
Abstract
Children who spend more time indoors at home could become vulnerable to respiratory illnesses due to indoor pollution. There is little documentation on this major threat to public health in Côte d’Ivoire, where 70% of the population uses biomass as a home energy source. As a part of an EcoHealth project, factors associated with the prevalence of respiratory symptoms among children under five years of age were studied in a peri-urban neighbourhood north of Abidjan. From May to July 2010, a transdisciplinary team administered a questionnaire and an observation checklist to collect data on the physical quality of 681 dwellings of 899 children and the children’s living conditions. The 25.6% prevalence of respiratory symptoms was high among children whose mothers were housewives. Solid fuel burning was also linked with respiratory symptoms, as were a number of factors degrading the physical quality of dwellings (presence of mould/mildew, average number of openings per room <2, temperature ≤30℃, humidity level ≥90%). Addressing these factors that originate in children’s indoor environments would help reduce their vulnerability to respiratory illnesses.
Introduction
After inadequate access to drinking water and poor sanitation, home pollution is the second leading environmental health problem affecting children in developing countries.1,2 In fact, children are particularly exposed because of their high lung aeration rate, an immature respiratory system and long periods spent in enclosed spaces. 2
The pollutants usually implicated are particulates less than 10 µm (PM10) in size and under 2.5 µm (PM2.5) in diameter, volatile organic compounds (VOCs), nitrogen dioxide (NO2), sulphur dioxide (SO2) and carbon monoxide (CO).3,4 Indoor sources of these pollutants range from biofuel and tobacco smoke to emissions from household maintenance products and building materials. 5 Furthermore, pollutant concentrations in homes depend on humidity level, temperature and ventilation.5–7
In Africa and Southeast Asia, more than 90% of the population burns wood, animal waste and vegetable residue for fuel, especially in rural and peri-urban areas.3,7,8 In Malawi’s rural and urban households, Fullerton et al. 9 found average levels of PM2.5 10 times higher than the 25 µg/m3 limit recommended by the World Health Organization (WHO). In these developing countries, where children keep their mothers company during meal preparation or housework, more than two-thirds of deaths are caused by indoor air pollution.3,4,10,11 Exposure to biomass smoke could double a child’s risk of lower respiratory tract infection, 11 pneumonia 12 or acute respiratory failure. 13 It could also contribute to asthma.3,4,12,14
Biomass represents almost 70% of energy sources in Côte d’Ivoire households, 15 but few studies have measured exposure levels and health effects of the pollution that ensues. Moreover, poorly managed urbanization has placed numerous households in a precarious state in a peri-urban zone. Physical degradation of this habitat compounds the issue of fumes from solid fuels, affecting the health of inhabitants. Consequently, any health promotion activity should take into account relevant data on indoor home environments. As affirmed in the Sundsvall Statement 16 and by Cicolella, 17 health represents the quality of people’s relationship with their ecosystem. Our study is part of an EcoHealth project intended to stimulate community participation in solving health problems through better environmental control. 18 In addition to emissions from biocombustibles, we examined the physical characteristics of risks to the health of tenants exposed to intra-domiciliary pollution. Our objectives were to determine the prevalence of respiratory symptoms among children under five years of age and to identify potential risk factors related to indoor home environments and living conditions.
Methodology
Study setting
Our study was conducted in the Anonkoi 3 neighbourhood, which is administratively linked to the Abobo commune in the north end of Abidjan City, the economic capital of Côte d’Ivoire. It is the second most populated commune in the Abidjan district, with a density of 167 inhabitants per hectare. Its moist, tropical climate provides two rainy seasons, a long one from April to July, and a short one from October to November, and two dry seasons, a long one from December to March and a short one from August to September. Rainfall reaches 2500 mm during the rainy season and 1600 mm during the dry season. The maximum temperature during the dry season is 33℃, which drops to 27℃ during the rainy season. Humidity levels vary from 80% in the dry season to 90% in the rainy season.
Anonkoi 3 was built around a village near one of Abidjan’s first railway stations. It comprises pavilion style and multi-unit homes in a wide variety of architectural styles. Its cosmopolitan population was estimated to be 4215 inhabitants in 2009, including 544 children under five years of age. 19 The 1998 general population and housing census counted 474 households in this neighbourhood.
