
Abstract
During the COVID-19 pandemic, Chinese universities implemented many interventions against SAR-CoV-2 transmission. Close contact is thought to be a major transmission route. However, the effect of university closure-related interventions on infection risk amongst students is still poorly understood. In July 2022, we conducted an online survey of 2,400 university students in Beijing and Shanghai. Combined with real human behaviours, we evaluated the infection risk via close contact during both periods of university closures and non-closures. During the non-closure period, undergraduate and postgraduate students spent the longest close contact time in classrooms and graduate student offices, averaging 1.9 h and 2.2 h, respectively. During university closures, students spent the longest close contact time in residences (dormitories and homes), reaching up to 2.8 h. Catering places and residences were the two main indoor environments for viral exposure via close contact. Viral exposure did not differ significantly by education background or gender (p > 0.05) but did by intervention levels in university or community (p < 0.05). The infection risk decreased by 30.0% for resident students and 63.6% for non-resident students during university closures. The findings could provide scientific support for intervention policy-making during public health emergencies such as COVID-19 pandemic.
Introduction
Since the outbreak of Coronavirus Disease 2019 (COVID-19) in December 2019, various countries have implemented a series of interventions to curb its spread, such as nucleic acid testing, vaccination and social distancing (e.g. school closure).1–4 School closures, implemented to counter Severe Acute Respiratory Syndrome Coronaviruses-2 (SARS-CoV-2) transmission, have impacted around 90% of global students, meaning over 1.6 billion students from at least 190 countries and regions were affected, with higher education students comprising about 1/8. 5 It is vital to assess the effectiveness of interventions relating to school closures on infection risk of students during the COVID-19 pandemic.
Close contact, defined as interactions (with or without conversation) within a range of 1.5 m, is the main transmission route of COVID-19. 6 Interventions of different intensities inevitably led to variations in students’ close contact behaviours. During the pandemic, the duration of students’ close contact in learning environments (e.g. classroom) was decreased by 66.0%, 7 and close contact rate in subway was 56.1%. 8 Moreover, changes in close contact behaviours have a direct impact on students’ infection risk. 6 Primary and secondary educational institutions usually mandate their students to stay at home during outbreaks. 9 Compared with adolescents, university students are more vulnerable to SARS-CoV-2, and their daily activities are more complex.6,10
Most studies have focused on assessing the effectiveness of strategies aimed at reducing the incidence rate amongst university students. Social distancing and mask-wearing on campus have been demonstrated to effectively reduce incidences of infection amongst students, with a potential reduction of approximately 87% of cases. 11 Testing and contact tracing measures may result in a reduction of over 30% of cases.12,13 The cumulative incidence amongst students differs by approximately 50% between weekly and monthly screenings. 13 Additionally, some studies have evaluated the risks of reopening campuses during pandemics. Early reopening phases may attract students from regions with high COVID-19 incidence, thereby increasing the infection risk. 14 In May 2022, universities in Beijing strictly enforced university closures and controlled campus access. 15 From 28 March to 1 June 2022, Shanghai underwent a 75-day lockdown. 16 After lifting the lockdown, Shanghai’s universities continued various levels of university closure-related interventions based on local transmission trends. However, the level of interventions implemented by schools or communities depends largely on the evolving epidemiological situation. Therefore, there remains a gap in understanding the impact of different levels of university closure-related interventions on infection risk amongst students.
In this study, utilizing online surveys, we targeted university students in Beijing and Shanghai to compare close contact behaviours during both non-closure and university closure periods. Combined with real student behaviours, we further quantified infection risk via close contacts associated with the Omicron variant, considering various personal protection measures and university closure-related interventions. This research would provide insights for more rational intervention strategies on campuses and within communities and would aid in alleviating the economic and social pressures in similar public health incidents.
Methods
Study design and participants
At 9:00 a.m. on 18 July 2022, we distributed 2400 online surveys to university students from seven universities in Beijing and three universities in Shanghai. By 5:00 p.m. that day, we completed the data collection. The questionnaire was made using the Questionnaire Star platform (www.wjx.cn) and was shared through WeChat (the most popular social app in China) groups. All respondents were enrolled in universities. Depending on their choices, participants may answer between 15 and 37 questions with an estimated completion time of 2 to 7 min. Each respondent had a single opportunity to submit their responses. Those who provided valid answers received a reward of ¥6.5 RMB (about $0.9 US dollars). Of the 2400 surveys collected, 2092 were valid, with 308 being invalidated (Figure 1). This survey was approved by the Ethics Committee of Beijing University of Technology (No. CJXB 05-07). Flow chart for screening online-collected surveys in Beijing and Shanghai on 18 July 2022.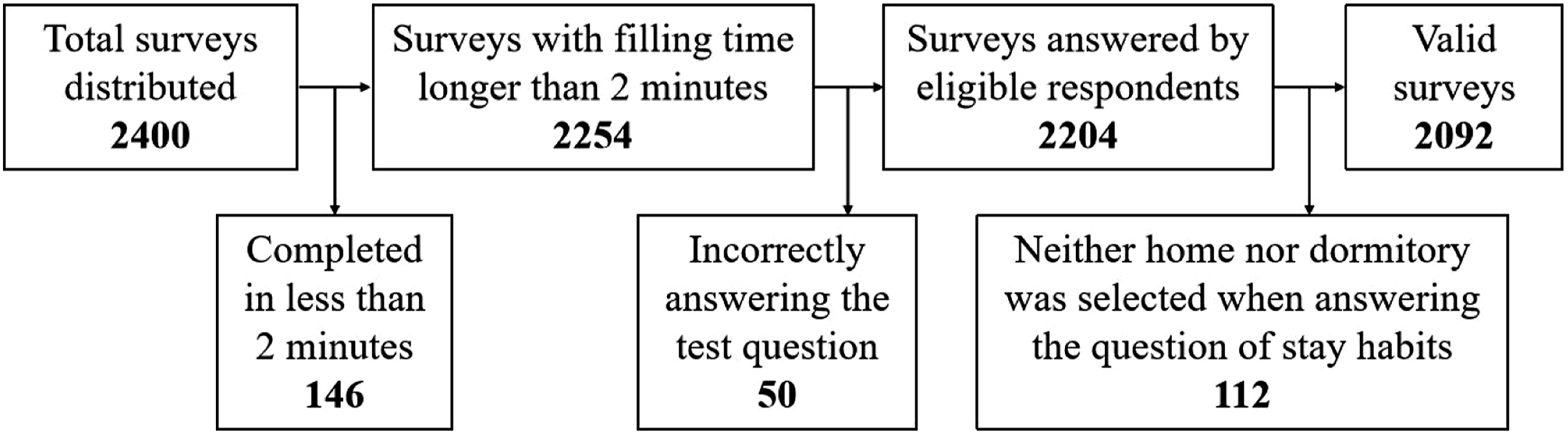
Data collected in the survey
This survey collected basic personal information of university students, university closure-related interventions they experienced and their stay habit in indoor environments. The basic information included gender, age, educational background and the city in which their university is located. Considering two periods (during university closure and non-closure) and two categories of students (resident and non-resident), we identified eight university closure-related interventions of varying intensities: (1) NA: Resident students, referred to as ‘residents’, during the non-closure period. (2) A3: Residents subjected to the intervention of ‘freedom of activity on campus’ during the university closure period. (3) A2: Residents who underwent the intervention of ‘allowed to leave the dormitory at a fixed time’ during the period of university closures. (4) A1: Residents who faced the intervention of ‘strict confinement within dormitory buildings’ during university closures. (5) NB: Non-resident students (non-residents) during non-closures. (6) B3: Non-residents who experienced the intervention of ‘free activity’ during university closures. (7) B2: Non-residents who underwent the intervention of ‘confined to the community’ during university closures. (8) B1: Non-residents who faced the intervention of ‘confined to the home’ during university closures.
