
Abstract
Growing numbers of lowlanders are travelling to high altitudes for occupational and recreational purposes. Hypoxia constitutes the principal physiological challenge at high altitudes, causing notable discomfort and potential life-threatening conditions. This study systematically analysed three key physiological systems during short-term high-altitude exposure and identified the most clinically relevant indicators for these systems. Six Acute Mountain Sickness (AMS) scales were summarized from a subjective monitoring perspective. Three hypoxia alleviation methods with practical implementation guidelines are presented. Based on identified limitations in current evaluation and intervention methods, we propose future research directions to improve safety protocols for high-altitude visitors and to optimize acclimatization strategies. The relevant indicators for three key physiological systems were selected. The key symptoms of six AMS questionnaires were analysed. Three methods of alleviating hypoxia are summarized. Development of an oxygen comfort assessment method is essential for mild AMS. Thermal-oxygen coupled environment control technology is prospective.
Keywords
Introduction
With the development of society and the construction of railways, more lowlanders are exposed to high altitudes for activities, such as mountain tourism, high–altitude industries (e.g., mining) and soldiers. High altitude terms as locations higher than 2500 m above sea level. Many physiological responses of the human body start notably developing above 2500 m. 1 High-altitude regions exhibit extreme environmental conditions characterized by hypobaric hypoxia, cold temperatures, large daily temperature swings, intense UV radiation, low humidity and strong winds. Hypoxia is the primary health challenge, negatively impacting multiple physiological systems, including neurological, respiratory, sensory, haematological, digestive and musculoskeletal functions. 2 Physiological strain caused by hypoxia impairs normal functioning and reduces work efficiency. 3 Severe cases may occur acute high-altitude illness (AHAI), 4 the characteristics of acute mountain sickness (AMS), high-altitude pulmonary oedema (HAPE) and high-altitude cerebral oedema (HACE) are outlined in Table 1. AMS typically occurs within 4–24 h after ascent to altitudes above 2500 m. The symptoms usually resolve without the need for descent. However, individuals who persist with AMS symptoms or experience fatigue, susceptibility to cold exposure and upper respiratory tract infections, resulting in more severe AHAI, such as HAPE and HACE. Consequently, ‘people short-term exposed to high altitude’ have been the focus of concern and consideration.
Descriptions of acute high-altitude illness.

This research spans multiple disciplines, including medicine, exercise physiology, civil engineering and Heating, Ventilation and Air Conditioning (HVAC). Medical research investigates the effects of hypoxia, oxygen enrichment. 10 and pharmacological interventions. 7 through changes in physiological parameters.11–13 and cognitive performance, 14 and even delves into the cellular and genetic mechanisms.15,16 Exercise physiology studies demonstrate that athletic performance can be enhanced by hypoxia. 17 Civil engineering research examines oxygen diffusion dynamics in tunnel environments. 18 HVAC research focuses on developing oxygen-enriched indoor environments to enhance high-altitude comfort. 19 While high-altitude research traditionally focused on medical and exercise physiology, interdisciplinary approaches have recently gained prominence. Given hypoxia's systemic effects, these studies inherently integrate medical science perspectives. Thus, this study synthesizes medical evidence to systematically summarize the high-altitude exposure effect.
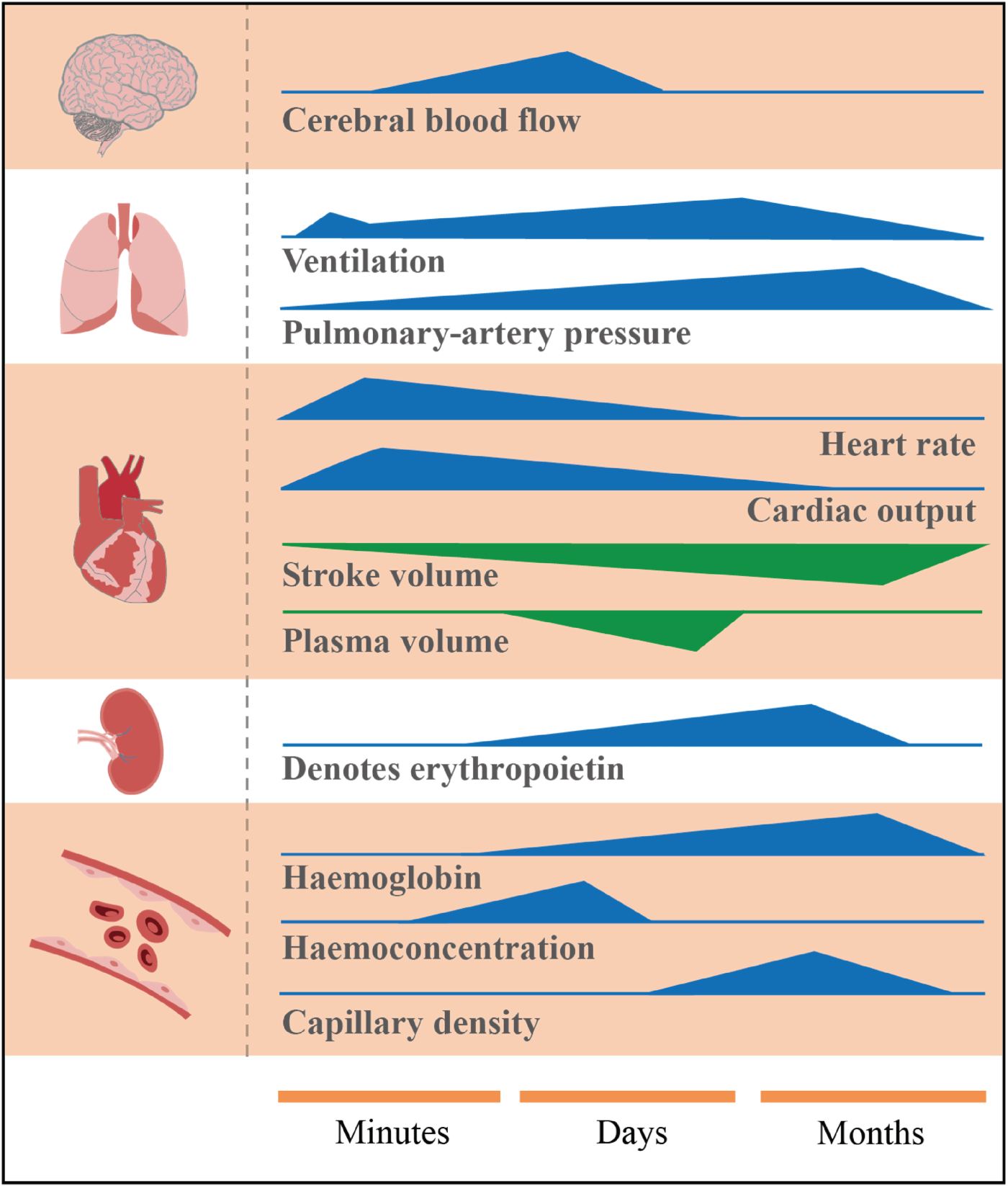
Current literature shows substantial variation in defining hypoxia exposure duration, ranging from acute to chronic conditions, resulting in heterogeneity in reported responses (Figure 1). Lowlanders typically experience acute exposure lasting days to weeks during high-altitude sojourns. Although Burtscher et al. 21 define acute exposure as the initial phase of hypoxia exposure with the most pronounced (patho)physiological responses (duration from minutes to days), this diverges from observed real-world scenarios. Thus, this study adopts the definition of Song et al. 22 for ‘short-term exposure’ (i.e., lowlanders staying at high altitudes for below 3 months). This study systematically investigated physiological mechanisms during short-term hypoxia exposure, evaluated subjective assessment tools and synthesized current effective hypoxia alleviation methods. It aimed to provide practical guidance for short-term high-altitude exposure and scientific insights for optimizing high-altitude adaptation strategies.
