
Abstract
The legal regulations and cultural environment for smoking bans in hotels and motels in South Korea differ depending on the type of accommodation. The aim of this study was to assess the thirdhand smoke exposure for hotel and motel guests staying at accommodations who are expected to be relatively vulnerable to thirdhand smoke. Biomarkers for 28 participants were assessed before and after lodging at a hotel or motel for approximately 14 h. Hotel participants had statistically decreased urinary cotinine concentrations after their stay, whereas motel participants experienced increased concentrations. The concentration of nicotine-derived nitrosamine ketone in dust in hotels was lower than that in motels, and the higher dust nicotine-derived nitrosamine ketone concentration in motels had more effect on an increase in urinary cotinine concentration. Both hotels and motels legally allowed smoking in guest rooms. However, the study participants in hotels were less exposed to thirdhand smoke than those in motels.
Keywords
Introduction
Since the first scientific report of secondhand smoke (SHS) as a leading cause of lung cancer in 1981, 1 several studies on the associated hazards of SHS have been conducted.1–5 This type of smoke exposure is also the cause of other cancers and serious diseases ranging from respiratory diseases to cardiovascular diseases, and SHS is estimated to cause 900,000 premature deaths annually worldwide. 6 In addition, the International Agency for Research on Cancer classified SHS as Group 1 carcinogen in 2004.7,8 This type of smoke exposure must be actively mediated because of the health consequences of others, regardless of the non-smoker's willingness to avoid tobacco smoke exposure.
Tobacco smoke exposure including SHS is the single most preventable cause of death. 9 The World Health Organization (WHO) is working to regulate smoking, and the WHO Framework Convention on Tobacco Control (FCTC) is the first international treaty in the field of health. 10 By June 2020, 168 countries signed the FCTC and 181 parties are participating in the treaty. 10 To be a treaty participant, the FCTC calls for the implementation by all parties of the main objectives to meet the general obligations of the treaty (Article 5), reduction of the demand for tobacco (Articles 6–14), reduction of the supply of tobacco (Articles 15, 16) and other provisions (Articles 17–22). Among these, Article 8 relates to SHS and monitors the implementation by parties in key places such as in educational facilities, shopping malls and private workplaces. 11 The implementation rate for Article 8 is the highest among all rates of the treaty articles. 11 South Korea is also strengthening the implementation of Article 8 as a treaty member of the FCTC. Tobacco control policies in the Republic of Korea have been continuously strengthened since the adoption of the National Health Promotion Act in 1995. Since then, smoking and SHS exposure rates have steadily declined. 12
Thirdhand smoke
Due to diminishing threats from these SHS, the evidence of the risk of thirdhand smoke (THS) has been steadily emerging. 13 THS is generally defined as residual tobacco smoke pollutants, such as nicotine and other chemicals that remain as residues on a variety of indoor surfaces and in dust after tobacco smoking. 13 The pollutants in THS can also be found in the air and dust as well as on surfaces. In addition to this initial contribution of THS to pollution, THS is then re-emitted from contaminated surfaces into the air over a period of weeks, thereby accumulating in the dust. 14 This degree of exposure has also been reported by another study that concluded that THS is as harmful as SHS. 15
Accommodation facilities
Accommodation facilities such as those in hotels and motels are one of the common places used by the public where individuals can stay for a relatively long time compared with other places such as restaurants or stores. Therefore, to prevent SHS or THS exposure due to individuals who smoke in these public places, a number of countries regulate smoking in hotel and motel accommodations. In Europe, Spain and Greece have a total smoking ban on the entire indoor environment for hotels, including guest rooms. 16 However, in most European countries, the smoking rules for guest rooms can be decided autonomously by the lodging rather than by law. 17 In the United States, laws vary among States. As of 2015, approximately 700 cities comprehensively prohibited smoking in all hotel buildings, including guest rooms18,19; moreover, in California, approximately 35% of hotels reported in 2017 that smoking was prohibited in their guest rooms. 20 In contrast, a recent study of California hotels revealed for the first time that the presence of contaminants in human body, urinary cotinine, surface nicotine and air 3-ethenylpyridine, are caused by THS exposure in the hotel environment. 21 The exposure depended on whether the hotel has rooms with a smoking ban as well as on the degree of regulatory compliance. Because the characteristics such as culture, law and implementation of non-smoking areas in hotels differ among countries, the research findings in various settings should be supplemented. In South Korea, there are different legal regulations and cultural norms for smoking bans depending on the type of accommodation.
Smoke-free law and cultural differences between hotels and motels in South Korea
Restrictions on smoking in South Korea depend on the type of accommodation. As of 2020, the law for motels allows smoking anywhere in the building, including on stairs and in the lobby. In contrast, the statutes require hotels, condominiums and resorts, as facilities frequently used by families and children, to designate the lobby and staircase areas as non-smoking areas, although smoking is allowed in guest rooms. The reason for not forcing a guest room to be a non-smoking area is that controlling violations is difficult. Not only the legislation for smoking but also the culture of smoking among accommodation facilities is very different. In South Korea, hotels are one of the industrial sectors led by multi-national franchises. In addition to multi-national hotel companies that implement smoke-free policies, such as Westin and Marriot Hotels, as well as Korean hotel franchises, tend to designate entire buildings, including rooms, as non-smoking areas. 19 In contrast, most motels are operated by individuals, not by franchises. Because motels are concentrated in places with many entertainment facilities such as nightclubs and bars, the culture of smoking and drinking in motels is generous.
