
Abstract
Background
Prostate-specific antigen (PSA) remains the most widely used biomarker for prostate cancer screening, diagnosis, and monitoring. However, despite decades of standardization efforts, significant inter-assay variability persists, with important consequences for clinical interpretation and decision-making.
Objective
This review aims to evaluate the impact of PSA calibration and harmonization on reference intervals, clinical thresholds, and population-based screening strategies in contemporary clinical practice.
Methods
A literature-based analysis was conducted, examining studies on PSA assay standardization, analytical variability, and evidence from population screening trials, including considerations from a Health Technology Assessment perspective.
Results
The introduction of the World Health Organization (WHO) International Standard 96/670 improved comparability among PSA assays, yet clinically relevant differences between platforms remain. This variability is driven by differences in calibration, antibody specificity, epitope recognition, and assay design. As a result, PSA values are not directly interchangeable across assays, and assay-specific cut-offs may be necessary to maintain diagnostic performance. Historically established thresholds, such as the 4 μg/L cut-off and the “gray zone,” were derived using specific assay systems and are influenced by methodological limitations. PSA-derived metrics, including PSA density, improve specificity but are still affected by inter-assay variability. Evidence from large randomized trials supports a PSA cut-off of 3.0 μg/L for population screening, showing a reduction in prostate cancer mortality when implemented within structured programs; however, this threshold is intrinsically linked to the analytical characteristics of the assays used. PSA also shows relevant intra-individual biological variability beyond analytical variation, with within-subject variation of 6–13%.
Conclusions
PSA standardization remains incomplete, and inter-assay variability and biological variability continues to influence clinical interpretation. The implementation of PSA-based screening programs must explicitly consider the assay-specific nature of evidence-derived thresholds, including the 3.0 μg/L cut-off, to ensure consistent, effective, and safe clinical decision-making.
Inter-assay differences in prostate-specific antigen levels
Prostate-specific antigen (PSA) remains the key biomarker in the management of prostate cancer patients. Since its clinical implementation in the late 1980s, PSA has been widely used to guide biopsy decisions, assess treatment response, and detect biochemical recurrence. 1 More recently, policy support for risk-adapted prostate cancer screening has redefined the clinical landscape of PSA use. This shift has been significantly shaped by the 2022 recommendation from the European Commission to implement organized PSA-based screening programs incorporating multiparametric magnetic resonance imaging (mpMRI) as a triage test.2,3 Within this framework, analytical accuracy, inter-assay comparability, and calibration traceability are essential to ensure consistent clinical decisions, as assay design directly influences reference intervals, biopsy thresholds, and ultimately patient selection in contemporary screening algorithms.
In the mid-1990s, concerns emerged regarding the lack of comparability among commercially available PSA assays. Semjonow et al. 4 highlighted that significant inter-assay variability could compromise the interpretation of PSA measurements in clinical practice, potentially resulting in misclassification of patients and subsequent diagnostic or therapeutic errors. At that time, they emphasized that decision thresholds established for one analytical assay could not be assumed to be interchangeable with those derived from another platform.
To address these discrepancies, the World Health Organization (WHO) introduced the PSA reference material 96/670 in 1999, defined as a preparation containing 90% PSA bound to α1-antichymotrypsin and 10% free PSA. 5 Most manufacturers subsequently recalibrated their assays against this standard, progressively improving inter-assay comparability.
Recent global evaluations of PSA harmonization, such as the study by Van Rossum et al., 6 indicate that PSA assays generally achieve acceptable agreement relative to consensus means across multiple external quality assessment programs. While these findings confirm that substantial progress has been made toward harmonization, residual inter-assay differences persist. Although PSA is broadly harmonized, careful interpretation of individual assay results remains essential for accurate clinical decision-making. Together, these data underscore the ongoing need for coordinated international efforts, such as the IFCC/ISOBM Working Group on Tumor Marker Harmonization, to further reduce variability and support consistent application of PSA-based thresholds in both screening and patient management.