Literature search strategy
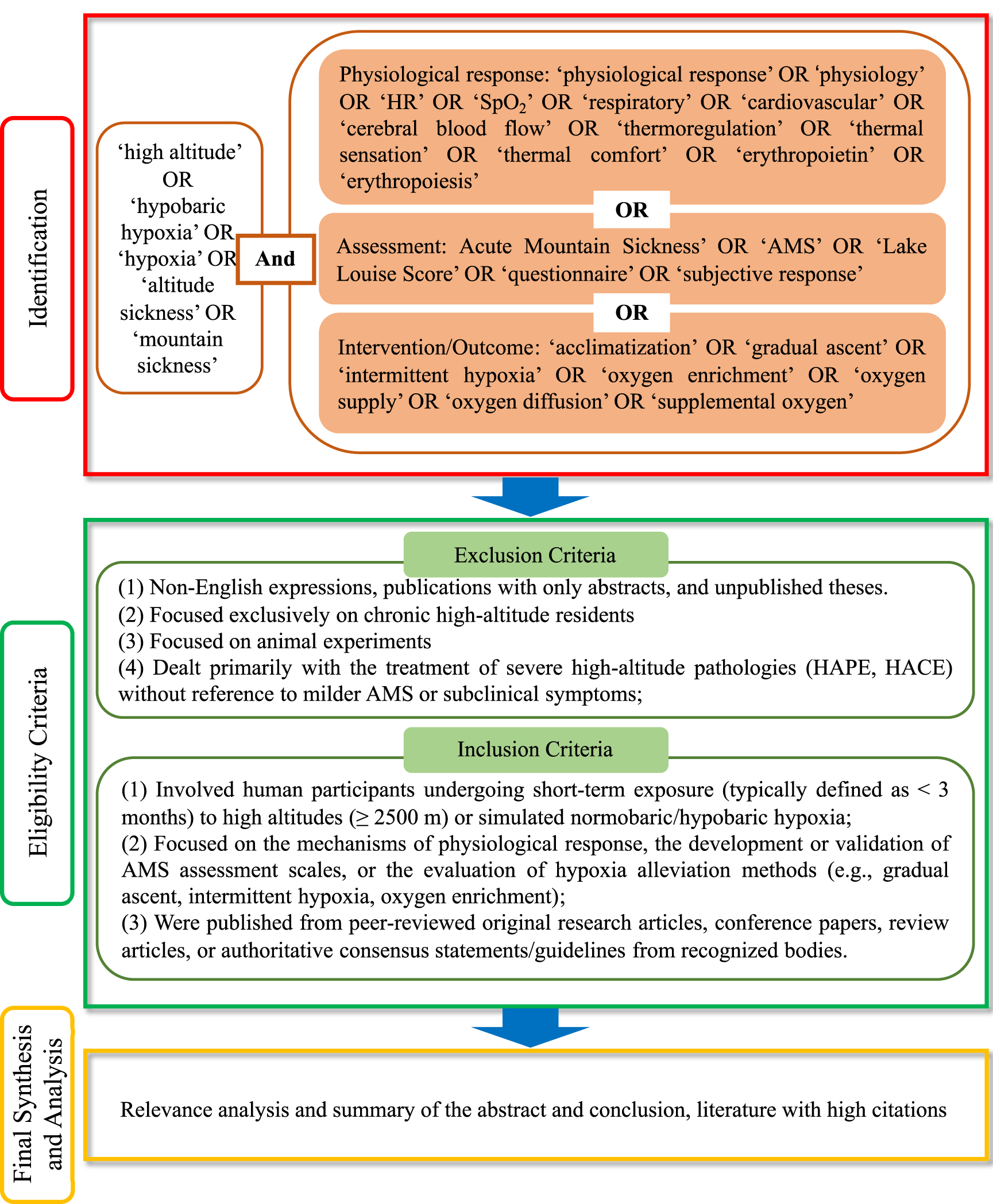
A systematic literature search was conducted to identify publications relevant to physiological responses, subjective assessment methods and alleviative methods for short-term high-altitude exposure in humans. The search was performed using electronic databases including Springer Link, Elsevier (Science Direct) and Web of Science, covering the fields of medicine, physiology, sports science and environmental engineering. The search was limited to articles published between 1950 and 2023. The search strategy, illustrated in Figure 2, was structured around three primary themes: ‘Physiological responses’, ‘Assessment’ and ‘Intervention/Outcome’. The specific search syntax was adapted to the rules of each database, using Boolean operators (AND, OR) to combine these concepts effectively. Subsequently, all retrieved articles underwent an initial screening based on eligibility criteria. Following this, the full texts of articles were carefully evaluated to select those with high relevance and significant citation impact for in-depth review.
Search and selection process of literature publications.
Systemic physiological responses and monitoring indicators during short-term high-altitude exposure
Physiological indicators represent critical biomarkers for assessing systemic functions and health status. The selection of appropriate physiological indicators is essential for monitoring hypoxic exposure in lowlanders and ensuring safety during high-altitude exposure. As depicted in Figure 1, predominant responses vary across different phases of high-altitude exposure. Therefore, we analysed the physiological systems during short-term exposure and identified key monitoring indicators for each system, as listed in Table 2 (spanning systemic to cellular levels).
The key monitoring indicators for the physiological system.
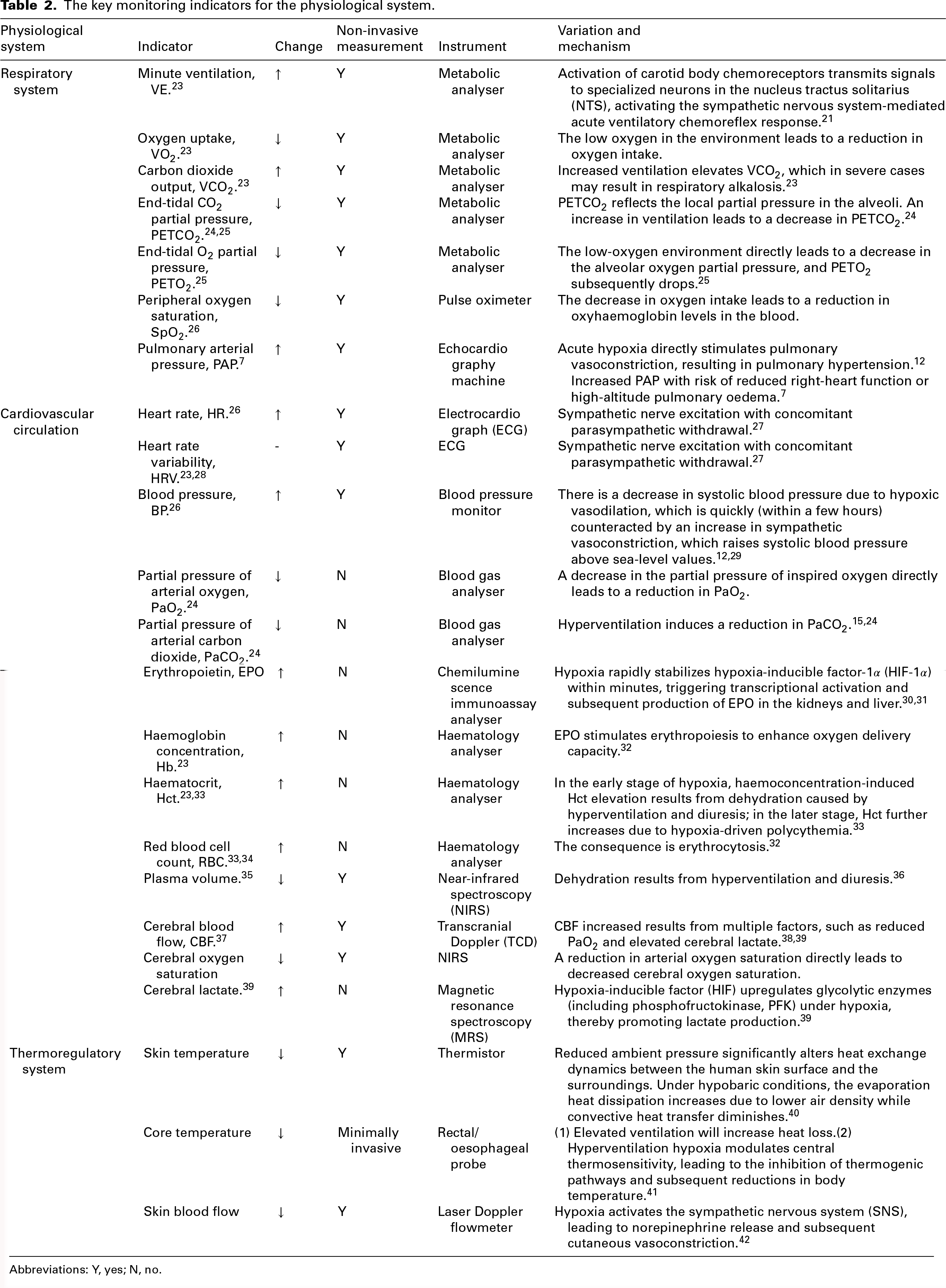
Abbreviations: Y, yes; N, no.
Respiratory system
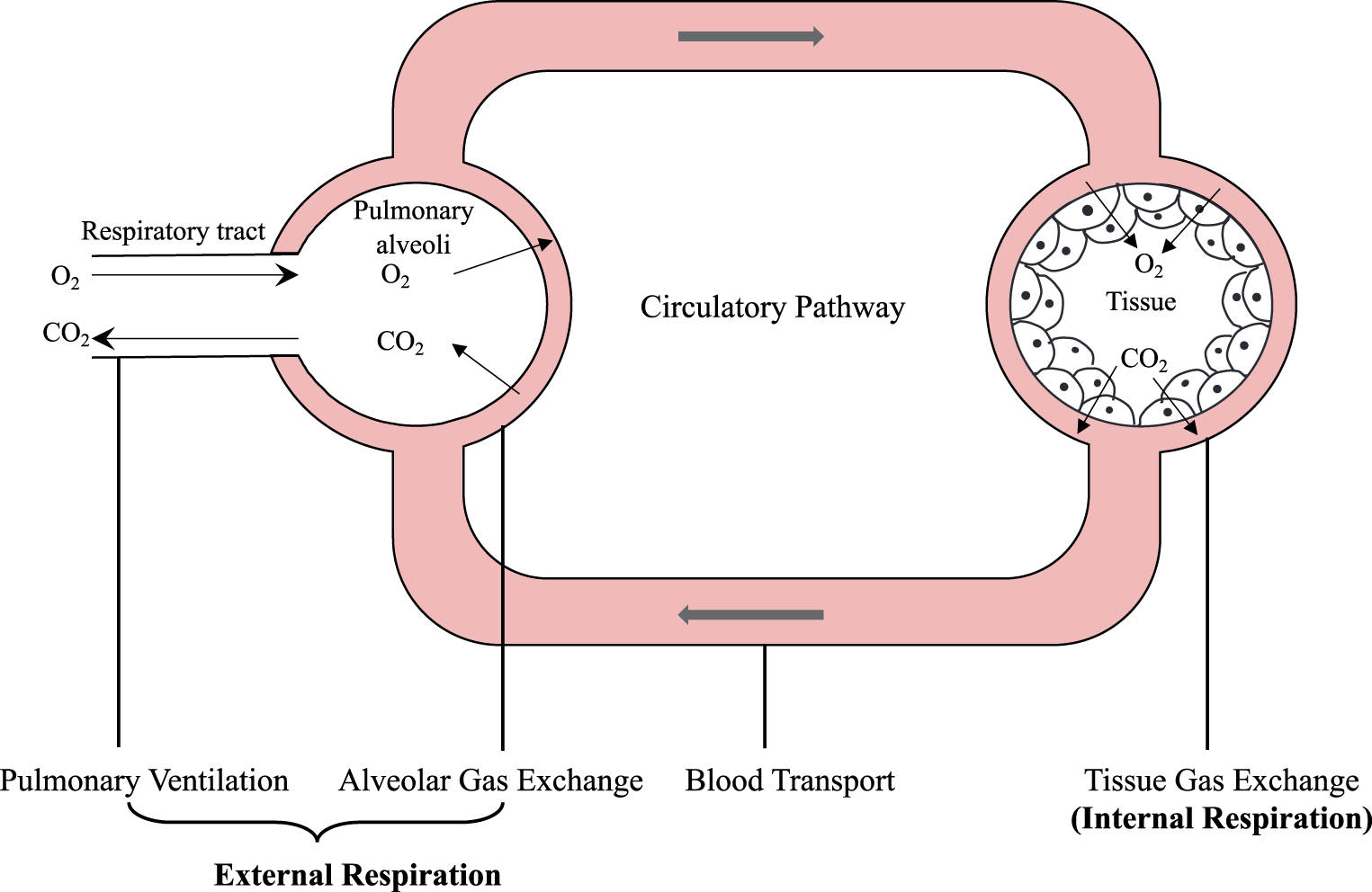
Respiration is a fundamental physiological process essential for sustaining normal bodily activities. The respiratory process comprises three interrelated and concurrent phases: external respiration, blood gas transport and internal respiration, as illustrated in Figure 3. During external respiration, gases diffuse through the respiratory tract and undergo gas exchange with the blood in the alveoli. Oxygenated blood subsequently perfuses tissues via systemic circulation. Internal respiration entails tissue-level gas exchange between capillaries and cells. These gas exchange processes are primarily driven by partial pressure gradients.
