
Abstract
The air temperature was critical to human health, especially for the mucosal immunity of the respiratory system. Amongst a few biomarkers, immunoglobulin was an effective material to evaluate respiratory health. In order to explore the effects of the natural air temperature on serum immunoglobulin concentrations of people, an epidemiological investigation was conducted between Jan 2018 and Dec 2019. In addition, an experiment was conducted to find the relationship between indoor air temperature and salivary immunoglobulin E (IgE) concentration, under the built environment within the comfort zone of people. Results of the epidemiological investigation showed that the serum IgE concentration was the most sensitive to temperature and was positively correlated with outdoor environmental temperature (p < 0.001, Spearman = 0.509). In addition, the experimental results showed that the salivary IgE concentration was also positively correlated with indoor temperature (p = 0.009, Spearman = 0.495), and it rose significantly with the increase of thermal comfort votes (p = 0.022, Spearman = 0.508). In a comfortable temperature range, keeping a higher air temperature can increase the concentration of IgE antibodies, which is one of the ways to improve the mucosal immunity of the respiratory system.
Keywords
Introduction
With the outbreak of COVID-19, human health in the living environment has attracted more and more attention. Indoor and outdoor air temperature is one of the factors affecting human health.1,2 Changes in environmental temperature have wide-ranging effects on human health, including cardiovascular, respiratory and mortality from infectious diseases. 3 Amongst them, respiratory diseases are one of the important causes for death and disability. 4 According to the statistics of the ‘World Health Organization’ and ‘Global health partners’ in 2018, 5 up to 650,000 people died each year from respiratory diseases caused by influenza. Influenza and pneumonia (COVID-19, MERS and SARS) are acute infections,6–9 which are self-limiting diseases of respiratory diseases. 10 The outbreak is seasonal, 11 and winter is a high-incidence period.12–15 Cold snap increased the hospital admission of respiratory diseases by 32%. 16 When the concentration or activity of the existing or new viruses in the body is stronger than the body’s immunity, the body will be in a state of infection. Therefore, the body’s immunity is the root of disease prevention. Improving the body’s inherent immunity is crucial to the prevention of such diseases.
As the basics of humoral immunity, antibodies can combine antigens such as viruses and bacteria to reduce the proliferation of pathogens in the body and prevent them from killing human cells. 17 Immunoglobulin is the chemical basis of antibodies, which exists in serum and exocrine fluid. It can be divided into immunoglobulin A (IgA), immunoglobulin M (IgM), immunoglobulin G (IgG), immunoglobulin E (IgE) and immunoglobulin D (IgD). Mucosal surfaces are used by most viruses as an entry point for their initial infection. The upper respiratory tract is exposed to the environment and in close contact with the outside world. Viral microorganisms are easy to invade the respiratory mucosa. The antigen stimulates the local immune system without the participation of the central immune system after entering the respiratory tract. The immune response can proceed on its own, secreting IgA and IgE. 18 The proportion of IgE secreted by the respiratory tract is much higher than that in blood, and it is also one of the largest groups of IgE plasma cells in the human body. 19 A large part of circulating IgE is thought to have been derived from the mucosa and then overflows through the lymphatic system. 20 Respiratory mucosal IgE is the main antibody against parasite infections such as worms, mites and schistosomes, which is the first line of defence in immunity.21–23 Although a high concentration of IgE can lead to an allergic reaction, this reaction only occurs at the most extreme and unsuitable end of the immune spectrum. At the other part of the spectrum, increasing IgE concentration can enhance resistance to pathogens. 21
The physiological control system can be changed by environmental stressors that regulate immune events. Hosts’ resistance to disease can be suppressed or increased by these changes. As one of the important components of environmental stress, temperature could affect antibody-mediated humoral immunity. 24 There is a continuing heat exchange between the environment and the respiratory tract, which affects the function of respiratory mucosal epithelial cells, and the germinal centre of the cells is one of the places where immunoglobulin is produced. 25 Therefore, immunoglobulin can be used as a biomarker to evaluate the health of environmental temperature, thus explaining the impact of environmental temperature on the human body. However, most of the existing literature was based on the medical perspective to study the pathological changes of immunoglobulin,26–28 ignoring the research on healthy subjects. In such studies, IgE concentrations usually exceeded the normal range and the subjects were in a pathological state. However, IgE’s protective function in host defence and the body’s immunity must not be ignored. 29 Therefore, our research aimed at healthy people, and the IgE concentrations of subjects were within the normal range.
Natural and built environments are not independent. The building’s indoor air temperature and human behaviour adjustment would vary with the outdoor climate. In this study, influences of the air temperature on immunoglobulin concentration were explored by combining outdoor and indoor air temperatures and using methods in medical engineering. The research contents included the following: 1. The effects of natural temperature on the concentration of four types of serum immunoglobulins were analysed through epidemiological investigation. The purpose was to explore the relationship between the natural environment and serum immunoglobulin, and screen biomarkers suitable for the indoor environment experiment. The results of the epidemiological investigation should provide support for the indoor environment experiment. 2. The lab research was designed under a controlled indoor environment. The influence of indoor environment temperature variations on IgE was analysed by observing the salivary IgE concentration at different temperatures. 3. In the experiment, the measurement of salivary IgE was combined with the thermal comfort survey of subjects to explore the relationship between subjective thermal perception and IgE.
In this study, the effect of the thermal environment on human immunoglobulin concentration was evaluated, and the benefits of both the natural or built thermal environment to human health were explored. This study could provide an important reference for the design of healthier indoor thermal environments for buildings thus improving the upper respiratory mucosal immune function of residents, and to provide a new idea for the prevention of respiratory diseases.