Given the distinct functions of various indoor environments, we categorized them into nine types: homes, dormitories, graduate student offices, catering places, classrooms, libraries, supermarkets, public transportation and entertainment venues (e.g. Karaoke Television, KTV). 6 We collected the stay habits of university students within each indoor environment during both the period of non-closures and university closures. The habit parameters include stay time, stay probability, close contact time and close contact rate (defined as the ratio of close contact time to stay time).
Data analysis
Considering that most people cover the mouth and nose when coughing and sneezing,
17
this study only considered two exhalation activities: breathing and speaking. Exhaled fine aerosols (≤5 μm in diameter) can be directly inhaled by susceptible individuals, while coarse aerosols (>5 μm) may settle on their facial mucous membranes, resulting in a potential infection risk.
18
As the aerosols generated from breathing are primarily smaller than 5 μm in particle size, coarse aerosols from this exhalation activity were not included in this analysis. The average load in fine aerosols produced by confirmed COVID-19 patients during breathing is 4.54 × 10−2 RNA copies/s and during speaking, the rates in fine and coarse aerosols are 1.01 and 7.43 × 10−2 RNA copies/s, respectively.
19
We used equation (1) to estimate the daily viral exposure via close contacts of university students during both the period of non-closures and university closures.
6
The infection risk P for susceptible individuals via close contacts could be calculated by the dose–response model, shown in equation (2).
20

Assuming the ratio of k i to k d is 0.1, we further evaluated the efficacy of personal protective measures adopted by university students during the COVID-19 pandemic. These measures included mask-wearing, interpersonal distancing and the duration since the completion of basal immunity (defined as on-time and full to complete the initial COVID-19 vaccination protocol). In our analysis, the fitted N95 respirator, surgical mask and cloth mask without a filter layer were evaluated with filtration efficiencies of 94.7%, 50.6% and 41.3%, respectively. 24 Three interpersonal distancing were considered, at least 0.5 m, 1.0 m and 1.5 m, respectively. Post-completion of basal immunity, the vaccine’s effectiveness against SARS-CoV-2 infection was 73.4% within 0 and 3 months, 30.5% between 4 and 6 months and 22.3% after 6 months. 25