Data collection and processing
The study was designed as a cross-sectional survey carried out from May to July 2010 (during the long rainy season). All households were visited to enroll children under five years of age living in the neighbourhood. This exhaustive survey was conducted door to door, and all duly-identified children under five years of age were retained. A transdisciplinary team formed for the purpose collected data with a pre-tested questionnaire. The data collection team was assisted by community health workers who helped gain access to households. The study received written ethics approval from West Abobo health district authorities and Anonkoi 3 community leaders. The target children’s mothers or guardians were interviewed after giving their verbal consent.
The questionnaire concerned demographic and health information on the children, type of dwelling, fuel and tobacco consumption in the home, mothers’ age and profession as well as the proximity of mothers to their children or lack thereof during meal preparation.
The presence of respiratory symptoms (cough, cold, rapid breathing, difficulty breathing) in children in the 15 days prior to the survey was verified during the interview. Team doctors also checked for these signs on the day of the survey.
Health inspection was undertaken with an observational checklist to gather data regarding various characteristics of the buildings and other indoor sources of air pollution. Items on the checklist concerned the number of rooms and openings, the transversal or non-transversal arrangement of openings, the presence of mould/mildew in dwellings and adequate ventilation (open doors and windows).
In each household retained, humidity levels and temperature were measured by thermohygrometer with an accuracy of ±3% for relative humidity and ±0.5℃ for temperature.
The average number of openings per room was calculated for each household by dividing the number of functional openings by the number of rooms. We defined a ‘physical quality of the dwelling’ variable that consisted of mould/mildew, humidity level, temperature and average number of openings per room. The physical quality of the dwellings was deemed to be altered if one or several of the following conditions was or were observed: mould/mildew, humidity level ≥90%, temperature ≤30℃ or average number of openings per room <2. Households were then divided according to the number of factors altering physical quality of the dwellings.
Statistical data analysis