Materials and methods
Epidemiological investigation
The epidemiological investigation was based on the physical examination report of healthy people in a large urban general hospital in northern China. The population of the city is 7–8 million, the number of outpatient and emergency patients is 1.6–1.9 million/year and the physical examination volume of the physical examination centre is 40,000–60,000 person times/year. A total of 1,500 healthy people who received physical examinations between Jan 2018 and Dec 2019 were selected. People with chronic diseases, asthma, allergy and immune diseases were excluded. We sent written informed consent requests to each examinee and obtained their consent before obtaining samples. A total of 1,181 valid samples were obtained. The age of the subjects was 48.7 ± 10.1 (mean ± standard deviation) and ranged from 16 to 79. Serum IgE, IgG, IgA and IgM concentrations were counted in their physical examination reports. Atmospheric temperature data on the day of the physical examination were obtained from the China Meteorological Data Network of the National Meteorological Science Data Centre.
Indoor environment experiment
The concentration of serum immunoglobulin could vary greatly. In addition to air temperature, it may also be affected by environmental chemicals, 30 dust mites, 31 pollen 32 and other factors. Otherwise, demographics, lifestyle 33 and metabolism may also be influencing factors. Therefore, in order to control the environmental and subject variables, we further designed an experiment under controlled environment in a climate chamber. Due to the popularity of room temperature adjustment equipment, the indoor temperature of the building is usually controlled in or near the thermal comfort zone. Therefore, the air temperature of the chamber was set in terms of the near comfort zone to simulate the real indoor environment.
Subject
Healthy subjects whose body mass index (BMI) was within the normal range (18.5–23.9), never smoke, never drink heavily and had no allergic symptoms such as gingivitis and stomatitis, were recruited in this study. The human immune system reaches maturity in adolescence (10–19 years old). 34 So subjects over 20 years old were recruited to avoid the error caused by age. Informed consent requests were distributed to subjects in advance. The experimental process complied with the ethical standards of the Qingdao University of Technology with an approval number of QUT. L.01. In order to reduce the impact of the subjects' daily living habits on the experimental results, the subjects were reasonably restrained 2 days before and during the experiment which mainly include the following: (1) to avoid drastic changes in eating habits, and the nutrient intake was roughly balanced every day; (2) to try to keep adequate sleep; (3) to avoid large fluctuations in mood and (4) to avoid taking medication that could affect the immune function or supplements, such as vitamins.
In the experiment, a total of 10 subjects were recruited, including 6 males and 4 females. The age of the subjects was 23.5 ± 0.9 (mean ± standard deviation) and ranged from 22 to 25. The BMI of the subjects ranged from 18.9 to 22.8. Subjects were asked to wear the same clothing with a thermal resistance of about 0.57 clo, as recommended by ASHRAE 55. 35
Experimental temperature and site
We chose three temperature conditions: cool (18°C), neutral (24°C) and warm (30°C). 18°C is the recommended minimum indoor temperature in winter. 36 24°C is close to the human thermal neutral temperature. 37 At 30°C, the human body begins to store heat, 38 and people feel warm at this temperature.
The experiment was conducted in September 2021. This experiment was carried out in a laboratory (7 × 3.1 × 3 m) with constant temperature and humidity air conditioning. The adjustable temperature range was −5°C to 18°C. The laboratory included two rooms: the climate room (5 × 3.1 × 3 m) and the waiting room (Figure 1). Laboratory diagram.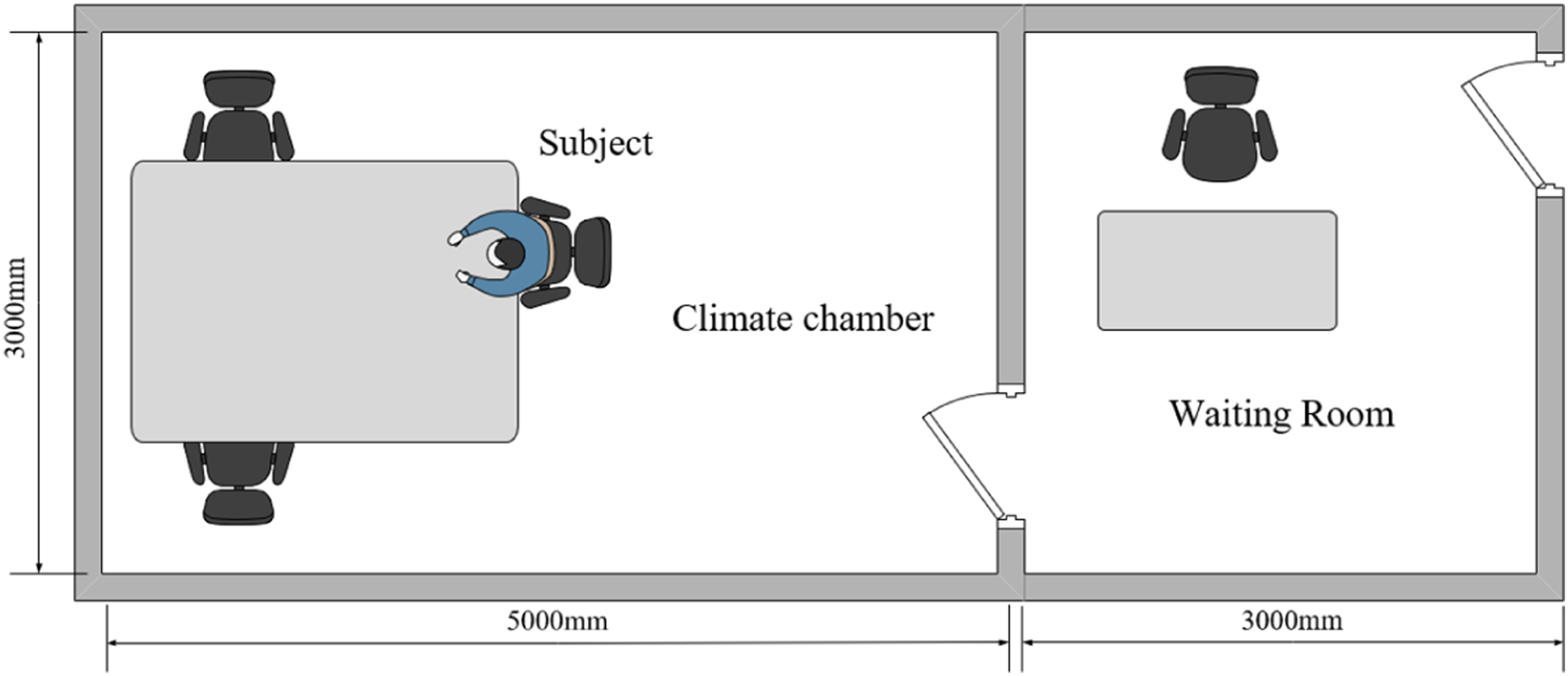
Air temperature
Air temperature in the experiment.