Schematic diagram of the respiratory process.
When environmental oxygen is reduced, intake of oxygen by the body decreases, resulting in a decrease in the partial pressure of alveolar oxygen (PAO2). This PAO2 reduction diminishes the oxygen partial pressure gradient between the alveoli and pulmonary capillaries, thereby impeding oxygen diffusion. Consequently, blood oxygen content in pulmonary capillaries decreases, leading to the partial pressure of arterial oxygen (PaO2). This process alters the affinity of haemoglobin for oxygen, ultimately resulting in decreased oxygen saturation and inducing hypoxic symptoms. Figure 4 illustrates the atmospheric and partial oxygen pressures at various altitudes. 43 To address the hypoxic condition, the human body has compensatory mechanisms. Carotid and aortic chemoreceptors of humans are activated by hypoxia, stimulating the respiratory centre to increase ventilation (hypoxic ventilatory response, HVR). HVR recruits previously non-ventilated alveoli, increasing the respiratory surface area and optimizing oxygen distribution. 2 This mechanism enhances alveolar gas exchange by increasing fresh air inflow. HVR also increases thoracic activity, enhances the negative pressure within the thoracic cavity, augments venous return, and promotes pulmonary blood flow as well as cardiac output. 2 Notably, hyperventilation decreases partial pressure of arterial carbon dioxide (PaCO2), resulting in respiratory alkalosis. This prompts the kidneys to induce a compensatory metabolic acidosis through acid retention and increased bicarbonate (HCO3−) excretion in urine. 24 Moreover, hyperventilation contributes to fluid loss in the respiratory system, potentially resulting in dehydration. 36 and haemoconcentration.
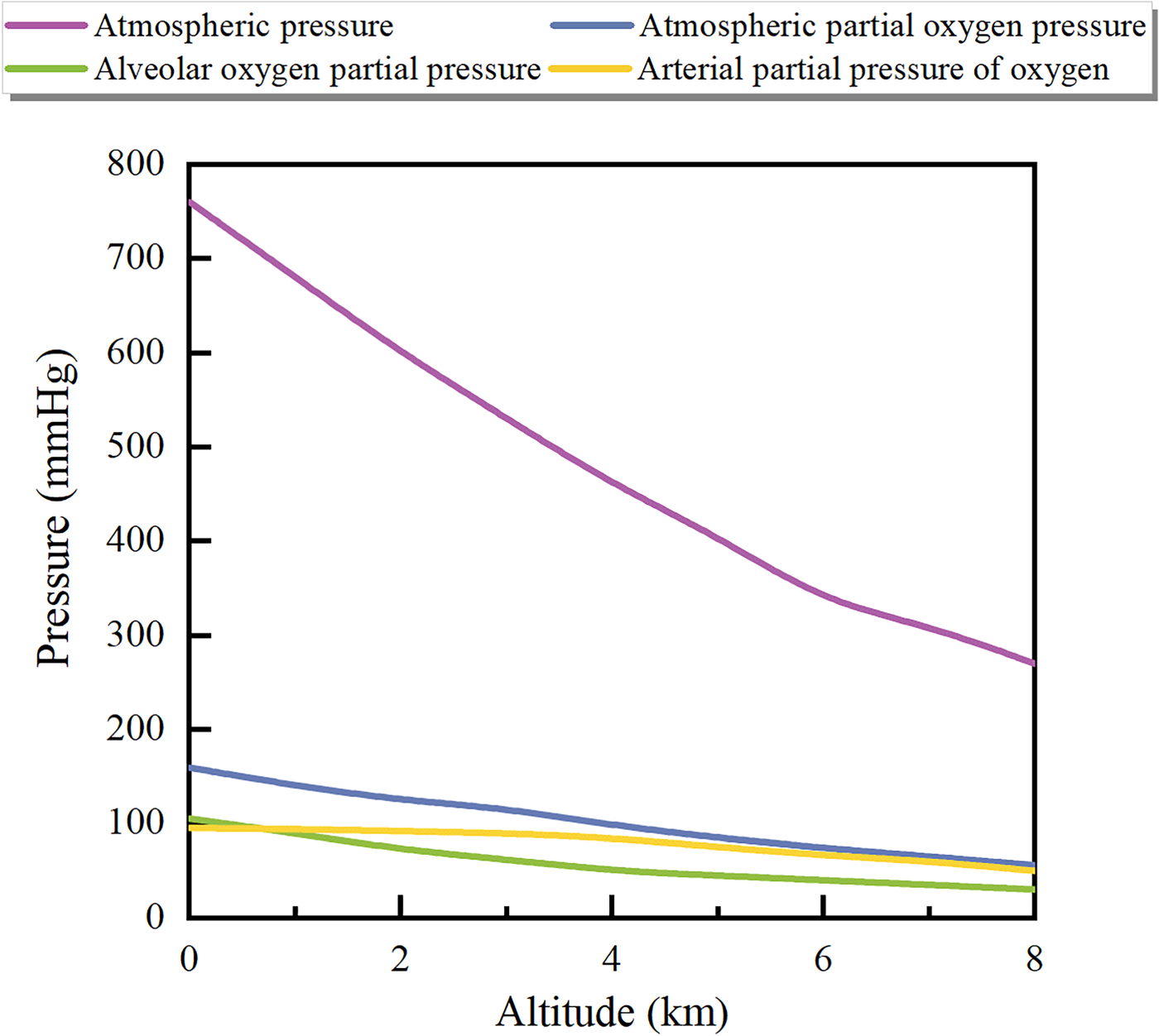
Atmospheric pressure and partial oxygen pressure at different altitudes (replotted from Liu. 23 )
Cardiovascular system
The cardiovascular system comprises the heart, arteries, capillaries and veins. As the central pump, the heart propels oxygenated blood through arteries to capillary networks. Within the capillaries, exchange of nutrients and gases occurs between the blood and tissue cells. The capillaries subsequently merge to form veins, which return to the heart. 44
When environmental oxygen decreases, the cardiovascular system initiates compensatory mechanisms. These mechanisms maintain consistent oxygen delivery to tissues by increased cardiac output. 45 Cardiac output (CO) depends on stroke volume (SV) and heart rate (HR). During short-term exposure to high altitudes, CO initially increases due to elevated HR without SV changes. 46 HR elevation reflects sympathetic nervous system activation. The sympathetic nervous system is excited through the central effect of the hypoxia and partly reflexes, through stimulation of chemoreceptors and possibly pulmonary arterial baroreceptors, and altered systemic baroreceptor function. 11 Sympathetic activation also increases blood pressure. 29 This masks the decrease in blood pressure that results from the endothelium-dependent and non-endothelium-dependent systemic vasodilation during subacute exposure to hypoxia,1,12 as presented in Figure 5. This figure illustrates that system and pulmonary circulation changes during acute hypoxia, as summarized by Parati et al. 1 With prolonged acclimatization, CO normalizes to the resting level observed in high-altitude natives, accompanied by persistent HR elevation and SV reduction. Furthermore, hypoxia rapidly stabilizes hypoxia-inducible factor-1α (HIF-1α) within minutes, triggering transcriptional activation and subsequent production of erythropoietin (EPO) in the kidneys and liver.30,31 Knaupp et al. 47 demonstrated that continuous hypoxia exposure lasting 84–120 min leads to a sustained serum EPO elevation. The glycoprotein hormone EPO enhances oxygen delivery capacity via erythropoiesis stimulation.32,33 HIF-1 also mediates the upregulation of vascular endothelial growth factor (VEGF), thereby promoting angiogenesis. 48
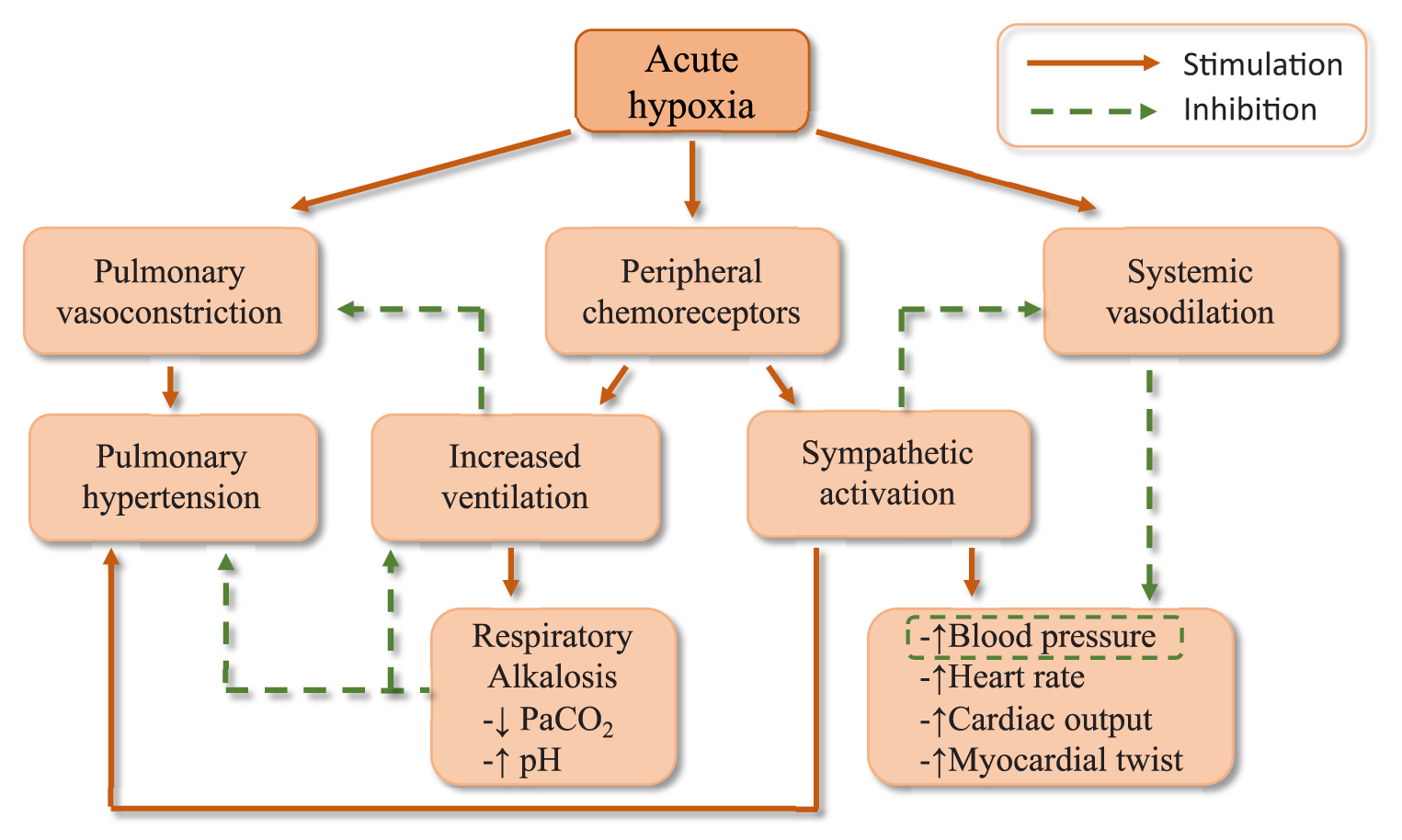
Effects of acute hypoxia on the system and pulmonary circulation (modified from Parati et al. 1 ). PaCO2, partial pressure of arterial carbon dioxide.
