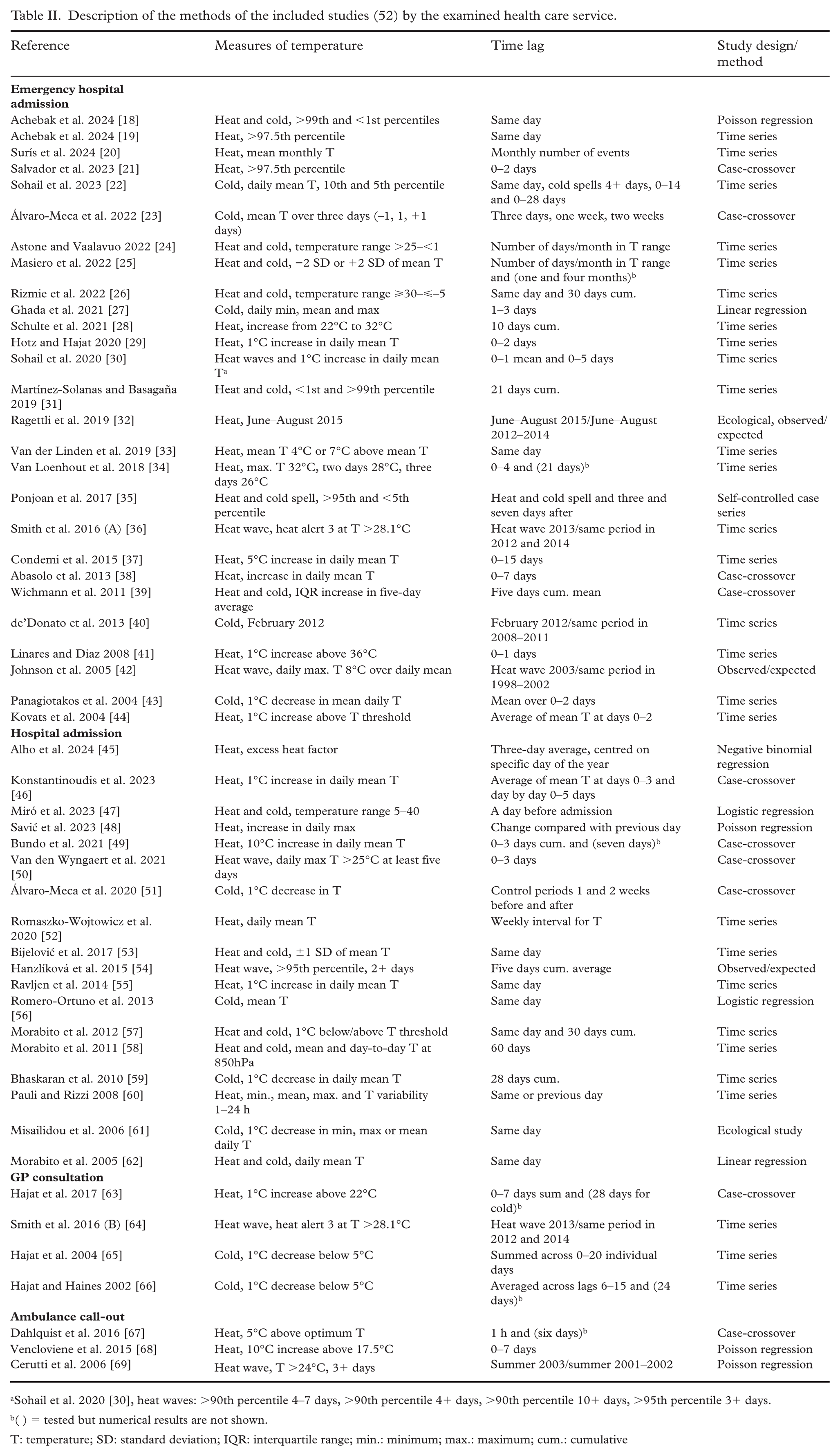
Sohail et al. 2020 [30], heat waves: >90th percentile 4–7 days, >90th percentile 4+ days, >90th percentile 10+ days, >95th percentile 3+ days.
