
Abstract
Many studies have demonstrated the adverse effect of the built environments on health and differentiated between their direct and indirect impacts. In the case of diabetes and other chronic diseases, such studies concentrate on the direct impact of built environments on the living conditions of citizens either at home or in the neighbourhood. In the Kingdom of Saudi Arabia (KSA), little research has tackled the indirect and so-called place-based impact of the built environment. This study reports on the findings of surveys carried out on 76 diabetics who usually visit the King Fahd Teaching Hospital of the University of Dammam, Al-Khober in the Eastern province of KSA. It investigates the relationship between the place-based impact of the built environment, diabetes and living conditions. The working hypothesis is that: living conditions found in the homes and surrounding neighbourhoods of those suffering from diabetes do aggravate the symptoms of the disease, which in turn have an adverse impact on the medical condition. The study provides evidence to support this hypothesis as the findings reveal there is a positive correlation between the place-based impact of built environments, diabetes, living conditions, homes and neighbourhoods and these jointly aggravate the symptoms associated with the medical condition.
Introduction
Focusing on the place-based impacts of the built environment, this paper studies how living conditions, homes and neighbourhoods affect the physical, social and emotional health of those suffering from the medical condition known as diabetes. Under this notion of place-based impacts, the paper offers a review of the literature currently available on built environments and relationship between diabetes and living conditions. It then goes on to examine the place-based impacts of built environments in terms of the relationship diabetes has to living conditions, homes and neighbourhoods. In particular, in terms of the place-based impacts that living conditions found in the homes and neighbourhoods of diabetics on their physiological, social and emotional health.
The material for this study of how living conditions, homes and neighbourhoods influence the physical, social and emotional health rests on a survey of 76 diabetic patients treated for this medical condition at the King Fahd Teaching Hospital (KFUH), University of Dammam, Al-Khober, Kingdom of Saudi Arabia (KSA). For the purposes of the study, qualified medical practitioners determine the diabetic patients’ physical, social and emotional health, while experts in the architecture and planning sector assess their living conditions, homes and neighbourhoods. The study also uses analysis of variance (ANOVA) tests and structural equation modelling (SEM) techniques to evaluate how living conditions, homes and neighbourhoods combine to affect the physical, social and emotional health of the diabetic patients. Discovering a positive correlation between the diabetic patients’ living conditions, homes and neighbourhoods and symptoms associated with the disease, this place-based impact assessment goes on to uncover those factors within the built environment having an adverse effect on their health.
The placed-base impact of built environments
Barton et al. 1 classify the impact of the built environment on health as twofold: direct and indirect. Direct impacts include those which are traditionally associated with environmental planning, e.g. water and drainage, air quality, noise and traffic-related injuries, whereas indirect impacts are place-based and include the way that buildings, homes and neighbourhoods in turn influence the physiological, social and emotional determinants of health.
Schootman et al. 2 studied the place-based impact of built environments. Based on the survey of homes and neighbourhoods, they examined the effects of unhealthy built environments on the physiological, social and emotional determinants of health. In terms of the home, they identify a number of factors determining physiological, social and emotional health. These include the following: cleanliness of the home, physical condition of the building's interior and exterior and state of the furnishings. In terms of neighbourhoods, much of the research undertaken seeks to examine the potential impact of neighbourhoods on health (e.g. Kawachi and Berkman 3 and Sampson et al. 4 ). Balanda and Wilde 5 and Frumkin et al. 6 link unhealthy built environments to physiological, social and emotional health, including cardiovascular disease, obesity and mental health. With regards to cardiovascular disease, obesity and mental health, Handy 7 notes those living in more “walkable” neighbourhoods, characterized by high population density, mixed land use and high levels of connectivity (e.g. good pedestrian and cycling facilities), are more physically active and as a consequence, less likely to experience cardiovascular disease, obesity and mental health.8–11
Diabetes
Diabetes mellitus is the most common non-communicable disease worldwide and the fourth leading cause of death in developed countries. 12 There are, in general, two types of diabetes. In diabetes type I (T1DM), the body itself has destroyed the insulin-producing beta cells in the pancreas. Although type II diabetes mellitus (T2DM) can have a genetic origin, unhealthy lifestyle is in fact the main cause. Common early warning signs include: frequent need to urinate; increase in thirst; rapid weight loss; blurred vision; rash or itching skin that can result in an infection; frequent tingling sensation in the hands and feet; and fatigue. While the direct symptoms of diabetes, such as thirst, frequent micturition and fatigue, can be mild and may cause little interruption to the activities of daily living, it is the complications of the disease that cause greatest concern, for example, blindness in adults 13 and non-traumatic lower-limb amputation. 14
The World health Organization (WHO) was the first to challenge the health of built environments. Their research recognises that between 10% and 30% of newly built developments have indoor environments, which cause allergic reactions. 15 While research into the design and construction of buildings has been unable to offer a clinical diagnosis of these allergic outbreaks, the study of diabetes does not experience such difficulties. This is because diabetes is a recognised medical condition and allergic reactions such as: lethargy and tiredness, headache, dry blocked nose, sore dry eyes, sore throat, dry skin and/or skin rashes are symptoms of the disease.
In this respect, Youle 15 and Morris and Hawkins 16 found that air-conditioning systems give rise to allergic symptoms. Apte et al. 17 have also found an association between ventilation rates, CO2 (i.e. carbon dioxide) concentration and diabetes symptoms. Particle pollution equal to or less than 10 µm in diameter (PM10) also leads to an outbreak of diabetic symptoms (see also Nemmar et al. 18 ).
Environmental pollution also affects the number and function of sweat glands in diabetic patients. This reduces the volume and rate of evaporation needed for the body to dissipate heat. This can considerably increase the risk of hyperthermia and heatstroke. 19 Diabetics with cardiovascular diseases are also more susceptible to the detrimental effects of environmental pollution. 20 This means patients are at a greater risk of admission to hospital during heighted periods of environmental pollution and even dying from such symptoms.21,22
Many studies have also shown a relationship between PM10 and diabetes.23,24 Long-term exposure to environmental pollution particles (2.5 µm in aerodynamic diameter (PM2.5)) is associated with a higher relative risk of mortality among people with diabetes, compared to the general population. 25 Other studies show environmental pollution linked with the development of T1DM. 26 Pearson et al. 27 found a similar association between the prevalence of T2DM and PM2.5. They investigated the relationship between diabetes and traffic-related NO2 (i.e. nitrogen dioxide) and found an association between the outbreak of diabetic symptoms and exposure to traffic-related NO2. An association between environmental pollution and the pathogenesis of diabetes, especially in children and adults with cardiovascular diseases, is also identified. 28
Studies of living conditions shift attention away from the epidemiology of diabetes and broaden the examination, to include how habit-persistent practices contribute to the medical condition. These include poor diet and “bad behaviours”, such as: smoking, alcohol consumption and lack of physical exercise. Ebbeling et al. 29 saw such habit-persistent practices as imbalances between energy intake (i.e. food consumption) and expenditure (i.e. physical activity), a situation leading to obesity. Another medical condition closely aligned with the spread of the disease.