An interesting case is the PSA reagent from Beckman Coulter, available with both WHO 96/670 calibration and the original Hybritech calibrator, the latter forming the basis of established clinical thresholds. PSA values obtained using the WHO calibration are approximately 20% lower than those obtained with the Hybritech standard. 7 Accordingly, Jansen et al. 8 underlines that biopsy thresholds of 3 and 4 μg/L should be adjusted to 2.4 and 3.2 μg/L when using WHO calibration.
The introduction of the WHO standard has reduced inter-assay variability, but it has not achieved absolute equivalence in results obtained with different reagents. 9 Several additional studies have consistently reported that despite standardization efforts, significant inter-assay variability in PSA measurements persists, underscoring the need for continued vigilance in assay interpretation.10–15 Interestingly, Stephan et al. 10 demonstrated in a study comparing five commercial PSA assays that, despite similar areas under the curve, assay-specific cut-offs must be applied to achieve comparable sensitivity and specificity across platforms. In this context, Foj et al. 11 reported that differences between PSA Access (Beckman Coulter) calibrated using WHO standards and PSA Immulite 2000 assay (Siemens) results, also using WHO standards, exceeded 20% in 74% of patients and surpassed 40% in 41% of cases, emphasizing the persistence of clinically relevant discrepancies among PSA assays, despite WHO-based standardization efforts. Obviously, these differences persist across the full range of PSA concentrations, consequently affecting the cut-off values established for clinical decision-making. For instance, Filella et al. 16 recently reported inter-laboratory discrepancies in the accurate determination of biochemical recurrence following radical prostatectomy.
Residual inter-assay differences are not solely attributable to the calibration standard, but also reflect variability in antibody specificity and epitope recognition, as highlighted in the ISOBM TD-3 Workshop, which characterized 83 PSA antibodies and demonstrated substantial differences in analytical performance. 17 Consistently, Ferraro et al. 18 evaluated four modern immunoassay platforms for PSA using native serum samples and demonstrated that, despite improvements driven by WHO reference materials, current PSA assays are still not fully harmonized. They reported that sample-dependent differences in assay results could arise from differences in antibody specificity and epitope recognition, cross-reactivity with related proteins such as hK2, and nonequimolar recovery of PSA forms.
Several clinical guidelines acknowledge differences in PSA measurements with WHO-calibrated assays, though not always accurately.19,20 For example, the American Urological Association’s Prostate-Specific Antigen Best Practice Statement: 2009 Update 21 reported that assays using the WHO 96/670 reference material yield results about 20–25% lower than those based on Hybritech. Similarly, the 2013 European Association of Urology Guidelines on Prostate Cancer 22 recommended a PSA cut-off of 3–3.1 µg/L for WHO-calibrated assays to match the sensitivity and specificity of the traditional 4 µg/L Hybritech-based threshold. More recently, the same concept has been highlighted in the laboratory operating instructions for PSA measurement issued by the regional prostate cancer screening program in Lombardy, Italy. 23 The document indicates that analytical platforms calibrated using the Hybritech standard report significantly higher results compared with assays calibrated according to the WHO standard.
Available evidence suggests that PSA concentrations obtained with WHO-calibrated assays are not systematically lower than those measured with the PSA Hybritech assay. Inter-assay differences cannot be attributed solely to calibration but instead reflect broader assay-dependent sources of variability. Consistent with this, good analytical agreement between WHO-calibrated Cobas PSA assay (Roche) and Hybritech-calibrated PSA assay (Beckman) has been reported by Stephan et al. 10 and by Blijenberg et al. 24 In the study by Stephan et al., PSA measurements from the Hybritech Beckman and Cobas assays showed close analytical agreement in both non–prostate cancer and prostate cancer patients, with only minimal differences in median values. Similar concordance was reported by Blijenberg et al., confirming that, despite minor numerical variations, the two platforms provide comparable results across patient groups. More recently, Filella et al. 25 reported a close analytical agreement between the Hybritech Beckman PSA assay (using the Hybritech calibrator), the Roche PSA assay, and the still non-commercialized Siemens hsPSA assay (the latter two calibrated against the WHO standard).
