
Abstract
This narrative review examines gender-affirming healthcare in the Nordic countries, highlighting historical developments, legal frameworks, epidemiological trends, and current clinical practices. Transgender healthcare dates back to the early 20th century and gained international attention in the early 1950s following one of the first widely publicized gender-affirming surgeries performed in Denmark. Since then, care models have evolved, supported by policy, research, and clinical practice across Europe and North America.
All Nordic countries, Denmark, Finland, Iceland, Norway, and Sweden, provide publicly funded gender-affirming healthcare, although service structures differ. Legal gender recognition has shifted toward self-identification in Denmark, Finland, Iceland, Norway, and from July 2025, also Sweden by removing medical or psychiatric prerequisites.
In parallel, epidemiological data reveal an increased healthcare utilization, particularly among youth assigned female at birth. Elevated rates of mental health challenges highlight the need for integrated psychosocial support. Clinical care typically follows a multidisciplinary model including psychiatric and medical assessment, hormone therapy, and surgery when indicated. Access to chest and genital surgery requires a formal diagnosis and is with few exceptions restricted to adults. Evidence supports the positive impact of gender-affirming treatment on gender congruence and health-related quality of life. Regret after gender-affirming surgery is rare but does occur, underscoring the importance of individualized care and thorough informed consent.
Ongoing challenges include long wait times, unequal access for non-binary individuals, and a growing number of individuals seeking private or cross-border care. Future efforts should focus on expanding public services, strengthening research, and promoting equitable, evidence-based care that reflects the diversity of gender identities.
Keywords
Terminology
Introduction
Transgender and gender-diverse is a term to describe individuals or communities whose gender identities or gender expression does not align with the sex assigned to them at birth. Some transgender and gender-diverse individuals may experience gender dysphoria and may seek gender-affirming medical and surgical treatment to make their bodies more congruent with their gender identity.
Transgender perspectives are frequently discussed in the media and represent a topic of growing interest to the general population. The number of individuals undergoing gender-affirming surgical interventions is increasing, and therefore, medical professionals, and in particular surgeons, need to be familiar with what these procedures entail.
The aim of this article is to provide a comprehensive overview of epidemiology, history, legislation, and scientific perspectives related to transgender healthcare in the Nordic countries.
Methods
An international team consisting of plastic surgeons, a psychiatrist, a pediatric and adolescent psychiatrist, and a breast surgeon collaborated to write this review article. All the Nordic countries were represented within the team. References included scientific publications identified via PubMed, as well as national clinical guidelines and governing policy documents.
History
The history of the first gender-affirming surgical procedures dates back to the early 20th century, with the first known operations taking place in Germany.1–3
Magnus Hirschfeld (1868–1935) was a German physician, sexologist, and a pioneering advocate for sexual minorities, particularly in the fields of homosexual and transgender rights. He is widely considered one of the founding figures of modern sexology, particularly transgender healthcare. In 1897, he moved to Berlin and co-founded the Scientific-Humanitarian Committee (Wissenschaftlich-humanitäres Komitee, WHK). The purpose of the WHK was to advocate for the abolition of the law criminalizing male homosexuality in Germany, and has been considered the first organization to work for the rights of homosexuals. 4
In 1933, after the Nazi regime had gained power, Hirschfeld’s Institute was destroyed, and in May 1933, German nationalist students burned thousands of books by Jewish, socialist, liberal, and scientific authors, including works by Hirschfeld and his institute. By that time, Hirschfeld had gone into exile and later died in Nice in 1935.