Thermal comfort questionnaire
Thermal comfort refers to the evaluation of people’s satisfaction with the surrounding thermal environment. 35 Studies have found that thermal comfort contributes the most to all the factors affecting indoor environmental quality. 39 We used a questionnaire survey to acquire the thermal comfort of subjects at three temperatures. Since the temperatures were set within the comfortable range, there were no intolerable temperatures during the whole experiment. Therefore, the ASHRAE thermal comfort level 40 was simplified and divided into three levels: comfortable, slightly uncomfortable and uncomfortable.
Salivary IgE collection and detection method
Multiple blood sampling in a short time can have an adverse impact on the subjects and bring confounding factors to the results. Considering that the human saliva also contains IgE, and the saliva collection is non-invasive, simple and easy to operate, saliva collection method was applied in vivo experiments of non-medical research by detecting salivary IgE concentration. 41 Therefore, the salivary IgE concentration was used as an indicator in the experiment.
One hour before saliva collection, we asked the subjects to rinse with pure water and prohibited drinking water or eating. When collecting saliva, the subjects were asked to use the spitting method to ensure that the unstimulated saliva was collected. After collection, saliva was immediately transferred to sterile test tubes containing phosphate buffer solution (PBS) and phenylmethanesulphonyl fluoride (PMSF) to prevent immunoglobulin degradation. The volume ratio of PMSF to PBS was 1:1000, and the volume of the mixed solution in each test tube was 1 mL. The test tube was then stored in an ultra-low temperature refrigerator at −80°C.
The salivary IgE concentration was detected by the enzyme-linked immunosorbent assay (ELISA) (Figure 2). The experimental process and data elimination method were strictly followed according to the product specification. The detection steps were as follows (Figure 3). Salivary IgE detection microplate. Salivary IgE concentration detection process.
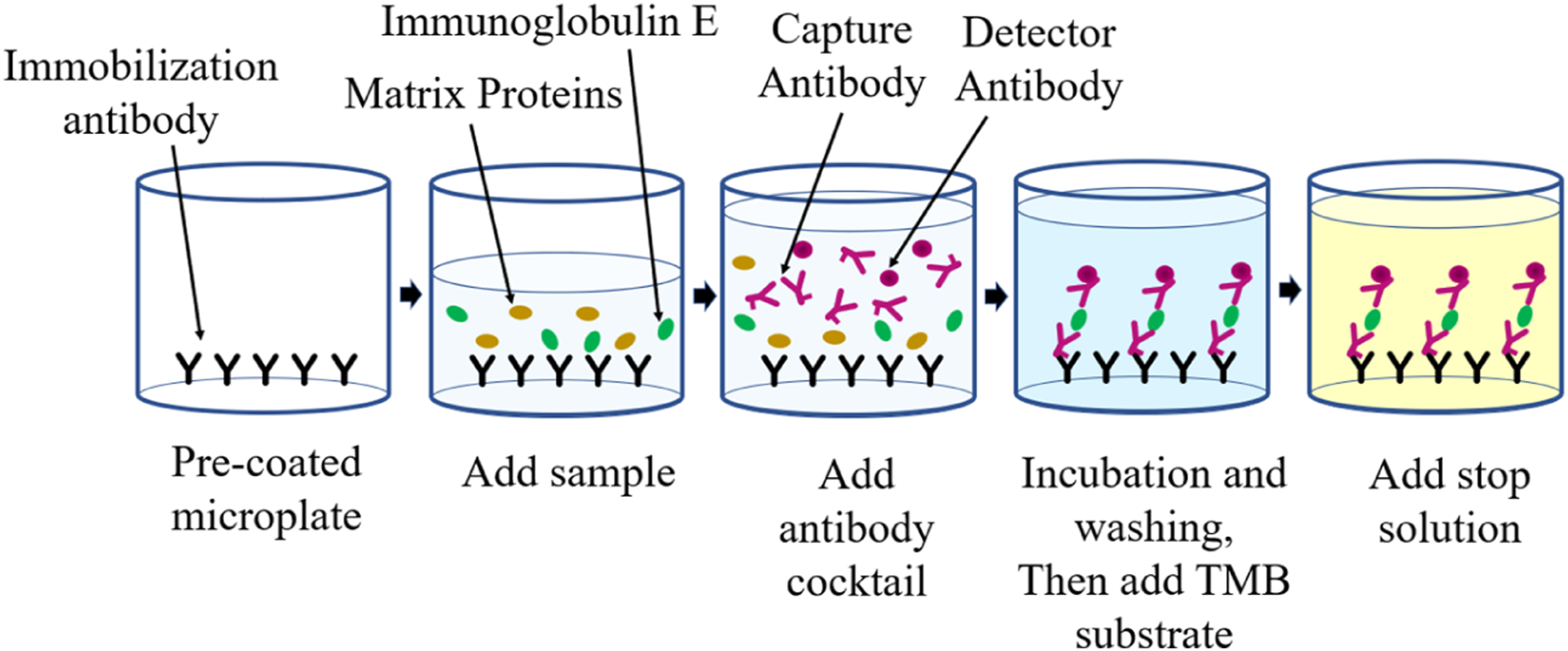
The saliva of the subjects was thawed and taken into the centrifuge tube. After centrifugation, the supernatant was taken as the prepared sample. All standards and reagents were prepared according to the instructions. The standard and sample were then added to the wells corresponding to the pre-coated microplate. A mixture of antibodies was added to all holes and the mixture was cultured at room temperature. The solution specific bound in the microplate: capture antibody combined with immobilised antibody; detector antibodies combined with the target analyte. After incubation and thorough washing, the substrate tetramethylbenzidine (TMB) was added for colour development. TMB was converted into blue under the catalysis of peroxidase, and the acid termination solution was added at the defined endpoint and the colour finally turned yellow. The optical density value (O.D. value) was measured at 450 nm by an enzyme-labelled instrument, and the sample concentration was calculated according to the O.D. value.
