
Abstract
Bioaerosols may produce poor indoor air quality and affect the health of the building occupants. We identified bacteria and fungi from bioaerosols and determined the microbial density values by the impaction method on solid surface in 104 locations distributed in 26 floors from an electrical headquarter building. Indoor contamination was interpreted as follow: >500 CFU m−3, indoor microbial density higher than the outdoor microbial density and pathogenic isolate. Results showed bacterial density values from 28 CFU m−3 to 522 CFU m−3 from which 18 theatres exceeded the non-contaminated density range, overcame the outdoor average density value (198 CFU m−3) or depicted the presence of the pathogenic bacteria Staphylococcus aureus and/or Staphylococcus saprophyticus. Other bacterial opportunistic pathogens were isolated. Airborne fungal detection depicted density values from 2 CFU m−3 to 800 CFU m−3. Fungal density values exceeding the non-contamination range were detected in 12 theatres distributed in 7 floors. No pathogenic fungi were detected. However, opportunistic pathogen or sick building syndrome (SBS)-associated fungal isolates, particularly Penicillum and Aspergillus, were widely distributed in almost all floors. Even though we did not associate our findings with SBS and building-related illness (BRI), we showed that this culture-based analysis proved to be an adequate way to determine the microbiological indoor air quality.
Introduction
Building occupants can be exposed to bioaerosols, chemical and physical factors in indoor air, causing unspecific health and comfort signs and symptoms known as the “Sick Building Syndrome” (SBS). Theses health hazards, particularly bioaerosols, appear to correlate to the exposure time and tend to disappear once the buildings occupants abandon the building and reappear when they get back. Unless indoor air managing procedures remediate such conditions, the SBS may get worse in time and become a permanent clinical condition in occupants [1,2]. Instead of unspecific sign and symptoms, clinically identifiable illnesses can also be experienced by building occupants exposed to specific airborne bacteria or fungi. This condition known as the “Building-Related Illness” (BRI) is common in hospital environments. Occurrence of both the SBS and the BRI depend mainly on the concentration and type of bioaerosols.
Bioaerosols usually contain dust particles and water drops with dead and viable bacteria, fungi, parasites, protozoan, algae, virus and cell derivatives [3,4]. These constituents together with the right influx of fresh air must be controlled inside buildings to reduce the density of bioaerosols [5,6]. Also, the nature of the building materials is especially relevant to bioaerosol generation, particularly those used in the construction of heating, ventilating and air conditioning systems (HVAC), carpets, walls, ceilings and other products and structures [7–9].
From all bioaerosol constituents, airborne bacteria and fungi are definitely the most relevant factors to be taken into account in considering the quality of indoor air in regular office buildings. Bioaerosols determination is not only a way to characterize the indoor air quality but also a means of testing the effectiveness and efficiency of indoor air cleaning procedures [10,11]. Several methods for bioaerosol sampling have been designed, which would allow the determination of microbial density as an indoor air quality index [12,13]. Gravity, impregnation and impaction of bioaerosols on liquid and solid surfaces are the main physical principles upon which microbiological air samplers are based. From these, the impaction method is widely used for rapid and reliable microbial density determination.
Even though the use of microbial (bacteria and fungi) density for evaluating indoor air quality has not been included in legislation concerning occupational health standards, several health organizations have proposed different criteria for assessing indoor air quality depending on the nature of the indoor area, mainly for white areas in hospital environments and non-white areas in regular indoor office rooms. For the purpose of this study, white areas were defined as those rooms with expected high air purity standards, mainly surgery rooms and intensive care units in hospital environments, while non-white areas referred to those indoor environments where a sterile or near sterile air condition is not required, such as rooms in regular office buildings. Such proposals depend then on the nature of the indoor area, mainly for white areas in hospital environments and non-white areas in regular indoor air office buildings. In regard to non-white areas, the National Institute for Occupational Safety and Health (NIOSH) has established that indoor areas with microbial (bacteria and fungi) density values ≥1000 CFU m−3 would be considered contaminated [14,15]. However, the American Conference of Governmental Industrial Hygienists (ACGIH) has reduced such value to 500 CFU m−3 [16]. Health Canada also proposed that fungi density should not be higher than 50–500 CFU m−3 depending on the fungi genera and fungi homogeneity [17]. The Department of Health of New York (NYHD) recognizes that security levels in terms of microbial density are hard to define [18], but indoor air evaluation should also consider microbial identification and outdoor air microbial density [19,20]. For white areas in hospital settings, The Spanish Association of Hospital Engineering (AEIH) has defined the following criteria for assessing indoor air quality [21]:
bacteria and fungi density values <10 CFU m–3 ⇒ very clean, bacteria and fungi density values 10–100 CFU m–3 ⇒ clean, bacteria and fungi density values 100–200 CFU m–3 ⇒ acceptable and bacteria and fungi density values >200 CFU m–3 ⇒ contaminated
The evaluation of the SBS and BRI was not part of the objectives of this study. Nevertheless, we investigated bioaerosols in a regular office building as one of the most relevant hazard factors that can affect the health of building occupants. This approach would allow a mean to evaluate the indoor air managing activities and alert for a poor indoor air quality condition, allowing the opportune application of bioremediation procedures. The project assumed that if indoor air is managed as a part of an enclosed HVAC system in a big office building, then a mixture of innocuous, SBS-associated, opportunistic and pathogenic bacteria and/or fungi could be found as a part of the bioaerosols’ constituents from a low to a high concentration. This study provides comprehensive data related to bioaerosols that have been obtained from 26 non-white office environments from an electrical headquarter building and analyzed the results in relation to the type of bacteria and fungi as well as their concentration in the indoor air.