Following the Second World War, in the mid-20th century, gender-affirming surgeries became more widely recognized. In the 1950s, an American transgender woman, Christine Jorgensen, gained international attention after undergoing gender-affirming surgery in Denmark, bringing public awareness to the possibility of medical transition. 5 The Danish endocrinologist Christian Hamburger, who was involved in overseeing Jorgensen’s transition, played a key role in establishing early treatment protocols for transgender care. From Stockholm and Oslo came reports of individuals who were treated in accordance with the methods described by Hamburger and coworkers. 6
In the 1960s and 1970s, medical institutions in the United States and Europe began establishing gender clinics offering gender-affirming healthcare, including hormone therapy and surgery. Harry Benjamin, a German-American physician and endocrinologist, played a pioneering role in the development of gender-affirming healthcare. In the mid-20th century, he was among the first to provide hormone therapy to transgender individuals in the United States and advocated for a medical approach that affirmed individuals’ gender identity. His landmark publication The Transsexual Phenomenon, 7 helped to legitimize gender-affirming healthcare and laid the groundwork for what later became the Standards of Care issued by the World Professional Association for Transgender Health (WPATH). 8
Surgical improvements and advancements in the late 20th and early 21st centuries improved the safety and aesthetic outcomes of gender-affirming procedures. Organizations such as the WPATH, founded in 1979, have played a crucial role in setting medical standards and advocating for access to gender-affirming care. 9
Gender-affirming healthcare has developed at different pace across the Nordic countries, shaped by distinct legal, cultural, and political contexts. While Sweden pioneered legal recognition and regulation of gender-affirming procedures as early as 1972, 10 other Nordic countries have introduced significant reforms in more recent decades. Denmark became the first European country to permit legal gender recognition based on self-identification for individuals aged 18 and above, without requiring a psychiatric diagnosis or surgical intervention, following a legislative reform in 2014. 11 In addition, individuals who identify as non-binary may apply for gender “X” in their passport. 12 In Iceland, the landmark Gender Autonomy Act of 2019 introduced self-identification for individuals aged 15 and older, without mandatory medical or psychiatric evaluation. The law also enabled the use of a third gender marker, “X,” on official documents. 13 Norway implemented its self-identification law in 2016, allowing individuals aged 16 and above to change legal gender without medical prerequisites. From July 2025, Sweden allows legal gender recognition based on self-identification from age 16. 14 In 2023, Finland introduced a law permitting adults to change their legal gender without medical intervention. 15
Historically, all Nordic countries required sterilization as a prerequisite for legal gender recognition in the context of gender-affirming healthcare. Sweden abolished this requirement in 2013, following a court ruling, and Denmark removed it in 2014 as part of its broader legal reform on self-identification. Norway eliminated the sterilization requirement in 2016 when its self-identification law was introduced, followed by Iceland in 2019 with the implementation of the Gender Autonomy Act. Finland was the last Nordic country to remove the sterilization requirement, doing so in 2023, introducing their new law allowing legal gender recognition based solely on self-identification for adults.
Epidemiology
Data from Denmark suggest that approximately 0.06% of the population identify as transgender. 16 In Sweden, the estimated proportion of transgender and non-binary individuals is reported to be around 0.5%.17,18 The Department of National Health and Welfare in Sweden reported that the prevalence of any gender dysphoria diagnoses between 2006 and 2018 was 0.06 % in the population. 19 A large adolescent population survey in Finland reported that 0.6% of participants identified with the opposite sex, and 3.2% identified as non-binary or other gender identities. 20 In Norway, the 2018 Students’ Health and Wellbeing Study reported that approximately 0.2% of respondents identified as transgender or non-binary. 21 Another study by Statistics Norway estimated that close to 0.4% of the adult population identified as transgender.22,23 As of 1 January 2024, the website “Statistics Iceland” 24 reported that out of a total population of 383,726, 159 individuals were registered as “non-binary/other,” representing approximately 0.04% of the population. In Denmark, from 1997 to 2020, a total of 3776 individuals either received a gender dysphoria diagnosis or changed their legal gender. This corresponds to a prevalence of approximately 0.1%. 12 That said, the proportion of individuals identifying as transgender and gender-diverse varies depending on the definition used and the methodologies of different studies.