As one of the core functions of the cardiovascular system, cerebral blood flow (CBF) delivers nutrients and oxygen to the brain, as well as eliminates cellular metabolic products and toxic by-products through precise regulatory mechanisms. 38 This is crucial for the brain, which exhibits high metabolic rates and limited energy storage capacity.
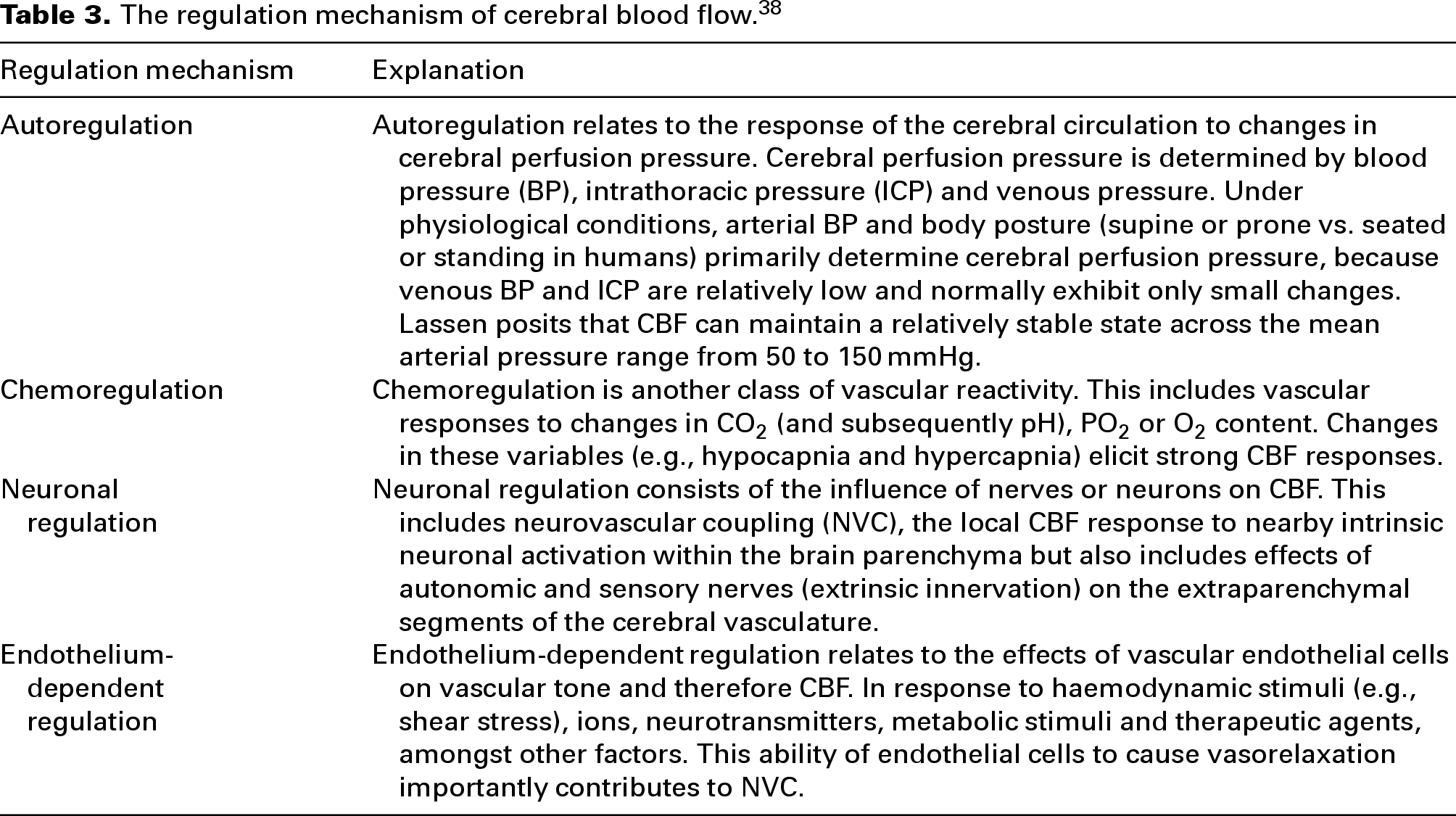
The regulation of CBF is a multifaceted process affecting pulmonary gas exchange and cardiovascular function, in addition to mediating intracranial cerebrovascular resistance. Therefore, a comprehensive understanding of CBF regulation remains challenging. The intricacies of human CBF regulation have been extensively discussed in the literature.38,49,50 Claassen et al. 38 simplified CBF regulation by dividing the mechanism regulating CBF into four different components or adaptive responses, as illustrated in Table 3. These regulatory mechanisms exhibit substantial interactions and functional overlap.
The regulation mechanism of cerebral blood flow. 38
The mammalian brain depends entirely on oxygen for the synthesis of adenosine triphosphate (ATP), making it particularly susceptible to hypoxia. Meanwhile, the brain accounts for approximately 20% of total resting oxygen consumption, establishing it as the highest oxygen-demand organ. 51 Therefore, reduced environmental oxygen rapidly affects the brain, particularly evident in CBF changes. Hypoxia modulates CBF through the aforementioned four regulatory mechanisms.
As detailed previously, hypoxia notably influences the BP, PaO2 and PaCO2. Thus, hypoxia impacts CBF through the respiratory and cardiovascular systems, mediated by autoregulation and chemoregulation. Autoregulation maintains relatively stable CBF across the mean arterial pressure of 50–150 mmHg. Chemoregulation activates when the PaO2 falls below approximately 50 mmHg (corresponding to SaO2 ∼ 80%), inducing vasodilation. 49 This response also depends on the prevailing PaCO2 levels. Hyperventilation reduces PaCO2, increasing cerebral vascular resistance and decreasing CBF. Specifically, each 1 mmHg reduction in PaCO2 decreases CBF by 1–3%.38,49 In addition, the endothelium-dependent regulation significantly influences CBF through vascular endothelial factors. 48 Neuronal regulation also plays a significant role including: (1) neurovascular coupling involves retrograde signalling from neurons and glial cells responding to local tissue hypoxia; and (2) the occurrence of brain extracellular acidosis resulting from heightened anaerobic metabolism in neurons and glial cells, which subsequently induces vascular dilation. 49 The impact of hypoxia on the human body is notably intricate. While hypoxia affects CBF through multiple pathways, detailed mechanistic analysis is beyond the scope of this article.
Thermoregulatory system
Most hypoxia research focuses on the pathological implications of the human body. Since the effect of hypoxia on body temperature minimally impacts human daily life, it has received limited research consideration. However, there are still some scholars who attempt to clarify the effect of hypoxia on thermoregulation under thermal comfort, but findings remain inconsistent. Ciuha et al. 52 observed that hypoxia did not alter rectal or mean skin temperature during bed rest, nor did it affect the thermal comfort zone. Similarly, Golja et al. 53 reported no significant effect of hypoxia on eardrum temperature or the human comfort zone. Conversely, Duan et al. 54 found that decreasing oxygen levels reduced mean skin temperature, particularly under colder ambient conditions. Beyond whole skin temperature, certain researchers have examined the effects of hypoxia on local skin temperature. Golja et al. 55 noted that hypoxia reduced cold sensitivity in the toes while leaving warmth perception unchanged. They suggested that this altered thermal perception might impair thermoregulatory behaviour during cold exposure at high altitudes. Supporting this, Keramidas et al. 56 proposed that hypoxia tends to blunt the sensation of coldness and thermal discomfort.