( ) = tested but numerical results are not shown.
T: temperature; SD: standard deviation; IQR: interquartile range; min.: minimum; max.: maximum; cum.: cumulative
The effect of temperature on health care use can vary depending on the type of exposure and can be observed over several days or weeks. The examined time lag, the period from temperature exposure to health care use, was generally longer for cold exposure (up to 28 days) compared with heat exposure (less than seven days, with a few exceptions). The most common methods used to analyse the association between temperature and health care use were time series (n=28, 54%) and case-crossover designs (n=10, 19%) (Table II).
In a case-crossover study design, which is suitable for examining associations between acute, transient or short-term exposures and various endpoints such as health care use, each individual acts as their own control, thereby controlling for stable or slowly changing individual-level characteristics (e.g. sex, genetics, socioeconomic status) [21,46]. The well-known variability in health care use by day of the week, public holidays, region and season was considered in most of the studies [28,29]. Especially in studies with long-term time trends, the calendar year was also controlled for [24]. Some studies controlled for seasonal disease outbreaks (influenza) [39]. Regarding other meteorological interference, air humidity or rain, wind speed and atmospheric pressure were considered [20,53]. Furthermore, air pollutants such as nitrogen oxides, sulphur dioxide, particles with a median aerodynamic diameter of <10 or <2.5 µm and ozone were controlled for [22,41]. Overall, there was great variation in the controlled factors across the 52 studies.
Association of ambient air temperature with health care use
Associations of ambient air temperature with health care use are presented by exposure type (heat and cold), outcome (emergency hospital admission, hospital admission, GP consultation and ambulance call-out) and medical condition (Table III).
Effects of heat and cold exposure on health care use among older people in Europe 2000–2024 by the health care service and medical condition.
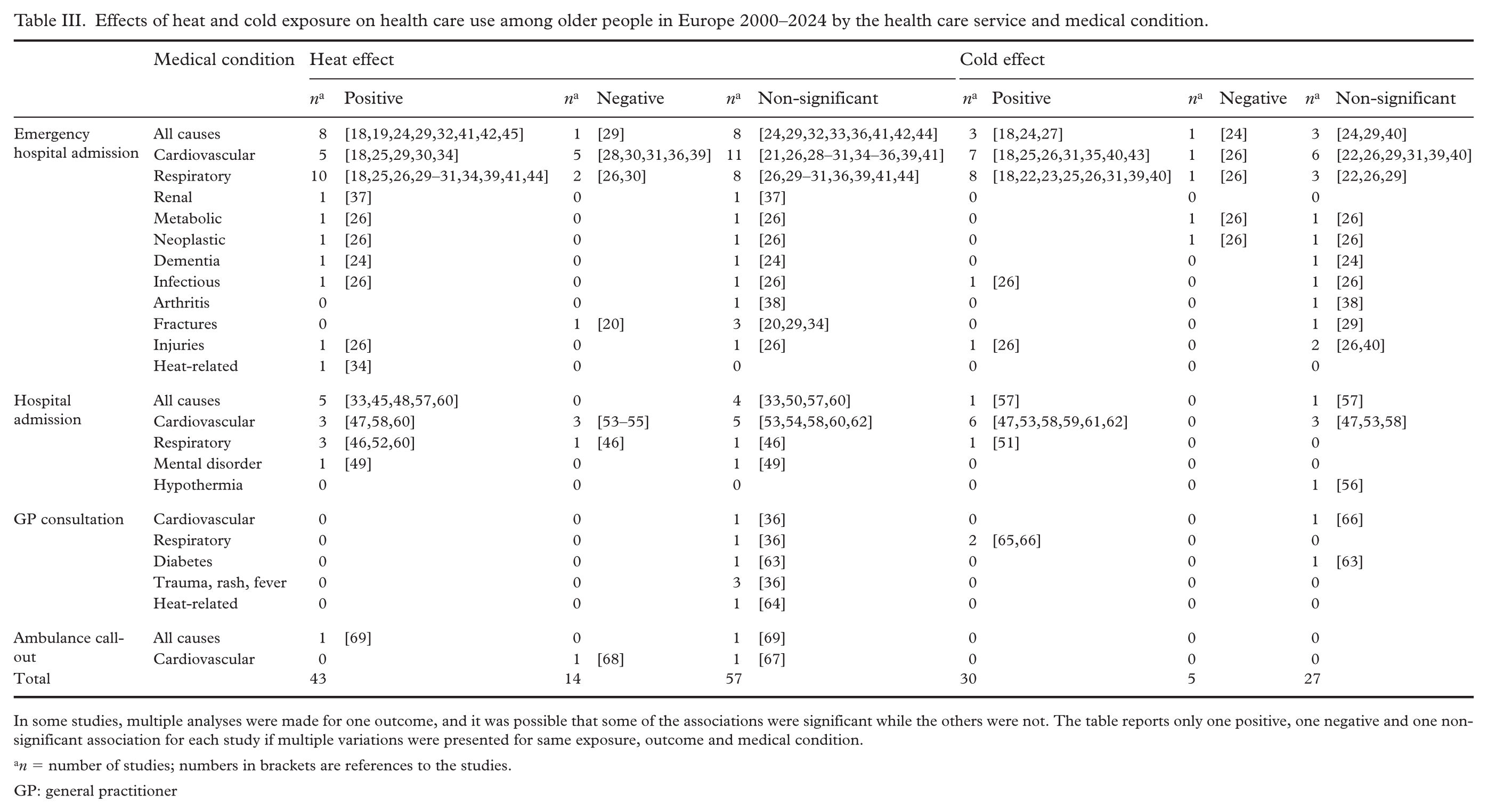
In some studies, multiple analyses were made for one outcome, and it was possible that some of the associations were significant while the others were not. The table reports only one positive, one negative and one non-significant association for each study if multiple variations were presented for same exposure, outcome and medical condition.
n = number of studies; numbers in brackets are references to the studies.
GP: general practitioner