The estimated proportion of transgender and gender-diverse individuals in the Nordic population aligns with a recent systematic review reporting that transgender identity among adults ranges from 0.3% to 0.5%, and from 1.2% to 2.7% among children and adolescents. 17 Using broader definitions, prevalence estimates increased to 0.5% to 4.5% for adults and 2.5% to 8.4% for children and adolescents. 17
Importantly, not all transgender and gender-diverse individuals seek gender-affirming treatment, and clinical prevalence data based on healthcare utilization are, therefore, generally lower than self-reported identity figures. In addition, prevalence figures based on clinical diagnoses should be interpreted with caution, as barriers to care, such as long waiting times, limited access, and restrictive clinical guidelines, may result in underestimation.
International reports, including data from the Nordic countries, have shown a marked increase in the number of individuals seeking transgender healthcare since the early 2000s, with a notable acceleration around 2012. This trend affects all age groups and both sexes but is particularly pronounced among younger individuals and those assigned female at birth. 17 The reasons for this increase are not yet fully understood, although possible explanations includes improved access to healthcare, greater availability of information through the Internet, and also increasing social awareness and acceptance of transgender and gender-diverse individuals.25 –27
Psychiatric conditions, such as depression and anxiety disorders, and autism spectrum disorders, are more common in transgender individuals compared with the cisgender population.28,29 These individuals also face an increased risk of suicide.16,30,31 The causes of these disparities are multifactorial, including experiences of rejection by their families, denial of care, minority stress, and discrimination.28,30 –32
Diagnosis and classification
In the Nordic Countries, the World Health Organization’s (WHO) diagnostic classification system, the International Classification of Diseases (ICD), is primarily used for diagnosing transgender and gender-diverse individuals in need of treatment. In the most recent version, ICD-11, adopted in 2019 and implemented 2022, conditions related to gender incongruence are no longer considered psychiatric disorders, in contrast to ICD-10. 33 Instead, they are listed under conditions related to sexual and reproductive health, an adjustment introduced with the intention to destigmatize transgender and gender-diverse individuals and improve access to and utilization of transgender healthcare services. 33
Until translations are finalized, ICD-10 remains in use in Finland, Norway, and Sweden. Denmark and Iceland, however, have started implementing ICD-11. Notably, Denmark took an early step in 2017 by introducing the code “DZ768E, contact regarding gender identity condition,” thereby formally relocating these diagnoses outside the psychiatric framework.12,34 While ICD is the primary diagnostic tool in most clinical settings, psychiatrists often use the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, version 5 (DSM-5), which refers to these conditions as Gender Dysphoria, emphasizing the distress that may accompany gender incongruence. In ICD-10, the diagnoses for these conditions are Transsexualism F64.0 or Other Gender Identity Disorders F64.8, the latter is often used for individuals with a non-binary identity.
Gender-affirming healthcare
Gender-affirming treatment aims to reduce gender incongruence and alleviate gender dysphoria. In most cases, this is achieved through a combination of hormone therapy, psychological support, and surgery.
Typically, individuals seeking care for gender incongruence begin by consulting their primary care physician, who refers them to a gender clinic. Due to high demand and limited resources, waiting times for the initial assessment at gender clinics can be long, often ranging from several months to years, depending on the country and region. In most Nordic countries, the first step at the gender clinic involves a comprehensive evaluation by a multidisciplinary team, usually comprising psychiatrists, psychologists, social workers, and endocrinologists. 35 In contrast, in Iceland, the initial assessment is typically conducted by a social worker, who may then refer the individual for further evaluation or treatment if indicated.