Materials and Methods
Office Building
A 26-floors electrical headquarter building was selected for this study due to its susceptibility to SBS and BRI. This building, which is located in a highly polluted urban area, was identified as having a non-maintenance-HVAC duct works status. Only minor parts of the centralized and decentralized chilled water HVAC system reported regular maintenance. This selected building is a 42-year-old construction from the early eighties, with 1,569 employees distributed in 20,000 m2. This building was selected based on a combination of several indoor environmental factors related to SBS and BRI, particularly building overcrowding, low HVAC maintenance, surrounding outdoor air pollution and occupants’ complaints. This building was experimentally managed as a non-white area since it was destined as a regular office building with no hospital activity.
Air Sampling
Air samples were taken by the impaction method over a solid surface. For that purpose, 1,000 m3 of air was sampled within a 10 min period using an Andersen 1 perforated platform type-microbiological air sampler MAS-100 (Merck, Germany). This device directs the air-stream onto the agar surface of standard Ø 90 mm Petri dishes utilizing a suction pump. Airflow was continuously monitored and regulated to a constant flow of 0.6 m3 per h at a speed of 36,000 m per h, allowing collection of up to 1 m3 per run. These properties equal the stage 5 in the typical six stages Andersen-impactor. Air sampling was run between 10 am and 3 pm in June–July, 2011. Indoor temperature and humidity during air sampling indicated 20–22℃ and 70–75%, respectively, while outdoor temperature and humidity registered 28–30℃ and 65–72%, respectively.
Air Samples
Indoor air samples were collected from the following 26-floor settings located in the electrical headquarter building as follows:
E4 (underground parking E4) E3 (underground parking E3) E2 (underground parking E2) U3 (underground storage room and executive parking) U2 (underground customer services) U1 (underground internal services) Hall (street level) Restaurant and gym, Floors 1–16 Floors 18–19 Outdoor air samples were collected from the following 3 street level-settings around the electrical headquarter building as follows: West East South-west
In order to ensure that air samples taken at each room were representative of the air prevailing at such quarters, triplicate samples from 4 spots, significantly apart from each other and 1 metre high, were taken from each location during normal office working conditions (Figure 1). In addition, one sample was taken just right at the outflow of the HVAC system (0.15 m apart). As controls, Petri dishes containing especially supplemented-nutrient agar and sabouraud agar were located within the air sampler without activation for 10 min after each run of air sampling and incubated under the same conditions as stated below.
Floor plan indicating air sampling spots (circles).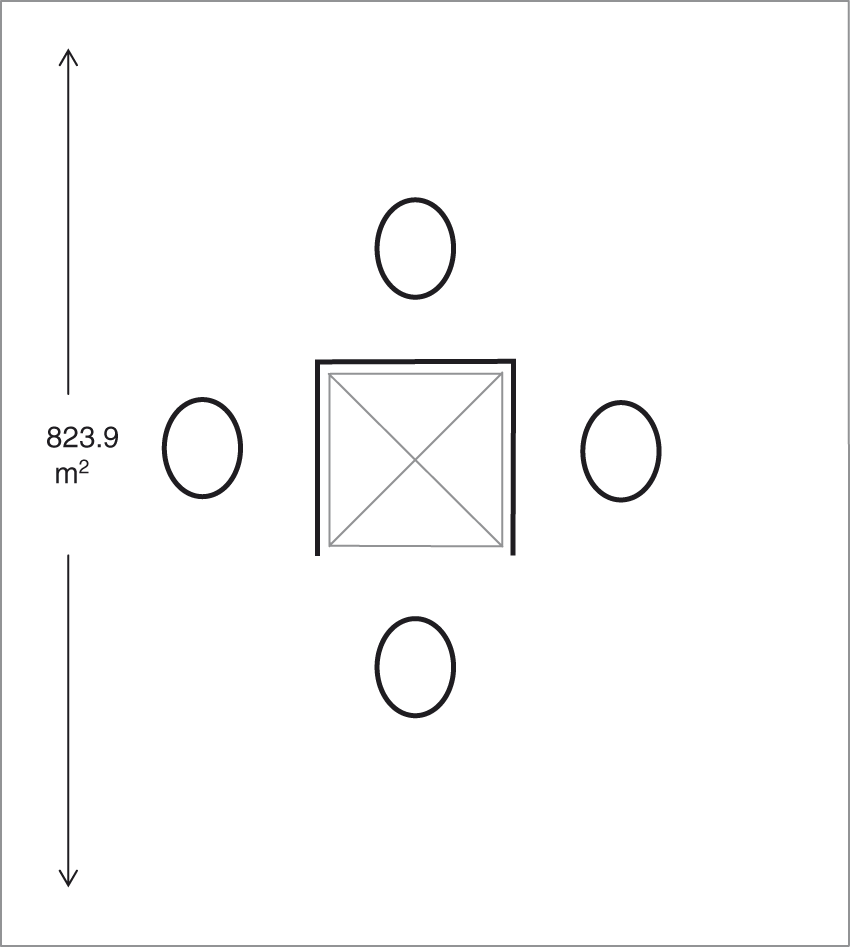
Culture Media
Sabouraud-4% Glucose-Agar (Merck, Damstadt, Germany) was especially designed for fungal growth while discouraging bacterial growth from bioaerosols (manuscript in preparation) by supplementing with a combination of amoxiciline and ampiciline (Calox International, Caracas, Venezuela) to a final concentration of 750 mg L−1 each.
Nutrient agar (Merck, Damstadt, Germany) was especially designed for bacterial growth while discouraging fungal growth from bioaerosols (manuscript in preparation) by supplementing with Itrakonasol (Janssen-Cilag, Puebla, Mexico) to a final concentration of 20 mg L−1.
Incubation Conditions for Bacteria and Fungi
Bioaerosols trapped onto the especially designed fungal and bacterial culture media were incubated at 30℃ and 37℃, respectively. In order to determine the density values associated with bacteria and fungi present in each gathered air samples, the same were subjected to incubation conditions for a period of 2 days and 7 days, respectively. Microbial density values were then determined in a colony counter (Darkfield Quebec Colony Counter, Buffalo, NY, USA) after the completion of the incubation periods.