Studies of living conditions also show how the design and layout of homes affect the spread of the disease. In this regard, Allanah et al. 30 found that badly designed homes and neighbourhoods lead to bad behaviours, which in turn contribute to the development of T2DM. Peckhan 31 and Eckel et al. 32 have also linked the absence of physical activity with diabetes. These studies propose physical activity would reduce the symptoms of coronary heart disease and strokes associated with T2DM. 6 Those living in more “walkable” neighbourhoods, characterized by high population density, mixed land use and high levels of connectivity (e.g. good pedestrian and cycling facilities), have been identified to be more physically active.9,10
In the interests of tackling diabetes, Frank and Engelke, 33 Frank et al. 9 and Pikora et al., 10 all suggest “healthy lifestyles” exist in neighbourhoods with high population densities. By this they mean, high-density neighbourhoods, within built environments made up of mixed land uses. Mixed land uses with diverse structures of tenure and green spaces that also have good connectivity (e.g. easy routes between destinations), public transport, pedestrian and cycling facilities, which combine to not only manage the effect of bad behaviours on the medical condition, but also control the habit-persistent practices responsible for the spread of the disease.
Living conditions, homes and neighbourhoods in KSA
There are a number of housing arrangements in KSA such as: gated compounds of different sizes and facilities; terraced housing, villas, blocks of flats, or mixed development. These also conform to social status, such as deprived and poor areas; middle- and high-income neighbourhoods. The facilities, level of finishing, furnishing and cleanliness varies from one district to another. There is also the irregular provision and access to community facilities. In particular, amenities such as: gardens, parks, leisure and recreation to take account of. 34 Accordingly, each of these spatial arrangements will have a unique effect on occupant’s health and well-being.
KSA has one of the highest percentages of diabetes in the world, with an estimated 3,414.51 people diagnosed with the disease in 2012, which is 23.38% of the population. 12 Previous surveys from the KSA suggest that diabetes is present in epidemic proportions throughout the country, with exceedingly high rates concentrated in urban areas. 35 Al-Hazzaa et al. 36 conducted a survey on the Saudi people in major cities across the KSA. They found the majority of Saudi adolescents spent more than 2 h watching TV, and around half of them do not meet the daily physical activity requirements. Around a quarter do not consume the recommended daily portions of milk, fruits and vegetables. Also, around a quarter of them have high daily intake of unhealthy food and drinks such as French fries, cakes and donuts, energy drinks and candy and chocolate (ibid). As diabetes also affects the functioning of sweat glands, it decreases both the volume and rate of evaporation. During heat waves, this can considerably increase the risk of hyperthermia and heatstroke.37–39,19
In spite of this, relatively little research has been conducted on the impact which the built environment has on diabetic patients in KSA, even though it is evident that living conditions
40
do aggravate the symptoms.
41
However, what is known is the:
rapid growth of industrial cities produces high air pollution in many cities across KSA;
42
this in turn generates an alarming increase of sulphur dioxide (i.e. SO2), nitrogen dioxide (i.e. NO2), carbon monoxide (i.e. CO) and particulate matter (i.e. PM) emissions in the Eastern province;
43
the extreme hot, dry and humid weather these conditions create also affects the type of activities they engage in; Saudis tend to engage in unhealthy activities: such as irregular sleeping patterns (e.g. afternoon nap, sleeping late), evening or late night trips to local malls and shopping arcades or sitting in coffee shops, late night’s heavy meals and these activities replace outdoor activities, such as children’s playgrounds and walking children to school;
34
poor living conditions add to these problems and adversely affect the health of all citizens, particularly those with diabetes.30,41 For as Sidawi and Meeran
44
and Sidawi
45
note: such living conditions make it difficult for diabetics to enjoy walking around their neighbourhoods due to the extreme hot, dry and humid weather conditions and high level of air pollution within cities; particular cultural issues should also be taken into consideration when exploring the relationship between diabetics and living conditions.44,45 These include the Islamic lifestyle, with as many as five daily trips to the mosque to perform prayers, Ramadan Fasting, pilgrimage to Makkah, gender segregation, regular male gatherings in the community centre and strong tribal and family ties.
The research objectives and methodology
The aforementioned literature makes valuable contribution to our understanding of the relationship between the place-based impact of built environments and diabetes. With respect to this contribution, the following aims to explore the effect that living conditions, homes and neighbourhoods have on the health of diabetics in the Eastern Province of KSA. The specific objectives of the study are:
to establish the strength of the link between the medical condition, physiology of the disease and reported symptoms in relation to the patients: perception of their living conditions; home and neighbourhood; to determine how the combined poor indoor and outdoor environments could have aggravated the symptoms of the disease; to identify the key factors (within the home and their surrounding neighbourhoods) that could affect their physiological, social and emotional health.
Consent to carry out the study was first obtained from the University’s ethics committee. The fieldwork began in January 2013 and drew upon a sample of diabetics who usually visit the medical clinic at the KFUH of the University of Dammam, Al-Khobar. This list of patients includes T1 and 2DM male and female adults, age 15–70 years and resident in the Eastern province, KSA.
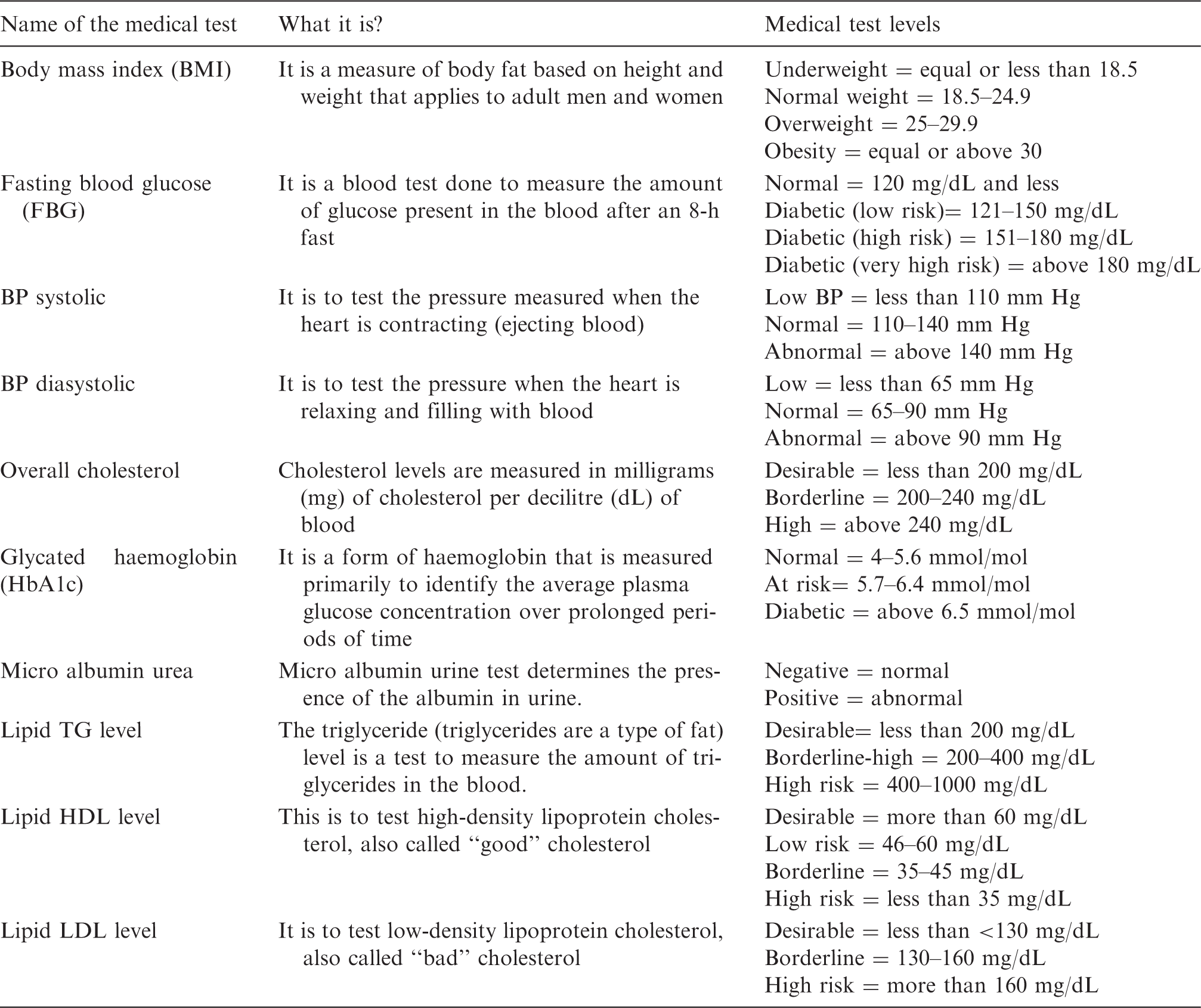
The definitions of medical tests and the measurement level for each patient.