The assessment process generally takes several months to years before resulting in a diagnosis of Transsexualism or Other gender identity disorder, according to the ICD-10 classification system. 35 Once a diagnosis is confirmed, a medical evaluation follows to assess eligibility for hormone therapy and/or surgery. Psychological support is offered through the whole process. However, the psychiatric diagnostic framework has been criticized for seeing a transgender identity as a psychiatric disorder that may violate human rights and pose barriers to appropriate healthcare access. This was one of the motivations behind the WHO decision to remove transgender-related diagnoses from the psychiatric chapter in ICD-11. 36
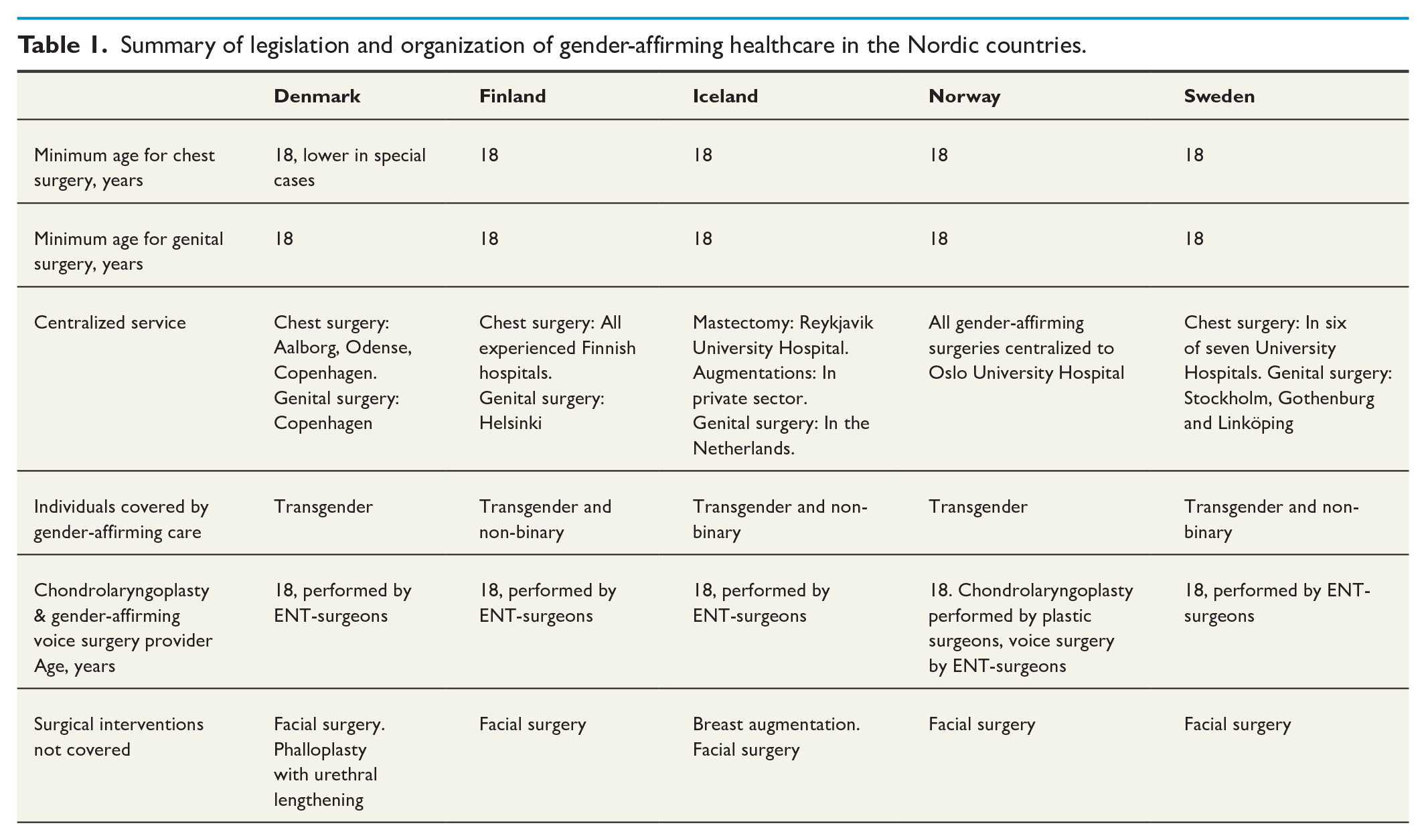
All Nordic countries provide publicly funded transgender healthcare services, covering the entire process from diagnosis to psychiatric, medical, and surgical treatments (Table 1). Hormone therapy is a key gender-affirming medical intervention that induces physical changes aligning with an individual’s gender identity, either masculinizing or feminizing.37,38 It is often a lifelong commitment and requires regular medical monitoring. For transgender youth, puberty-blocking hormones provide an option to delay the onset of puberty.39,40 Although used in rare cases, this intervention allows the individual to explore their gender identity before undergoing permanent physical changes, thus enabling the individual to “pass” easier as their gender identity, as an adult. Before starting hormonal treatment, individuals should be offered fertility preservation procedures. 22
Summary of legislation and organization of gender-affirming healthcare in the Nordic countries.