Experiment procedures
In addition to indoor air temperature, other environmental parameters such as air speed, relative humidity and illumination were kept constant. Air conditioning temperature settings and orders were confidential to each subject. The experimental process is shown in Figure 4. The experiment at each temperature lasted for 35 min. The subjects sat in the climate chamber for the first 30 min. Then they were required to complete the thermal comfort questionnaire and collected saliva in the following 5 min. The reason for letting subjects adapt themselves to each temperature for 30 min is that the human body would function normally at such air temperature after the 30-min exposure.
42
After the experiment under each temperature condition, the subjects went to the waiting room to take a 30-min rest and then entered the climate chamber to conduct the experiment under the next temperature condition. The temperature of the waiting room was about 25°C. Experimental process.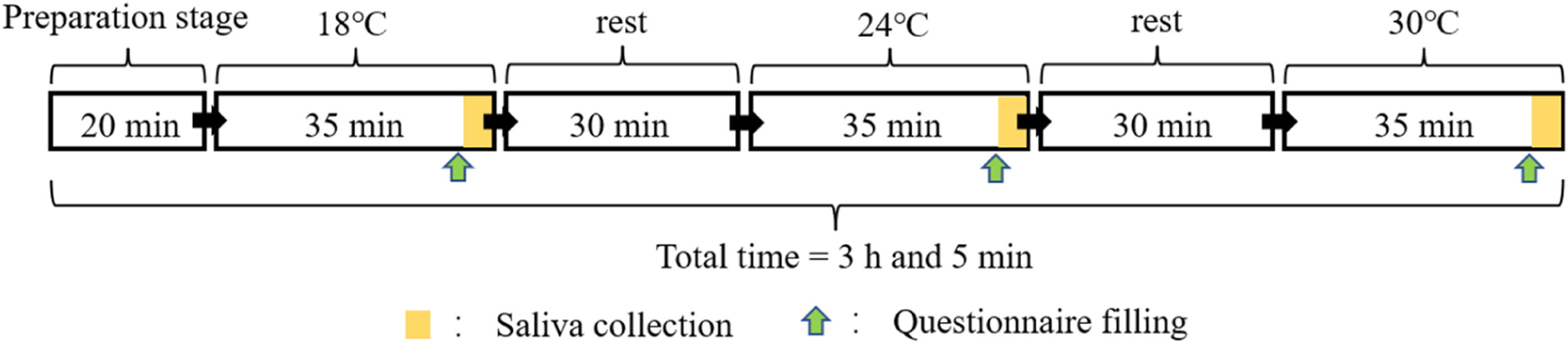
Data processing
The content of each immune parameter in the human body is quite different. In order to put each immune parameter on the same horizontal line for comparison, the data of the convection was processed dimensionless. The immune index was expressed as follows: the ratio of the measured value to the lower limit of the normal range value, indicating the multiple of the real value relative to the lower limit.
Before data analysis, box charts were generated and used to eliminate abnormal values. SPSS 26 was used for statistical analysis of the correlation and significant differences amongst data. Shapiro–Wilk test was used for normality testing. Independent sample T-test and Mann-Whitney test were used to analyse the significance of thermal comfort on salivary IgE concentration. Friedman rank-sum test was used to analyse the influence of air temperature on salivary IgE concentration. Pearson correlation analysis or Spearman correlation analysis was used to study the correlation between each parameter and IgE. All the explicitness tests were conducted based on the double-tailed test, and the explicitness level was set to 0.05 (p < 0.05).