Studies on the detection of smoking substances in the human body caused by THS in lodging establishments are still scarce. As the accommodation culture varies from country to country, we must be cautious while generalizing previous findings to other countries. Academic studies on human exposure to THS in accommodation establishments in Europe and Asia have not yet been reported. They have only been reported in the United States. Besides, to confirm whether THS is due to staying in a lodging establishment, changes in biomarkers in the human body before and after a stay at the lodging facility should be confirmed. However, there was no study-model for this setting.
Aims
The aim of the present study was to assess the THS exposure for guests staying at hotel and motel facilities in South Korea. For this purpose, cotinine and 4-(methylnitrosamino)-1–(3-pyridyl)-1-butanol (NNAL) concentrations in study participants before and after lodging were measured. These facilities were categorized as either a hotel or motel providing accommodations that were expected to be relatively vulnerable to THS. To determine whether this exposure was caused by the place targeted in this study, the concentrations of nicotine-derived nitrosamine ketone (NNK), which is a tobacco-specific nitrosamine (TSNA) derived from nicotine, were measured. 22
Material and methods
Procedures
To identify the THS according to the type of lodging for participants, accommodations were classified as either: (1) hotels that restrict smoking only in public areas, such as stairs, hallways and the lobby, and otherwise allow smoking in a guestroom; or (2) motels that legally allow smoking in all areas of the building. There was no particular restriction on the participant’s choice of accommodation; however, the research team made adjustments if the participant’s choice of accommodation was the same ‘dong’ or a nearby area. The term dong describes an administrative regional unit in South Korea, and each city is composed of several dongs, which are similar to towns across the United States. Participants were recruited through social networks and snowball sampling. Participants criteria were as follows: must be a lifelong non-smoker or a former smoker who has not smoked in the past year and is not currently living with a smoker. This observation can be explained by the fact that ex-smokers showed a high risk of re-smoking even after quitting smoking. In general, individuals must not smoke for > 6 months to successfully quit smoking. In some cases, individuals who have not smoked in the past one year are classified as non-smokers. 23 Based on these criteria, we finally recruited 28 participants, most of whom were college students and randomly assigned 10 of them to hotels and 18 to motels. Recruited participants received separate training before starting sample collection. Training comprised the following points: (1) lodging was for only one participant per facility, and the research team decided that 14 h would be appropriate for overnight stays and checking out after breakfast. Furthermore, in previous studies that have estimated the level of THS in accommodation facilities, the average stay was 14 h. 21 Therefore, we recommended participants to stay for approximately 14 h; (2) participants were required to check in to a non-smoking room only; (3) no smokers could accompany participants when visiting facilities; (4) at least three days before sample collection, participants could not visit other places where SHS or THS may occur, such as singing room and pubs/bars; (5) participants were prohibited from drinking during the collection period; (6) participants must lightly wipe an amount of dust sufficient to stay on 2 × 2 inch-cotton paper, and they should prioritize the back of the television for dust collection; or, if no dust was present there, they should wipe the back of the air conditioner or the computer in the room and (7) participants must provide a urine sample for collection in a kit provided by the research team about 12 h before and after visiting the accommodation facility. The collected urine samples were stored in a deep freezer at –70°C.
Measurements of smoking indices: Urinary cotinine, urinary NNAL, dust NNK and smell
This study used biochemical urinary cotinine and NNAL concentrations to evaluate smoking exposure in addition to environmental dust NNK, which is a chemical produced by nicotine reacting with air and is representative of TSNA.24,25 To measure urinary cotinine concentrations, the urine sample was mixed with internal standards including cotinine-methyl-d3 (Co-d3) and extracted with methylene chloride. Extracts were evaporated and redissolved in 100 µL of the mobile phase. Cotinine concentration was measured by liquid chromatography–tandem mass spectrometry system on an API 4000 system using the TurboIonSpray interface and multiple reaction monitoring (Applied Biosystems/MDS Sciex). The NNAL sample was mixed with a phosphate buffer of β-glucuronidase enzyme and added to an aqueous solution of d3-NNAL internal standard solution. The mixture was incubated at 37°C for 24–27 h. The method involves liquid–liquid extraction followed by conversion to hexanoate ester derivative, which facilitates separation from interfering urinary constituents by extraction and chromatography and enhances detection with electrospray ionization mass spectrometry. NNK is a representative biochemical substance that is present in side-stream smoke. 26 The measurement of the NNK concentration relative to the level of SHS and THS can be obtained with one of two methods. The first method involves vacuum-suctioning dust,22,27 and the other method consists of wiping with cotton.28–30 We used the wiping method. For measurement of dust NNK, filter paper that was soaked in 50% methanol and left to dry was used to collect the dust samples. After collection, 100 mM ammonium acetate was added to extract samples from the filter paper. Samples were analysed using Agilent 1260 rapid resolution liquid chromatograph (Agilent Technologies) coupled with a triple quadrupole mass spectrometer equipped with a TurboIonSpray TM source (AB Sciex). The limit of detection (LOD) and limit of quantitation (LOQ) for the urinary cotinine concentration were 0.27399 ng/mL and 0.3057 ng/mL, respectively. In addition, the LOD and LOQ for the urinary NNAL concentration were 0.1066 pg/mL and 0.5469 pg/mL, respectively. Finally, the LOD and LOQ for the NNK concentration were 5 pg/mg (S/N 3.2) and 25 pg/mg (S/N 7.2), respectively. Precision (both within-day and between-day) of the method was found to be acceptable (coefficient of variance, CV < 10%).