Quantitative Indoor Air Quality Index for White Areas
In accordance with the American Conference of Governmental Industrial Hygienists [16], Health Canada [17], The Department of Health of New York [18], the following microbiological quality index was used in indoor air:
Bacterial and fungal density values >500 CFU m−3 ⇒ contaminated. Fungal density values of a same specie fungus >50 CFU m−3 ⇒ contaminated Indoor bacterial and fungal density values > outdoor bacterial and fungal density values ⇒ contaminated.
Qualitative Indoor Air Quality Index for White Areas
Bacteria and fungi isolates were identified by standard microbiological methods. In accordance with the guidelines of the Department of Health of New York [18], the following microbiological quality index was used in indoor air regardless of the bacteria and fungi density values:
Presence of pathogenic bacteria and fungi ⇒ contaminated.
Statistical Analysis
Results were expressed as average CFU m−3. Student’s t test was used for statistical analysis.
Results
In this study, we evaluated 104 locations in a 26-floors electrical headquarter building. This building held 6 underground floor levels, 1 street level hall, 1 intermediate floor and 19 consecutive floors dedicated to office activities.
Bacteria Analysis
In relation to airborne bacteria, individual bacterial density values ranged from 28 CFU m−3 (west side of floor 18) to 522 CFU m−3 (office area of customer services in U2). Based on average density values in each floor and bacterial identification, 18 locations distributed in all indoor settings were found contaminated either because bacterial density values exceeded the outdoor bacterial density or because bacterial pathogens were isolated (Figure 2).
Contaminated indoor air locations. Selected theatres were based on indoor air average bacterial density values that exceeded the outdoor air bacterial density values and/or depicted the presence of bacterial pathogens. Vertical dotted line indicates the average outdoor bacterial density value.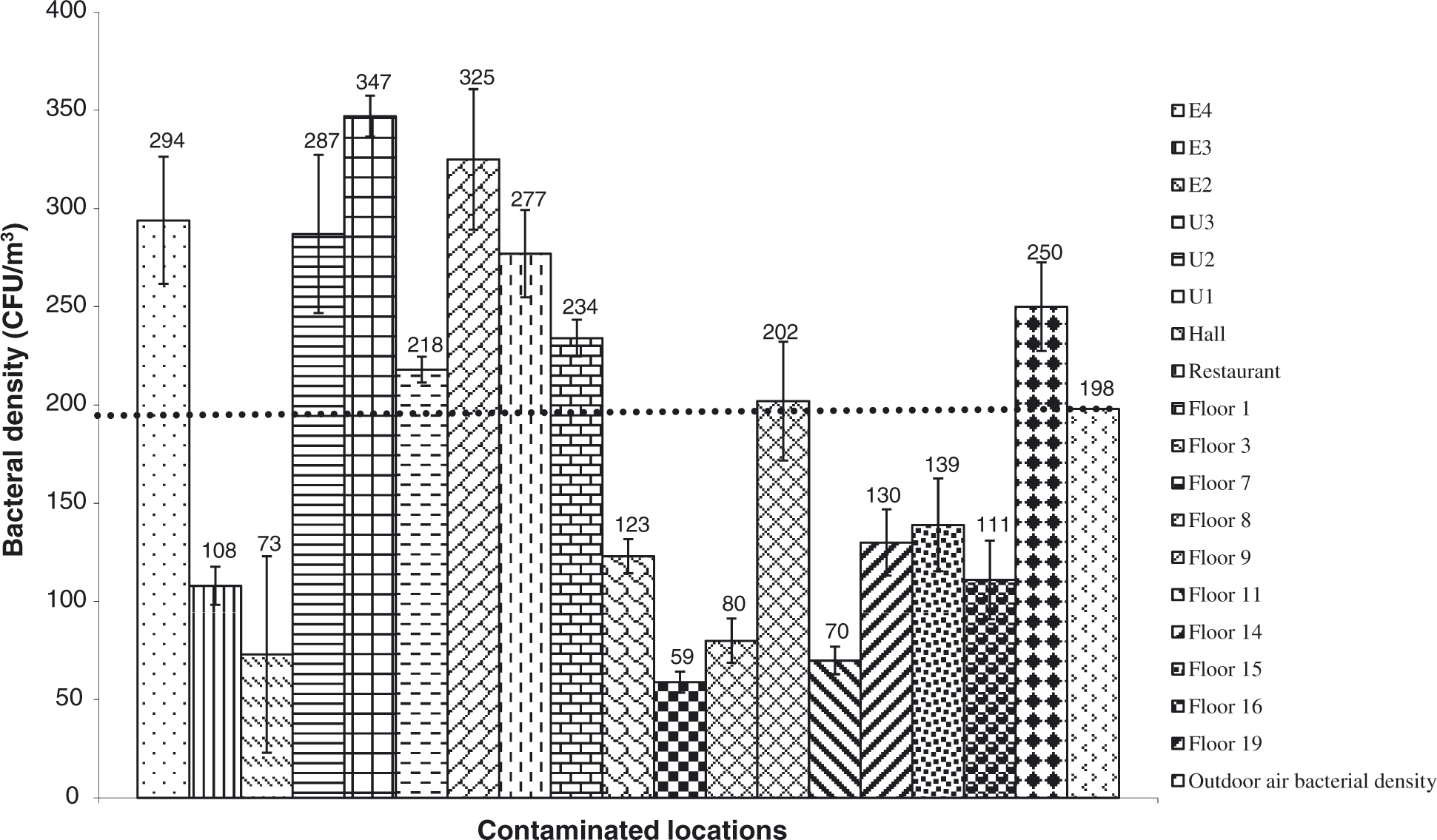
Distribution of bacterial isolates
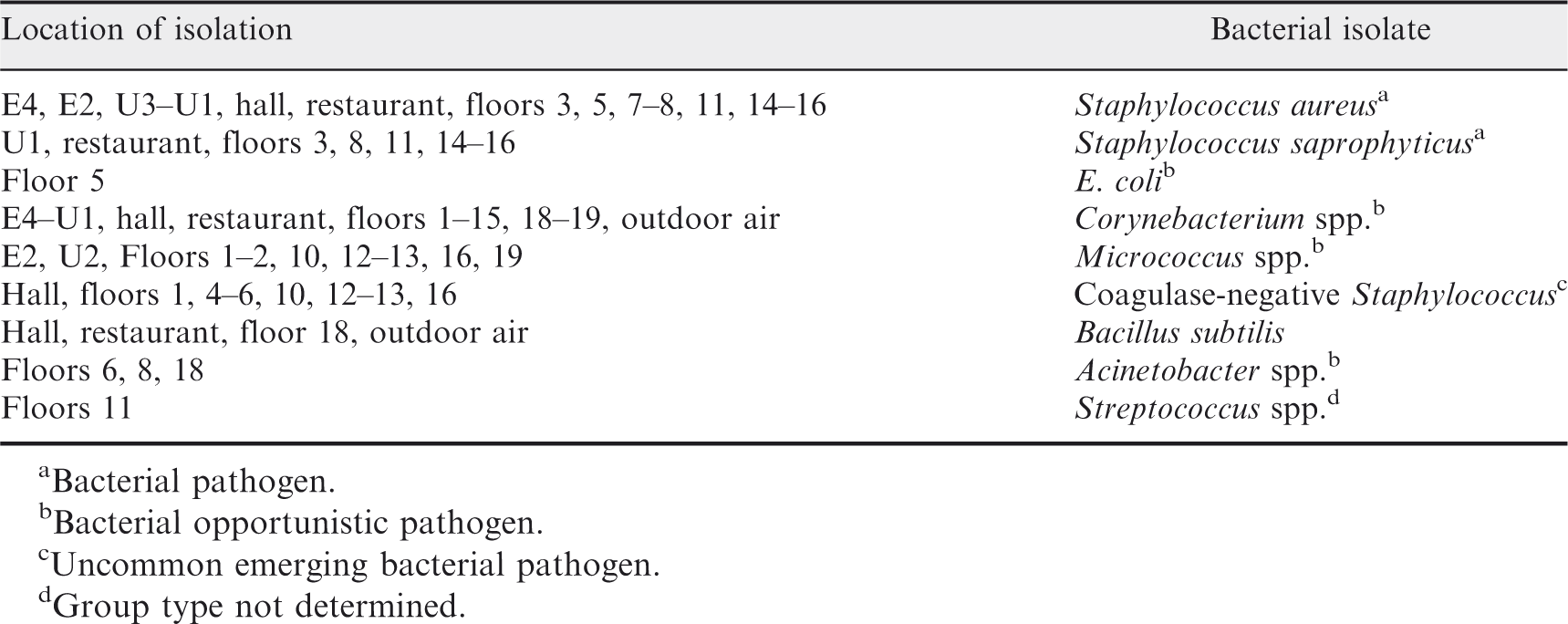
aBacterial pathogen.
bBacterial opportunistic pathogen.
cUncommon emerging bacterial pathogen.
dGroup type not determined.
The rest of the selected locations were found with a contamination based on average indoor air density values that significantly exceeded the outdoor air bacterial density values (p<0.05). From these, locations E4, U3-U1, hall, restaurant and floors 3 and 5 met both the contamination criteria adopted in this study as either Staphylococcus aureus or Staphylococcus saprophyticus and/or both pathogens were isolated.