Results
Natural environment temperature and immunoglobulin
The non-dimensional concentrations of serum IgE, IgG, IgA and IgM in the physical examination report of the epidemiological investigation were counted at 5°C intervals. They were divided into eight subgroups (Figure 5). The statistical analysis results are listed in Table 2. The variation of non-dimensional serum IgE, IgG, IgA and IgM concentrations with temperature (mean ± 95% confidence interval, * is p < 0.05, ** is p < 0.01). Correlation analysis and significance test of non-dimensional immunoglobulin concentration and air temperature.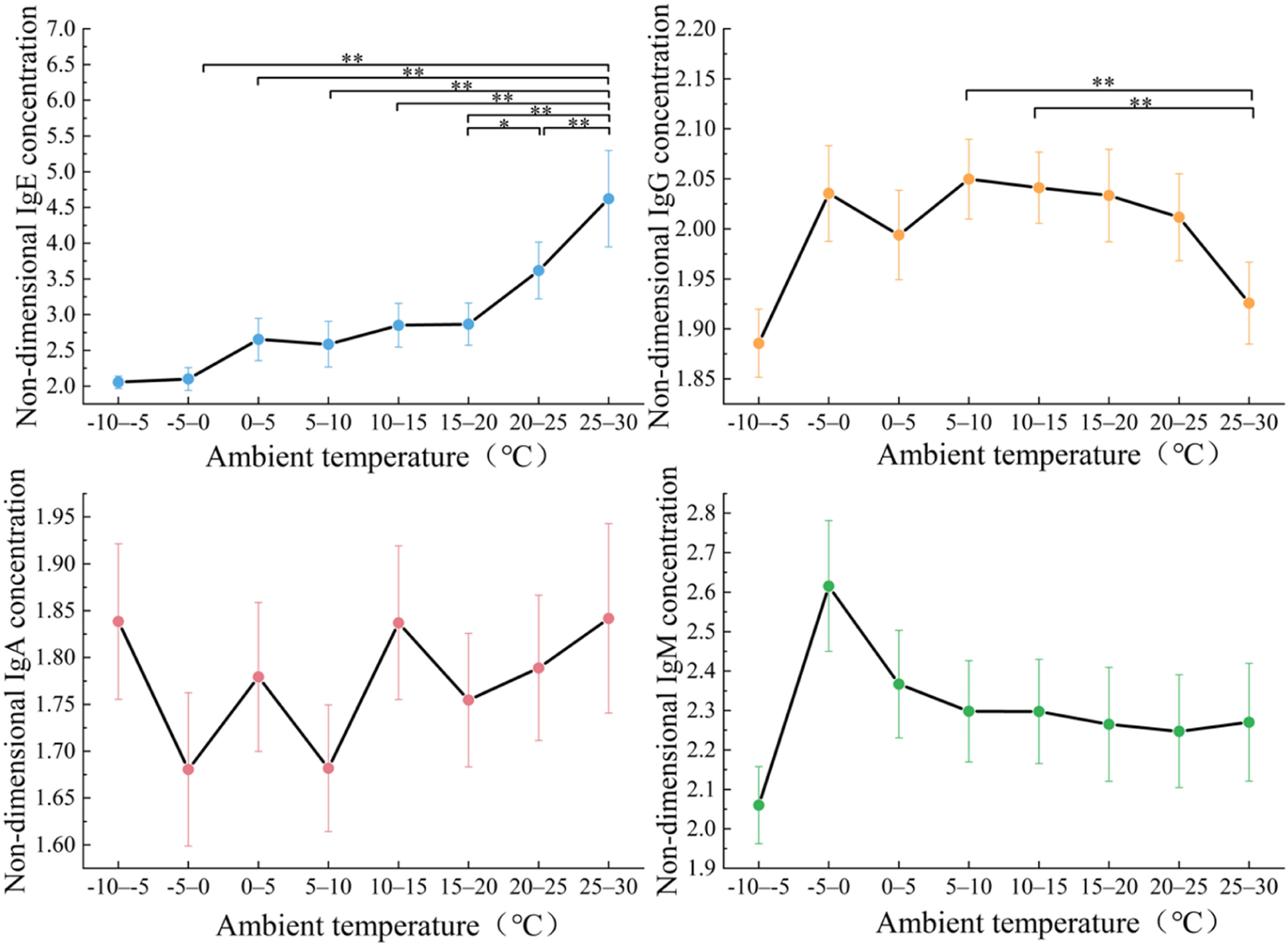
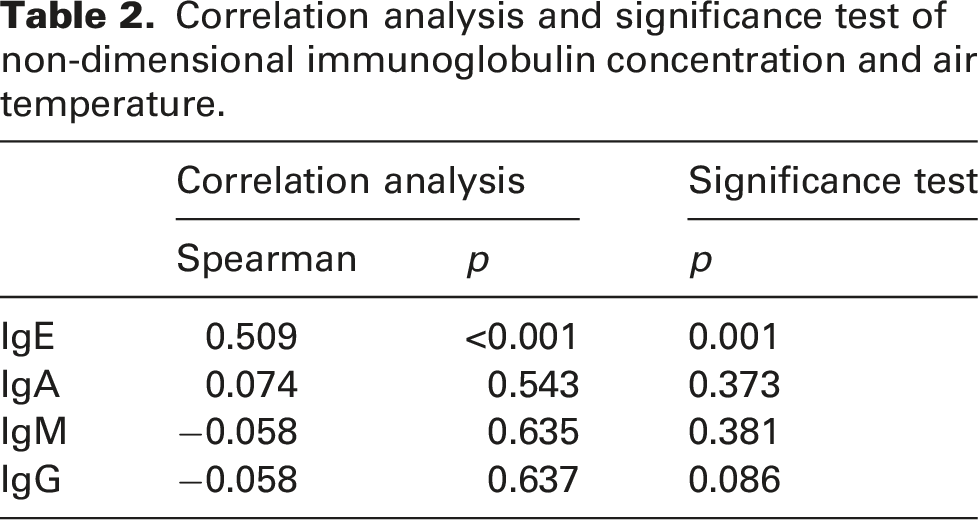
Non-dimensional IgE concentration increased significantly with the air temperature (p = 0.001). The above two parameters were significantly positively correlated (p < 0.001, Spearman = 0.509). The rise of the IgE concentration was small at 0–15°C and increased at 15–30°C. The non-dimensional IgE concentrations of subjects in the highest temperature range were 2.3 times that of the lowest temperature range. Significant differences existed between the non-dimensional IgE concentrations at 25–30°C and concentrations at each temperature range at −5 to 25°C.
Non-dimensional IgG concentrations showed an inverted U-shaped distribution with the increasing air temperature, which reached the highest value in the temperature range of 5–10°C and reached the lowest concentrations within the highest or lowest temperature range. The average non-dimensional IgG concentration in the interval of 5–10°C increased by 8.34% relative to the interval of −10 to 5°C and increased by 6.71% relative to the interval of 25–30°C. The results of statistical analysis showed that significant differences existed between 25 and 30°C, 5 and 10°C and 10 and 15°C. In short, IgG showed a decreasing trend under the most extreme conditions of atmospheric temperature in this city.