Urine is the most sensitive substance for evaluating effects of SHS and THS. 31 Cotinine and NNAL concentrations are widely used to evaluate smoking and passive smoking.31–33 However, our study assessed the effect of THS and was conducted by excluding SHS. We measured cotinine/creatinine ratio (C/Cr) and NNAL/creatinine ratio (NNAL/Cr) as a means to correct creatinine concentrations in non-smokers, which have good correlation with smoking substances.34,35
Smoke smell
A five-point Likert scale with values ranging from 1 (‘not at all smelly’) to 5 (‘extremely smelly’) was used to assess whether tobacco smoke odour was detected when entering the property buildings and rooms. To determine whether the air was ventilated, the room was examined for windows; if the room had a window, but it did not open, window air ventilation was considered to be absent.
Statistical analysis
A descriptive analysis was performed for the facility and participant characteristics. Moreover, urinary C/Cr, NNAL/Cr and dust NNK values were confirmed by use of the geometric mean and median. Urinary C/Cr and NNAL/Cr ratios were paired for a t test to confirm that the change in concentration before and after the visit was statistically significant. The correlations between changes in C/Cr and NNAL/Cr and NNK were analysed. In addition, bootstrapping was performed as a t test to determine if correlations between NNK and urinary C/Cr were higher in either of the lodging groups (hotel vs. motel). Statistical analyses were carried out converting natural logarithms.
Results
Characteristics of the accommodation and length of stay
The smoking indices between the hotel group (10 participants) and motel group (18 participants) were analysed (Table 1). All hotels offered participants a non-smoking room; no motels offered participants a non-smoking room. The hotel and motel visitors stayed on average 14.4–14.8 h, and residence times between two groups did not differ (Table 1). All 10 hotel rooms had windows that could be opened. For motels, one had a room without an openable window and the other 17 rooms had openable windows. Using a five-point Likert scale with values ranging from 1 (‘not at all smelly’) to 5 (‘extremely smelly’) to evaluate the building/lobby, all hotel participants responded, ‘not at all smelly’ when entering the building in contrast to the responses from motel participants: 13 (72.2%), 4 (22.2%) and 1 (5.6%) responded ‘not at all smelly’, ‘mildly smelly’ and ‘moderately smelly’, respectively. Using the same scale to evaluate the room upon entering, all participants in the hotel group responded, ‘not at all smelly’, whereas participants in the motel group responded, ‘not at all smelly’ (13, 72.2%), ‘mildly smelly’ (2, 11.1%) and ‘moderately smelly’ (3, 16.7%).
Accommodation length of stay and windows and the characteristics of smell.
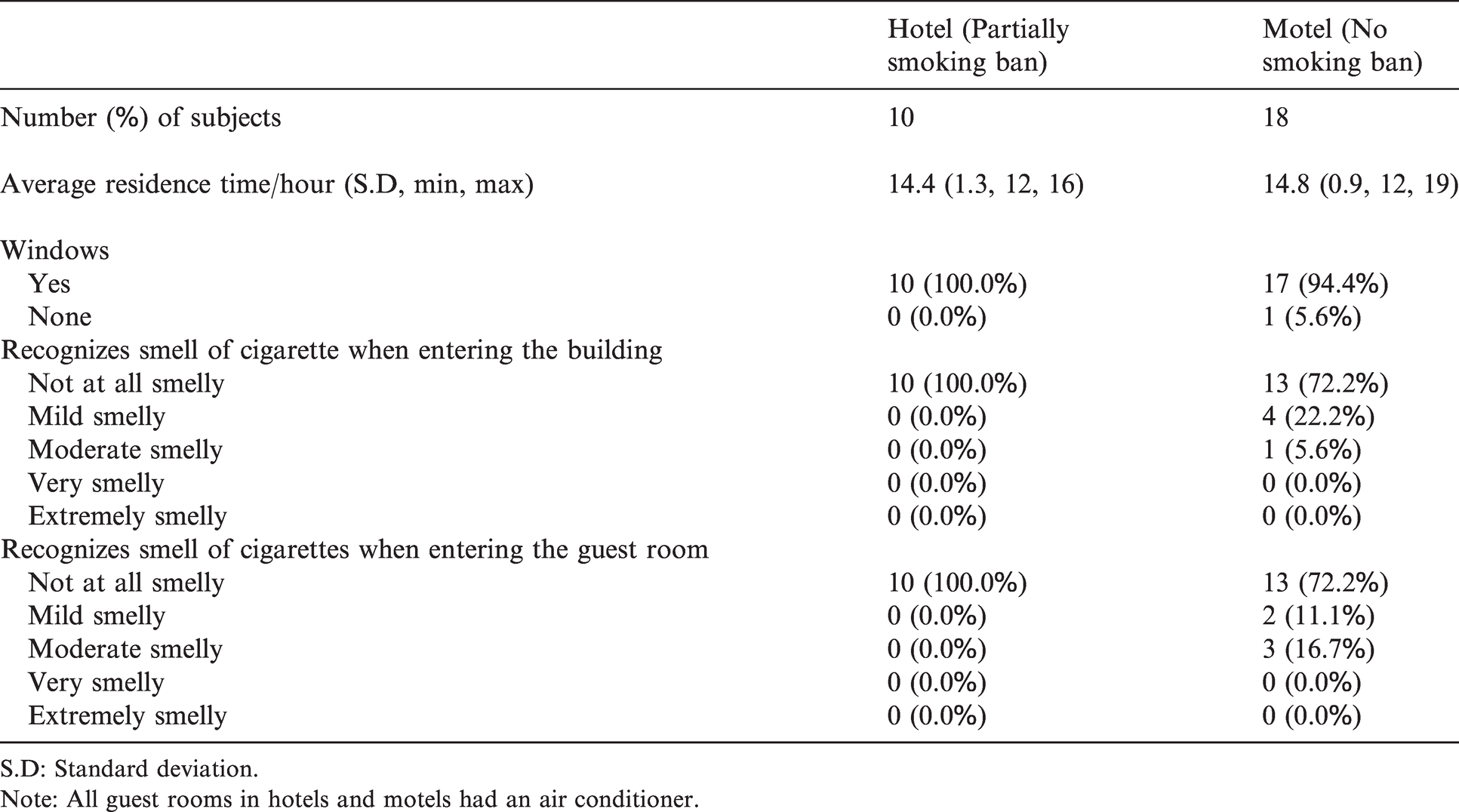
S.D: Standard deviation.