The precise mechanisms by which hypoxia on thermoregulation remain unclear, complicating the interpretation of physiological changes. Hypoxia affects the thermoregulatory system in multiple ways, ultimately altering heat dissipation, heat production and body temperature. Hypoxia increases respiratory heat loss by hyperventilation. As heat dissipation rises, heat production may decline, as supported by several animal studies. Specifically, the inhibition of brown adipose tissue (BAT) sympathetic nerve activity (SNA) triggered by peripheral chemoreceptor activation directly contributes to (or is permissive for) hypoxia-induced reductions in body temperature and oxygen consumption. 57 Hypoxia also modulates central thermosensitivity, leading to the inhibition of thermogenic pathways and subsequent decreases in body temperature. 41 From a thermodynamic perspective, reduced ambient pressure significantly alters heat exchange dynamics between the human skin surface and surroundings. Under hypobaric conditions, the evaporation heat dissipation increases due to lower air density while convective heat transfer decreases. 40 These modifications have a substantial impact on thermoregulation and thermal perception.
In summary, although the effect of hypoxia on thermal comfort remains debated, biomedical evidence suggests that hypoxia potentially modulates thermoregulation. Therefore, systematic monitoring of thermoregulatory parameters is needed to clarify the mechanistic pathways of hypoxia.
Questionnaires for the measurement of AMS
Individuals may develop various hypoxic symptoms after exposing to high-altitude environments. In severe cases, AHAI (e.g., HAPE and HACE) can pose a life-threatening risk (as presented in Table 1), underscoring the importance of assessing the condition of lowlanders at high altitudes. Physiological parameters provide objective evaluations of hypoxic stress, but their practical application is limited and cannot accurately assess subjective symptoms such as headache, anorexia and nausea. Consequently, low-cost, immediate-use subjective questionnaires for assessing AMS have been extensively investigated.
AMS assessment scales
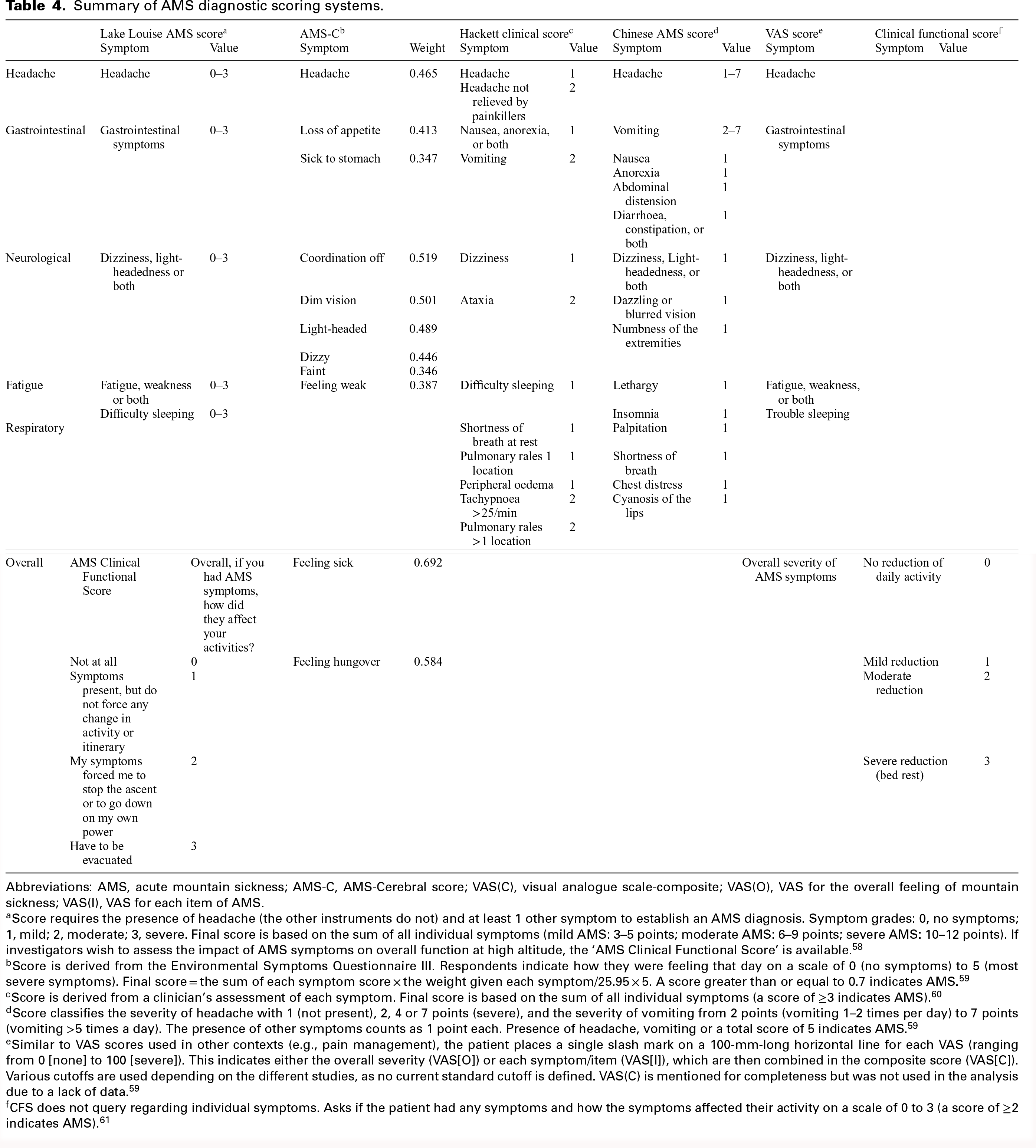
The diagnosis of AMS primarily relies on questionnaires. Six predominant assessment scales are widely used in global clinical and research settings. Table 4 summarizes these scales and respective scoring criteria. The most frequently used scales include the Lake Louise AMS Score (LLS), AMS-Cerebral score (AMS-C) and Hackett clinical score. These instruments evolved from the Environmental Symptoms Questionnaire III score. They assess symptoms through either summation or the weighted averaging methods. The Chinese AMS score (CAS) is also evaluated based on symptoms. The Visual Analogue Scale (VAS(O)) provides a continuous metric for quantifying overall disease severity. This continuous scale minimizes variations in textual interpretation by eliminating categorical thresholds. 59 The Clinical Function Score (CFS) represents the most straightforward tool, utilizing a single uncomplicated question. Amongst them, the LLS is globally recognized as an extensively quantitative benchmark. Some researchers compared the accuracy of other questionnaires with LLS. Meier et al. 62 demonstrated that the VAS(O), AMS-C and CFS exhibited comparable diagnostic accuracy to the LLS for identifying moderate to severe AMS (LLS ≥ 5). The positive likelihood ratios for these measures ranged from 3.2 to 8.2, with specificities between 67% and 92%. Wu et al. 63 reported that the positive rate of AMS identified through the CAS exceeded that determined by the LLS. The ROC curve analysis indicated that the sensitivity and specificity of CAS at the optimal cut-off value of 3.5 points were 76.5% and 90.2%, respectively, demonstrating its efficacy in accurately diagnosing AMS. However, the relatively small sample size limits its generalizability and international adoption. The Hackett clinical score exhibits similar characteristics. 62
Summary of AMS diagnostic scoring systems.
Abbreviations: AMS, acute mountain sickness; AMS-C, AMS-Cerebral score; VAS(C), visual analogue scale-composite; VAS(O), VAS for the overall feeling of mountain sickness; VAS(I), VAS for each item of AMS.
Score requires the presence of headache (the other instruments do not) and at least 1 other symptom to establish an AMS diagnosis. Symptom grades: 0, no symptoms; 1, mild; 2, moderate; 3, severe. Final score is based on the sum of all individual symptoms (mild AMS: 3–5 points; moderate AMS: 6–9 points; severe AMS: 10–12 points). If investigators wish to assess the impact of AMS symptoms on overall function at high altitude, the ‘AMS Clinical Functional Score’ is available. 58
Score is derived from the Environmental Symptoms Questionnaire III. Respondents indicate how they were feeling that day on a scale of 0 (no symptoms) to 5 (most severe symptoms). Final score = the sum of each symptom score × the weight given each symptom/25.95 × 5. A score greater than or equal to 0.7 indicates AMS. 59
Score is derived from a clinician's assessment of each symptom. Final score is based on the sum of all individual symptoms (a score of ≥3 indicates AMS). 60
Score classifies the severity of headache with 1 (not present), 2, 4 or 7 points (severe), and the severity of vomiting from 2 points (vomiting 1–2 times per day) to 7 points (vomiting >5 times a day). The presence of other symptoms counts as 1 point each. Presence of headache, vomiting or a total score of 5 indicates AMS. 59
Similar to VAS scores used in other contexts (e.g., pain management), the patient places a single slash mark on a 100-mm-long horizontal line for each VAS (ranging from 0 [none] to 100 [severe]). This indicates either the overall severity (VAS[O]) or each symptom/item (VAS[I]), which are then combined in the composite score (VAS[C]). Various cutoffs are used depending on the different studies, as no current standard cutoff is defined. VAS(C) is mentioned for completeness but was not used in the analysis due to a lack of data. 59
CFS does not query regarding individual symptoms. Asks if the patient had any symptoms and how the symptoms affected their activity on a scale of 0 to 3 (a score of ≥2 indicates AMS). 61
Assessment of short-term exposure to AMS
Current AMS assessment protocols (Table 4) primarily target severe symptom management and pathological prevention, emphasizing medical safety. However, non-severe cases need attention. Empirical studies revealed that at altitudes of 3000 m, 3600 m. 64 and 4400 m, 65 the combined prevalence of mild AMS and asymptomatic reactions reached 81.42%, 75.26% and 71.18%, respectively. These data indicate that mild AMS or subclinical hypoxic responses affect larger populations than moderate/severe AMS. Although seldom requiring medical intervention, these individuals experience discomfort that significantly impairs quality of life.