After 12 months (i.e. in December 2013), the medical reports were reviewed and compared with the previous examination. The data collected from the physical examination and questionnaire survey has been analysed using SPSS 16 and Amos. This analysis calculated the mean, standard deviation, skewness and percentages for use in the ANOVA and SEM. The results of this modelling serve to test the effect of an independent variable on a dependent variable. This is analysed through a number of co-variables. Only ANOVA and SEM relations having a significance value (i.e. p < 0.05) are reported on. The levels of significance considered are as follows: p < 0.05 as the common level: p < 0.01 as the moderate level and p < 0.001 as the high level. These significance levels in turn determine whether the association between two variables is likely, highly likely, or very highly likely to exist in the population (i.e. in diabetic patients throughout the KSA). Any positive correlation means that two or more variables change in the same direction and in the same proportion, and vice versa.
While data obtained on living conditions, homes and neighbourhoods relates to the patients’ own self-evaluations of their condition, the fact these interpretations of the symptoms are linked to two clinical assessments of their physiological health is seen to give the study particular weight. For this way, i.e. by connecting the self-evaluation to the clinical assessment, it becomes possible to put critical distance between them and correlate the perceptions of health with the medical condition. That is to say, subject the relationship between them to statistical tests, which correlate the significance of living conditions, homes and neighbourhoods to the physical, social and emotional health of diabetic patients.
While previous research has focused on the impacts of built environments on the physical, social and emotional health of diabetic patients, the effect, which indoor and outdoor environments, vis-a-vis living conditions within the home and throughout the neighbourhood on the medical condition, is something that is unique to this particular study.
Findings
Physical, social and emotional health
This survey found that 32% of the diabetics have a positive level of micro albumin urea and 66% of them are overweight or obese. It also found 17% have a FBG level of above 200 mg/dL and that 88% of the participants have HbA1c levels above 6.5, which is above diabetic level and 47% of the patients have borderline or high risk HDL. The most frequent diabetes manifestations experienced are: extreme fatigue and related tiredness, tension and stress, blurred vision and inability to control their nervous system. Whereas the least experienced symptoms are: cardiatric problems, loss of sensation, loneliness and isolation and blood pressure problems.
The study has compared the medical results of two examinations (i.e. January and December 2013) and presented in terms of the respective micro albumin urea, FBG, HbA1c, cholesterol, lipid TG level, lipid HDL level and LDP level. The medical tests revealed that the percentage of patients who have high level of HbA1c and low level of lipid HDL level (i.e. risky level of good cholesterol) increases from January to December 2013 (i.e. for HbA1c; 96% vs. 100% and for HDL; 80% vs. 88%). The self-reported domestic and social life of upper-income groups do reveal some bad habits such as watching TV or working longer hours at the office. However, it also found those within low-income groups suffer adversely from living conditions at home and in their surrounding neighbourhoods, because unlike their counterparts they experience such symptoms as blurred visions, burning sensations, numbness of limbs and stress.
Living conditions
In terms of diet: 48–59% rarely or never drink fizzy drinks or eat junk food meals and 86% of the respondents said that they never or rarely smoke. Approximately 77% said that they often or always eat fruits and vegetables. When asked about their home and social lives, more than half of them (57%) said while at home they never or rarely engage in physical activity. Also, 33% said that they never or rarely participate in religious activities. Indeed approximately 25% rarely or never walk for more than 30 min a day and only 48% said they walk for 30 min. As much as 41% say they never or rarely get involved in social activity.
Home and neighbourhood
The frequency of experiencing indoor and outdoor environmental conditions (note: this has been grouped by gender).