Mental healthcare and psychological support are also critical components of gender-affirming healthcare.41,42 Among youth, a neuropsychiatric evaluation may form part of the assessment process, given the higher prevalence of conditions such as autism spectrum disorders in this population.28,29
Voice and speech play a central role in gender expression, and many individuals seek voice therapy to develop a voice that better aligns with their gender identity.34,43 –45 Gender-affirming chondrolaryngoplasty (tracheal shave surgery) and voice surgery, are interventions offered to transgender individuals identifying as female. Chondrolaryngoplasty to reduce the size of the thyroid cartilage to create a more feminine appearance. Voice surgery, such as anterior glottic web formation and cricothyroid approximation, aims to feminize the voice.
Some of the most common gender-affirming surgical interventions include breast augmentation for transfeminine, and mastectomy for transmasculine individuals. Gender-affirming genital surgery typically includes vaginoplasty for transfeminine, and phalloplasty or metoidioplasty for transmasculine individuals, respectively. 46
An increasing number of transgender and gender-diverse individuals seek gender-affirming healthcare outside the public healthcare system. Some receive a diagnosis from private providers or online services, obtain hormones through unofficial channels, and in some cases undergo gender-affirming surgeries abroad or through private clinics. Although the full extent of this practice remains poorly documented, in Norway this is understood to reflect dissatisfaction with long waiting times and restrictive criteria in the public healthcare system. 47
Self-initiated hormonal treatment can complicate the psychiatric evaluation and delay diagnosis and access to publicly funded healthcare. Complications after gender-affirming surgery performed in private practices or abroad, may need corrective procedures, for which individuals seek help from public healthcare.
In Sweden, recently updated guidelines for adolescents that restrict the use of hormonal treatment in youth with gender dysphoria and long waiting lists in adult healthcare have led to individuals seeking medical treatment online. Others undergo breast/chest surgery in the private sector and genital surgery abroad.
Scientific evidence supporting improvements in health-related quality of life and gender congruence following gender-affirming surgery is increasing.46,48 –50 Nevertheless, a small proportion of individuals report regretting gender-affirming treatment. Studies indicate regret rates of less than 1%.51 –53 A Swedish study by Dhejne et al. 54 reported that 2.2% of individuals who underwent gender-affirming surgeries between 1960 and 2010 later sought legal detransition or reversal procedures. A more recent Norwegian study followed individuals below the age of 18 who were assigned female at birth and who received gender-affirming hormonal treatment between 2000 and 2020 (N = 783). Of these, 11 (1.4%) no longer identified as transsexual at the end of follow-up. 55
Denmark
Since 2014, individuals aged 18 and older in Denmark can change their legal gender through an administrative procedure. After applying, a 6-month reflection period is required before the change is confirmed and all legal documents are updated. A name change to match one’s gender identity can be made by submitting a declaration to the Family Court, stating that the individual identifies with a different gender than the one assigned at birth. With parental consent, individuals from the age of 15 can also change their legal gender. This does not require a medical or psychiatric diagnosis, hormone treatment, or surgical intervention. Individuals may apply for gender “X” in their passport if they identify as non-binary. Access to gender-affirming healthcare for non-binary individuals however remains limited.