Note: All guest rooms in hotels and motels had an air conditioner.
Concentrations of urinary C/Cr, urinary NNAL/Cr and dust NNK
At baseline, both the urinary C/Cr and NNAL/Cr concentrations showed insignificant differences between hotel and motel groups (Table 2). The changes in C/Cr concentrations and dust NNK samples before and after participants’ visits were analysed after classifying which samples were from hotel versus motel participants. The C/Cr geometric means for hotel participants were 22.59 (median, 14.97 ng/mg) before the visit and 9.17 (median, 10.08 ng/mg) after the visit. For motel participants, the geometric means increased from 9.84 (median, 11.00 ng/mg) before the visit to 22.01 (median 16.03 ng/mg) after the visit. For urinary NNAL/Cr for hotel participants, geometric means were 13.73 (median, 8.85 ng/mg) before the visit and 14.04 (median, 13.69 ng/mg) after the visit. For urinary NNAL/Cr for motel participants, geometric means were 9.04 (median, 9.43 ng/mg) to 10.05 (median, 8.45 ng/mg). The dust NNK concentration’s geometric means for hotels were lower at 69.92 (median, 71.97 pg/mg) than for motels at 244.43 (median, 261.87 pg/mg).
Concentrations of urinary cotinine, urinary NNAL and dust NNK.
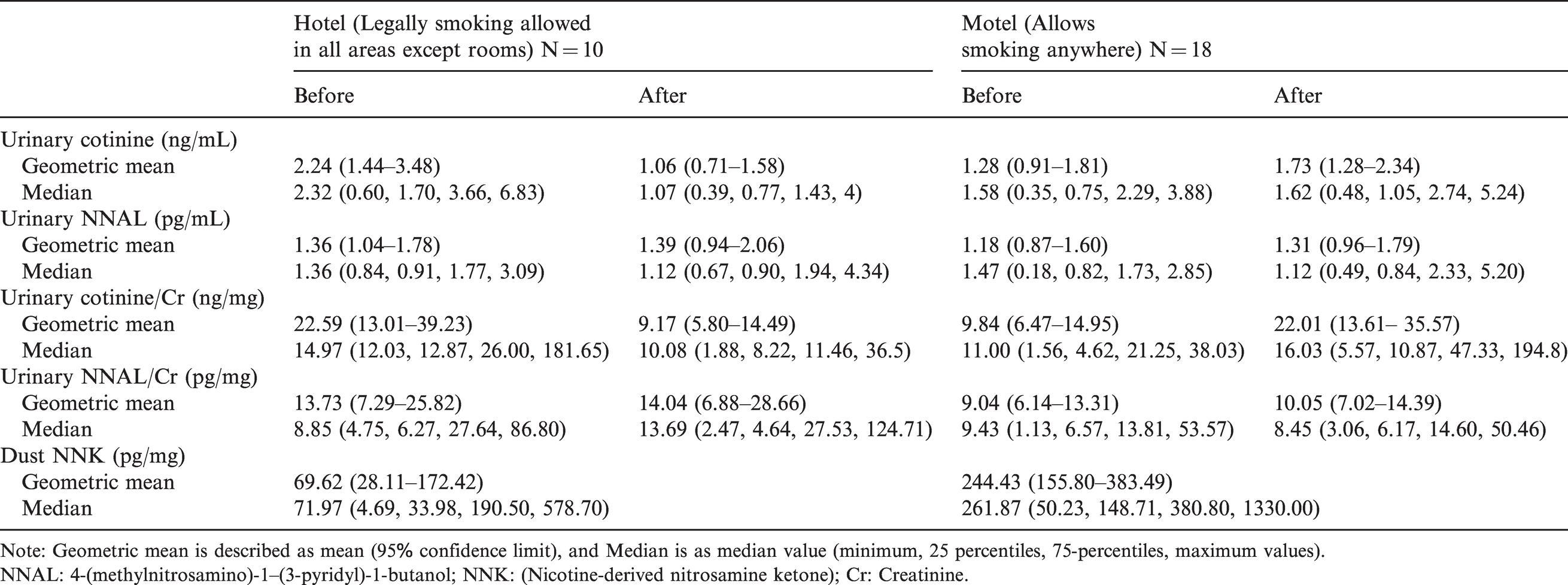
Note: Geometric mean is described as mean (95% confidence limit), and Median is as median value (minimum, 25 percentiles, 75-percentiles, maximum values).