Data processing
Data were presented as frequencies and proportions or as medians with interquartile ranges (IQRs). When calculating the average value of close contact rates, we excluded the bottom 2.5% and top 2.5% of the data. The chi-square test was used to examine the differences in frequency distributions of categorical variables. Close contact time and exposure risk data did not follow a normal distribution. Thus, the Mann–Whitney U test was used for independent sample comparisons, examining differences between resident and non-resident students, undergraduates and postgraduates or males and females during non-closure periods. The Kruskal–Wallis one-way ANOVA test was employed to compare differences amongst various interventions, followed by pairwise comparisons with significance values adjusted using the Bonferroni correction method. The median value of exposure risks under different interventions was used to calculate the average infection risk for students. Weighted averages were used to describe infection risk. A two-sided p-value of less than 0.05 was considered statistically significant. Statistical analyses were conducted using IBM SPSS Statistics 26, and MATLAB 2018b was utilized for calculating the k i values.
Results
Basic characteristics of surveys
Baseline characteristics of the survey data.
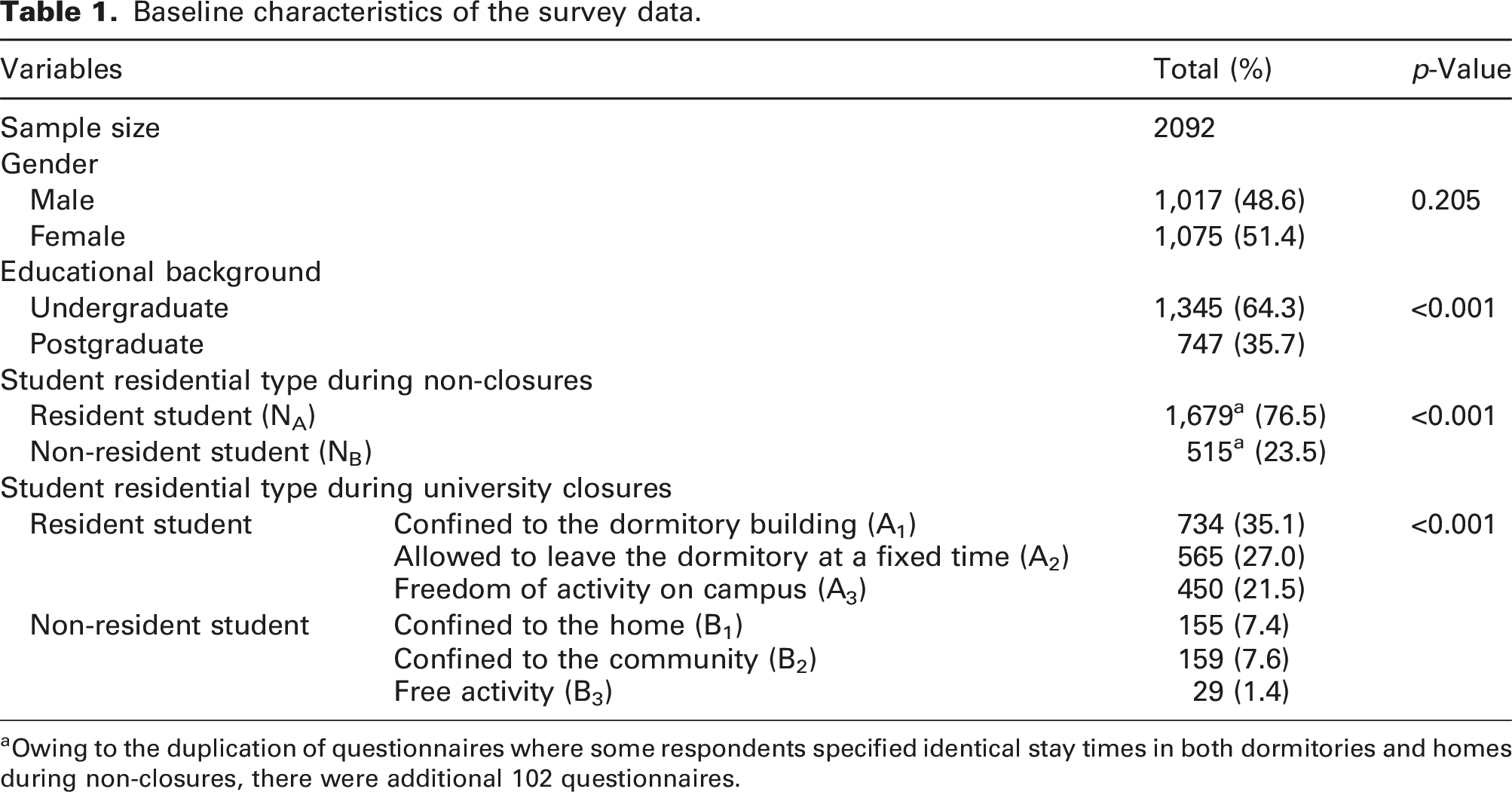
aOwing to the duplication of questionnaires where some respondents specified identical stay times in both dormitories and homes during non-closures, there were additional 102 questionnaires.
Human close contact behaviour
Close contact time in various indoor environments and daily total close contact time amongst university students under different intervention scenarios.
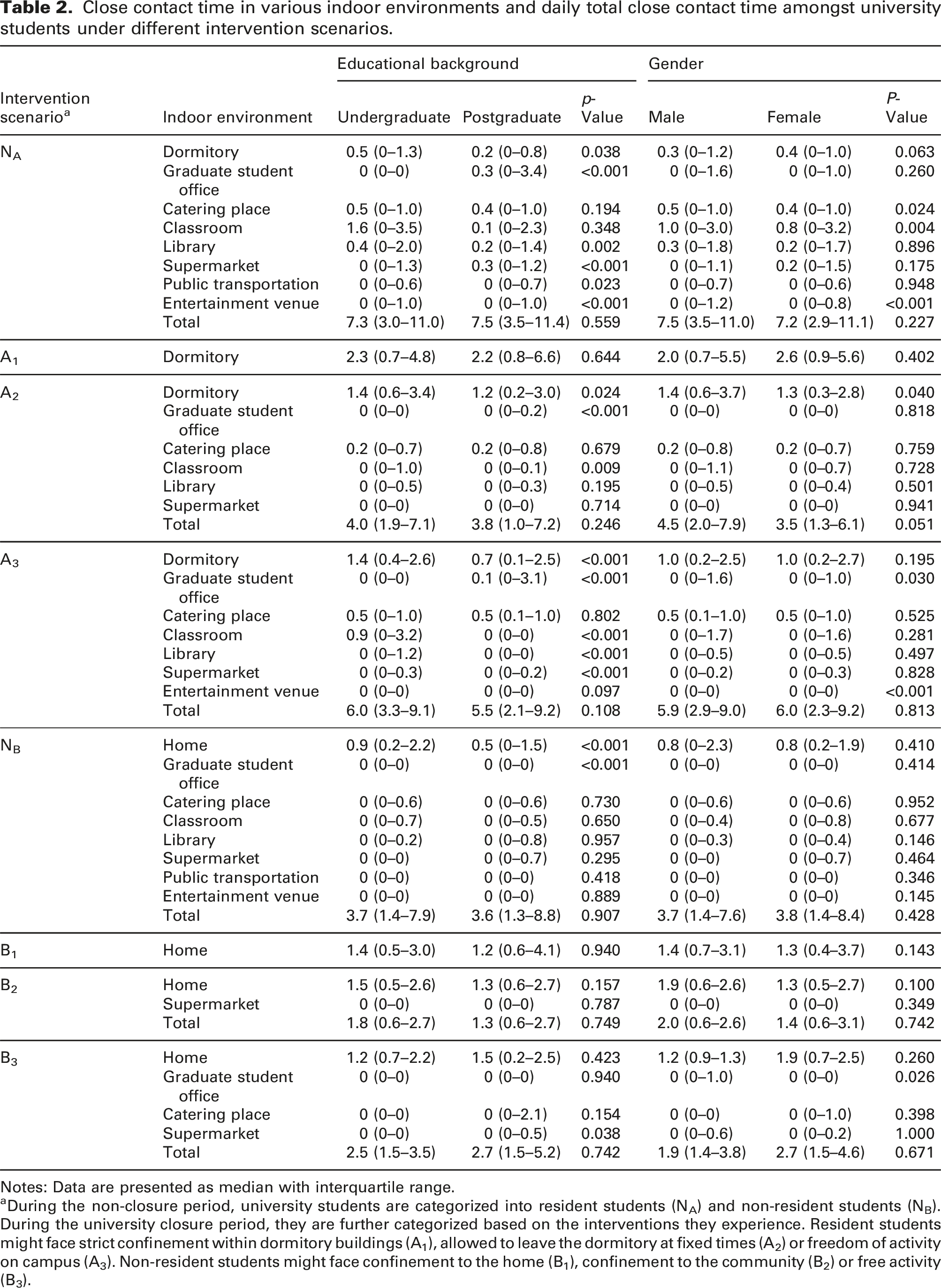
Notes: Data are presented as median with interquartile range.
aDuring the non-closure period, university students are categorized into resident students (NA) and non-resident students (NB). During the university closure period, they are further categorized based on the interventions they experience. Resident students might face strict confinement within dormitory buildings (A1), allowed to leave the dormitory at fixed times (A2) or freedom of activity on campus (A3). Non-resident students might face confinement to the home (B1), confinement to the community (B2) or free activity (B3).