Non-dimensional IgM concentrations peaked at −5 to 0°C but tended to be flat with the increase in the air temperature. The IgM at different air temperature intervals overlapped with the confidence intervals of adjacent temperatures. Non-dimensional IgA concentrations fluctuated up and down with the temperature rising, without obvious rules. There was no significant difference between IgM and IgA with the temperature change.
Based on the above results, we chose IgE as the biomarker in the experiment for the following reasons: (1) The concentration of IgE varied the most with the change of temperature, which was much higher than the other three types of immunoglobulins, which showed that IgE was most sensitive to air temperature. (2) Part of IgE is produced by the plasma cells of the lamina propria of the respiratory tract mucosa, which is related to respiratory tract infection and can be used as a biomarker indicating the immunity of the respiratory tract mucosa. (3) With the popularisation of room temperature regulating equipment, people are more inclined to adjust the indoor temperature to their comfort zone or near the comfort zone. As a result, there are fewer extreme temperatures in the building interior. Therefore, IgG does not meet the application scenarios of the indoor environment experiment.
Built environment temperature and immunoglobulin E
Figure 6 shows the salivary IgE concentrations of different subjects in the experiment at 18, 24 and 30°C. The salivary IgE concentrations of 70% of Subjects (1–7) were increased with the increase of the air temperature. IgE concentrations of 20% of Subjects (8 and 9) were the highest at 24°C and the lowest at 18°C. The thermal comfort vote of Subjects 8 and 9 under different working conditions showed that Subjects 8 and 9 felt most comfortable at 24°C. The reason for not adding Subject 10 was that abnormal salivary IgE concentration was observed in Subject 10 whose IgE concentration was significantly higher. The salivary IgE concentration of different subjects.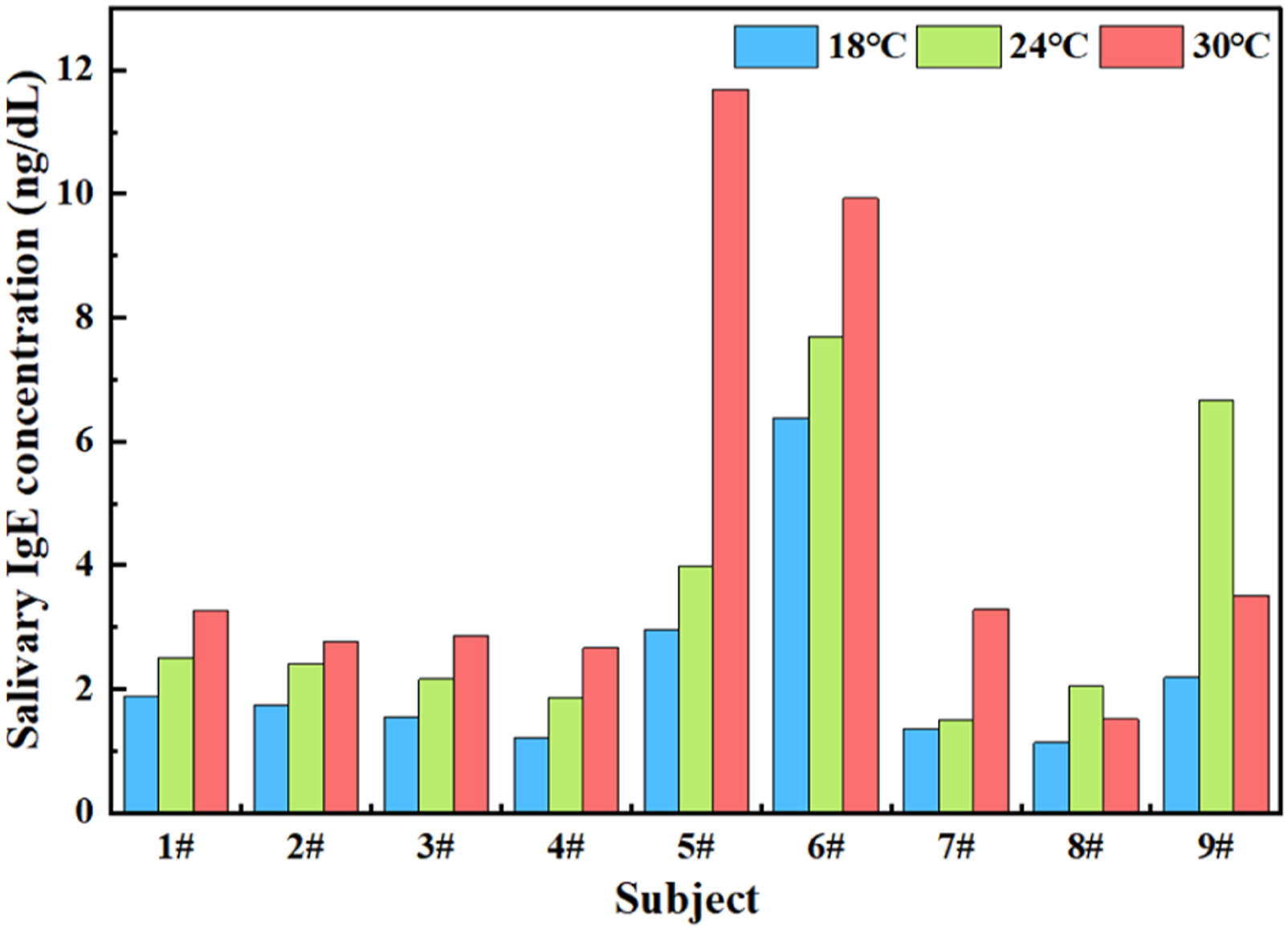
The air temperature had a significant effect on salivary IgE concentration (p = 0.002), and the two were positively correlated (p = 0.009, Spearman = 0.495). There were differences in the influence of air temperature on IgE of people with different constitutions. However, in general, for most people, maintaining a higher air temperature within a comfortable temperature range was conducive to increasing the IgE concentration in the human body, thereby enhancing the ability of the upper respiratory tract mucosa to resist external virus microorganisms.