NNAL: 4-(methylnitrosamino)-1–(3-pyridyl)-1-butanol; NNK: (Nicotine-derived nitrosamine ketone); Cr: Creatinine.
Comparison of urinary C/Cr and NNAL/Cr concentrations
A paired t test was conducted to confirm whether urinary C/Cr and NNAL/Cr ratios were statistically significantly changed before and after visiting the accommodation site. For hotel participants, urinary cotinine concentrations showed a statistically significant decrease (p = 0.002), and NNAL/Cr showed no statistically significant change (p = 0.92). For motel participants, urinary C/Cr concentrations showed a statistically significant increase (p = 0.021), and NNAL/Cr showed no statistically significant change (p = 0.59) (Figure 1).
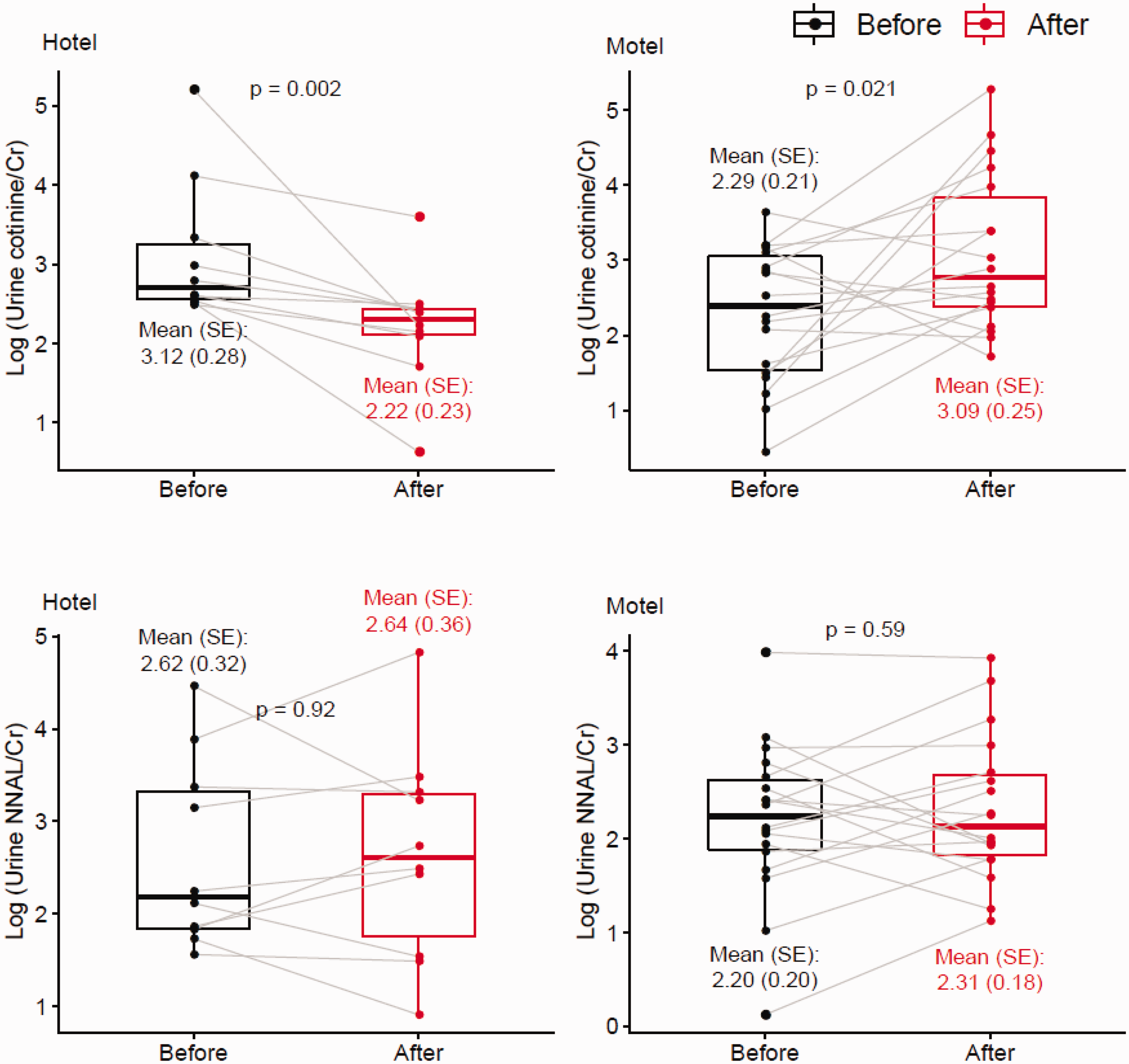
Changes in urinary cotinine and NNAL concentrations before and after staying at a hotel or motel. The p values were measured by the t test. Units of urinary cotinine/Cr (C/Cr) and urinary NNAL/Cr values are ng/mg and pg/mg, respectively.