Other non-pathogenic but SBS-associated bacterial species were isolated in sampled locations, with an indoor air bacterial density value below 500 CFU m−3 or lower than the outdoor air bacterial density value (Figure 3).
Noncontaminated indoor air locations. Selected theatres were based on average indoor air bacterial density values were below 500 colony forming units (CFU) m−3, below the outdoor air bacterial density values or did not depict bacterial pathogens. Vertical dotted line indicates the average outdoor bacterial density value. In any case individual indoor air bacterial density value in each location exceeded the outdoor bacterial density value.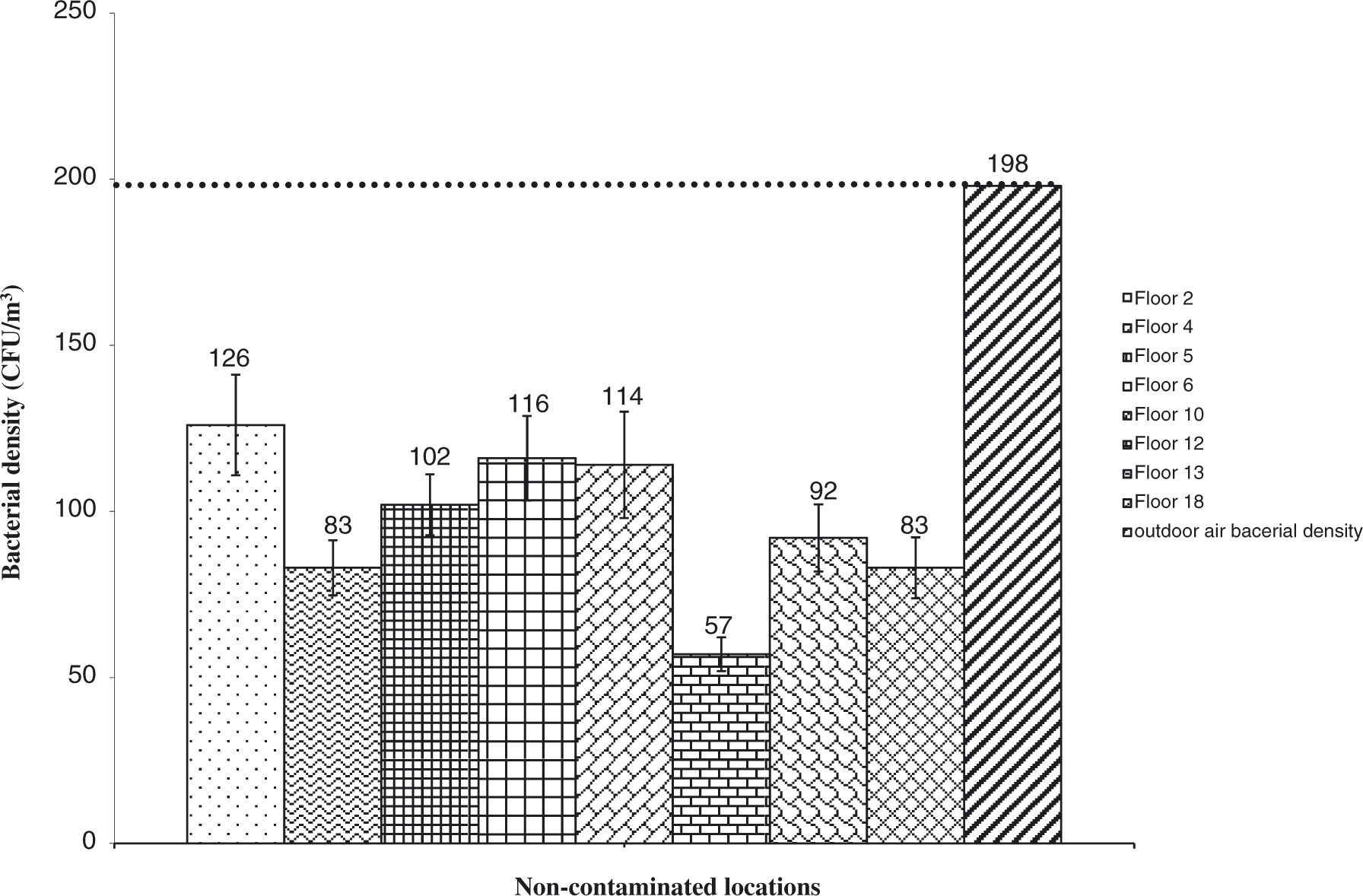
E. coli and Streptococcus spp. were unique as they were only found in floors 5 and 11, respectively. In addition, E coli has not been a common indoor air isolate and it has been involved in faecal contamination. Bacillus subtilis, which was also isolated from the outdoor air (Table 1), was the only innocuous bacterial specie found in the studied settings, while the rest of the non-pathogenic bacteria have been associated to opportunistic human infections (Table 1). Contrary to Bacillus subtilis, which was restricted to only 3 settings in the building, Corynebacterium spp. (the other predominant outdoor air bacterial isolate) was found in almost all sampled settings. The highest concentration of airborne bacteria was mainly detected in the underground or first levels of the building (Figure 2). Streptococcus could not be identified to the species level; therefore, the pathogenicity of such microorganism was not determined.