It was common for studies to analyse multiple exposure specifications, such as different temperature thresholds, exposure durations and time lags. As a result, some studies reported multiple estimates for the same outcome, with some analyses yielding statistically significant associations while others did not. Our principle was that if multiple variations were presented for the same exposure, outcome and medical condition, findings were summarised as one positive, one negative and/or one non-significant association. For example, across cold temperature categories, Astone and Vaalavuo 24 reported mixed associations with emergency department visits, showing positive associations in some temperature ranges (<1°C, 4–7°C and 10–13°C) and non-significant associations in others (1–4°C and 7–10°C). Following our principles of not emphasizing the results of a single study and of reporting also non-significant associations, such heterogeneous findings were summarized as one positive and one non-significant association. A detailed description of the process leading to results is provided in Supplemental material 3.
All-causes
Of the 42 studies examining heat exposure, the results from 114 analyses were included in this synthesis. Heat exposure was positively associated with health care use in 43 analyses (38%) and negatively in 14 analyses (12%), indicating a decrease in health care use with increasing temperature, and had a non-significant association in 57 analyses (50%). Of the 23 studies examining cold exposure, 62 analyses were included. Cold exposure was positively associated with health care use in 30 analyses (48%), negatively in five analyses (8%) and had a non-significant association in 27 analyses (44%) (Table III and Figure 2(b)).
Cardiovascular conditions
The most commonly examined cause-specific conditions were cardiovascular (28 studies) and respiratory diseases (20 studies). Of the studies examining cardiovascular conditions, most investigated all cardiovascular diseases combined, corresponding to International Classification of Diseases (ICD)-10 codes I00–I99 and ICD-9 codes 390–459. In addition to the combined categories, several studies examined myocardial infarction and cerebrovascular diseases separately. Among the 35 analyses focusing on heat exposure, a positive association with health care use due to cardiovascular conditions was reported in eight analyses (23%), a negative association in nine analyses (26%) and a non-significant association in 18 analyses (51%). Among the 24 analyses focusing on cold exposure, a positive association was reported in 13 analyses (54%), a negative association in one analysis (4%) and a non-significant association in 10 analyses (42%) (Table III and Figure 2(c)).