Correlation between changes in urinary C/Cr and NNAL/Cr concentrations and dust NNK concentrations before and after visit
Figure 2(A) illustrates the correlation among C/Cr change, NNAL/Cr change and dust NNK concentration. NNK concentration did not correlate with NNAL/Cr change but showed a statistically significant correlation with C/Cr change (r = 0.37, p < 0.05). Urinary NNAL/Cr ratio was not correlated with dust NNK concentrations (data not shown). Furthermore, correlations of dust NNK and urinary C/Cr concentrations were assessed by accommodation type; however, the small sample size (10 hotels and 18 motels) yielded insignificant results. Therefore, the bootstrapping method was used with the resampling number of 1000, yielding correlations between dust NNK and urinary C/Cr concentrations in hotel participants that were significantly lower compared with those in motel participants (Figure 2(B)).
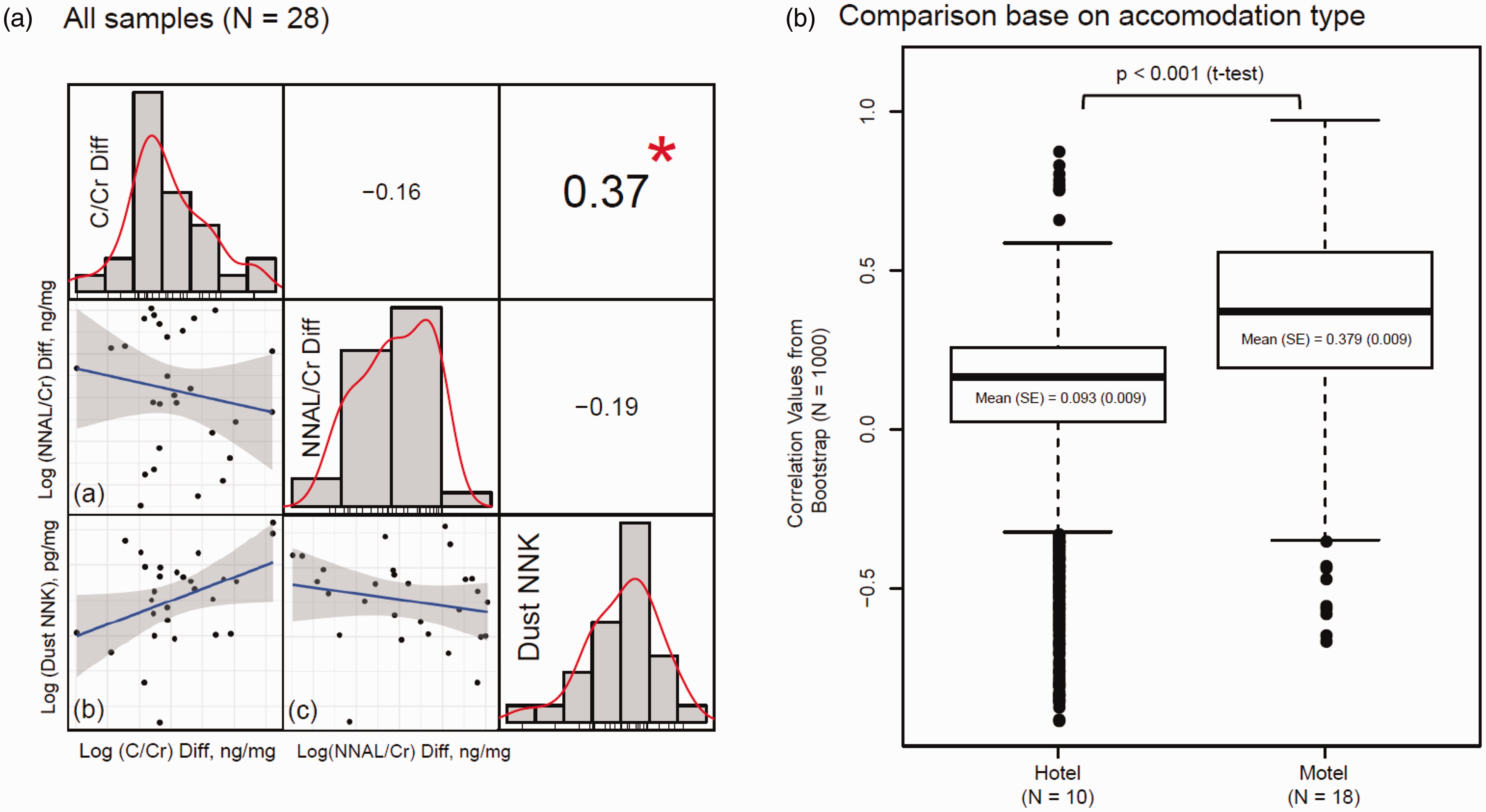
Correlations among smoking indices (urinary cotinine/Cr: C/Cr, NNAL/Cr and dust NNK). (A) A matrix of diagonal components that show distributions of log-transformed urinary C/Cr, NNAL/Cr and dust NNK; upper triangular components that show Pearson’s correlation values and lower triangular components that show correlational plots. * denotes p < 0.05, and 0.37 refers to the coefficient between the C/Cr diff and dust NNK (Alpha = 0.05). (a) is a graph showing the correlation between the NNAL/Cr diff and dust NNK. (b) is a graph showing the correlation between the C/Cr diff and dust NNK. (c) is a graph showing the correlation between the NNAL/Cr diff and C/Cr diff. (B) Two lists (hotel and motel) of 1000 correlational values between dust NNK and urinary C/Cr were compared based on accommodation type (hotel and motel) by t test. The list of 1000 correlational values was curated from bootstrapping with number of resampling (1000).