Fungi Analysis
In regard to the fungi characterization in the indoor air environment, fungi density values were found to range from 2 CFU m−3 (north side of floors 3 and 5) to 800 CFU m−3 (gym and microwave area of the restaurant). Fungi contamination was detected in 12 indoor settings distributed in 7 floors (Figure 4).
Contaminated indoor air settings. Selected theatres were based on indoor air average fungal density values that exceeded the outdoor air fungal density values. Vertical dotted line indicates the average outdoor fungal density value.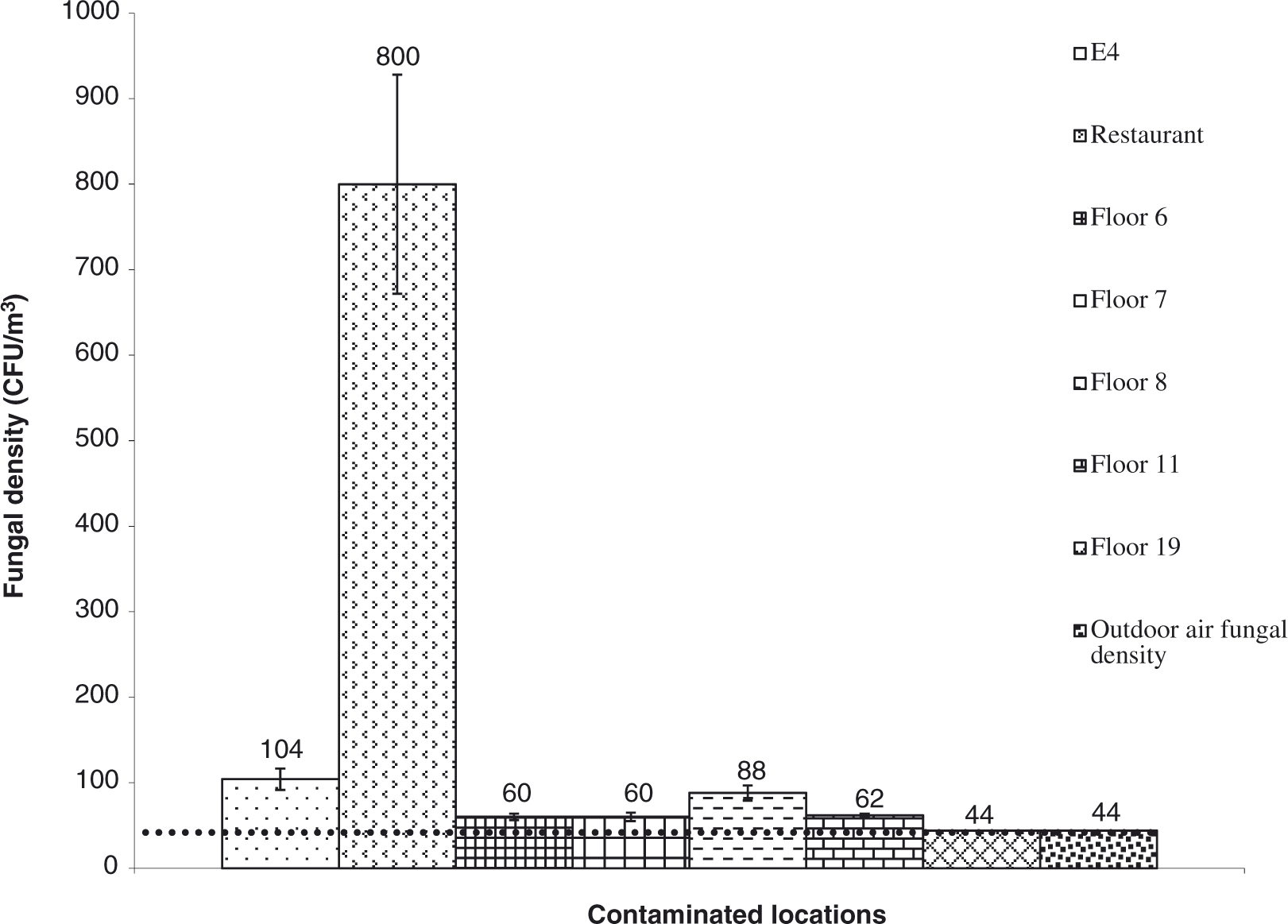
Distribution of fungi isolates
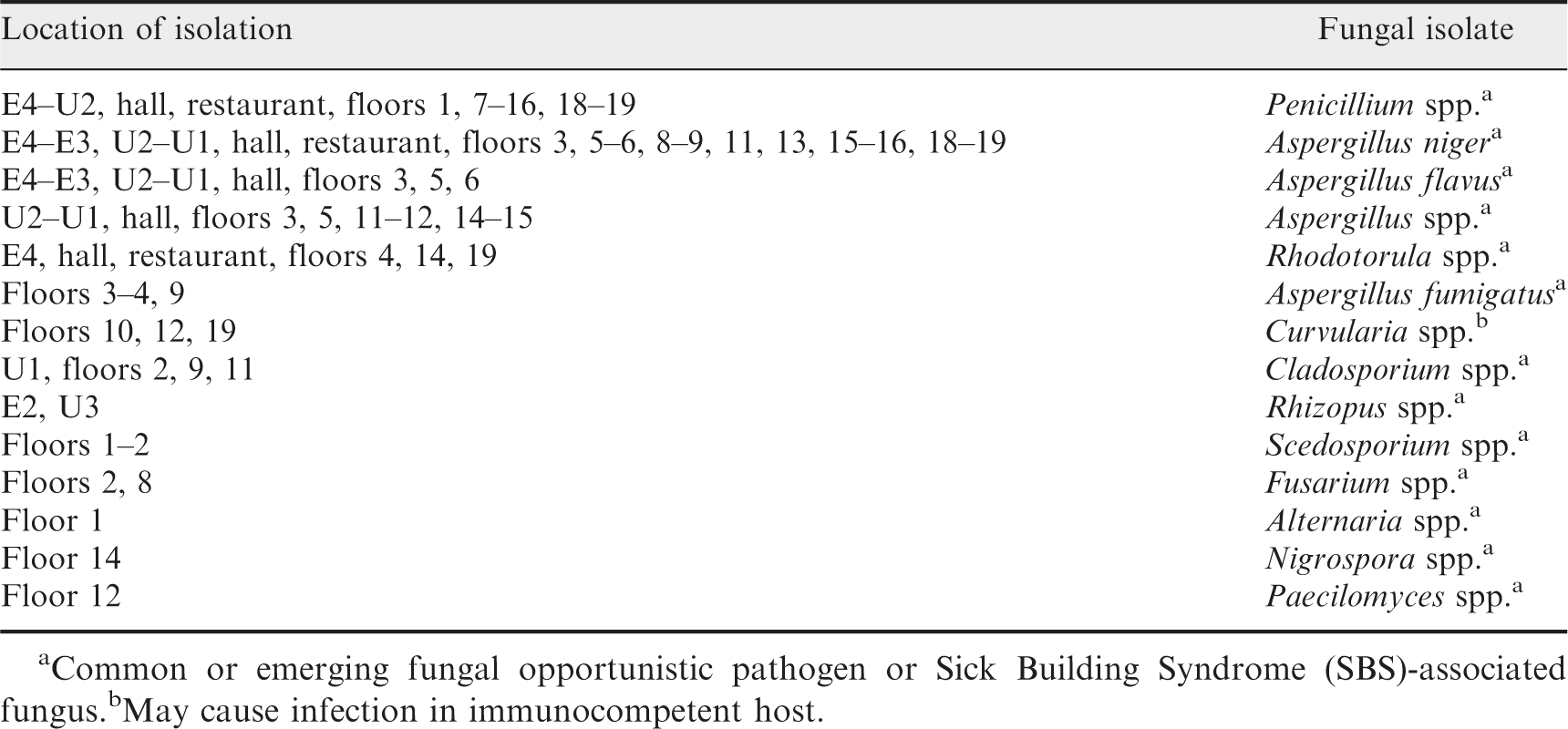
aCommon or emerging fungal opportunistic pathogen or Sick Building Syndrome (SBS)-associated fungus.
bMay cause infection in immunocompetent host.
Alternaria spp., Nigrospora spp. and Paecilomyces spp. were the only fungal species isolated individually from floors 1, 14 and 12, respectively (Table 2). However, the density values of such fungi did not exceed the contamination criterion ≥50 CFU m−3 in air for a single fungal species isolated from any of the above mentioned floors of the building (Figure 5).