Respiratory conditions
Most studies examining respiratory conditions investigated all respiratory diseases combined, corresponding to ICD-10 codes J00–J99 or ICD-9 codes 460–519. For the specified conditions, the most commonly examined were asthma, chronic obstructive pulmonary disease and pneumonia. Among the 29 analyses focusing on heat exposure, a positive association with health care use due to respiratory conditions was reported in 13 analyses (50%), a negative association in three analyses (12%) and a non-significant association in 10 analyses (38%). Among the 15 analyses focusing on cold exposure, a positive association was reported in 11 analyses (73%), a negative association in one analysis (7%) and a non-significant association in three analyses (20%) (Table III and Figure 2(d)).
Positive associations by the type of health care service
We also examined the associations of non-optimal air temperatures with the use of different types of health care services. Heat exposure was positively associated with emergency hospitalizations in 30 out of 76 analyses (39%), with hospitalizations in 12 out of 27 analyses (44%), with GP consultations in zero out of seven analyses (0%) and with ambulance call-outs in one out of four analyses (25%). Positive association of cold exposure with emergency hospitalizations was reported in 20 out of 45 analyses (44%), with hospitalizations in eight out of 13 analyses (62%), with GP consultations in two out of four analyses (50%) and there were no analyses on ambulance call-outs (Supplemental material 5).
In sum:
Although more studies examined heat exposure in relation to health care use than cold exposure, a higher percentage of analyses on cold exposure showed a positive association with health care use.
Cardiovascular and respiratory conditions were the most commonly examined causes of health care use. Positive associations were most frequently identified for respiratory conditions in emergency hospitalizations (both heat and cold), and for cardiovascular conditions in hospitalizations related to cold exposure.
Across the different types of health care services, the highest proportion of positive associations was observed for hospitalizations.
The harvesting effect, also known as morbidity or mortality displacement, refers to the phenomenon where the number of events increases as an immediate response to high or low temperatures but the number of events is lower than expected in the following period. The harvesting effect for the population aged over 65 years was examined and discussed in two out of 52 articles. The first article found a minor effect in emergency hospital admissions using two-month moving averages [25]. The second article found a clear effect on hospitalizations, with an initial increase in admissions for haemorrhagic stroke (at 0–2 lag days) followed by a clear short-term harvesting effect across 3–6 lag days [58].
The modifying impact of social vulnerability and sex differences was examined in seven studies (Supplemental material 6). Those with low income or living alone had a slightly increased risk of emergency hospital admissions [24]. Based on national deprivation indexes, individuals with deprivation had an increased risk of emergency hospitalizations due to respiratory conditions [26] and hospitalizations due to hypothermia [56]. Additionally, two studies found that higher temperatures were associated with a decrease in hospitalizations due to asthma [46] and an increase in emergency hospitalizations due to renal colic and urinary stones [37] among women, but not men. Furthermore, two studies reported similar associations in emergency hospitalizations due to hip fractures, cardiovascular and respiratory conditions, or all causes, across both sexes [18,20].
Discussion
This systematic scoping review examined how non-optimal ambient air temperatures are associated with health care use in populations aged over 65 years in Europe. In addition, we explored how medical conditions and social vulnerabilities modify the association.
Our first aim was to describe the extent and nature of the evidence. Employing systematic scoping review methods over period 2000–2024, we identified 52 studies that reported associations between heat or cold exposure with health care use and numerical results for people aged over 65 years in Europe. Research has concentrated on Spain, UK and Italy, leaving several areas unexplored, especially from eastern parts of Europe. Most records included were published in the past eight years and overall there has been an increase in the number of high-quality studies with large study populations and established methods of analysis. Most studies have focused on heat exposure, but we identified also studies involving cold exposure, and many examined cause-specific conditions of health care use. It was common to test several temperature measures and different time lags but not the harvesting effect. Despite recommendations from earlier reviews, only a few studies investigated the modifying impact of social vulnerability.