Thermal comfort and salivary IgE concentration
The relationship between thermal comfort and salivary IgE concentration in the experiment is shown in Figure 7. Human comfort induced by the thermal environment was related to salivary IgE concentration. The average salivary IgE concentration in the comfortable state was the highest and was increased by 76.4% and 110.3% compared with that under the slightly uncomfortable and uncomfortable conditions, respectively. There was a significant difference in the average salivary IgE concentration between comfortable and uncomfortable states (p = 0.025), but there was no significant difference between comfortable and slightly uncomfortable, slightly uncomfortable and uncomfortable (p = 0.145, p = 0.199). This trend inferred that people have a higher level of mucosal immunity in the respiratory system in a thermally comfortable state. Therefore, the improvement of the antibody concentration of upper respiratory mucosa may be possible by creating a comfortable thermal environment. Relationship between thermal comfort and salivary IgE concentration in the experiment (* is p < 0.05, IQR is the interquartile range).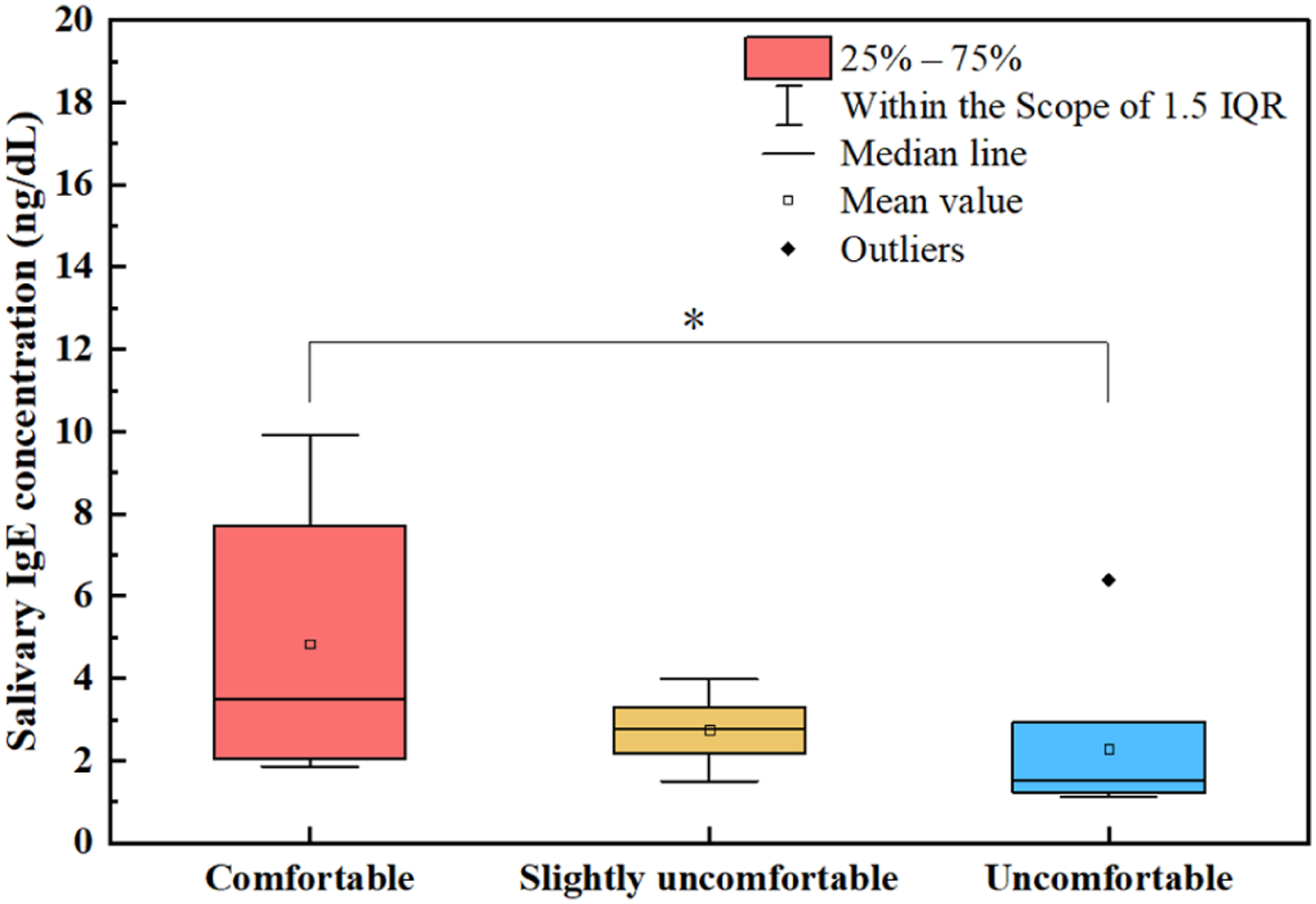
Discussion
There were two stages in this study. The first stage was the epidemiological investigation and the second stage was the experiment under a controlled indoor environment. The epidemiological investigation explored the relationship between population immunoglobulins and environmental temperature, aiming to screen biomarkers suitable for the experiments. The important observation was that, compared with other immunoglobulins, IgE can better reflect the impact of temperature changes on human immunity. The serum IgE concentration was positively correlated with the temperature. However, the epidemiological investigation was difficult to rule out the influence of factors other than the temperature on the concentrations of immunoglobulin. In addition, the outdoor temperature cannot represent the indoor air temperature in living spaces. People spend 90% of their time indoors, and the air temperature inside buildings is usually kept within the comfort zone or near the comfort zone. Therefore, we further designed an indoor environment experiment to verify the relationship between individual IgE concentration and indoor air temperature under the premise of controlling variables, aiming to explore the indoor air temperature that is conducive to upper respiratory mucosal immunity. The results of the experiments showed that most subjects had higher salivary IgE concentrations at warmer and more comfortable indoor air temperatures, which verified the correctness and applicability of the epidemiological investigation. Improper temperature regulation of indoor air conditioners is one of the causes of sick building syndrome (SBS). 43 In the design of the building’s thermal environment, a much healthier indoor environment can be created by ensuring a warm and comfortable thermal environment. Besides, the serum and salivary IgE concentrations mentioned in this study were within the normal range of the human body. All analysis was based on the IgE indicators of healthy individuals and did not involve the pathological range. So, the findings of this study could only be applicable to healthy people.