Viral infection risk via close contacts
Classrooms were the indoor environment with the lowest exposure rate, at 2.9 × 10−6 RNA copies/s. In contrast, catering places had the highest exposure rate of 3.2 × 10−5 RNA copies/s, approximately 10 times that of classrooms (Figure 2). During the non-closure and university closure periods, viral exposure rate via close contact amongst university students of (a) educational backgrounds (undergraduate/postgraduate) and (b) gender (male/female) in various indoor environments under different intervention intensities.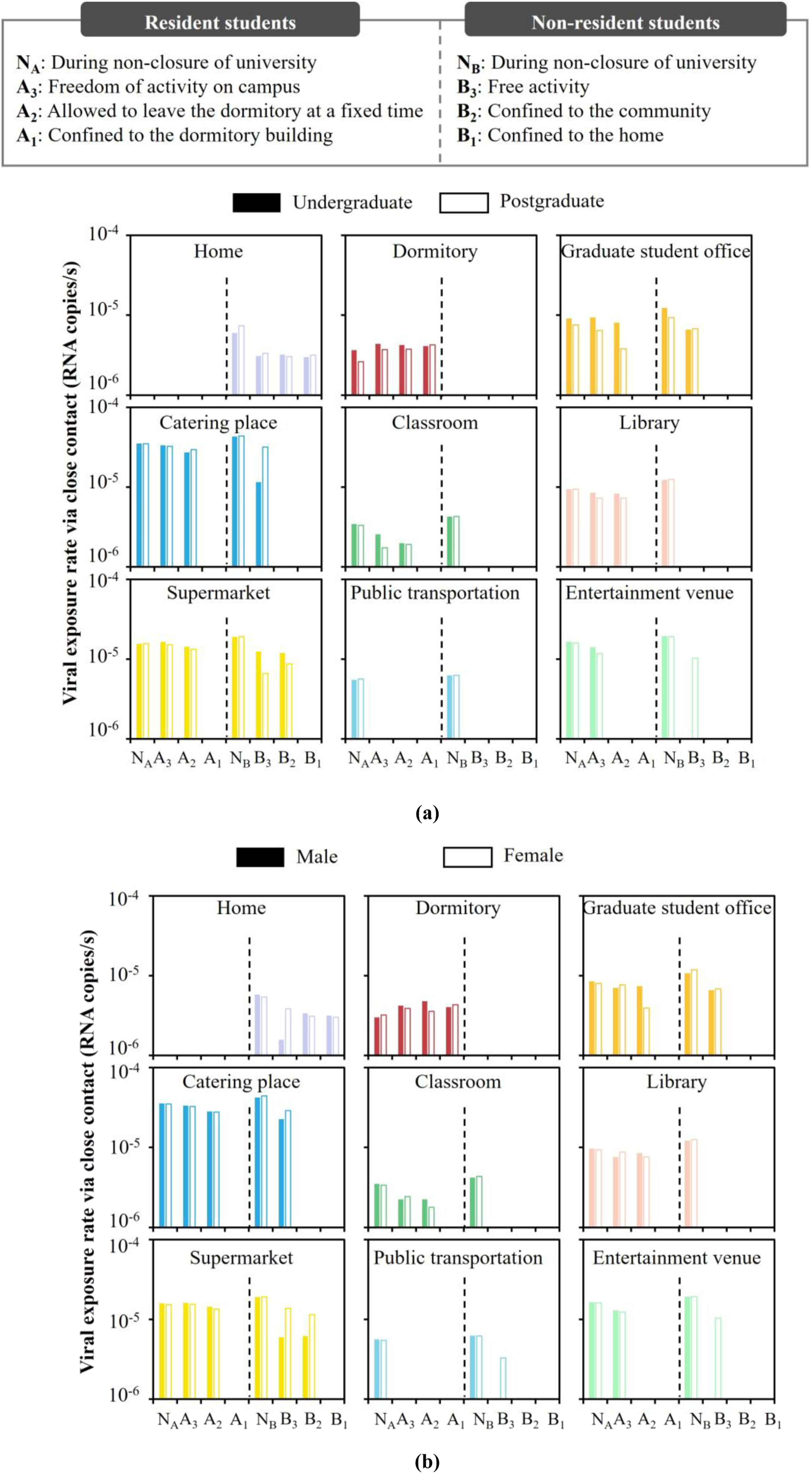
During the non-closure period, resident undergraduates had the highest viral exposure in catering places, with a contribution rate of 29.4% (Figure 3). Non-resident undergraduates primarily encountered the highest viral exposure at home (25.7%), followed by catering places at 21.5%. Resident postgraduates faced the most viral exposure in their offices, accounting for 26.6%, then catering places at 24.5%. Non-resident postgraduates predominantly spent time at home, with a contribution rate of 25.4%, followed