The research was published in a variety of journals, surprisingly often in the field of environmental science and less frequently in public health or health services research journals. Because of the emphasis on meteorological or environmental factors, health care services were not always clearly defined. In some cases, even basic information such as the number of people or health care visits was missing from the reports. This information is crucial for understanding which services are needed and to what extent.
The second aim was to summarise the main findings from a multidisciplinary body of knowledge. Heat exposure was positively associated with health care use in almost 40% and cold exposure in almost half of the reported associations. These proportions reflect the percentage of all positive associations restricted to one result per study, if multiple variations were presented for same exposure, outcome and medical condition. We identified four types of health care services: emergency hospital admissions, hospital admissions, GP consultations and ambulance call-outs, and, of these, the most examined was emergency hospital admission. Of the cause-specific conditions studied, most common were cardiovascular and respiratory conditions. The proportion of positive associations was highest for emergency hospitalizations owing to respiratory conditions (both heat and cold) and for hospitalizations owing to cardiovascular conditions related to cold exposure.
We suggest two reasons why cardiovascular and respiratory conditions stood out in the results. First, prior research has identified several mechanisms linking non-optimal air temperatures with these two conditions. Cold temperatures are shown to increase blood pressure and blood viscosity, activate clotting pathways and, for instance, exacerbate the symptoms of chronic pulmonary disease and asthma [70]. Conversely, heat is shown to decrease blood pressure, increase heart rate and increase cardiac demand while decreasing the heart’s filling pressure [4]. Second, our findings on the most common conditions leading to health care use during non-optimal air temperatures might reflect the fact that health care use due to cardiovascular and respiratory conditions was examined the most and, especially among the older populations, exacerbation of these underlying conditions. Direct heat- or cold-related illnesses and injuries, such as heat strokes and hypo- or hyperthermia, were examined only in a few studies. Research on a broader range of conditions is recommended for a more comprehensive view of the consequences of non-optimal air temperatures on health care use.
Non-optimal air temperatures have less consistent associations with health care use, regardless of the type of care service, compared with mortality. It has been hypothesized that some deaths occur rapidly among isolated individuals before they can access health care. A nation-wide study from Finland (2000–2014) shows that 21% of the deaths during heat periods occurred before a person was admitted to health care and half of the deaths occurred after admission to hospitals or health centres [71]. To better understand and quantify the extent to which non-optimal air temperatures are related to different types of health care services, research on all types of services and transitions between them is needed. More detailed information could help in preparing for sudden spikes in health care needs in different parts of the care system, which is highly interdependent.
Evidence on the modifying impact of social vulnerability in the association between non-optimal air temperatures and health care use remains scarce after this review. The three studies [24,26,56] that reported results for social vulnerability suggest a slightly increased risk for older people with low income, those living alone and those defined as deprived based on the national deprivation index. Additionally, two studies [18,20] reported no sex differences, while two other studies [37,46] reported both increased and decreased risk for women, but not for men.
Inconsistencies in the results between the studies included in this review are likely to reflect differences in local climate, infrastructure and health care system, as well as methodological choices, including different temperature thresholds, time lags and controlled factors. For instance, health care provision in terms of the number of available hospital beds or practices in ambulance call-outs might determine the quality and quantity of health services received. Regarding exposure, humidity is known to affect heat burden because it is related to sweating ability, but it was not considered in all the studies.
This systematic scoping review was not only limited to studies reporting on ambient air temperatures, but none of the studies reported findings on indoor temperature or aimed to control for it. Information on building characteristics or activity behaviour would provide a more comprehensive understanding of the real exposure to heat or cold. However, health care registers rarely have this kind of information available, and examining health care use in relation to non-optimal air temperature requires large sample sizes, which are usually available from hospital and health care registers. Another limitation is related to the definition of health care use. For example, it was not possible to separate emergency hospital admission from other hospital admission in all cases.