Noncontaminated indoor air settings. Selected theatres were based on average indoor air fungal density values were below 50–500 colony forming units (CFU) m−3, below the outdoor air fungal density values or did not depict fungal pathogens. Vertical dotted line indicates the average outdoor fungal density value. In any case individual indoor air fungal density value in each location exceeded the outdoor fungal density value.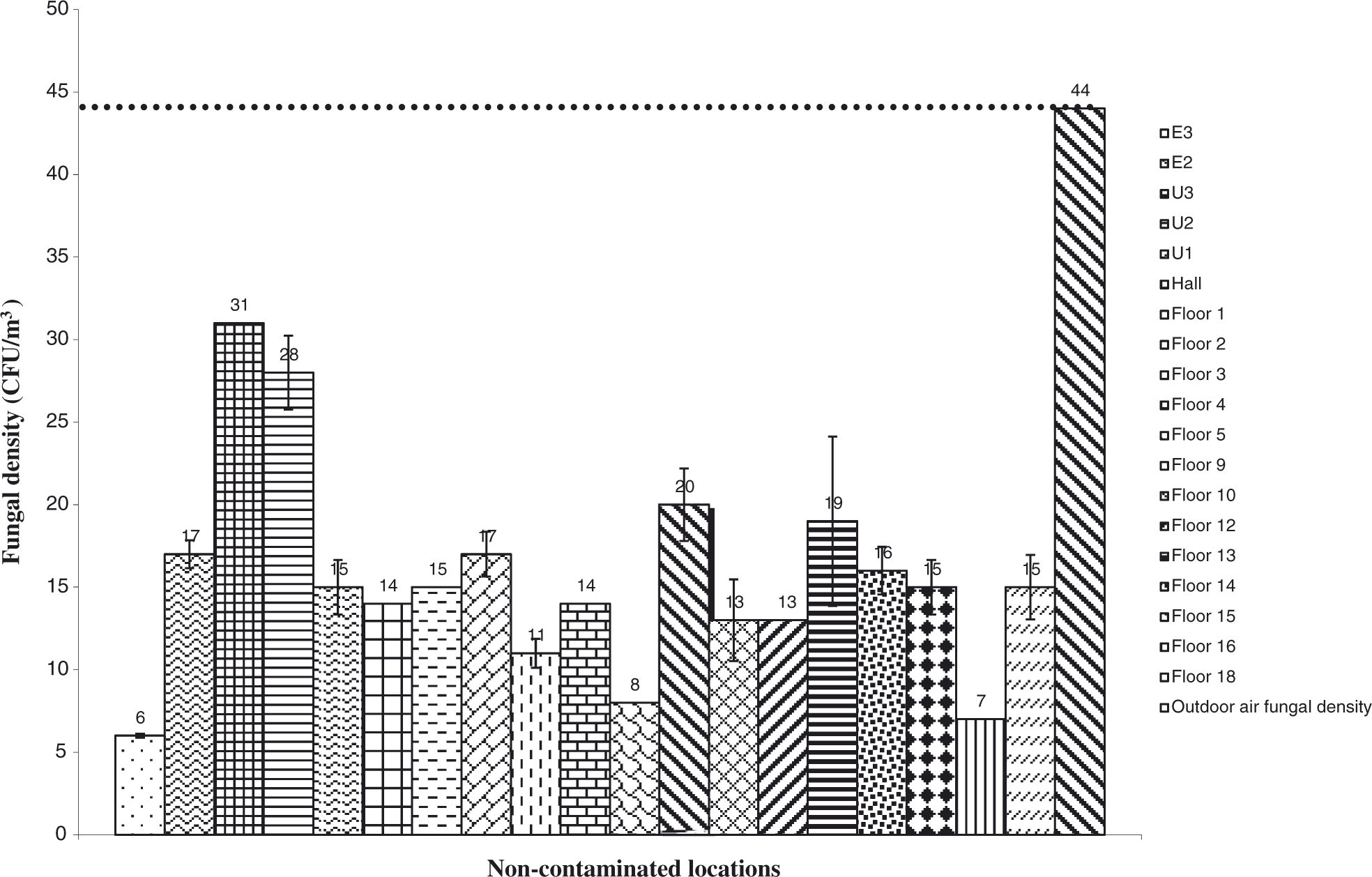
According to the number of affected theatres, bacteria-caused contamination was 3 times higher than that caused by fungi. The highest fungal density value was detected in the restaurant floor (an intermediate floor above the street level), particularly in the microwave area where people are allowed to heat their own food, whereas the serving food area just next to the microwave area did not show fungal contamination. Also, high-fungi density value was found in a gym located on the same floor, where people are crudely gathered just before the lunch time (Figure 4). Penicillum spp., Aspergillus niger and Rhodotorula spp. were the most common fugal isolates in this setting, while Penicillum spp., Aspergillus spp., Aspergillus niger, Aspergillus flavus and Rhodotorula spp. were the most frequent fungal isolates in all the studied theatres (Table 2). In all cases, the fungal isolates found in this study have been associated with SBS or opportunistic human infections [22–27]. Contrary to the bacterial contamination, fungal contamination was mainly concentrated in the upper floors, well above the underground levels.
Discussion
Enclosed buildings, especially those with little windows airing, are susceptible of SBS and BRI, especially when fresh airflow is restricted to less than 10% in relation to recycled airflow and when indoor air management is inefficient in terms of controlling the concentration of bioaerosols, which may include virus, bacteria, fungi, other microorganisms and cell derivatives. Particularly, the characterization of bacteria and fungi has been usually selected as a tool for evaluating the microbiological quality of the indoor air. Contrary to the indoor air control in white theatres from hospitals and other special environments, indoor air management in regular office buildings has not been clearly established. Even though it has been difficult to demonstrate the threshold density values of bacteria and fungi responsible for causing SBS or BRI, some authors have proposed several microbial indexes for indoor air quality, based on the average microbial density values registered in this type of environments. In addition, it has been accepted that the presence of microbial pathogens in indoor air sets a biological hazard condition that could threaten the health of the building occupants. Finally, indoor air management should be in place to keep bioaerosol concentration below the bioaerosol concentration found in the outdoor air, which otherwise would indicate that bacteria and fungi are being concentrated inside the building [28]. We have used a combination of these three criteria to establish a microbiological indoor air index useful to evaluate the indoor air condition.
Beyond the significance of the absolute bacteria and fungi density values, which may be relative to the health conditions of the building occupants and type of microorganism, indoor air management has to procure low concentrations of bioaerosols, pathogens or SBS-associated opportunistic pathogens as compared to those found in the outdoor air. We have shown in this study that a culture-based method for detecting bacteria and fungi from bioaerosols would allow monitoring of the microbiological indoor air condition.