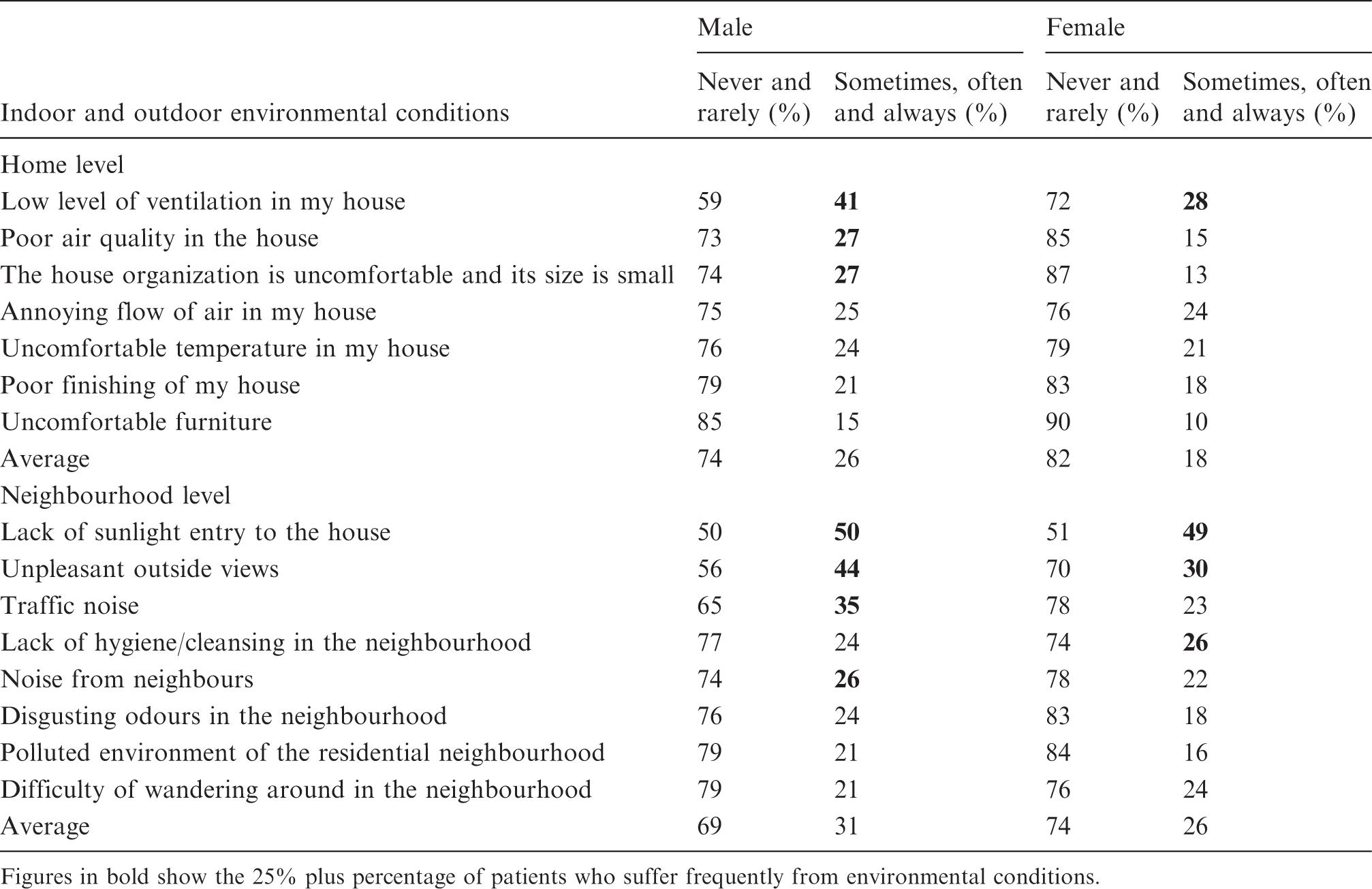
Figures in bold show the 25% plus percentage of patients who suffer frequently from environmental conditions.
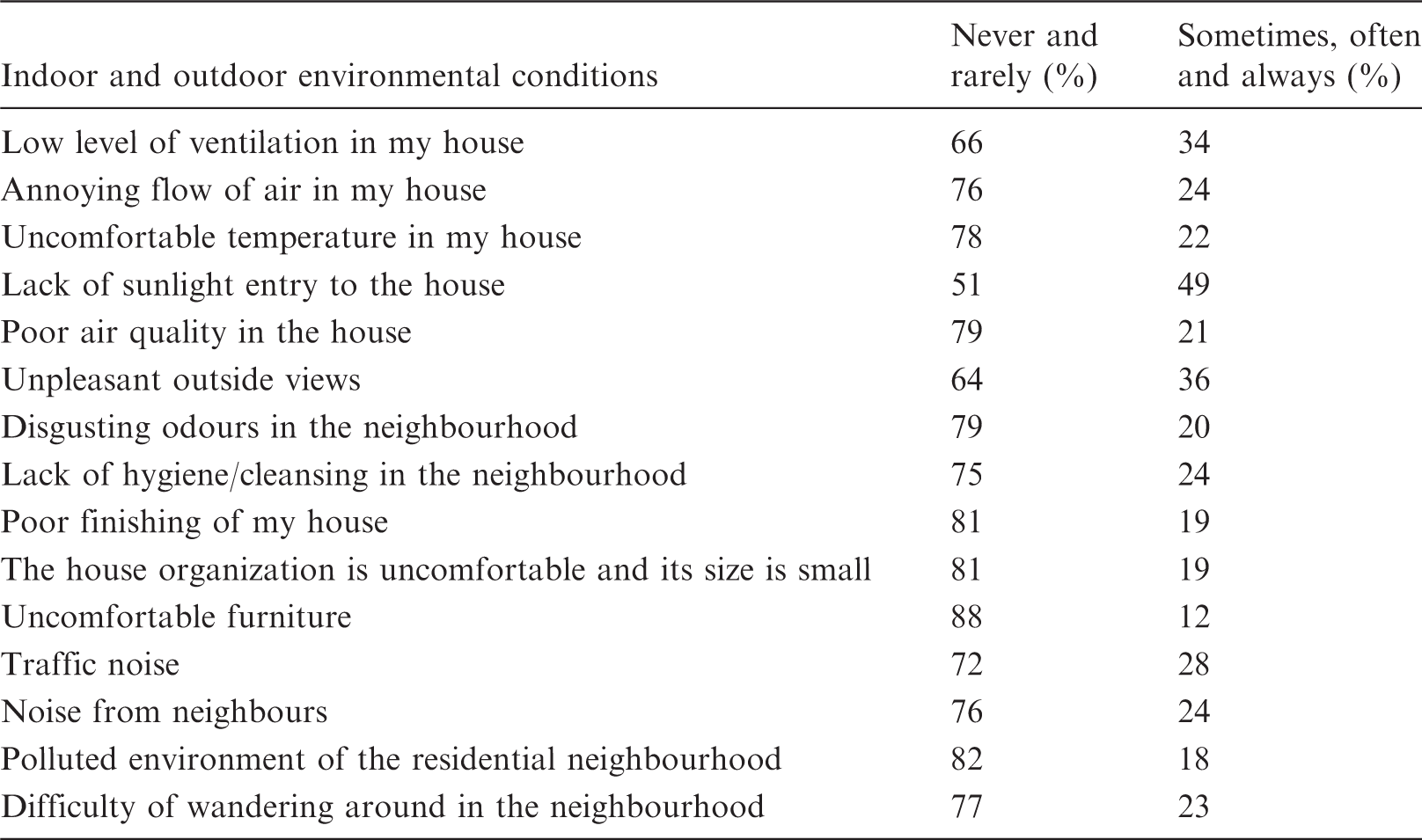
The percentage of diabetic patients (i.e. the whole sample; males and females) experiencing indoor and outdoor environmental conditions.
More than the quarter (i.e. 26–35%) of the male respondents also indicate they more frequently suffer from following home conditions:
poor air quality in the house; the organization of the home is uncomfortable and too small.
Within the surrounding neighbourhoods, the same percentage of male respondents above indicated they suffer from:
a lack of sunlight within the house; unpleasant outside views.
Here approximately 28% of the female respondents said that they more frequently suffer from one particular home condition i.e. low level of ventilation in the house.
In respect to their surrounding neighbourhoods, the same percentage above, said they suffer from:
traffic noise; noise from neighbours.
More notably around half of the female respondents said that they more frequently suffer from a lack of sunlight entry to the house. More than a quarter of the female (i.e. 26–30%) respondents also indicate they more frequently suffer from the following neighbourhood conditions:
unpleasant outside views; a lack of hygiene/cleansing in the neighbourhood.