Recently, at the request of the WHO, the National Institute for Biological Standards and Control (NIBSC) has prepared a second International Standard to replace the 96/670 standard, because stocks of the original preparation had become depleted. 26 Consequently, a new reference material, designated 17/100, was established to ensure continuity of assay calibration, traceability, and comparability of PSA measurements worldwide, in accordance with the recommendations of the WHO Expert Committee on Biological Standardization.
In this context, the evaluation by Ferguson et al. 27 showed that the replacement preparations had assigned mass concentrations consistent with their intended values and were commutable across a range of widely used immunoassay platforms, supporting their suitability for continued international standardization of PSA measurements. However, although the introduction of 17/100 standard may reduce certain sources of variability, clinically relevant inter-assay bias between commercial immunoassays persists. Full harmonization of PSA results has therefore not yet been achieved, suggesting that the introduction of the second WHO International Standard for PSA alone is unlikely to enable the establishment of universally applicable reference intervals across different assay platforms. To date, to the best of our knowledge, no studies have been published comparing the performance of newly developed commercial assays calibrated against the 17/100 standard in extensive cohorts of clinical samples.
Impact of standardization on reference values and specificity of prostate-specific antigen
In 1986, Myrtle et al., 28 using the Hybritech Tandem-R assay system, first proposed a PSA cut-off of 4 μg/L. This study had methodological limitations, as PSA levels were assessed in 860 apparently healthy men without systematically excluding prostate disease. Nonetheless, the 4 μg/L threshold was subsequently validated by Catalona et al. 29 in a multicenter study across six university hospitals, using the Hybritech Tandem-R assay system or the Hybritech Tandem-E assay system. The study included 6630 men over 50 years of age, all of whom underwent both PSA testing and digital rectal examination. In 1994, the Food and Drug Administration approved PSA measurement for the early detection of prostate cancer, establishing 4 μg/L as the threshold for recommending biopsy.
The concept of a “gray zone” was later introduced to describe PSA levels within an intermediate range, initially defined as 4–10 μg/L, where the risk of prostate cancer is uncertain. 30 Current guidelines have expanded this range downward to 2–3 μg/L in many clinical contexts, reflecting evidence that clinically significant prostate cancers can occur at lower PSA levels. 31 Diagnostic approaches within this gray zone have evolved beyond the use of the free-to-total PSA ratio, now also incorporating advanced biomarkers such as the Prostate Health Index (PHI), 4K score, and the Stockholm 3 test, which demonstrate superior diagnostic accuracy compared to traditional PSA derivatives.32,33 These novel biomarkers can reduce unnecessary biopsies by 20–40% while maintaining 90–95% sensitivity for clinically significant prostate cancer (Grade Group ≥2).
Various strategies to improve PSA specificity were developed in the 1990s. For instance, in 1992, Carter et al. 34 proposed that an annual PSA increase greater than 0.75 μg/L could indicate prostate cancer. Physiological age-related prostate growth has led to the proposal of age-adjusted PSA thresholds, 35 ranging from 2.5 μg/L in men aged 40–49 to 6.5 μg/L in those aged 70–79, with variations across ethnic groups. Additionally, PSA density (PSAD)—the ratio of serum PSA to prostate volume measured by transrectal ultrasound or mpMRI—has been proposed to reduce false-positive results, 36 with values above 0.15 μg/L per cm3 considered indicative of clinically significant prostate cancer. 37 While age-adjusted PSA thresholds and PSA velocity have not been consistently supported by subsequent studies and provide limited added value, PSAD can improve specificity by distinguishing benign prostatic hyperplasia from clinically significant prostate cancer, thereby guiding biopsy decisions and selection for active surveillance.38,39 In this line, the European Association of Urology clinical guideline describes the likelihood of clinically significant prostate cancer based on PI-RADS classification and PSAD, categorizing PSAD into four levels: low (<0.10), intermediate-low (0.10–0.15), intermediate-high (0.15–0.20), and high (>0.20 μg/L). 40
The traditional 4 μg/L cut-off and the gray-zone thresholds for PSA as well as all discriminative PSA-derived values must be interpreted in the context of assay-dependent variability. Early landmark studies by Myrtle et al. and Catalona et al. employed the Hybritech assay, as did Oesterling et al. and Benson et al. in their original descriptions of age-adjusted PSA thresholds and PSAD, respectively, highlighting the importance of assay-specific context in interpreting these values. PSA concentrations obtained using the PSA Hybritech assay differ from those generated by other platforms, introducing substantial inter-assay variation. As a result, direct comparison of PSA measurements across studies and clinical settings is inherently problematic unless the assay used in the measurement has a good alignment with Hybritech PSA.