Data were collected with Epidata 3.1 and analysed by SPSS 12.0. Standard descriptive statistics served to characterize indoor environment and the prevalence of respiratory symptoms.
Chi-square test was applied for the univariate analysis of respiratory symptoms according to potential risk factors. Logistic regression included variables that proved to be statistically significant in univariate analysis. Adjusted odds ratios (OR) and their 95% confidence intervals (95% CI) were calculated. The significance level of the statistical tests was fixed at 5%. All reported p values were two-sided.
Results
Indoor household environment
The survey involved 681 households, of which 23.9% lived in courtyard housing. Mould/mildew was observed in 26.3% of households, and the average number of openings per room was <2 in 10.4% of households. Home ventilation was inadequate in 60.6% of households owing essentially to the non-transversal arrangement of openings (43.6%) and the presence of window obstructions (33.2%), as reported in Figure 1.
Reasons for inadequate ventilation in peri-urban homes in Anonkoi 3, Abidjan, 2010: n (%).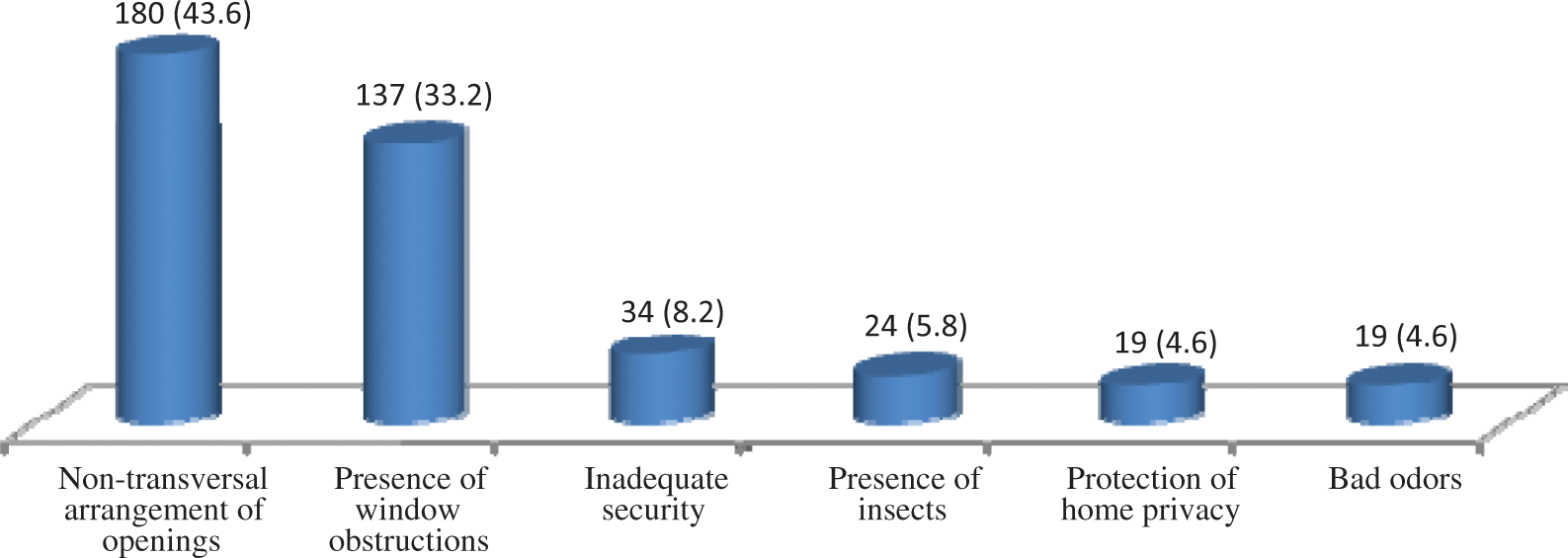
Average temperature and humidity level (standard deviation) in 622 households were 30.2℃ (1.9) and 76.5% (10.5), respectively. Gas was the sole combustible energy source in 27% of households. Solid fuels associated or not with gas were burned in other households. There was at least one smoker in 16.9% of households. Figure 2 provides a breakdown of these households according to the number of factors degrading physical quality of the dwellings.
Breakdown of households by number of factors altering the physical quality of dwellings in a peri-urban area, Anonkoi 3, Abidjan, 2010: n (%). 0: no factor; 1: 1 factor; 2: 2 factors; 3–4: 3–4 factors.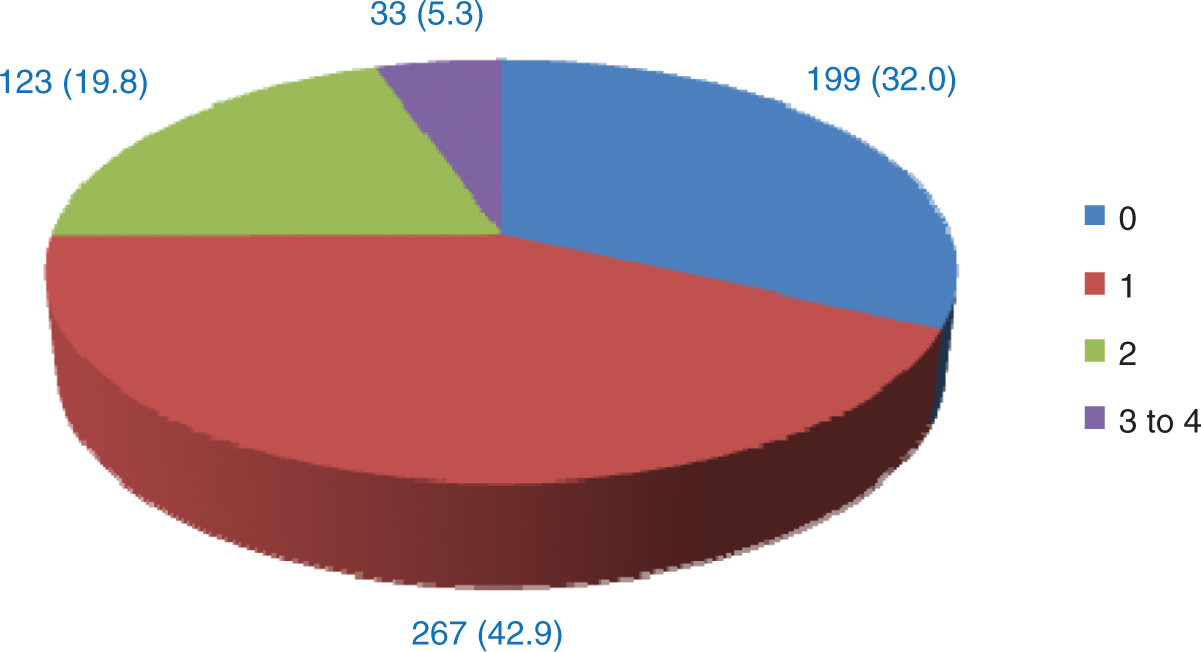
Children’s and mothers’ characteristics
From a total of 924 identified children under five years of age, 734 mothers provided information on 899 children recruited in 681 households, that is to say, 1.32 children under five years of age per household. The children’s average age (standard deviation) was 26.0 (16.9) months and the gender ratio was 1.09. The mothers’ average age (standard deviation) was 30.1 (7.1) years. Among the mothers, 37.1% were housewives, while 35.3% were informal sector workers, 14.8% were administrative or service employees and 12.3% were students. Approximately one-quarter (26.3%) of mothers carried their children or kept them close during meal preparation.