by offices at 20.7% and catering places at 19.1%. During university closures, when students were free to move on campus (A3), the highest viral exposure was in catering places with an average contribution rate of 35.3%, followed by the offices (17.9%). When other interventions were implemented, residences were the indoor environment with the highest viral exposure, with a contribution rate of no less than 47.2%. During non-closure and university closure periods, daily close contact viral exposure amongst university students of different (a) educational backgrounds (undergraduate/postgraduate) and (b) gender (male/female) in various indoor environments under different intervention intensities.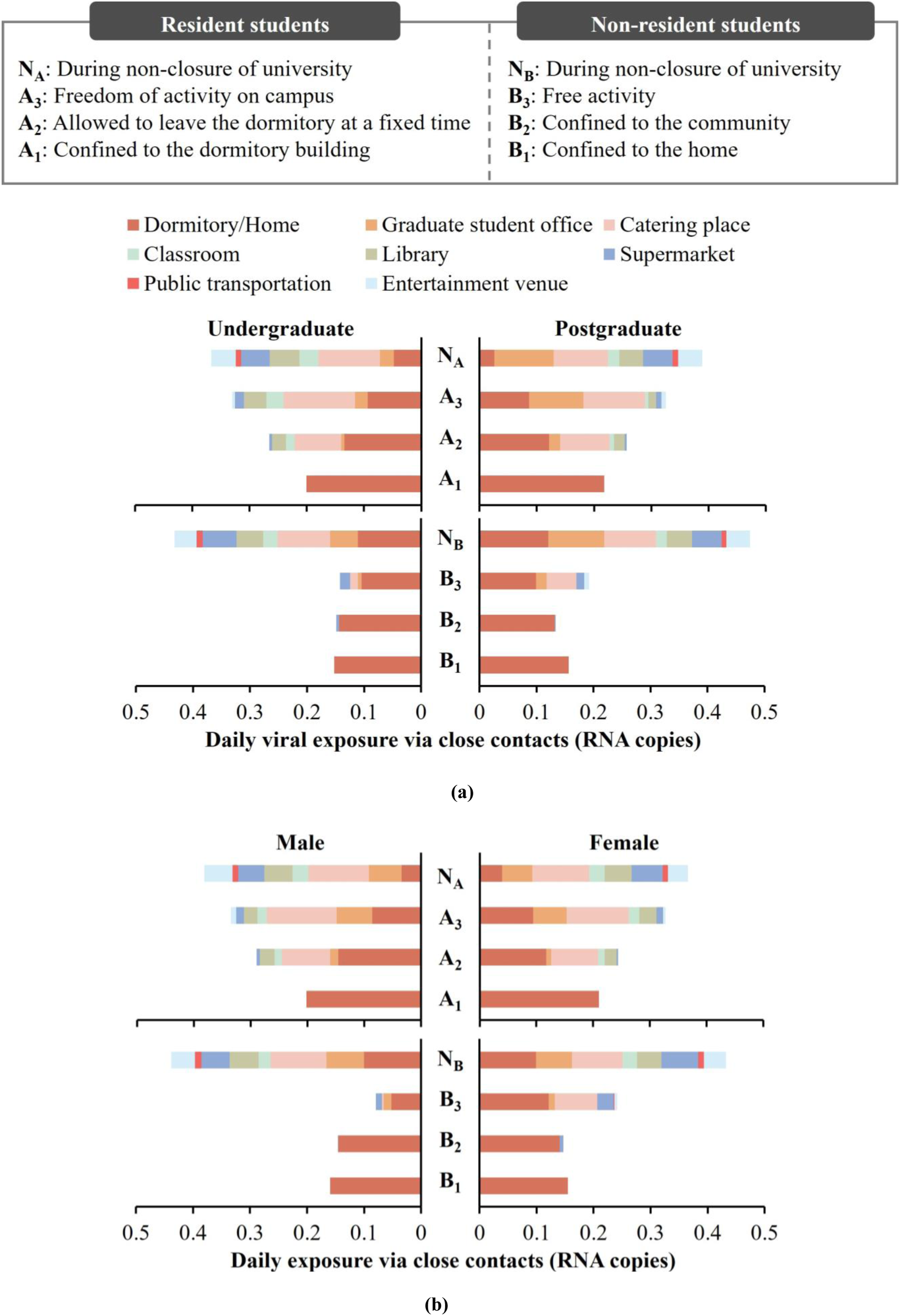
Overall, there was no significant difference in daily virus exposure amongst students of different education backgrounds and genders (p > 0.05) (Figure 4). Therefore, subsequent analyses did not distinguish between student types. Merely being confined to the university or community did not significantly affect daily exposure risks. Significant reduction in