Key factors affecting the interpretation of historical PSA thresholds in contemporary clinical practice.
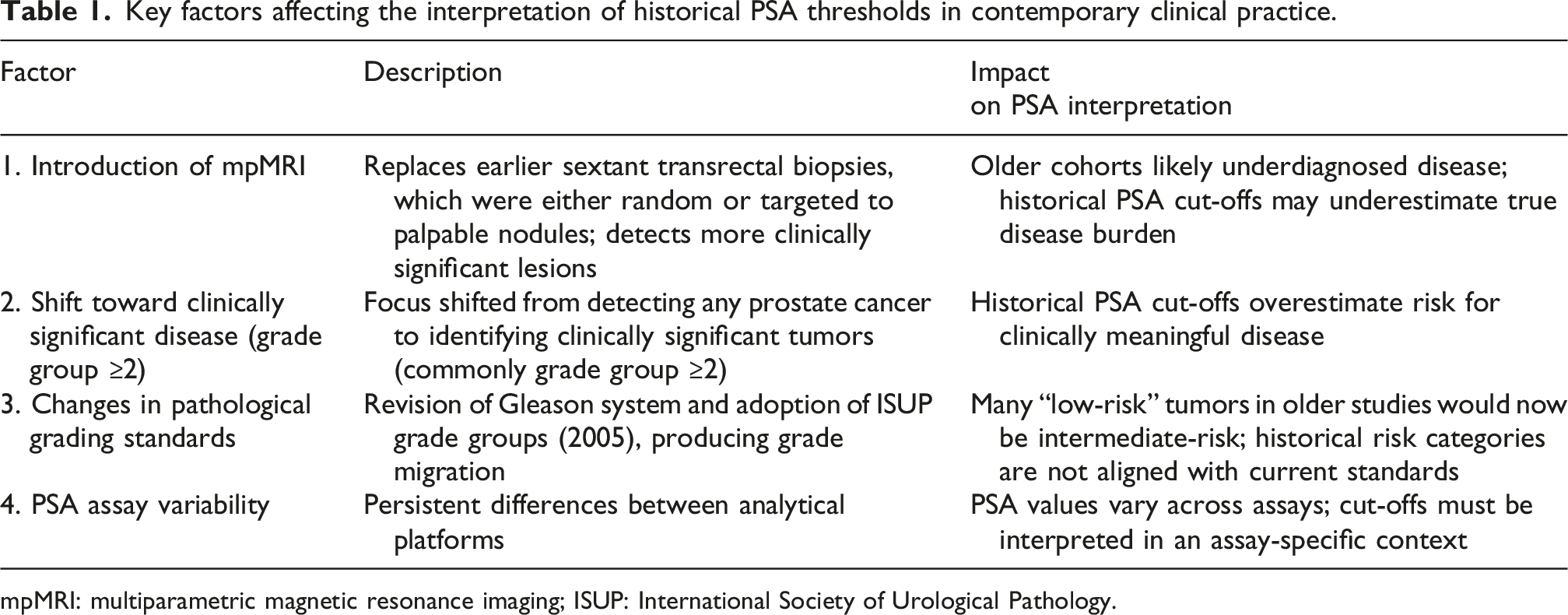
mpMRI: multiparametric magnetic resonance imaging; ISUP: International Society of Urological Pathology.