The results however show differences between the patients occupying the homes and neighbourhoods. For example, grouping respondents in respect to the gender indicated differences between males and females.
The most frequent reported factors for males are: a lack of sunlight entry to the house, unpleasant outside view, low level of ventilation in the house and traffic noise. The most frequent annoying factors for females are: a lack of sunlight entry to the house, unpleasant outside view and poor level of hygiene in the neighbourhoods. Some factors: such as low level of ventilation in my home are experienced more by males, than by females. The neighbourhood conditions are more annoying for both males and females than home conditions. In addition, the home conditions are more irritating for males than females (see Table 2).
When asked about the distance between their homes and amenities of their surrounding neighbourhoods, more than half of the respondents said amenities are within walking distance, i.e. up to 500 m, whereas 24% said they are more than 1000 m from where their homes. Around 23% of the respondents said the public garden is more than 2000 m from their home. An additional 28% said that the recreation and sport centre is more than 2000 m away.
ANOVA results of January 2013’s investigation
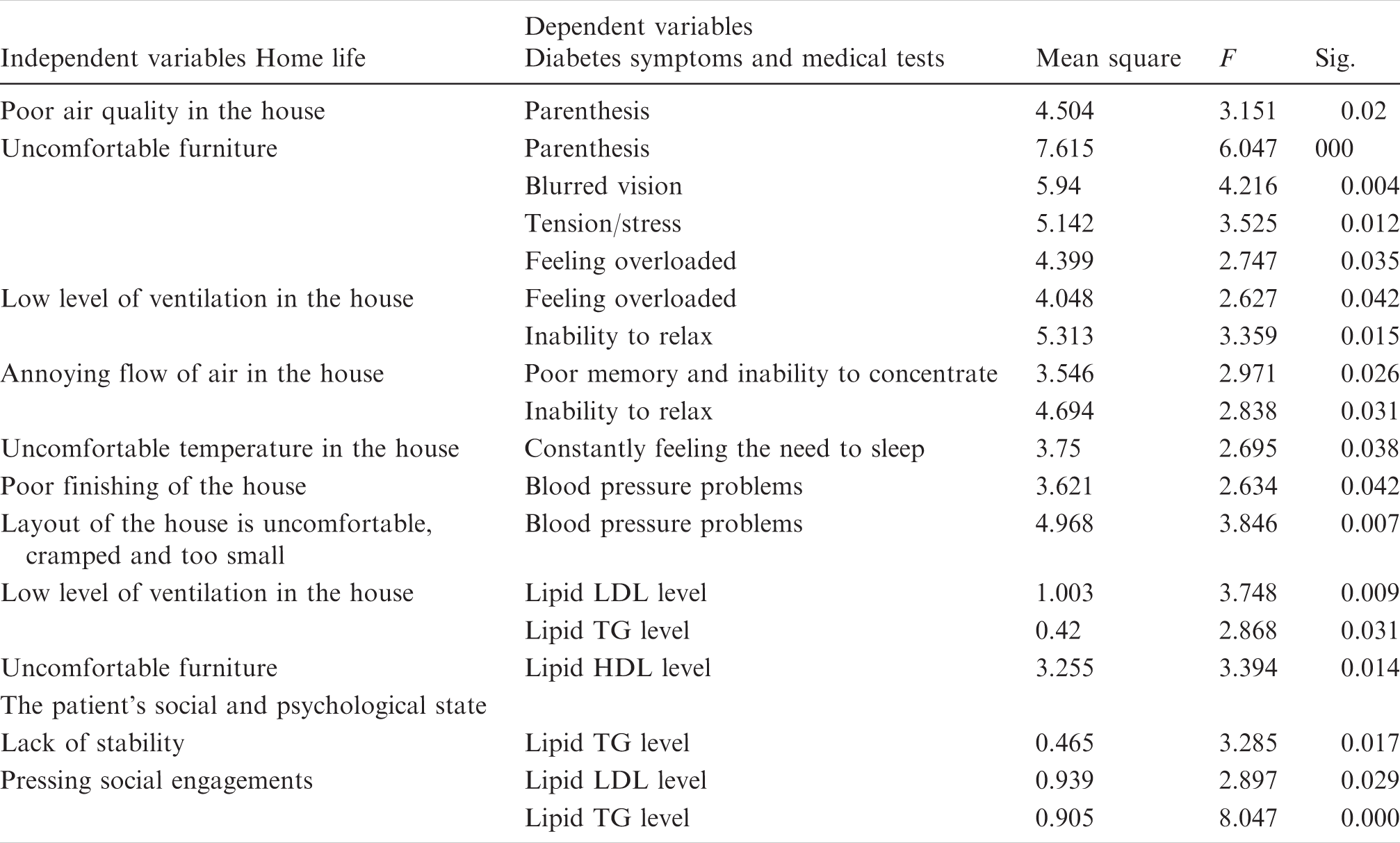
The relation between the home conditions with diabetes symptoms and January’s medical tests (note: ANOVA test significance level <0.05, sample size 76).
The relation between the home conditions and the patient’s social and psychological state with December’s medical tests (note: ANOVA test significance level <0.05, sample size 76).
The ANOVA results also show the indoor environment experienced at home and as part of the patients’ domestic arrangements are linked with the disease’s symptoms. For as Table 4 indicates, patients who more frequently experience a low level of ventilation in their homes, say that they more frequently feel stressed. Those who frequently experience an annoying flow of air in their homes, say they more frequently suffer from a poor memory, and an inability to concentrate and relax. Uncomfortable temperatures also cause problems, because it constantly forces the patient to sleep.
Those who suffer more frequently from the poor air quality say they experience paresthesia, i.e. symptoms relating to blurred visions, burning sensations, numbness of the limbs and stress. Patients, who experience uncomfortable furnishings, say that they suffer more frequently from blurred vision, numbness of the limbs, and stress. Those who reported a poor finishing of their homes or the layout of their homes to be uncomfortable, say they more frequently experience problems associated with high blood pressure (see Table 4). This ANOVA study also reveals an association between the medical test results, the patients’ living conditions and domestic arrangements. For example, those who suffer more frequently from low level of ventilation in their homes have higher lipid low-density lipoprotein (LDL) and TG levels. Patients who reported disgusting odours and high levels of pollution in their neighbourhoods said they more frequently suffer from symptoms relating to blurred visions, burning sensations, numbness of the limbs and stress.
The ANOVA results show significant link between increasing levels of instability at home with a higher level of lipid TG level. They also indicate an increasing level of social pressure associated with the higher level of lipid LDL and TG levels the analysis captures.