Since 2017, gender incongruence is no longer classified as a psychiatric diagnosis in Denmark. Transgender healthcare is instead provided through gynecological or endocrinological departments, with multidisciplinary teams including psychologists, psychiatrists, and plastic surgeons.
Care is centralized to three centers in Copenhagen, Odense, and Aalborg, with genital surgery performed exclusively in Copenhagen. Current clinical guidelines emphasize that the role of healthcare providers is not to determine if someone is gender incongruent, but to support someone’s gender identity and evaluate the need for gender-affirming treatment. 34
Care for children and adolescents is centralized to the Sexology Clinic at the Psychiatric Centre Copenhagen. Assessment and treatment are carried out in collaboration with the Department of Growth and Reproduction at Rigshospitalet and the Child and Adolescent Psychiatric Centre, Psychiatric Centre Copenhagen.
If a child has not yet reached puberty, counseling is offered to the family. In early puberty (Tanner stage 2), 56 puberty blockers may be initiated following a thorough assessment and multidisciplinary evaluation. From the age of 15, treatment with gender-affirming hormones may be initiated to support the desired gender development. 57 Although Denmark previously had a more permissive approach regarding care of adolescents compared with other Nordic countries, recent years have seen the introduction of more restrictive clinical guidelines, including longer assessment periods and stricter requirements for multidisciplinary review.
To undergo gender-affirming breast/chest surgery in the public healthcare system the individual needs a formal diagnosis of gender incongruence. These procedures are rarely performed before the age 18. Gender-affirming genital surgery is only offered to individuals aged 18 or older.
Finland
As of 2023, Finland reformed its legal gender recognition laws, allowing adults to change their legal gender through self-identification, removing the previous requirement of sterilization.
Gender-affirming healthcare in Finland is centralized to Helsinki and Tampere. To assess gender-affirming medical or surgical treatment, a diagnosis of Transsexualism or Other gender identity disorder is required. Psychiatric diagnostic units are located at the university hospitals of Helsinki and Tampere, with units for adolescents and adults. These units also coordinate referrals to gender-affirming hormonal therapy and surgery. Hormonal treatment is initiated at gynecological clinics in these university hospitals and later continued in primary care.
Gender-affirming chest surgery is not centralized and is provided at hospitals with appropriate expertise. Genital surgery is centralized, though removal of internal reproductive organs can be done in central hospitals. Finland requires prior hormone therapy before eligibility for gender-affirming surgery, typically at least 6 months for chest masculinization and 2–3 years for breast augmentation, and is only offered from the age of 18. 58
For children and adolescents, puberty blockers and gender-affirming hormones may be initiated only after comprehensive assessment and psychiatric evaluation, typically beginning in early puberty for blockers and from the age of 16 for hormones; however, the use of both treatments is very limited. Legal gender recognition for minors is not permitted.
Iceland
The Gender Autonomy Act, passed by the Icelandic Parliament in June 2019, allows individuals to legally define their own gender without the need for a medical diagnosis or treatment, affirming the principle that gender identity is a personal and autonomous decision. Individuals aged 15 and above have the right to change their gender registration in official records, based on their personal gender identity. For those below the age of 15, legal gender change is possible with parental consent, or through an approval by an expert committee.
Iceland follows the ICD-11 classification system and applies an informed consent model for access to gender-affirming healthcare. Individuals seeking treatment are initially seen by a social worker who can refer them for gender-affirming treatment interventions such as hormonal therapy and mastectomy. Psychological assessment may be included, but only with the individual ’s consent. Individuals seeking gender-affirming genital surgery must, however, undergo evaluation by a psychologist before referral. Psychiatrists are not part of the standard care team and individuals requiring psychiatric care are referred separately to mental health services.