daily virus exposures only occurred when students faced stricter interventions (p > 0.05). In summary, during university closures, the daily exposure risk for university students was reduced by 37.3% compared with the non-closure period. This represented a 31.5% reduction for resident students and a 66.6% reduction for non-resident students. Comparison of daily close contact viral exposure amongst university students of different educational backgrounds (undergraduate/postgraduate) and gender (male/female) during non-closure and university closure periods (*** represents statistical significance with a p-value less than 0.001).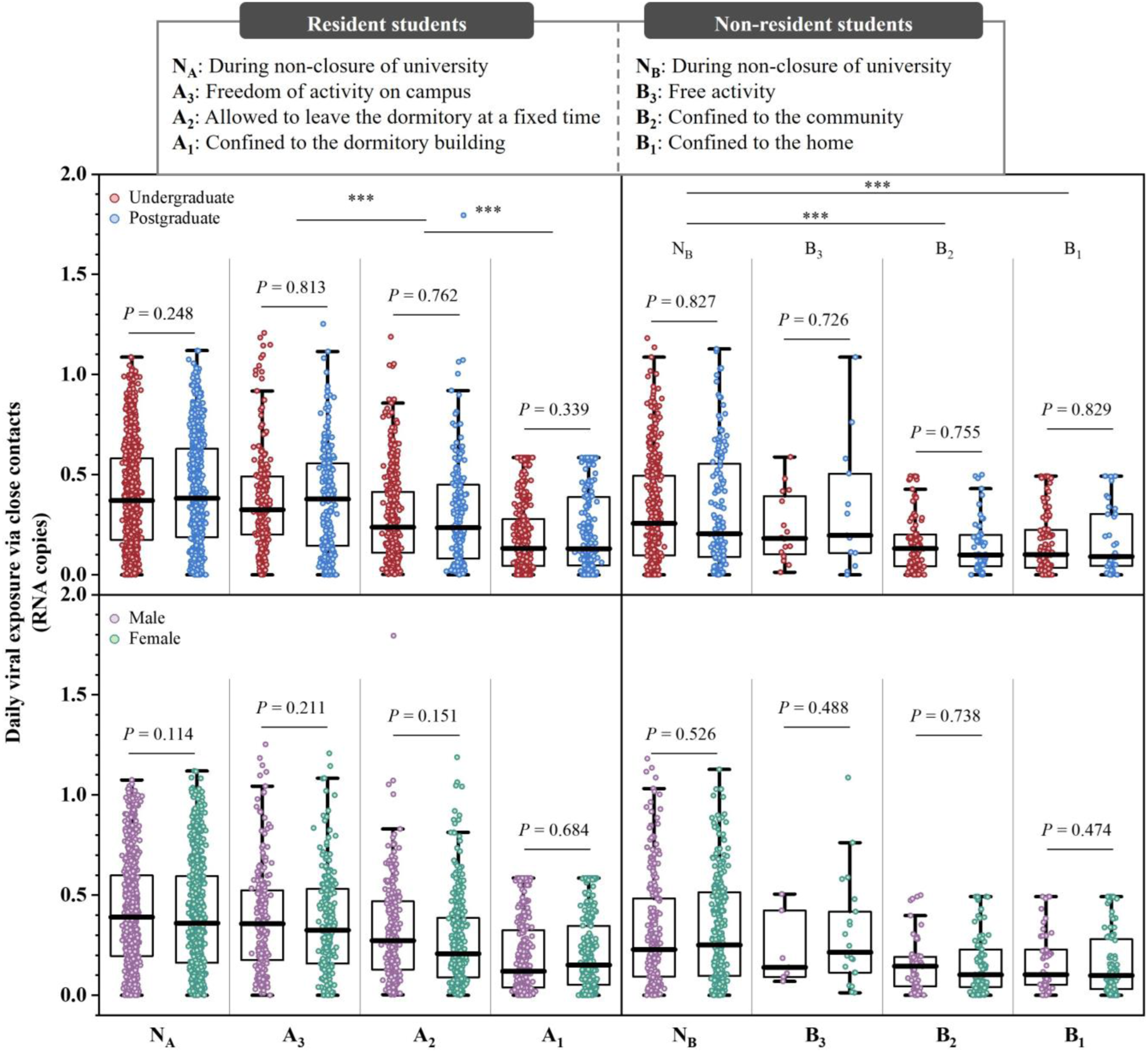
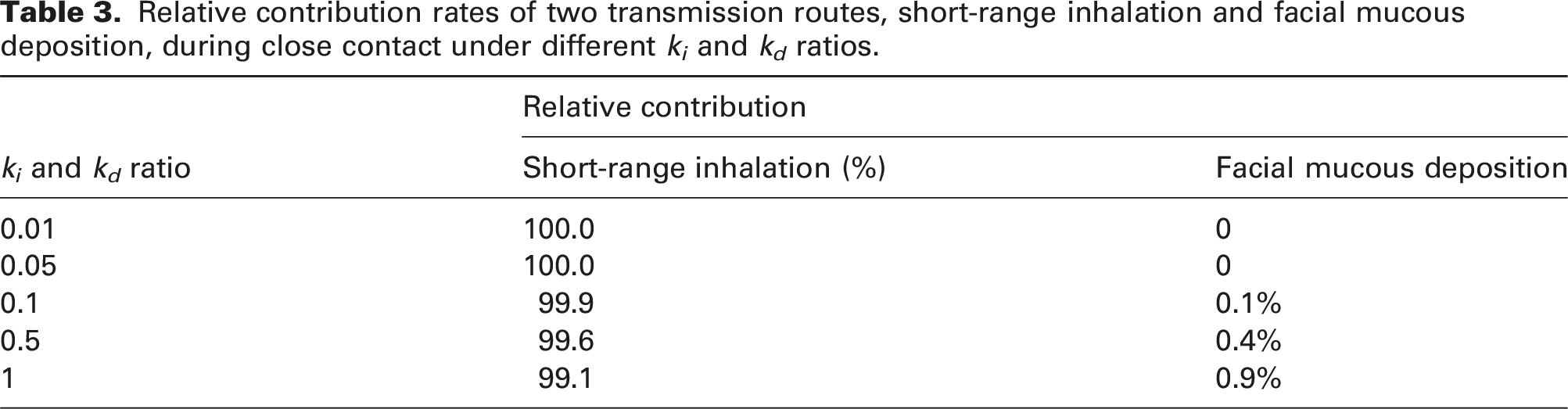
Relative contribution rates of two transmission routes, short-range inhalation and facial mucous deposition, during close contact under different k i and k d ratios.
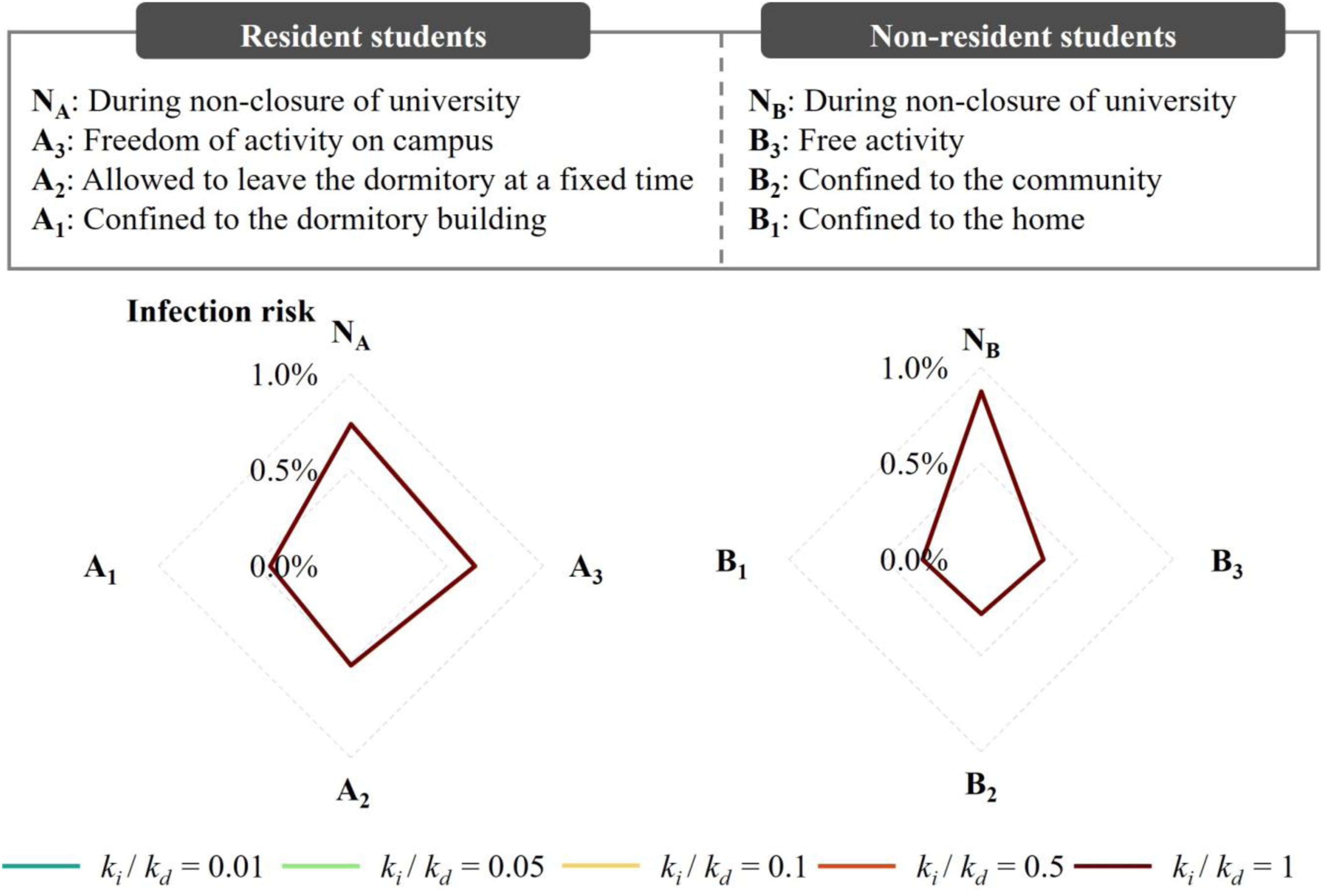
During non-closure and university closure periods, daily infection risk via close contact for university students at different k i and k d ratios under various intervention intensities.