ANOVA results of the December 2013’s examination
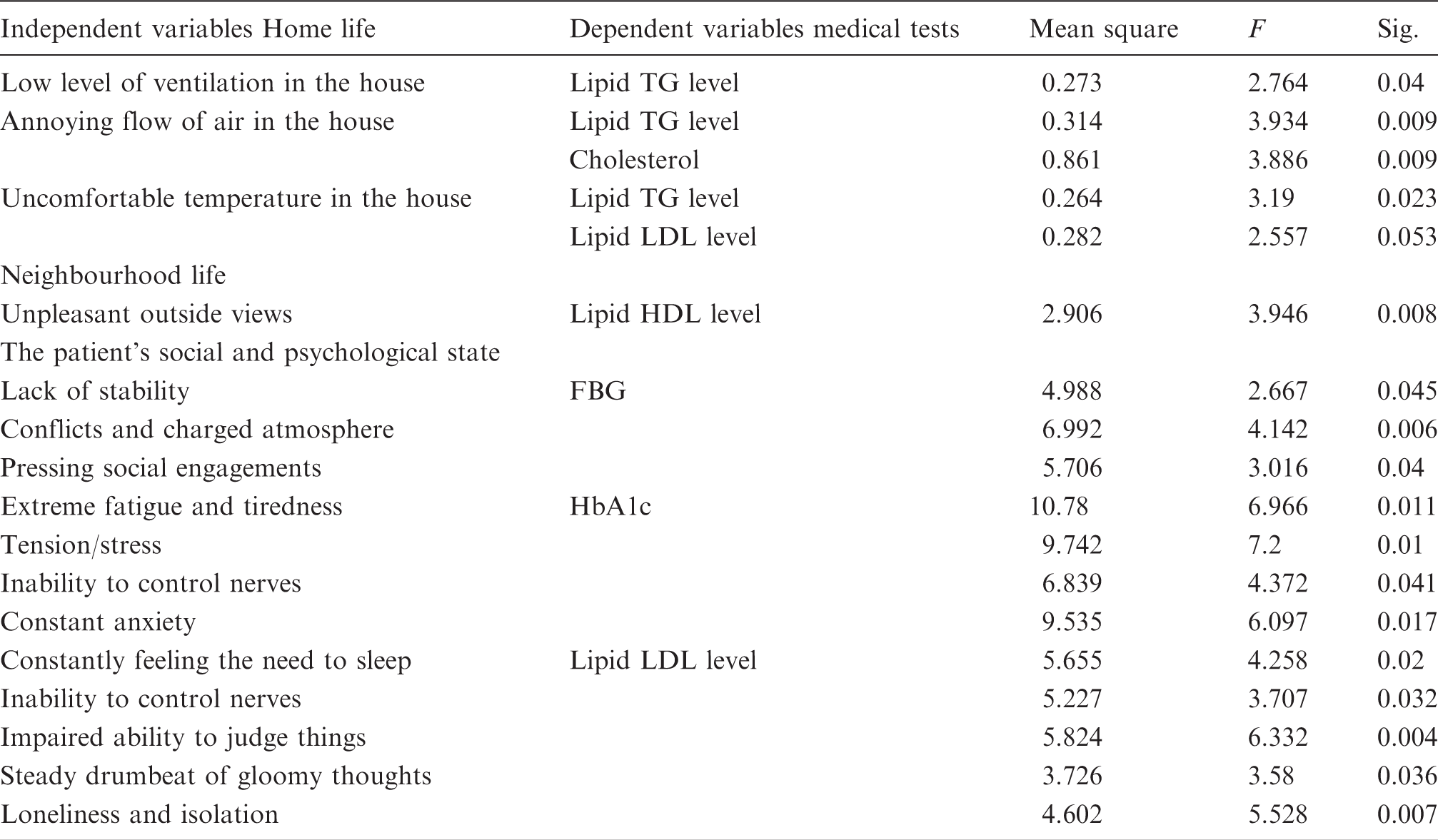
The December 2013 examination highlights the significant relation between the place-based impact of the built environment (i.e. as reported on in the previous section) and pathology of the disease revealed by the clinical tests carried out by KFUH, the University of Dammam. For instance, the ANOVA study found:
low levels of ventilation in the patient's house is associated with a higher lipid TG level; inadequate circulation of air in the patient's home is associated with higher cholesterol and lipid TG levels; higher temperatures in the home are associated with higher lipid TG and LDL levels; unpleasant outside views of the neighbourhood are associated with lower (i.e. risky) lipid HDL levels (Table 5).
This study has also found there is a significant link between social and emotional parameters of the examination and results of the medical exam. For example, the study found there is a link between the lack of stability in domestic arrangements, conflicts, social pressure and emotionally charged atmosphere with higher levels of FBG. It also found increased levels of HbA1c are associated with higher levels of the followings: extreme fatigue and tiredness, tension and stress, impaired nervous systems and an increased state of anxiety. Increased levels of lipid LDL are also associated with higher levels of the followings: constantly feeling the need to sleep, nervous disposition, an impaired ability to judge things, steady drumbeat of gloomy thoughts, loneliness and isolation (Table 5).
This suggests that while being treated by physicians for the disease, the symptoms have become aggravated, but as there is no medical reason for this, the explanation for this escalation must lie in “environmental factors” relating to their living conditions, home and surrounding neighbourhood.
Results of SEM
Here the aim is to test whether these poor indoor and outside environments in turn relate to the home and neighbourhood. In addition, whether indoor environments combine with outside environment to aggravate the physical, social and emotional health of diabetic patients. So for each SEM diagram (see Figure 1 as an example), the study investigates the effect one of the neighbourhood attributes (as an independent variable) has on all of the homes indoor environments and medical condition of the patient (as a dependent variable). Only significant results (i.e. p <0.05) are reported below.