Mastectomies are publicly funded and performed from age 18, at the university hospital in Reykjavík. In contrast, breast augmentation is not publicly funded but is performed in private clinics after self-referral, at the individual’s own expense. Gender-affirming genital surgery is publicly founded from 18 years of age and is carried out in one private gender clinic in the Netherlands, as the procedure is not performed in Iceland.
Access to gender-affirming healthcare is available to individuals below 18. Puberty blockers may be initiated at the onset of puberty (Tanner stage 2) following clinical assessment and informed consent from both the individual and their guardians. Gender-affirming hormones treatment may typically begin from the age of 16, depending on individual readiness and medical evaluation. All medical treatment is coordinated through the national university hospital in Reykjavík, where a multidisciplinary team, led by pediatric endocrinologists and supported by social workers and, when needed, psychologists, oversee the care. Psychological support is available but not mandatory, and referrals are made only if the individual requests it or if concerns arise during the process.
Norway
In Norway, the Legal Gender Amendment Act regulates the process of changing legal gender, and since 2016 individuals aged 16 years and older can change their legal gender through an administrative procedure without requiring any medical or surgical interventions. For individuals aged 6–15, parental consent is necessary. No psychiatric evaluation, hormone treatment, or surgery is mandated for legal gender change. 59
There is no minimum legal age for receiving a diagnosis of gender incongruence in Norway. However, assessment in children and adolescents is conducted by specialized pediatric or adolescent gender teams within mental health services and follows strict clinical protocols. Hormone treatment (e.g. puberty blockers or gender-affirming hormones) is considered experimental and subject to strict criteria. According to current Norwegian guidelines, puberty blockers may be offered from Tanner stage 2, following comprehensive interdisciplinary assessment. Gender-affirming hormone treatment is not initiated before the age of 16, and only in exceptional cases where there is a long-standing experience of gender incongruence and a very stable psychosocial situation.
Access to gender-affirming surgeries, such as mastectomy or breast augmentation requires a formal diagnosis of gender incongruence. Candidates must be evaluated and approved by a multidisciplinary team. 60 Individuals who identify as non-binary are however currently not included in the treatment protocols of the national healthcare service and are often denied access to gender-affirming healthcare.
There is no explicit legal age limit for chest surgery, but in practice, these procedures are only performed in individuals aged 18 years or older. Genital gender-affirming surgeries are only offered to individuals aged 18 or older, following an evaluation by a multidisciplinary team.
Transgender healthcare services are centralized in Norway. The national treatment service for gender incongruence is located at Oslo University Hospital. In addition, there are Regional Centers for Gender Incongruence in all four health regions that offer specialized services for individuals experiencing gender incongruence, including assessment, counseling, and ongoing support, primarily for children, adolescents, and young adults, as well as for parents and families. Some centers also provide services for adults. Medical treatment is coordinated with the national treatment service at Oslo university hospital where all gender-affirming surgeries are performed as well.
Access to these Regional Centers for Gender Incongruence is typically arranged via referral from a general practitioner or local mental health services. These centers aim to offer early support, guide individuals and their families through the healthcare system, and ensure safe and individualized care pathways.
Sweden
As of July 2025, Sweden has implemented a new legal framework intended to simplify the process of changing legal gender. Under the updated law, individuals aged 16 and older will be permitted to change their legal gender without a formal diagnosis of gender dysphoria or the requirement of medical or psychiatric treatment, though those below 18 will require legal guardian consent. Nonetheless, Sweden has not adopted a full self-determination model, as seen in other Nordic countries, and individuals will need a medical certificate along with an application to the National Board of Health and Welfare. 14
From July 2025, a new law also regulates access to gender-affirming genital surgery and removal of gonads. Under this new legislation, individuals aged 18 and older, will be eligible for gender-affirming genital surgery and removal of gonads lowering the previous age limit of 23 years. Eligibility requires that the individual has, for a prolonged period, felt that their body does not align with their gender identity and is expected to continue living in accordance with this identity. The revised law will also remove the binary requirement, making gender-affirming genital surgery no longer restricted to binary individuals (thus also include non-binary individuals), and the legal change of gender will no longer be prerequisite. Approval for gender-affirming genital surgery will be granted following evaluation by a multidisciplinary healthcare team. Gender-affirming breast/chest surgery remains unregulated by specific legislation and is accessible from the age of 18.