Efficacy of interventions
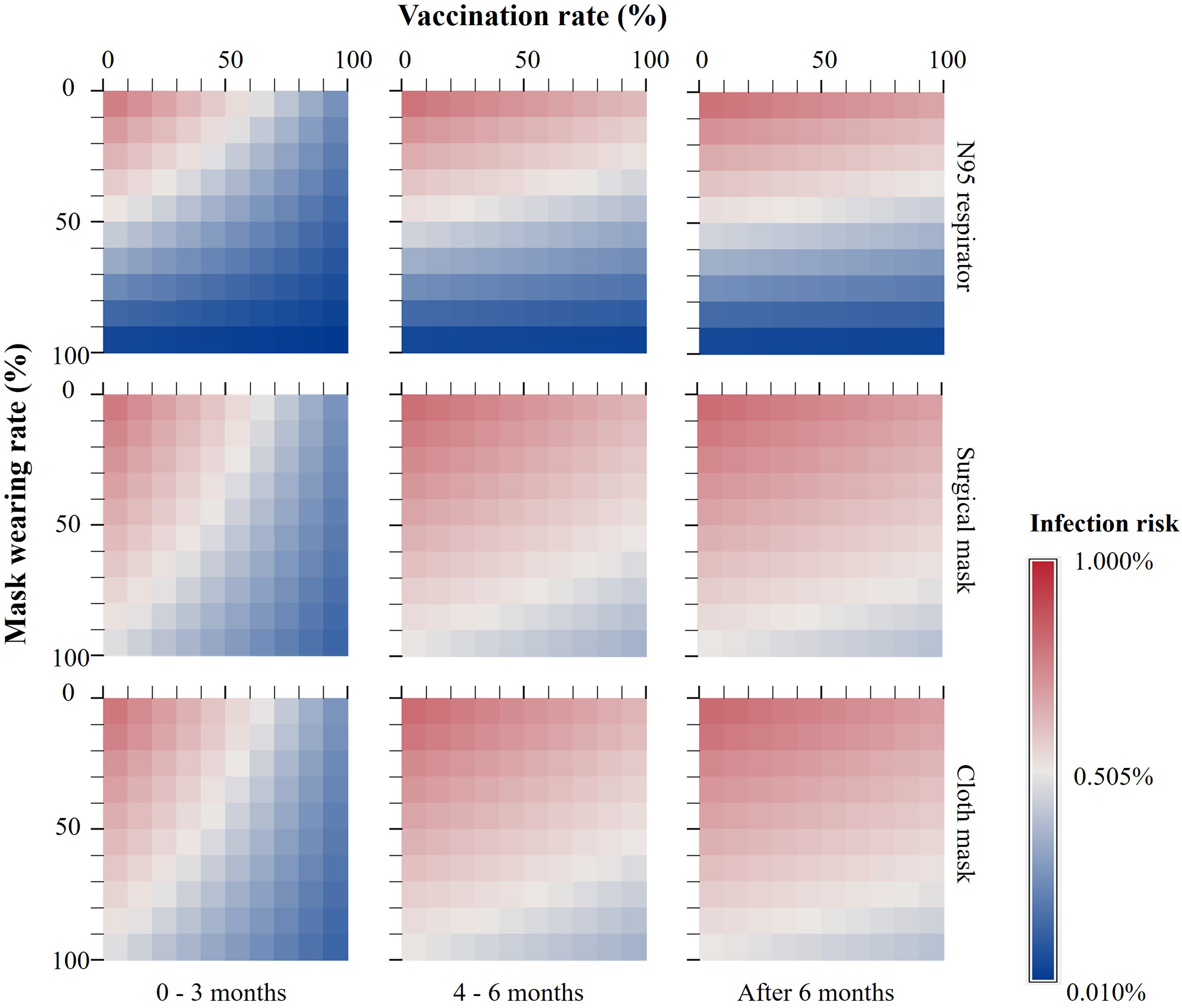
In scenarios where students consistently wore cloth masks, surgical masks or N95 respirators in indoor environments (excluding catering places) during university closures, the reduction in infection risk was 49.5%, 41.6% and 40.9%, respectively, when compared with the non-closure period (Figure 6(a)). Similarly, students’ daily infection risk via close contact fell by an average of 38.4% when interpersonal distances of at least 0.5 m, 1.0 m and 1.5 m, respectively (Figure 6(b)), or was reduced by an average of 38.9% when university students completed basal immunity within 3 months, 4–6 months, or after 6 months, respectively (Figure 6(c)). When students received a vaccine booster every 3 months and consistently wore N95 respirators during the non-closure period, their infection risk was 1/44 compared with the scenario where universities were locked down without any personal protections (Figure 7). During non-closure and university closure periods, daily infection risk for university students when (a) wearing masks (fitted N95 respirators/surgical masks/cloth masks without a filter layer) in a given indoor environment and (b) interpersonal distance was maintained at least at a certain level (0.5 m/1.0 m/1.5 m) in a given indoor environment; and (c) the changes of the time (0–3 months/4–6 months/after 6 months) for which basal immunity against COVID-19 was completed on infection risk in various indoor environments (for resident students, residences are referred to dormitories; for non-resident students, residences are referred to homes. ‘All places’ were considered cumulative infection risk for students across various indoor environments throughout the day. Considering it is impossible to wear masks in the catering space for a long time, ‘All places’ in (a) did not include the catering place). Variation in infection risk for different completion times of basal immunity and mask wearing during the non-closure period.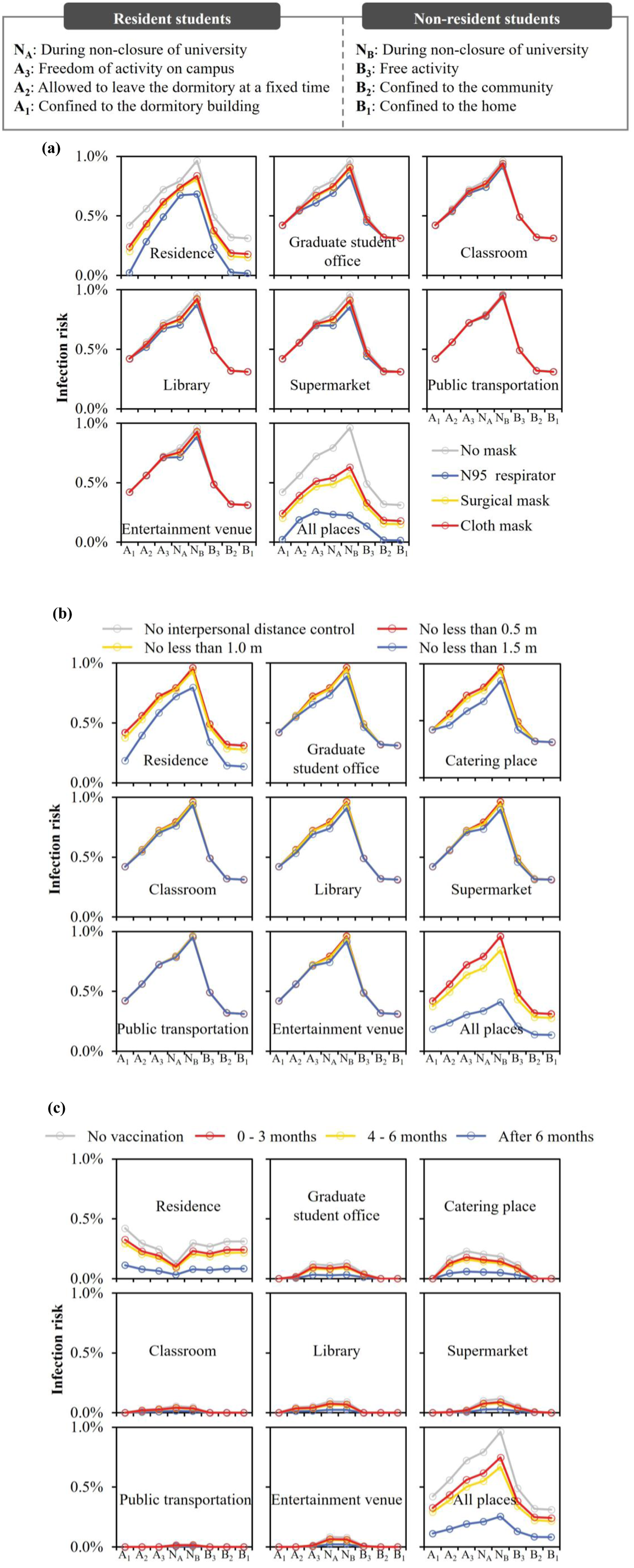
Discussion
During the COVID-19 pandemic, universities and communities implemented interventions of different intensities in response to the severity of local transmission. However, assessments of the impact of the university-closure-related intervention on infection risk for students via the close contact route are lacking. This study collected close contact data of university students during periods of non-closures and university closures with different intervention intensities through both device detection and online surveys. We quantified the infection risk via close contacts. Taking the Omicron variant as an example, we further assessed the impact of personal protections (e.g. wearing masks, maintaining interpersonal distancing and vaccination) on the infection risk for university students. The research aimed to provide scientific and targeted support for infectious disease prevention and control in universities.
Various factors influence human contact behaviour, including gender, age and educational background. Social distancing between males tends to be longer than those between females or between individuals of opposite genders. 26 Students tend to have more contacts than the elderly. 7 Our study observed that undergraduate students experienced the longest close contact time (1.9 h) in classrooms while postgraduate students spent their close contact time (2.2 h) in office spaces longer. This was caused by the fact that postgraduate students generally have fixed workstations. 