With the exception of locations E4, the restaurant and floor 19, which showed both, bacteria and fungi contamination, the rest of the studied locations had one or the other type of microbial contamination. In the case of the underground E4 location, which was the deepest floor level of this building, it was found that the HVAC system was set with a lower influx level of outdoor air [5,29]. Also, indoor air humidity and temperature were not strictly controlled in this setting. We believe these conditions may have contributed to the bioaerosol concentrations found in the building [29]. On the other hand, the restaurant, with a gym located next to it, was characterized by frequent food manipulation with little hygienic conditions as people would warm up their meals on their own in the microwave devices. In addition, overcrowded people in the gym facilities may have added bioaerosols to this setting. Finally, floor 19, where all the electric system units were located, had a particular environment suitable for microbial growth as outdoor air was not controlled [5,9]. Apart from these special conditions, which would explain the combination of bacteria and fungi contaminations, it was shown by this study that contrary to other reports that present fungi as the most frequent contributor to indoor microbiological pollution [24], bacterial contamination was shown to be more disseminated than fungi contamination in terms of microbial density, occurrence and microbial distribution. These results suggested that filters from the HVAC system would have selected for fungi growth only in underground floor levels with poor indoor air management, particularly in relation to air temperature and humidity control. Instead, other environmental conditions would have prevailed in favour of bacteria growth in the upper floor settings. Tsai and Macher who reported statistical data from 100 buildings studied by the US Environmental Protection Agency in 1994–1998 concluded that the average range for bacteria density in non-complaint buildings would be about 116 CFU m−3–175 CFU m−3 depending on seasons [30], which was similar to our findings (mean value of 159 CFU m−3). However, season was not a factor to be taken into account in our study since Venezuela lacks this type of climatic changes during the year. On the other hand, Bouillard et al. reported higher indoor air bacteria density in 25 non-complaint offices (44-2,511 CFU m−3) with a median of 277 CFU m−3 [31]. Similarly, Gołofit-Szymczak and Górny reported a mean range of 39–221 CFU m−3 in the indoor air from 4 non-complaint buildings depending on the age of the building and the quality of the indoor air management [32]. These two studies revealed that airborne bacteria density in non-complaint buildings may be higher than those values in complaint buildings as reported in our study.
Our data indicated that half of the indoor settings that showed bacterial contamination in terms of pathogens or opportunistic pathogens had density values that did not exceed the outdoor air bacteria density or 500 CFU m−3 in air. Even though the diversity of the bacterial pathogens was restricted to Staphylococcus aureus and Staphylococcus saprophyticus, which is low in relation to hospital environments, it was shown that these microorganisms were found frequently in many floor settings. In addition, such bacterial species were not part of the outdoor air bacterial isolates, which suggested that they may have been imported from other sources inside the building and disseminated by the HVAC system. The presence of E. coli in floor 5, a very uncommon indoor air bacterial isolate in this type of environment, indicated an uncommon airborne contamination from faecal source.
All these results indicated that the bacterial identification was necessary for a more complete evaluation of the indoor air quality; otherwise underestimation could occur if only the bacterial density was taken into account. Our study stressed the fact that both the microbial density and type of microorganism are relevant to the evaluation of the indoor air quality, which was based on the premise that some of the microbes are biologically risky because of their pathogenic nature; others that are environmentally common may be pathogen to human when they occur in concentrations higher than normal, and some may only be opportunistically pathogen to people who are immuno-compromised.
Contrary to the low diversity of pathogenic bacteria found in all floor settings, which is usually associated to the building occupants themselves, the rest of bacteria and fungi isolates were similar to hospital environments [33]. Corynebacterium spp., Micrococcus spp., Coagulase-negative Staphylococcus, Aspergillus spp. and Penicillum were the most frequent microorganisms found in this study, which suggested that common SBS-associated indoor factors, such as poor air temperature, humidity control and low HVAC maintenance, may have been involved [34]. Fungal density values were found to be different from those findings reported by Chao et al. who studied 4 office buildings in Boston, USA [35]. In relation to our findings, these authors obtained a lower median fungal concentration (22 CFU m−3 vs. 58 CFU m−3). On the other hand, Burge et al. observed that the indoor fungal density values were in all cases below those outdoors and concluded no contamination [36]. However, they did not go into taxa considerations. Even though we obtained 6 zones with higher fungal density values in relation to those outdoors, we concluded that contamination was additionally relevant in other places where SBS-associated fungal species were found. Kemp et al. found a low incidence of indoor fungal concentration in a non-complaint building [37]; however, they concluded contamination since Paecilomyces lilacinus was isolated. This criterion was similar to ours since fungal density values were considered insufficient to evaluate indoor air microbial quality. Numeric reference then plays a secondary role when the results reveal the presence of well-recognized pathogenic or allergenic taxa.
Even though the determination of the possible sources of microbial contamination was not included in this study, preliminary observations revealed that the ductwork and the condensate water collection pans were important sources for bioaerosols generation. Other sources for microbial contamination, such as old and inadequate carpets, wall and ceiling materials, waste disposal procedures, toilets, file rooms, absence of HEPA filters in the HVAC systems and low influx of fresh air [5,9], may have contributed to the overall increase of the microbial density.
Conclusion
Our data indicated that the building analyzed in this study showed bacterial and fungal indoor air densities within the range of normally reported non-complaint buildings. An indoor air microbiological quality index could be used for bacteria and fungi as an early building occupant warning system to alert about the poor indoor air quality and the potential occurrence of SBS or BRI. These values range from 50 CFU m−3 to 1000 CFU m−3. Because of this, microbial taxa should also be addressed to complete indoor environmental studies. Also, such an index could be applied to evaluate the effectiveness and the efficiency of remediation procedures as part of the indoor air management activities. We presented a culture-based sampling technique as a quick mean of characterizing the indoor air microbial quality [38]. In addition, we gathered for the first time in Venezuela new data that show the distribution of bacteria in relation to fungi and the type of microorganism found in a regular office building and its surrounding environment.
Footnotes
Acknowledgement
We acknowledge Mrs. Zaida Sierra for backing up all the logistic of this study. Final del formulario