With increasing human activity in high altitudes, 54 environmental demands have transformed from survival thresholds to comfort optimization. Consequently, oxygen comfort has become a critical factor for high-altitude sojourners. Standard AMS assessment protocols lack sensitivity for mild symptoms or subtle discomfort gradation. To address this limitation, researchers have adopted 5- or 7-point scales from ISO 10551 . 66 to differentiate overall perceptions, such as oxygen sensation, comfort and acceptability.54,67,68 Building on this approach, Cao et al. 68 further refined the evaluation by implementing a 5-level grading scale to assess symptoms associated with the respiratory, circulatory, nervous and digestive systems. Nevertheless, these classification systems remain insufficiently intuitive and clear for individuals experiencing hypoxia for the first time. In response, Song et al. 22 pioneered an Oxygen Comfort Evaluation Method (OCEM). This method assesses hypoxic symptoms using both phenomenological descriptors and physiological indicators. The core component is a symptom questionnaire comprising 19 symptom indices, each rated on a five-point scale (None, Mild, Moderate, Heavier and Severe). Crucially, each grade is accompanied by specific behavioural or sensation descriptors, which significantly enhance the accuracy and consistency of subjective reporting by participants. Experimental validation demonstrated a 93% prediction accuracy for oxygen sensation and a strong agreement (weighted kappa = 0.825) for the final comfort level. Compared to LLS, OCEM detected a wider range of discomfort symptoms (76.8% were supplementary symptoms not covered by LLS), showing a stronger ability to identify subtle uncomfortable states related to oxygen comfort. The OCEM offers a novel framework to quantify oxygen sensitivity and guide indoor oxygen regulation in high-altitude buildings. Nevertheless, further empirical validation is required to establish reliability. Currently, there remains a scarcity of research focused on oxygen comfort. We advocate expanded scholarly focus on oxygen comfort to refine assessment methodologies and enhance the high-altitude experiences for short-term sojourners.
Methods of alleviating hypoxia
To ensure the safety of lowlanders exposed to high altitudes, researchers have studied pharmacological interventions, including acetazolamide, dexamethasone and sildenafil for high-altitude illness prevention. 69 Although these medications can alleviate or prevent high-altitude illnesses, they may induce side effects. 70 Therefore, the altitude alleviation methods are the most effective approach for optimizing hypoxic adjustment and maintaining physiological performance. These methods reduce AMS sensitivity, enhance physical performance and facilitate ascent to higher altitudes.71,72 Researchers have leveraged the body's hypoxic acclimation capacity to develop various adaptation strategies.
Gradual ascent
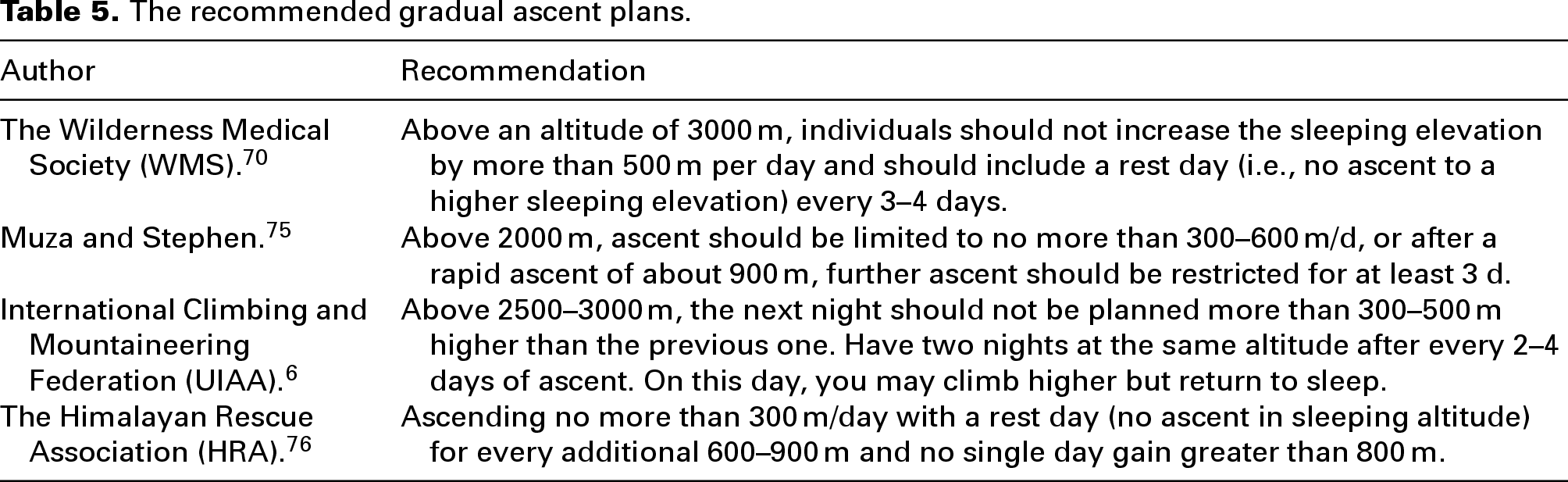
Gradual ascent (GA) refers to taking short breaks every time ascending to a certain altitude to alleviate hypoxia. This strategy is widely used in high-altitude mountaineering. Field studies confirm its effectiveness in reducing AMS incidence and severity73,74 and enhancing exercise performance. 20 Practical application guidelines have been developed across fields, as summarized in Table 5.
The recommended gradual ascent plans.
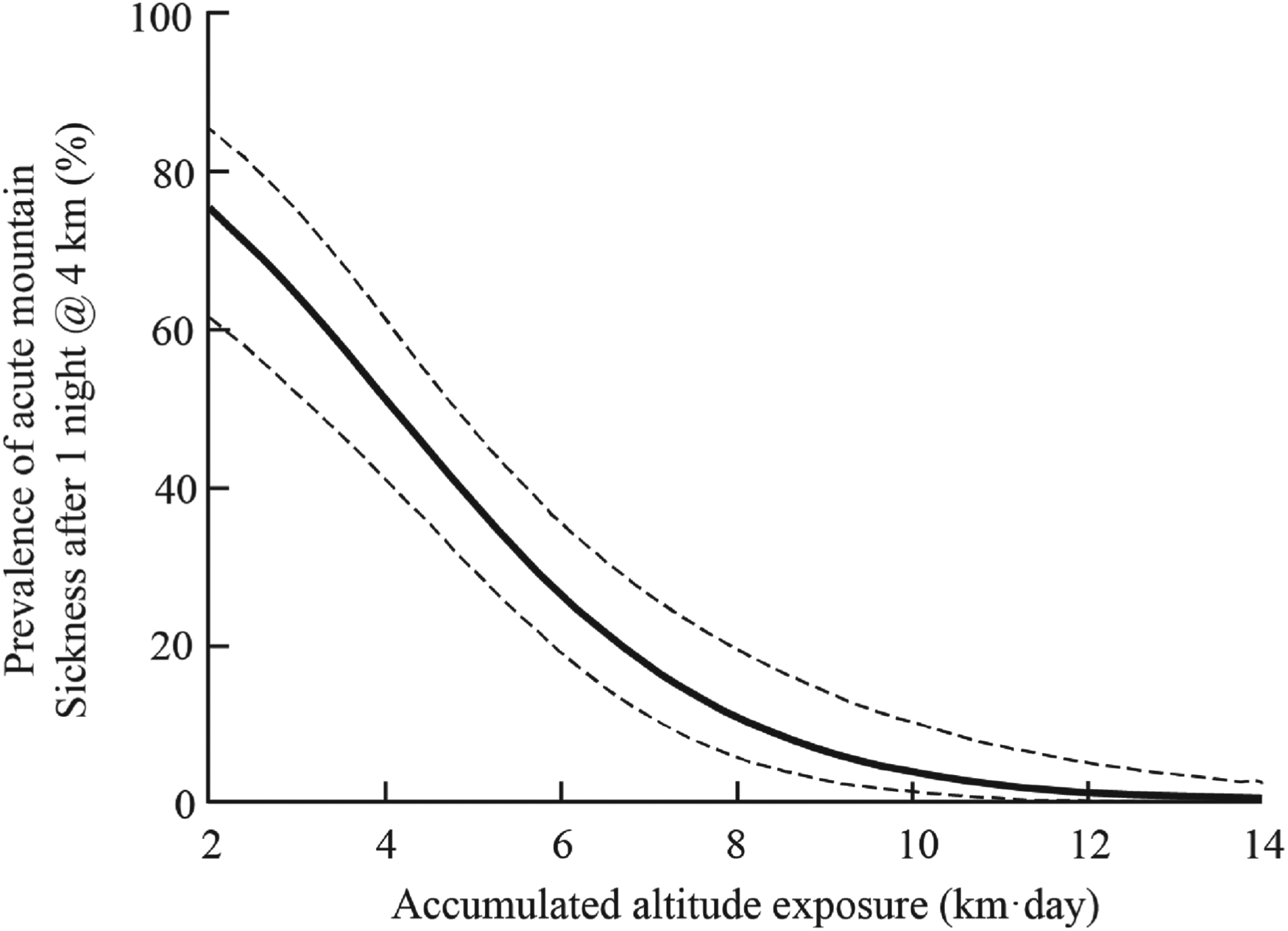
Prolonged rest periods at moderate altitudes (2200–3000 m) during ascent enhance safety through short-term acclimatization. This approach is termed ‘stage ascent’ (SA). 70 Both GA and SA can alleviate the decline of SpO2 and reduce the incidence and severity of AMS. These benefits derive from sufficient time to acclimate for improving ventilation and oxygenation. 77 and reducing PAP associated with HAPE.78,79 However, the recommended GA plans are not consistent, and adhering to these requirements is challenging during actual ascent. The quantitative prediction AMS model established by Beidleman et al. 80 addresses this limitation. This approach calculated accumulated altitude exposure (AAE), which was defined as the ascent profile and was calculated by multiplying the altitude elevation (km) by the number of days (d) at that altitude before ascent to 4 km. It predicted the probability of AMS occurring ∼ 24 h after exposure to an altitude of 4 km. Figure 6 represents the changes in the prevalence of AMS at 4 km following various ascent profiles inducing various AAE (km d). The dotted line indicates the 95% confidence interval of the prediction. Although limited to a target altitude of 4 km, this method integrates the two multilevel factors of altitude increase and duration of stay into a novel indicator, providing a new perspective for future investigations into gradual ascent and holds significant milestone implications.