27 Shifts in the environment also had an influence on contact behaviour. For instance, during the non-closure period, students can freely choose indoor environments they prefer. However, university closures significantly altered students’ staying habits in three main ways. Firstly, changes in how frequently they stayed in specific indoor environments were corroborated by studies focused on restaurants, libraries and public transportation.7,28,29 Secondly, variations in the number of contacts and duration were noted. 7 Specifically, during the COVID-19 pandemic, there was an 83.0% decline in students’ close contacts. Lastly, the close contact rate also fluctuated, influencing indoor close contact time. The changes in staying habits were elucidated from both social and psychological perspectives. On one hand, during severe outbreaks of the pandemic, the government, communities or schools might take interventions to mitigate the spread of COVID-19 by limiting or shutting down areas with high footfall or enclosed public spaces.2,30 On the other hand, students’ risk perception towards the COVID-19 pandemic had profoundly impacted their behavioural patterns. 31
The infection risk of university students was directly influenced by their surroundings and their behaviours. When personal protective measures were not considered, non-resident students recorded a 1.2 times higher infection risk than resident students during non-closures. However, during university closures, the risk for non-resident students fell to 5/9 that of resident students. In addition, non-resident students showed a more positive learning attitude and mood during the pandemic. 32 Hence, encouraging students to return home during the pandemic was a judicious decision. During the COVID-19 pandemic, restaurants were often the hotspots for viral transmission.33–35 However, there is currently no direct evidence supporting university policymakers in enforcing policies prohibiting students from dining in restaurants. This study illustrated that restaurants could constitute the main environment for virus exposure amongst university students, thus offering direct evidence in favour of such policy implementation. This study has also contributed to filling the current research gap regarding the impact of various intervention intensities on students’ infection risk during university closures. It offers a scientific basis for policymakers to make informed decisions.
This study analysed the infection risk of university students via close contacts under different intervention intensities. Amongst the limitations of this study, some are as follows: (1) This work did not account for factors like major, race, height, obesity and posture, which might influence the infection risk of close contact amongst students.36–38(2) This study primarily focused on the close contact transmission of SARS-CoV-2, overlooking other potential routes like the long-range airborne or faecal-oral transmission.39–41 (3) Given that the surveys were predominantly distributed in Beijing and Shanghai, it might not comprehensively capture the policies implemented or behavioural patterns of students in other parts of China. (4) The close contact behaviours were mainly based on self-reports by students, which may introduce subjective biases.
Conclusions
In summary, residences and catering areas were the main virus exposure environments. Resident students experienced a 30.0% reduction in infection risk and 63.6% for non-residents during university closures compared with non-closures. Implementing stringent personal interventions was proven as effective as university closures. The findings could provide scientific support for intervention policy-making during public health emergencies such as COVID-19 pandemic.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 52108067).
Author statements
Data Availability Statement
The data used in this study may be accessed by contacting the corresponding author.