Respiratory symptoms and risk factors (Tables 1 and 2)
Respiratory symptoms and related factors among children under five years of age in Anonkoi 3, Abidjan, 2010.

Physical quality of dwellings: mould/mildew present + <2 openings + temperature ≤30℃ + humidity > = 90%. 0 = no factor; 1 = 1 factor; 2 = 2 factors; 3 to 4 = 3 to 4 factors.
Respiratory symptoms among children under five years of age in Anonkoi 3, Abidjan, in 2010, and predictive factors (final logistic model).
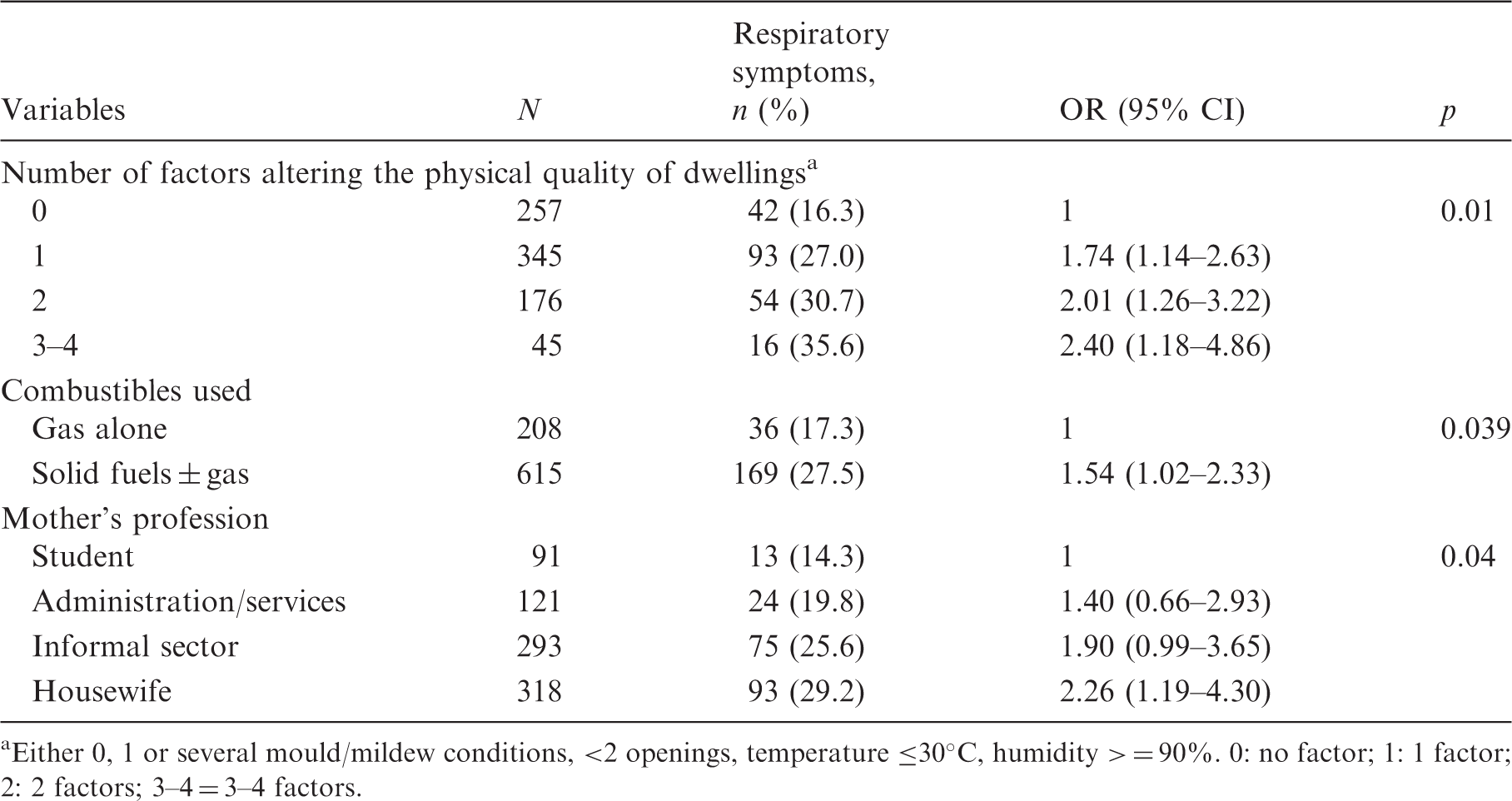
Either 0, 1 or several mould/mildew conditions, <2 openings, temperature ≤30℃, humidity > = 90%. 0: no factor; 1: 1 factor; 2: 2 factors; 3–4 = 3–4 factors.