The quantitative model of altitude acclimatization status (reprinted from Beidleman et al., 80 Copyright (2019), with permission from Wiley).
Intermittent hypoxia exposure
Individuals engaged in activities such as travel, hiking, combat and occupational work often face temporal, financial and logistical constraints in different locations for acclimatization. Intermittent hypoxia (IH) addresses these constraints. 34 IH alleviates adverse effects of prolonged exposure to high altitudes, including immunosuppression, 81 increased oxidative stress, 82 elevated inflammation. 83 and sleep disorders. Therefore, IH is a promising non-pharmacological strategy for acclimatization. Intermittent hypoxic exposure (IHE) is defined as repeated exposure to hypoxia, ranging from seconds to hours per session, administered over several days to weeks. 84 IHE research focuses on three areas: disease treatment and prevention in sleep medicine,85,86 exercise capacity improvement in sports medicine84,87 and altitude acclimatization in mountain medicine. 20
The application of IHE mainly depends on three factors 75 : altitude of exposure, duration of each treatment and total number of IH treatments. Researchers have investigated various IHE protocols, as summarized in Table 6. IHE essentially capitalizes on the body's adaptations to hypoxia. The cardiopulmonary system responds most rapidly, while the haematological system requires longer stimulation periods, as illustrated in Figure 1. Given the constraints of time and resources in pre-acclimatization, high-efficiency strategies with shorter durations are often prioritized. Accordingly, physiological changes in Table 6 primarily emphasize cardiopulmonary and cerebral parameters. However, there has been no universally accepted IH framework. Based on these empirical findings, we propose several recommendations for optimizing IHE protocols in future research. Regarding the altitude of IHE, higher altitudes should be considered. Hypoxic responses intensify with altitude elevation, whereas lower altitudes require prolonged exposure durations for equivalent acclimatization. Katayama et al. 88 and Townsend et al. 96 demonstrated that at similar IHE altitudes, significant acclimatization effects were observed only after an extended duration of IHE. Therefore, increasing the IHE altitude may enhance pre-acclimatization efficiency. However, indiscriminate increases in the altitude of IHE may lead to adverse physiological consequences. Navarrete-Opazo et al. 86 suggested that modest hypoxia (9–16% inspired O2) and low cycle numbers (3–15 episodes per day) most often lead to beneficial effects without pathology, whereas severe hypoxia (2–8% inspired O2) is associated with progressively pathological mechanisms. For the duration of each treatment, Katayama et al. 92 found that equivalent HVR enhancement between 1-h and 3-h continuous IH sessions when other parameters were held constant. Wojan et al. 32 observed that erythropoietin levels reached the peak at 4 h with an increase in exposure time. These findings indicate that there is a certain threshold for the physiological effects corresponding to altitudes, and longer durations are not necessarily superior. The principle also applies to the total number of IHE treatments. 71 Garcia et al. 90 discovered that the HVR reached its peak at day 5, returning to the initial level by day 12. Excessive treatment may induce hypoxia adaptation, thereby diminishing the potential benefits of hypoxic stress.
Changes in physiological indicators after IHE.
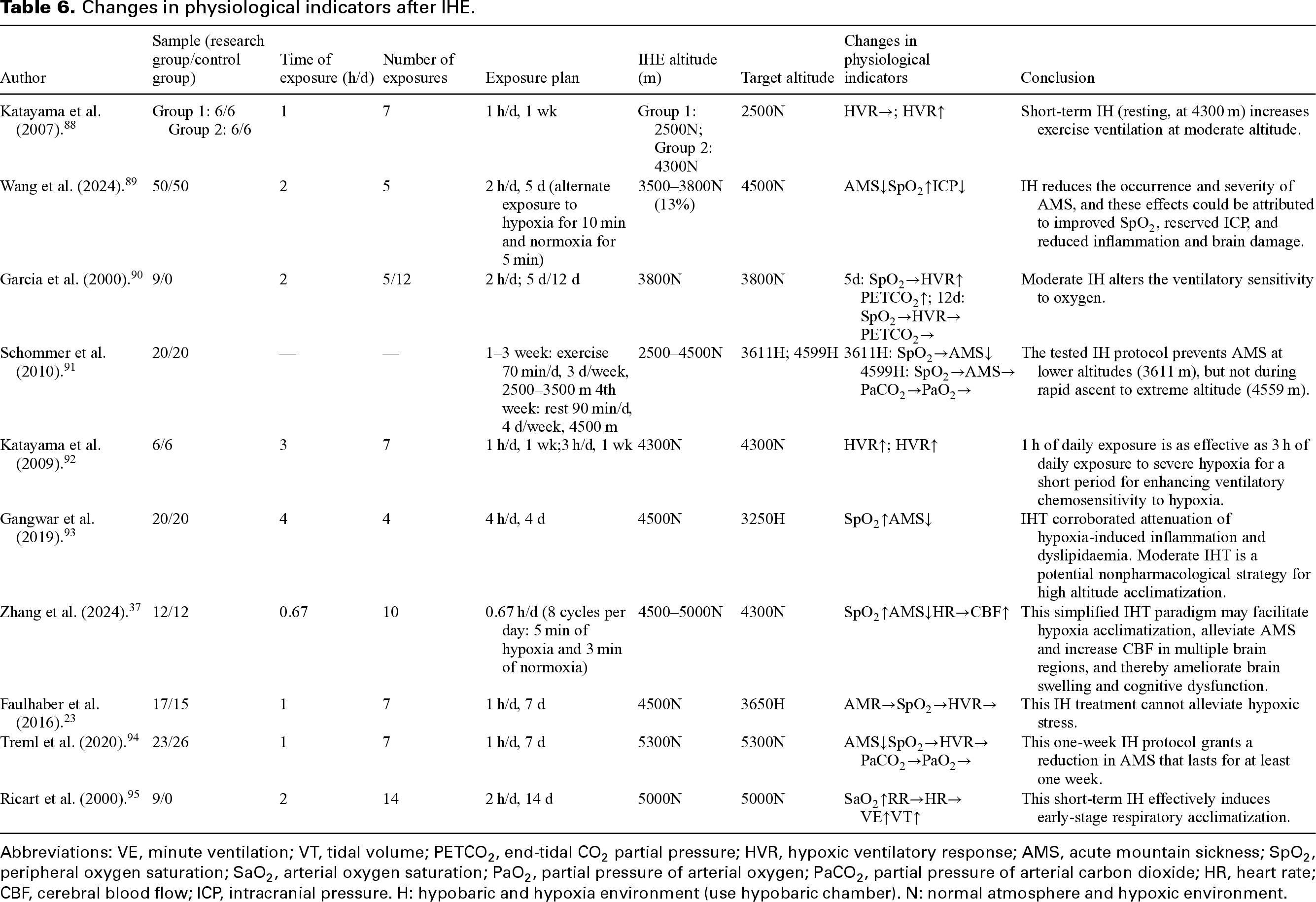
Abbreviations: VE, minute ventilation; VT, tidal volume; PETCO2, end-tidal CO2 partial pressure; HVR, hypoxic ventilatory response; AMS, acute mountain sickness; SpO2, peripheral oxygen saturation; SaO2, arterial oxygen saturation; PaO2, partial pressure of arterial oxygen; PaCO2, partial pressure of arterial carbon dioxide; HR, heart rate; CBF, cerebral blood flow; ICP, intracranial pressure. H: hypobaric and hypoxia environment (use hypobaric chamber). N: normal atmosphere and hypoxic environment.
In addition, it should be noted that normobaric hypoxia (NH) and hypobaric hypoxia (HH) have different effects on human physiological responses. NH is widely used for convenience, but the effect of ambient pressure is ignored. HH typically induces more pronounced physiological stress than NH, attributable to differences in ventilatory patterns, alveolar gas disequilibrium and dissimilar acute hypoxic ventilatory responses. 97 These factors lead to more severe symptoms of AMS in HH, yet they may also enhance the efficacy of high-altitude acclimatization. 97
Oxygen enrichment
Lowlanders often lack sufficient time for pre-acclimatization, increasing risks during direct exposure to high altitudes. Hypoxia can be fundamentally addressed through oxygen enrichment. This method increases SpO2, reduces HR and reduces the incidence or severity of AMS.26,98 It is the most direct, convenient and safe method of prevention and treatment for high-altitude exposure.
Oxygen delivery methods are typically classified into two primary modalities. The first modality is nasopharyngeal oxygen delivery via nasal cannulas or masks, mostly used in emergency medical and portable hypoxia in life or work. Although achieving high oxygen utilization rates, this method causes nasal cavity discomfort. 99 and reduces work efficiency by increasing physical anxiety. 100 The second modality is diffusion oxygen supply, which increases ambient oxygen concentrations. This system exhibits wide applicability and excellent comfort, rendering it particularly suitable for daily living environments. West. 98 pioneered the oxygen enrichment concept, establishing that a 1% increase in oxygen concentration (e.g., from 21% to 22%) corresponds to an equivalent altitude reduction of 300 m. This seminal research substantially advanced oxygen-enriched environment comprehension. Subsequent field and laboratory studies have consistently demonstrated that oxygen enrichment benefits human physiology, psychology, cognitive performance, work efficiency and sleep quality.26,101,102 However, the widespread adoption of oxygen enrichment has been hindered by low oxygen delivery efficiency. 19 Consequently, researchers have explored alternative oxygen delivery methods (e.g., point source oxygen supply. 19 and targeted oxygen supply device. 103 ) and distribution strategies. 104 to enhance efficiency. Furthermore, oxygen concentrations cannot be arbitrarily increased, even disregarding efficiency concerns. Safety standards mandate strict upper98,105 and lower18,106 concentration limits to prevent fire hazards while ensuring safety and comfort. The US National Fire Protection Association 99B (NFPA 99B). 107 stipulates that the volume fraction of O2 must not exceed 23.5% at 101.3 kPa. Furthermore, by referencing the burning rate of filter paper at 23.5% at 101.3 kPa, this standard provides the upper concentration limits for oxygen-enriched indoor environments under different atmospheric pressures. Accordingly, West et al. 98 established equivalent altitude corresponding to the actual altitude and the oxygen concentration under U.S. National Fire Protection Association guidelines, 107 shown in Figure 7.