The SEM diagram showing the relation between the independent variable noise from neighbours on the dependent variable micro albumin urea. The indoor conditions act as mediating variables (note: the diagram shows the standard regression weights only). SEM: structural equation modelling.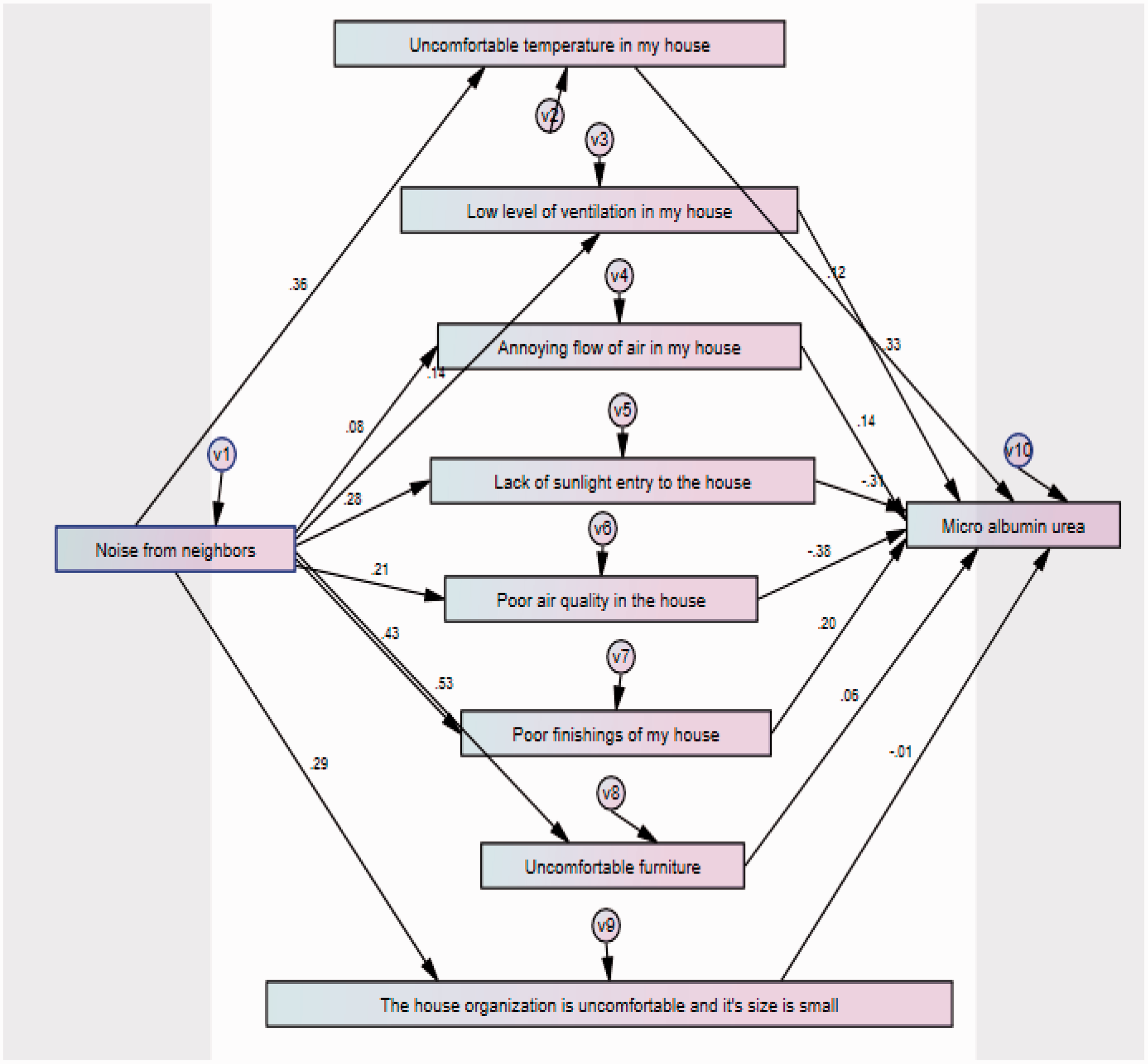
In general and as expected, the SEM figures showed homes and neighbourhoods act together in aggravating the physiological, social and emotional health of diabetics. For example, homes and associated neighbourhoods frequently experience (see Table 6):
uncomfortable furniture in the home and neighbourhood noise, both of which are related to higher levels of FBG and vice versa; polluted environments in the neighbourhood and uncomfortable furniture in homes that are linked to higher level of FBG and vice versa; unpleasant outside views of the neighbourhood and low level of ventilation in the house connected with higher levels of lipid LDL (i.e. “bad” cholesterol) and vice versa. disgusting odours in the neighbourhood and uncomfortable furnishings linked to patients who have lower level of lipid HDL (i.e. “good” cholesterol) and vice versa; traffic noise and uncomfortable furniture are connected with lower level of lipid HDL and vice versa. SEM links between variables showing the positive regression weights.
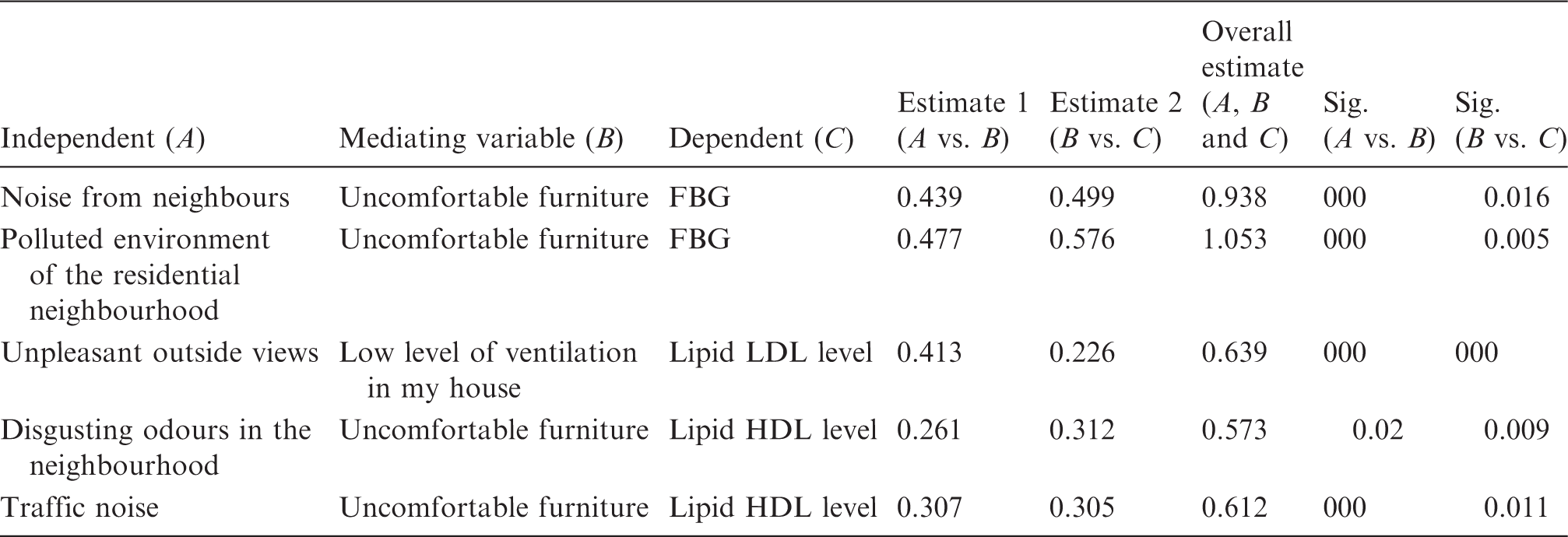
By linking the findings illustrated in Tables 4, 5 and 6 together and relating them to the frequency results, it can be suggested that: unpleasant outside views, which are in turn associated with low level of ventilation within the home (with 36% and 34% scores, respectively), are the most harmful combined indoor and outdoor factors affecting diabetic patients' health. Tables 4 and 5 also tend to suggest that certain home conditions have an adverse effect on the psychological state of the patient, which in turn exacerbates their medical condition.
SEM links between variables showing the negative and positive regression weights (note: the negative values are in bold).