Discussion
In this study, the relationship between factors that degrade indoor air and respiratory symptoms in children under five years of age was examined in a peri-urban neighbourhood of a developing country with West African inter-tropical climate. Combustion-related factors were associated with respiratory symptoms, as was the ‘physical quality of dwellings’ variable, which comprised temperature, humidity, mould/mildew and average number of openings per room.
Case definition for measuring the prevalence of illnesses was based on respiratory symptoms typically encountered in community-based Integrated Management of Childhood Illness. 20 In fact, these symptoms, which mothers recognize easily, are helpful in promoting community understanding of health problems. However, this definition lacks specificity and leads to the grouping of cases of severe and/or chronic lower respiratory tract illnesses with cases of minor upper respiratory tract illnesses. It probably results in classification bias that underestimates OR values. Nevertheless, potential risk factors usually reported in the literature were found in our study.
High humidity levels and high temperatures have been identified as factors that increase the risk of respiratory illness with thresholds of 50% and 20℃ in temperate-climate countries. 5 However, during our investigation in a tropical zone, the prevalence of respiratory symptoms was greater for humidity levels higher than or equal to 90% or temperatures lower than or equal to 30℃. These observations may be partly attributed to the rainy season, where homes are closed up for long time periods, promoting mould and mildew. An insufficient number of openings per room provides inadequate ventilation and accentuates the above-mentioned factors. The physical quality of the dwelling variable was therefore constructed to assess the effect of combining these altering factors on indoor air degradation and, ultimately, on respiratory symptoms. The increased risk of respiratory symptoms with the accumulation of factors modulating the physical quality of dwellings reflects their synergetic effects in the degradation of indoor air quality.
Even when indoor–outdoor air exchanges allow satisfactory ventilation, the amount of pollutants emitted from solid fuels remains significant, and their concentrations in homes as well as related exposures may be high. 11 Solid fuel use is therefore universally linked to respiratory illnesses.3,4,9,13,14,21,22
These conditions, which increase the risk of respiratory illnesses, could combine, particularly in the homes of children whose mothers are housewives and where poverty promotes the consumption of these lower-cost solid combustibles.9,23,24 Furthermore, lack of financial means delays healthcare and maintains a high prevalence of respiratory symptoms. These households thus accumulate social health-inequality factors. 25
Our study helped to identify objective elements of a population’s living conditions that are associated with a high risk of respiratory symptoms among children under five years of age. These elements indicate socio-economic behaviours and characteristics that need to be addressed to reduce the burden of respiratory illnesses in the community.
Conclusion
Children’s respiratory health is affected by biofuel use, poverty and the presence and accumulation of unfavourable physical factors. Authorities need to pay closer attention to this interaction between children’s health, dwellings and poverty. The links observed between indoor environmental quality and respiratory health must, of course, be verified by other studies. In this regard, our work delivers elements that can help guide future research. Furthermore, a comprehensive approach to health, linking public health actors as well as building, housing and social policies should be considered.
Footnotes
Acknowledgements
The authors thank the West African Health Organisation (WAHO) for financial support that allowed finalization of the thesis which inspired this article. Thanks are also due to Mr. Ovid Da Silva for translation of the original text to English.