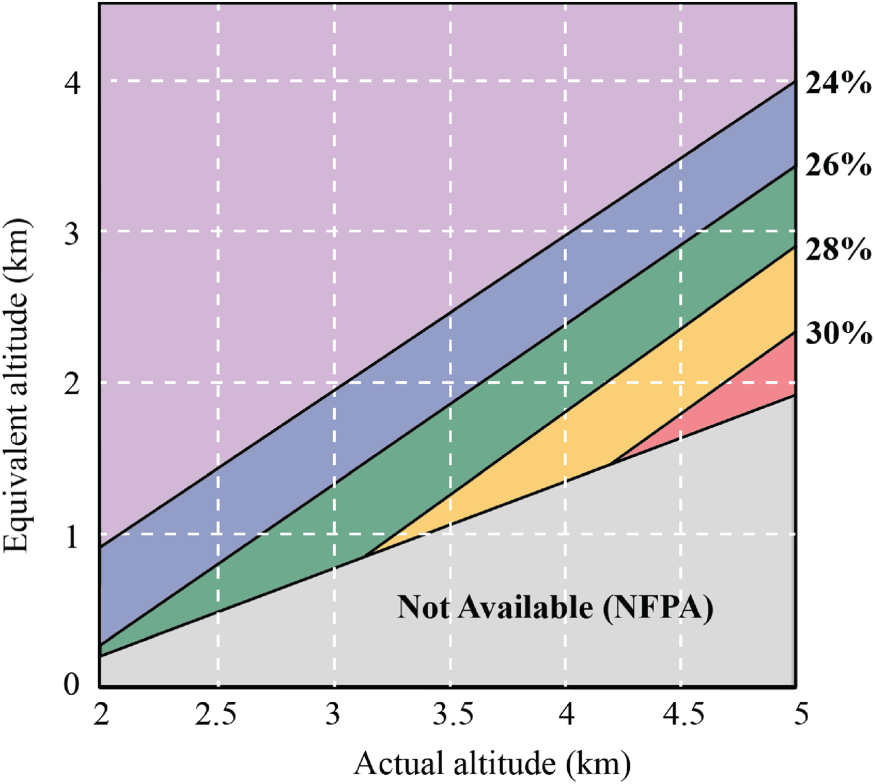
Oxygen conditioning diagram (replotted from West 98 ).
As highlighted in the section ‘Assessment of short-term exposure to AMS’, the substantial population with oxygen comfort requirements cannot be overlooked. Consequently, determining the optimal oxygen concentration balancing delivery efficiency and safety has emerged as a critical research frontier and a societal necessity. Surprisingly, this critical aspect remains largely unexplored, with only the pioneering work by Song et al. 67 addressing this gap. Their innovative study combined subjective and objective parameters to classify lowlanders at high altitudes into three oxygen adaptation levels (high, medium, low), achieving an impressive prediction accuracy of 94.96%. Eventually, the correlation between adaptation levels and optimal indoor oxygen environment parameters was established, enabling personalized oxygen delivery strategies. This foundational research provides valuable insights for future investigations of optimal oxygen concentrations.
Challenges and future perspectives
Societal development has increased lowlanders’ exposure to high-altitude environments, and the issue of alleviating hypoxia has become a concern for the public. Based on our analysis, we propose the following strategies to enhance high-altitude experiences.
Empirically based guidance in gradual ascent
Gradual ascent is widely regarded as the most valuable approach for preventing high-altitude illnesses. However, existing ascent recommendations are inconsistent and largely rely on traditional empirical guidelines, as described in the section ‘Gradual ascent’. These recommendations lack robust physiological mechanistic support and exhibit substantial practical limitations due to individual differences, environmental variability and other multifactorial influences. The quantitative prediction AMS model established by Beidleman et al. 80 has significantly improved the objectivity and practicality of ascent recommendations. However, the model is limited to target altitudes of 4000 m, restricting its generalizability to other elevations. Future research should focus on the following directions: (1) Extending model applicability across altitude ranges to establish ascent recommendation standards suitable. (2) Integrating clinical monitoring indicators, such as resting and exercise SpO2, PAP and HRV, to enable multimodal data fusion with the Ascent Advice Evaluation (AAE) model. This approach promises to develop a more precise and personalized risk assessment system. Ultimately, high-altitude ascent guidelines can evolve from experience-based to evidence-driven, supporting safer and more scientific mountaineering for diverse populations.
Development of a universal oxygen comfort evaluation standard
Current AMS studies primarily focus on pathophysiological mechanisms and clinical interventions within the biomedical field. However, a critical research gap exists in diagnosing mild and subclinical hypoxia manifestations. Over 70% of high-altitude sojourners experience mild or subclinical hypoxic symptoms that substantially impact quality of life despite not requiring medical intervention (as discussed in ‘Assessment of short-term exposure to AMS’). Existing assessment questionnaires lack sensitivity for grading these symptoms. Only the pioneering work by Song et al. 22 has developed a multidimensional symptom severity method to comprehensively diagnose mild and subclinical hypoxia. Nevertheless, this method lacks empirical validation in heterogeneous populations, and the absence of dynamic monitoring and verification only at 3650 m.
Future research should prioritize: (1) incorporating high-risk populations (e.g., elderly and chronic disease patients) with multi-omics (genomics/metabolomics) profiling to decode individual hypoxic response variations; (2) developing dynamic oxygen prediction models through wearable device-reinforcement learning integration for personalized environmental regulation; (3) constructing multi-altitude experimental platforms with cross-cultural validation protocols; and (4) translating intelligent oxygen supply technologies into evidence-based clinical interventions and architectural guidelines, ultimately enabling a paradigm shift from pathological remediation to proactive comfort optimization in high-altitude public health strategies.
Personalized dynamic prediction of Ih protocols
The optimization of IHE protocols for pre-acclimatization faces two core challenges: (1) Unlike fixed-altitude aerobic training for athletes, IHE must account for dynamic variations in target altitudes, rendering conventional single IHE protocols inadequate; and (2) Current research focuses on verifying IHE ‘effectiveness’ while lacking mechanistic understanding of dose–response relationships and individualized response thresholds. Future studies should: (1) Develop quantitative models correlating adaptation altitudes with target altitudes to elucidate dynamic relationships between altitude gradients and exposure duration; (2) Integrate multidimensional physiological indicators (SpO2, HRV) to establish intelligent prediction systems; and (3) Create personalized pre-acclimatization protocols based on individual characteristics (e.g., age and gender). These advancements will transform IH research from phenomenological observation to mechanistic understanding, providing scientific foundations for altitude-specific personalized pre-acclimatization.
Thermal-oxygen coupling in high-altitude environmental control
The physiological mechanisms and engineering applications of thermal-oxygen coupling remain critical knowledge gaps in high-altitude research. Current studies often examine oxygen or temperature stressors separately, neglecting their combined effects on human thermogenesis (e.g., brown adipose tissue activation) and oxygen transport efficiency (e.g., temperature-dependent haemoglobin-oxygen dissociation). Duan et al. 54 demonstrated that hypoxia discomfort decreases under thermal comfort. However, two key limitations persist: (1) Absence of quantitative models for thermal-oxygen parameter interactions, particularly regarding temperature regulation dynamics under oxygen enrichment (FiO2 > 0.21) across altitudes; and (2) Failure to integrate individual thermal preference (e.g., inhabitants from different climatic zones) with dynamic physiological demands. Future research must develop multiphysics coupling models using computational fluid dynamics (CFD) to simulate oxygen-thermal distribution patterns, combined with reinforcement learning algorithms to optimize ‘temperature-oxygen concentration’ combinations, ultimately informing novel environmental control strategies for high-altitude eco-architecture.
Conclusion
In this article, we reviewed physiological and objective indicators associated with exposure to high altitudes. A summary of methods aimed at alleviating hypoxia was also provided. This study systematically analysed the effects of short-term high-altitude exposure on respiratory, cardiovascular and thermoregulation systems. For each system, we have identified clinically valuable physiological indicators to provide precise assessment criteria. Through comprehensive evaluation of six existing AMS questionnaires, we conducted comparative analyses between five representative assessment tools and the gold-standard LLS. The limitation is insufficient evaluation of subclinical or mild AMS manifestations, highlighting the need to establish a novel oxygen-comfort-oriented assessment system. Current acclimatization methods were systematically reviewed and elaborated, including gradual ascent, intermittent hypoxia exposure and oxygen enrichment. Some specific implementation recommendations for each approach are provided.
To advance high-altitude comfort management research, we propose four key research priorities: (1) constructing a more comprehensive empirical-guided gradual ascent model, (2) establishing subjective oxygen comfort evaluation standards for subclinical or mild AMS, (3) developing personalized intermittent hypoxia exposure protocols, and (4) innovating thermal-oxygen coupled environment control technologies. These recommendations construct a comprehensive technical roadmap encompassing assessment methodologies, preventive interventions and environmental regulation, ultimately providing systematic solutions to ensure the comfort of plains populations in high-altitude environments.
Footnotes
Acknowledgements
The authors wish to thank the financial support of the National Natural Science Foundation of China (Nos. 52038009 and 52578145).
Author's contribution
Yue Hu: conceptualization, writing – original draft, writing – reviewing and editing, and visualization. Xiaoling Cao: writing – reviewing and editing. Xiaowen Su: writing – reviewing and editing. Yanping Yuan: writing – reviewing and editing, supervision, and funding acquisition. Liangliang Sun: conceptualization, writing – reviewing and editing, and funding acquisition.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant nos. 52038009, 52578145).