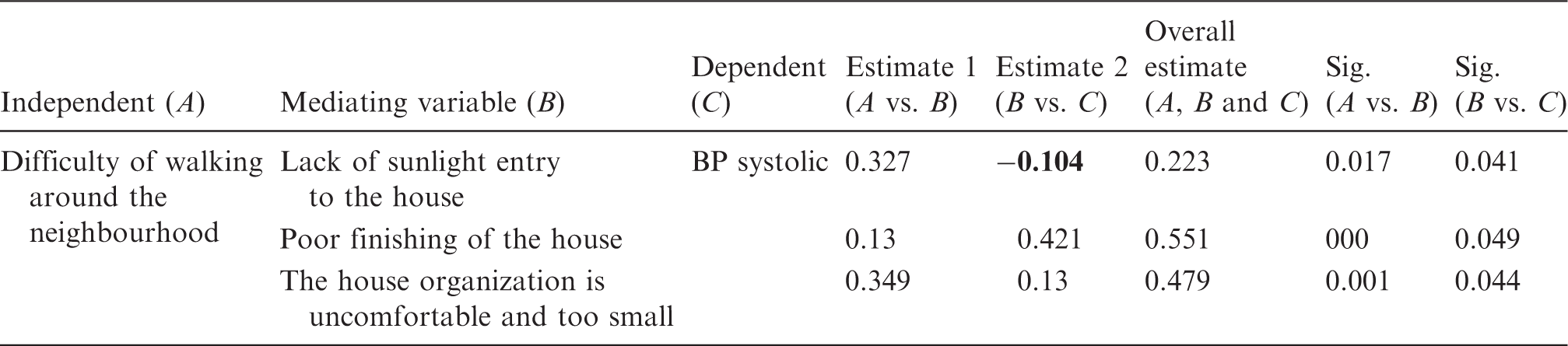
The indoor variables having a twofold, i.e. positive and negative association with the health of the diabetics are: uncomfortable furniture, poor air quality in the house, poor finishing of the home and uncomfortable temperatures in the home. The study also noticed differences between the regression weights and standardized regression values. For example: standardized regression weights for lack of sun entry association with Micro albumin urea are always negative in all SEM diagrams, whereas the regression weights for the same association is sometimes negative and at other times positive. This would indicate the high level of deviation in the correlation between these two variables.
Conclusion
This research has sought to answer a number of serious questions about the complex nature of the relationship between place-based impacts, unhealthy built environments and diabetes in KSA. The answers to these questions are as follows:
(a) Is the built environment healthy?
Unfortunately, the evidence gathered on place-based impacts from the literature review and the research reported in this paper suggest that the KSA's built environment is not healthy. This research suggests KSA’s unhealthy built environment relates to certain living conditions. In the home, this relates to poor air quality, ventilation, temperature and layout. In the neighbourhood, this is linked to the irregular setting of amenities, such as: gardens, parks, recreation facilities and sport centres.
Based on these findings, the study estimates around 38% of diabetics suffer symptoms connected to living conditions connected with their homes and surrounding neighbourhoods.
(b) Are unhealthy built environments related to living conditions?
As the previous statement indicates, this study finds around 38% of diabetics suffer symptoms related to their living conditions and the medical condition they experience is in turn associated with the patients’ homes and surrounding neighbourhoods. In light of this, it is felt evidence exists to suggest the poor air quality, ventilation, temperature and layout of their homes coupled with the irregular setting of amenities, such as: gardens, parks, recreation facilities and sport centres, does give sufficient grounds to classify the indoor and outdoor arrangement of these built environments as unhealthy. It is also felt the grounds for this classification of the built environments as unhealthy are warranted because the symptoms of those diabetic patients’ living in these homes and neighbourhoods exhibit higher than normal levels of FBG and HbA1c.
(c) Are living conditions linked to physiological, social and emotional health?
This study also highlights the linkage between living conditions and the physical, social and emotional health of patients and how this in turn is connected to the social status of the homes and neighbourhoods (i.e. low, middle and upper-income groups) in question. This tends to support the research findings of studies23,46 previously undertaken to explore the relationship between the health of diabetic patients and quality of the built environment.
(d) Is health connected to homes and neighbourhoods?
This research highlights the health of diabetic patients who suffer from poor living conditions, inside their homes and in their surrounding neighbourhoods. In particular, those patients who are unable to access sport centres, parks, recreation facilities and walkways. The findings of this particular study suggests poor indoor and outdoor environments force people to adopt domestic and social lives that not only contribute to the growth of T2DM diabetes, but which also lead to a deterioration in the health of T1DM patients (see also Allanah et al., 30 Eckel et al., 32 Goldberg et al., 46 Michaud et al., 47 Franklin et al. 48 and Jirtle and Skinner 49 ).
This study also finds significant links (level of significance p < 0.05) between the physical, social and emotional health of diabetics, their home and neighbourhood. Here it found an association between the house type, i.e. flat, duplex, villa and the patients' perception of what their home and neighbourhood contribute to domestic and social well-being.
(e) Do homes and surrounding neighbourhoods exacerbate the symptoms?
The study has also found links between these indoor and outside environments and symptoms experienced, whereby such conditions have significant connections with higher levels of LDL, TG and lower HDL evidenced in the findings of the repeat medical tests.
This suggests that while being treated by physicians the health of the diabetic patients have deteriorated. As there is no medical reason for this, the explanation for the escalation of the symptoms they experience must lie in “environmental factors”. As the medical practitioners treating the disease cannot explain the diabetic patients’ aggravated symptoms, the reason for this must lie in the built environment and living conditions found in their homes and neighbourhoods. This study suggests the exacerbation of the symptoms relates:
uncomfortable furniture in the home and neighbourhood noise and to those who have a higher level of FBG and vice versa; polluted environments in the neighbourhood and uncomfortable furniture in homes to those who have higher level of FBG and vice versa; unpleasant outside views and low level of ventilation in the house to patients who have a higher level of lipid LDL and vice versa; disgusting odours in the neighbourhood and uncomfortable furnishings to those patients who have a lower level of lipid HDL and vice versa; traffic noise and uncomfortable furniture to those who have a lower level of lipid HDL and vice versa.
The study also found that patients who live in low-income neighbourhoods complain about the poor air quality in their home and noise from neighbours more than those who live in the middle and upper class neighbourhoods. Exactly how the pathology of the disease found in these environmental settings exacerbates the symptoms captured here and in turn adversely affects the social and emotional health of diabetics is not known, but what is understood is the relationship that exists between them is significant in the sense which it imputes some kind of causal link and connection.
(e) Are homes and neighbourhoods detrimental to health?
The literature review indicated important relations between health, living conditions, homes and neighbourhoods. However, this study found that the relationship they in turn have to their indoor and outside environments is far more complicated than indicated. In this study, it has become evident that males and females perceive the effect of indoor and outside environments in different ways and do not assign them the same level of significance.
This study has tested their joint effect on domestic, social and emotional health using the indoor living conditions as mediating parameters. This has revealed their joint effect on the health of diabetics is in the main positive across homes and neighbourhoods, but in some instances, it is also negative. This finding indicates indoor environments sometimes have negative relations with the health of diabetics. The study has also found this relationship is personal (e.g. gender, level of education), dependent upon type of residence (e.g. type of the house and income-group) and neighbourhood area. This in turn suggests further research should be carried out to assess how these factors interact with indoor and outside environments to aggravate the symptoms of the disease, vis-à-vis have the effect of being detrimental to health.
Footnotes
Authors’ contribution
Each author contributed equally to the production of the manuscript.
Acknowledgement
The authors would like to acknowledge the University of Dammam’s (UoD) support for this study (project Number: 2012107).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research is funded by the University of Dammam (project Number: 2012107), KSA.