Air temperature plays an important role in the adaptive immune system. 44 Exposure to cold conditions increases the risk of respiratory infections. 45 Body temperature is closely related to immunity. When the body temperature falls by 1°C, human immunity would be reduced by 30%. 46 Body temperature could also affect the number of white blood cells in the body. 47 Higher body temperature could activate more immune cells in the human body; thus, viruses and bacteria could lose their activity under high body temperature, 48 so that immune cells can better annihilate invading pathogenic microorganisms and maintain physical health. At the same time, the psychological state is also one of the important factors affecting immunity; positive emotions have been reported to contribute to the physical health of humans. 49
As one of the important factors affecting the human thermal environment and comfort, clothing is the main means for people to actively adapt to external climate change. Clothing affects the heat and moisture exchange between the human body and the surrounding environment, thereby affecting the skin temperature of the human body and further affecting the immunity of the human respiratory system. Exercise can significantly improve the body’s metabolic rate, thereby increasing body temperature. When the number of exercises increases and the metabolic level improves, the human body could increase heat dissipation through sweating and maintain body temperature constant. Studies have found that a certain level of exercise (such as fitness and other aerobic exercises) can improve the body’s metabolism. Under high metabolism, the body’s demand for oxygen and food increases, and heat production and body temperature would increase, thereby enhancing the body’s immunity. Furthermore, the acceleration of metabolism caused by exercise can also speed up the excretion of antigen-antibody binding reactants, thereby reducing the antigen concentration in the body. Fitness exercise can also relax the body, relieve tension, regulate the endocrine and improve the comprehensive immunity of the body. For example, the square dance in Wuhan shelter hospital plays a positive role in sports and emotion. As a natural heat source, solar radiation not only contributes to the synthesis of antimicrobial peptides but also can improve thermal sensation and skin temperature. When the radiation temperature decreases, the radiation heat transfer between the human body and the environment would reduce and decrease the skin temperature. Therefore, as the season changes from warm to cold, the radiation temperature of the external environment on the human body decreases, which would reduce the skin temperature to a certain extent, which is not conducive to the improvement of immunity.
The higher core temperature may not always benefit the human body. Not all immune cells of the human body prefer a high-temperature environment. When the body temperature is 38–40°C, the activity of human leukocytes reaches the top level, but the activity of natural killer cells (NK cells) and macrophages decreases under high temperatures.50,51 Excessive body temperature for a long time could accelerate material metabolism, thus interfering with the normal physiological functions of the digestive system and nervous systems, and reduce the anti-infective ability of the body and leading to organ dysfunction. Heat stress above 41°C is also associated with lymphocyte reduction and apoptosis,48,52 so the human body cannot maintain a high temperature for a long time. Moreover, high-intensity and competitive sports could reduce the concentration of IgA and increase upper respiratory tract infections. This could probably be ascribed to the fact that high-intensive exercise usually brings more sweating thus contributing to the reduction of the core temperature. This conclusion has been verified by many studies.53–55 During a moderate and vigorous aerobic exercise of less than 60 min, the recycling and function of a series of cells that play an important role in the immune system (such as the activity of macrophages against pathogens, NK cells, B cells and T cells) have been greatly improved. 56 Whether exercise is beneficial to immunity is related to environmental temperature. That is, there is an interaction between exercise and temperature on human immunity. At the air temperature between 6°C and 34°C, moderate exercises do not affect mucosal immunity, nor do they affect the upper respiratory tract infection rate. 57
There were several limitations in this study. First of all, the sample size in the experiment was not big enough, and all these subjects were young people. There was a lack of research on children or the elderly, which would limit the potential applications in real life. Secondly, there were few temperature settings thus leading to narrowed indoor air temperature range. In future studies, more temperature will be applied and more subjects will be recruited for experiments, so as to obtain more comprehensive and universal observations.
Conclusions
In this study, the effects of the air temperature on the IgE concentration of healthy people in both the natural environment and built environment were analysed, through epidemiological investigation and experiment. The findings are given below. 1. Through the epidemiological investigation, the serum IgE concentration was found to be the most sensitive factor to the air temperature compared with the other three immunoglobulins. Its concentration had a significant positive correlation with the air temperature. Consequently, the IgE was chosen as the biomarker in the experiment under controlled conditions. 2. Results of the experiments showed that the salivary IgE was positively correlated with the indoor air temperature within the comfortable temperature zone, and increased significantly with the increase of thermal comfort votes.
The findings of this study implied that keeping a warm air temperature within the comfortable temperature range could elevate the IgE concentration of antibodies in the normal range. In daily life, creating a comfortable and warm built thermal environment is one of the measures to improve the mucosal immunity of the human respiratory system, especially during the outbreak of influenza and pneumonia.
Footnotes
Author contributions
Songtao Hu: conceptualisation, resources and writing – review and editing. Rujin Liu: investigation, data curation, original draft and writing – review. Hui Li: investigation. Hui Zhu: review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the National Natural Science Foundation of China (No. 52108080).
Ethical approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of Qingdao University of Technology (QUT.L.01).
Data availability
Data are not publicly available due to restrictions regarding the privacy of the participants.