First, the introduction of mpMRI has transformed prostate cancer diagnostics. Earlier cohorts were typically stratified on the basis of sextant transrectal ultrasound–guided biopsy, which has since been shown to miss a significant proportion of clinically relevant lesions. mpMRI-based targeting and improved systematic sampling now provide superior disease characterization, highlighting that many cancers were likely underdiagnosed in older series. 41
Second, the clinical focus has progressively shifted from detecting any prostate cancer to identifying clinically significant disease, commonly defined as Grade Group ≥2.42,43 This reorientation complicates the interpretation of earlier datasets and the corresponding cut-offs that did not distinguish between indolent and aggressive tumors. Thus, their proposed PSA cut-offs inherently overestimated risk, and cannot be directly applied to present-day definitions of clinically meaningful disease.
Third, temporal changes in pathological grading standards—including revisions to the Gleason system and the adoption of the current Grade Group classification—have produced marked grade migration.44–46 The 2005 International Society of Urological Pathology (ISUP) revision reclassified numerous patterns previously considered Gleason 6 into higher grades, thus increasing Gleason scores across cohorts. Clinical validation studies further show that reapplying modern ISUP criteria to older prostatectomy specimens markedly improves prediction of metastasis and reclassifies many tumors into higher risk groups, highlighting the non-comparability of historical grading. 47 As a result, the risk categories of historical PSA outcome studies are not aligned with contemporary standards. Many “low-risk” cancers in older publications would today be considered intermediate-risk, and a substantial share of “clinically insignificant” tumors in early PSA cohorts would not qualify as such under modern criteria.
Fourth, the persistent lack of standardization across PSA platforms continues to generate clinically meaningful discrepancies in measured values, reinforcing the need for assay-aware interpretation. Despite this, contemporary clinical guidelines generally rely on fixed numerical cut-offs without specifying the analytical context in which these thresholds were derived, thereby overlooking the impact of assay-dependent variation.
Collectively, these factors underscore the need for caution when extrapolating historical PSA or PSAD thresholds to modern clinical decision-making and highlight the importance of assay calibration and methodological context when interpreting the evidence base.
Finally, in addition to analytical variability between laboratory measurements, PSA levels also show significant intra-individual biological variability. PSA concentrations may fluctuate spontaneously from day to day within the same subject, even in the absence of clinically relevant changes in prostate pathology. Data from the EFLM Biological Variation Database indicate that the within-subject biological variation of total PSA is approximately 6.8% (95% CI: 6.1–7.4) in healthy individuals, 48 whereas studies conducted in screening populations of men have reported somewhat higher variability, generally around 10–13%. 49 Additionally, in a large screening cohort of men, considerable intra-individual PSA variability was observed, with 22–30% of elevated values reverting below diagnostic thresholds on repeat testing. 50
For this reason, PSA should be interpreted in the context of serial testing rather than on the basis of a single measurement. Therefore, when an unexpected or borderline elevation is observed, repeat testing after an appropriate interval is recommended before proceeding to further diagnostic tests, such as mpMRI or prostate biopsy. This approach may help mitigate the clinical impact of intra-individual variability.
PSA cut-off for population screening in the era of health technology assessment
Health Technology Assessment (HTA) has become a central framework for decision-making in modern healthcare systems, particularly when implementing diagnostic technologies at the population level. 51 Unlike traditional approaches that focus primarily on analytical performance or diagnostic accuracy, HTA evaluates technologies based on their impact on patient outcomes, healthcare organization, and cost-effectiveness. This perspective is particularly relevant for biomarkers, whose value is indirect: they influence downstream clinical decisions rather than providing therapeutic benefits themselves. Consequently, the evaluation of a biomarker must go beyond sensitivity and specificity, considering whether its use ultimately improves health outcomes, reduces harm, and represents an efficient use of healthcare resources.
PSA screening is a prime example of how HTA principles apply in practice. The early widespread adoption of PSA testing was driven largely by its diagnostic performance and biological plausibility. However, its indiscriminate use led to significant concerns regarding overdiagnosis, overtreatment, and unnecessary biopsies. The HTA perspective shifted the evaluation of PSA from simple cancer detection to its ability to reduce prostate cancer mortality while minimizing harms and resource utilization. In this context, randomized screening trials represent the most robust evidence linking a biomarker-based strategy to meaningful clinical outcomes.