Discussion
Research has already documented that institutional smoking bans have reduced SHS exposure. 36 However, few studies have compared THS exposure-based differences in the types and cultural norms of facilities, such as hotel and motel accommodations. This study confirmed that, although hotels and motels have similar legal restrictions on smoking, the experience of visitors and their exposure in hotels and motels shows different characteristics, and that motel visitors are more likely to experience THS. The first scientific evidence supporting this point is the change in the smoke exposure indices of urinary cotinine and NNAL concentrations before and after lodging at these facilities. For hotels participants, urinary cotinine concentrations decreased after the visit, but increased for motel participants after the visit. This finding indicates that THS, which increases cotinine concentrations, occurs in motels. In contrast, the reason for the decrease in hotels can be estimated through the research methodology in this study. Through a pre-training, participants avoided smokers from three days before the visit to end of the sample collection and agreed to not visit with the potential presence of SHS and THS. The average half-life of cotinine is about 18 h; therefore, the assessment of SHS in the past one to three days is easy. 25 As a result, hotel visitors were exposed to less smoking than usual on their typical day, which resulted in urinary cotinine concentrations decreasing to lower levels than those before lodging. This point can also be confirmed through the NNAL concentrations, which have a half-life of 10 days to 3 weeks, making it difficult to assess exposure to three days before and after the visit.25,32,37,38 In both groups, the changes in NNAL concentrations were not statistically significant, indicating that changes in urinary cotinine concentration were due to exposure in the past one to three days. The second evidence that indicates THS in this setting is the correlation of urinary cotinine concentrations with dust NNK concentrations. Further studies are needed to evaluate and confirm whether changes in urinary cotinine concentrations are due to exposure in the establishment. Once this is confirmed, chemical markers that can affect the body cotinine should be identified. In other words, there was no change in the NNAL concentration detected in the motels in this study, but the increased cotinine concentration indicates that motels were exposed to higher concentrations of smoking-related substances within the previous one to three days. In addition, only the change in cotinine was positively correlated with the NNK concentration, indicating that NNK did influence the increase in cotinine. In conclusion, our study shows that THS did not occur in hotels but occurred in motels. Principally, in our study, although C/Cr and NNAL/Cr acted as variables, we have used the terms urinary cotinine and NNAL concentrations in the Discussion section for the convenience and readability of readers.
The concentration of dust NNK could reflect urinary cotinine concentrations but not urinary NNAL concentrations (Figure 2(A)). This correlation between dust NNK and urinary cotinine concentrations was stronger when dust NNK concentration was high (Figure 2(B)). However, few studies have analysed the correlation between dust NNK and urinary cotinine concentrations. The dust NNK is one of the indices for exposure to tobacco constituents. 22 Whitehead et al. 22 reported that dust NNK concentration was 6.3 pg/mg, which was 6.9-fold significantly higher in homes with smokers than in homes without smokers. In the data in this study, the median dust NNK concentrations were 71.97 pg/mg for hotels and 261.87 pg/mg for motels. These differences in concentration between previous studies and the current one were due to the sample collection method. This is a higher value than that reported previously at this level.27,39–41 The results should therefore be cautiously interpreted considering that the floor dust was collected using a vacuum in the previous study; but in the present study, the samples were collected by dusting the back side of a home appliance or a corner where the dust had accumulated using a cotton paper. In addition, in the previous study, wherein the dust was collected in the same way as in our study, NNK concentration was also high 28 probably because the previous study collected relatively old dust to find dust samples. In other words, more NNK may have accumulated in the old dust. To examine this aspect, more studies are needed to assess the collected NNK by different methods. Furthermore, differences may also have been observed because individuals may smoke more in hotels and motels more than in their homes. In this study, concentrations of dusk NNK in motels were about 3.6-fold higher than those found in hotels. This difference suggests that smoking was more frequently conducted in motels than in hotels.
Previous studies of THS in hotels have shown that smoking substances in air and dust in hotels increased TSNA in the human body and have confirmed that the separation of smoking areas in buildings did not completely protect them from these substances.20,21 This exposure can depend on the size of the hotel. 20 In South Korea, hotels are generally much larger than motels. Therefore, our research is an extension of results of related previous research. In addition, even if smoking is regulated, many guests will be exposed to smoking by poor implementation and enforcement of the regulations. The current study is one of the earliest studies to reveal THS exposure according to the level and culture of smoking regulations in lodging, which are factors that were not addressed in previous studies.
In South Korea, there are no policies on smoking exposure and controlling hazards associated with smoking in motels, although the government has plans to strengthen their regulation of smoke-free area. Therefore, the authors believe that this study will be valuable to help the government to create, implement and enforce smoking policies for public spaces and to create awareness for high-risk groups. In the hotel and motel guest rooms, smoking is not legally restricted currently in South Korea. Nevertheless, this study has confirmed that THS was a more serious concern in the motel environment. In South Korea, this difference may be a result of different characteristics of smoking-related cultural norms for hotels and motels. Although motels guests are legally allowed to smoke in the lobby or stairways, one does not expect people to smoke in public areas in the building. In this study, results showed that only 5.6% of the motel participants reported detecting a ‘moderately smelly’ odour when entering the motel building. In other words, a significant increase in C/Cr values only in motels may have been influenced by the influx of smoking substances from the corridors and lobby 21 and is most likely due to the fact that smoking is performed more often in motel guest rooms.