Our third aim was to identify gaps in literature to support future research planning. The number of studies and the quality of the data has increased over the past 24 years. However, to address knowledge gaps and support adaptation and mitigation efforts related to climate change and health care use, more research using large datasets is needed. Large datasets are needed to explore 1) a broader range of conditions leading to health care use, 2) multidimensional modifying risk factors including individual and area-based vulnerability, and 3) different types of health services and transitions between them.
From a methodological perspective, none of the studies examined mortality as a competing risk for health care use. Given the well-established association between non-optimal air temperatures and mortality, especially among older people, accounting for mortality as a competing risk could offer new insights into why individuals do or do not use health care. Furthermore, only a few studies examined the harvesting effect referring to an increase in health care use as an immediate response to extreme temperatures, followed by lower-than-expected health care use in the subsequent period. Distinguishing between excess health care use and a temporal shift in health care use could enhance understanding of the magnitude of health burden caused by non-optimal air temperatures and improve estimates of the associated health care costs. As more people are living longer than before, increasing the demand for health care, exploring the harvesting effect has become even more important.
Older people have many distinct characteristics, which is why reporting results for this group separately might improve the quality of interpretation. For instance, the likelihood of living in residential care increases with age. Exposure to non-optimal temperatures and the possibilities for monitoring, such as ensuring adequate hydration, might differ depending on the place of residence. It has been shown that, in general, the use of health care services, such as emergency department visits, is significantly higher among those living at home compared with those living in residential care [72]. Moreover, activity patterns, such as going outdoors during periods of non-optimal temperatures, might vary substantially among older people, depending on their place of living, and they differ from those of the working-age population.
We conducted this scoping review following the PRISMA-ScR guidelines, which included predefined research questions, comprehensive database searches, independent dual screening and iterative data charting followed by a narrative synthesis. We did not pre-register a protocol, but we consider our scoping review process rigorous and transparent because of the extensive and detailed reporting provided in the Supplemental materials 1–6. This scoping review process also has limitations inherent to broad evidence mapping. For example, owing to the multidisciplinary nature of the research, health care services were not always clearly defined, and the large regional differences as well as methodological heterogeneity might affect the interpretation of associations between air temperature and health care use. To reduce the influence of publication bias, we systematically report associations in both positive and negative directions, including statistically non-significant findings, from all included studies.
To conclude, our synthesis indicates that even though not systematically, non-optimal temperatures are associated with higher health care use among older Europeans. The results underscore the importance of considering both heat and cold as drivers of health service demand. In ageing societies, health care systems are under increasing pressure owing to the unprecedented growth in the older population. Since older individuals are more susceptible to non-optimal air temperatures, climate warming is expected to place additional strain on health care systems that are already stretched to their limits in some regions. Because different population groups such as older people, people living alone or those having financial deprivation, as well as different living areas, differ in their exposure to non-optimal air temperature and their adaptive capacities, climate change has the potential to exacerbate social inequalities in health and health care use. To address these timely challenges, more research is needed from the public health and health services research perspectives.
Supplemental Material
sj-docx-1-sjp-10.1177_14034948261460380 – Supplemental material for How are non-optimal air temperatures related to health care use among older populations in Europe? A systematic scoping review 2000–2024
Supplemental material, sj-docx-1-sjp-10.1177_14034948261460380 for How are non-optimal air temperatures related to health care use among older populations in Europe? A systematic scoping review 2000–2024 by Linda Enroth, Laura Kananen, Ella Tapola and Jutta Pulkki in Scandinavian Journal of Public Health
Footnotes
Acknowledgements
We thank Jere Tiitto for his valuable assistance in testing the search terms and participating in first stage screening.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research work was done in the framework of the Centre of Excellence in Research on Ageing and Care, funded by the Research Council of Finland (grant numbers 336670 and 352974) and in the Project ‘Care system shocks and their consequences on use of healthcare services among older people in Finland’, funded by the Research Council of Finland (grant number 371338).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.