The recent recommendation by the European Commission for member states to implement organized prostate cancer screening programs incorporating PSA testing and mpMRI2,3 has brought renewed urgency to the question of optimal PSA cut-off thresholds. This policy shift reflects a fundamental change in the European approach to prostate cancer early detection, moving from opportunistic testing toward structured, population-based programs. In this context, the selection of PSA cut-off values becomes not merely a technical decision about assay performance, but a critical determinant of program effectiveness, resource utilization, and the balance between benefits and harms at the population level.
The cut-off of 3.0 μg/L PSA used in the European Randomized Study of Screening for Prostate Cancer (ERSPC) represents the most robust evidence base for population screening. 52 The ERSPC, initiated in the early 1990s across eight European countries, enrolled 162,236 men aged 55–69 years. 53 The trial protocol used Hybritech PSA assays, specifically the Tandem E assay from 1994 through 2000 and subsequently the automated Access assay by Beckman Coulter.54,55 From 1996 onward, most centers defined a PSA level of ≥3.0 μg/L as a positive screening result, prompting further diagnostic evaluation and referral for biopsy. 56
After 23 years of follow-up, the trial demonstrated a 13% reduction in prostate cancer mortality (rate ratio 0.87; 95% CI 0.80–0.95), with an absolute risk reduction of 0.22%. Critically, the harm-benefit ratio has improved substantially over time. At 23 years, one prostate cancer death was prevented for every 456 men invited to screening and every 12 men diagnosed, compared with 628 and 18 men, respectively, at 16 years. 56 The Rotterdam section of ERSPC, which provided the largest single-center contribution, reported even more favorable outcomes after 21 years: a rate ratio for prostate cancer mortality of 0.73 (95% CI 0.61–0.88) and for metastatic prostate cancer of 0.67 (95% CI 0.58–0.78). 57 These data indicate that a PSA threshold of 3.0 μg/L, when applied systematically with repeated screening every 2 to 4 years, is associated with a meaningful reduction in prostate cancer mortality. It also maintains an acceptable balance between benefits and harms, a balance further enhanced by the adoption of active surveillance strategies and the integration of mpMRI into the diagnostic pathway.