Although smoking was allowed in the guest room of the hotels, urinary cotinine concentrations were decreased for the hotel participants in this study. This finding indicates that smoking exposure in hotels is relatively low or absent compared with that in motels. Although there are no related studies or statistics for this point cannot be verified, in South Korea, even if guests smoke in the guest rooms, the hotel rarely penalizes them. Although smoking in guest rooms is not legally prohibited, smoking in the hotel guest rooms is likely to be significantly less common than in motel guest rooms because of the hotel's own smoking bans and public awareness. Therefore, encouraging establishments to voluntarily implement smoke-free policies, along with legal regulations that make the entire room non-smoking, is essential to reduce THS in accommodations. However, there are various difficulties in enacting and enforcing smoking regulation laws. Therefore, a cultural approach to prevent smoking in an accommodation can be an alternative. Autonomously choosing a smoke-free policy should be encouraged for property owners, as it is an important means to protect the health of customers and can also be beneficial for the business.42,43 In the same way, motel owners must make efforts to designate room(s) as non-smoking, which is the minimum intervention that can protect non-smokers from SHS; nevertheless, it may not protect guests from other guests who choose to smoke regardless of prohibitions. Also, even for visitors to lodging establishments, the rooms are not a completely smoke-free place. For guests, a campaign is needed to improve the perception that rooms are public places used by many people, rather than places where smoking is freely permitted.
In this study, few participants detected the smell of cigarettes in hotels and motels. For this reason, lodging guests may not feel the need for an establishment to provide an entirely non-smoking area. Compared with THS, although SHS exposure may occur in higher concentrations because the individual is directly exposed to cigarette smoke, this exposure is often for a relatively short time; at certain time periods when smoking occurs, and this exposure in most public places, such as restaurants and streets, can be avoided. In contrast, lodging is relatively one of the long-term places of hospitality because a visitor stays there for at least a few hours, and thus this site is characterized by a longer exposure to smoking substances. Therefore, THS may have adverse health effects similar to those of SHS. 44 Moreover, THS is invisible and persists for a long time. In other words, THS is a ‘quiet killer’ for hotel and motel guests. Continuing to send these messages to the public could lead to legal or voluntary smoking restrictions at the hotel and motel property. In addition, for places where smoking is frequent, cleaning to remove smoking substances can help reduce smoking exposure. However, cleaning that does not completely remove smoking substances will not completely prevent the THS. 45
This study has several limitations. First, this study is not a probability extraction. The research team restricted visits to accommodations within the same area; nevertheless, samples were extracted conveniently, they had low representativeness. Second, because of the small sample size, the research team was unable to control other variables that could affect smoking exposure. When smoking occurs, THS cannot easily be prevented through ventilation, 46 but ventilation can influence the level of exposure to THS. 47 Windows or ventilation may affect the level of exposure to harmful substances related to smoking. Despite the fact that there was only one room without a window, all study participants show decreased levels of cotinine concentrations in hotels, whereas cotinine concentrations were increased in many of participants in motels. Therefore, the smoking culture, based on the type of accommodation, such as hotel or motel, has a greater influence on the occurrence of THS, rather than the presence or absence of a window. Third, there was a difference in the cotinine and NNAL concentrations before visiting the hotel and motel. This difference can be attributed to the fact that the concentration of one hotel participant was high. However, this figure was sufficiently acceptable for non-smokers, and in this study, the change value was much more important than the initial value. Therefore, we believed that this aspect did not affect our findings. In terms of the research methodology, it is practically difficult to exclude them before analysis; therefore, it is better to secure a greater number of samples to resolve this issue. Fourth, this research did not confirm whether smoking actually occurred more commonly in motels than in hotels. Finally, the recent market for peer-to-peer accommodation facilities such as Airbnb has been expanding, and smoking-related problems in these facilities are a new challenge to understand. 48 Therefore, further studies on these facilities will be necessary.
Conclusions and future research
Our findings confirm that the cotinine concentrations increase in participants after staying in accommodations in cultures that allow smoking, even though they were not exposed to SHS, indicating that this is due to the THS. After an average of 14 h of stay, the increase in cotinine concentrations positively correlates with indoor dust NNK concentration, which is an environmental indicator, and not that of NNAL. Both hotels and motels legally allow smoking in guest rooms, but THS is more common in motel guest rooms. Despite a lack of smoking bans at hotels and motels, cultural norms and the property’s own smoke-free rules may have the effect of reducing THS exposure.
Footnotes
Acknowledgements
Authors’ contribution
Myung-Bae Park and Jee Eun Oh designed the study; conducted the literature review and statistical analysis; and wrote the article. Tae Sic Lee and Do Hoon Lee reviewed related articles and references. All authors reviewed and approved the final version of the article.
Availability of data and materials
The processed data is available from the author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Ethics approval was obtained from IRB of Pai Chai University (2–1040766-AB-N-01–2017-02). All participants provided written informed consent.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (NRF-2017R1C1B5017638, NRF-2020R1C1C1007913).