From a HTA perspective, these observations have important implications. Screening strategies should ideally be implemented under conditions that replicate those in which clinical benefits were originally demonstrated, particularly given the well-documented variability among commercial PSA assays. Differences in calibration, antibody specificity, epitope recognition and the assay design can lead to systematic deviations in PSA values compared with the original Hybritech assay, potentially resulting in inconsistent clinical decisions if universal cut-offs are applied without appropriate analytical alignment (Figure 1). PSA assay variability and screening outcomes.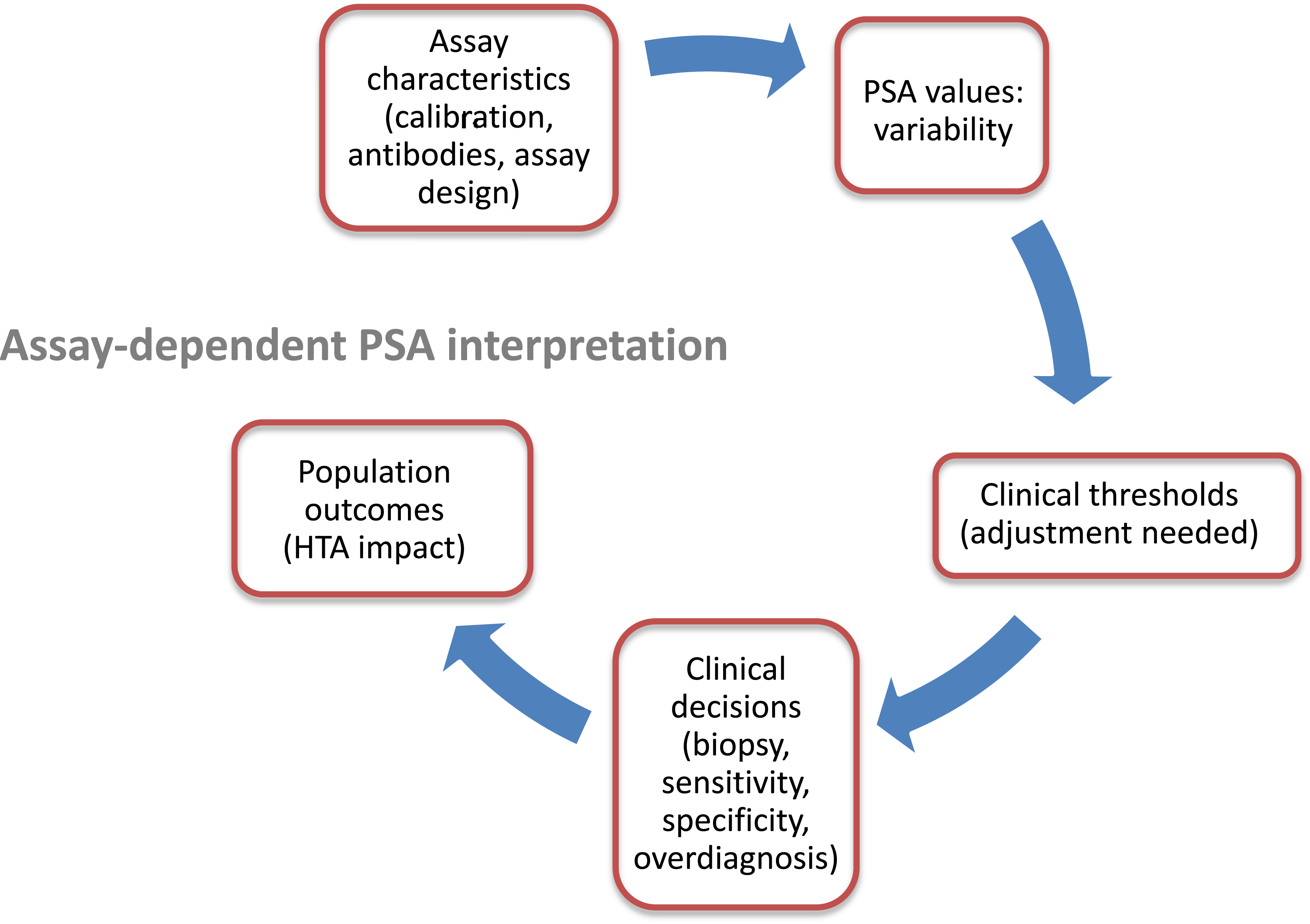
Modifying key parameters, such as using an assay that does not align with Hybritech PSA results, may alter the balance between benefits and harms by influencing biopsy rates, overdiagnosis, and resource utilization. Consequently, the clinical utility of a given PSA threshold cannot be interpreted independently of the analytical context in which it is applied. The observed reduction in prostate cancer mortality reflects the performance of a screening strategy defined by both a specific assay and its corresponding decision threshold.
In light of current evidence, a PSA cut-off of 3.0 µg/L remains the most evidence-based threshold for population-based screening, provided that the assay used is aligned with the Hybritech reference system. When systematic deviations exist, threshold adjustment may be required to preserve equivalence with evidence-based strategies.
In conclusion, PSA standardization remains incomplete, and assay-dependent variability continues to influence clinical decision-making. The use of fixed PSA cut-offs without consideration of analytical context may compromise consistency and reproducibility, particularly in population-based screening. Ensuring coherence between assay reagent and clinically validated thresholds is therefore essential for the effective and safe implementation of PSA-based strategies.
Footnotes
Acknowledgments
The authors declare that they have no acknowledgements.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Xavier Filella, as the principal investigator, entered into an agreement with Siemens Diagnostics to evaluate the Atellica hsPSA assay.