Since 2024, transgender healthcare has been centralized to three national centers: Gothenburg /Umeå, Linköping/Lund and Stockholm /Uppsala. Multidisciplinary diagnostic assessment for adults and adolescents, initiation of hormonal therapy, voice treatment, gender-affirming vaginoplasty and phalloplasty, and vocal cord surgery, are classified as nationally highly specialized care and may only be performed in one of these centers. The centralization was introduced to improve access to care, strengthen research, and enhance quality control within gender-affirming healthcare.
Diagnostic assessments are conducted by multidisciplinary teams comprising psychiatrists, psychologists, and social workers, based within adult or child and adolescent psychiatry. Following the diagnostic evaluation, individuals may be referred for gender-affirming treatments. The assessment team remains in contact with the individual until the aimed transition is finished. The National Board of Health and Welfare has issued National guidelines of care, both for adults and adolescents.61,62 According to the latest guidelines, the use of puberty blockers to pause pubertal development, as well as use of gender-affirming hormones, is restricted to individuals in a clinical trial, and in exceptional cases, if there has been a long-lasting gender incongruence and a very stable psychosocial situation is prevalent. 61 The new guidelines regarding gender-affirming treatment for youth were constructed because the scientific evidence regarding the safety of hormonal treatment in prepubertal individuals were considered poor. 61
Discussion and future perspectives
Gender-affirming healthcare in the Nordic countries reflect a commitment to advancing human rights, reducing health disparities, and ensuring access to care for transgender and gender-diverse individuals. The region has historically demonstrated leadership in transgender healthcare and legal recognition, as evident by early legislative milestones. Nevertheless, important challenges remain, particularly in developing healthcare models that are inclusive, evidence-based, and responsive to the evolving needs of transgender and gender-diverse individuals.
Across all Nordic countries, there are challenges in balancing the principles of accessibility and autonomy on one hand, and the need for robust evidence-based and cautious clinical decision-making on the other hand, particularly in the care of minors. The evolving protocols mirror broader international debates concerning safety and effectiveness of gender-affirming interventions in adolescents.
Future priorities should focus on reducing waiting times, expanding research efforts, particularly through prospective national cohort studies with long-term follow-up, and developing inclusive models of care that are responsive to the diverse needs of transgender populations. In addition, efforts to improve healthcare provider competence and reduce stigma within healthcare settings are essential for enhancing both the quality and accessibility of gender-affirming healthcare.
Although regret following gender-affirming treatment is rare, it is not non-existent. This highlights the importance of continuous evaluation of clinical practice, shared decision-making, and access to psychological support throughout the transition process, especially for younger people.
In both Norway and Denmark, publicly funded gender-affirming healthcare is largely limited to individuals with a binary transgender identity. This excludes non-binary individuals, who often face barriers to accessing care despite legal recognition in some contexts. Future healthcare policies should ensure that gender-affirming services are inclusive with flexible pathways that reflect the diversity of gender experiences.
Another critical concern is the long waiting times for assessment and treatment. These delays are a source of significant distress and may drive some individuals to seek healthcare outside the public healthcare system, including self-medicating with hormones obtained online, turning to international telehealth providers, or pursuing surgery abroad. Conversely, for some, the waiting period may provide valuable time for reflection and exploration of their gender identity and goals for transition. Balancing timely access with thorough, individualized assessment remains a key challenge.
In summary, despite progress, Nordic gender-affirming care must continue evolving to ensure accessible, inclusive, and evidence-based care for transgender and gender-diverse individuals.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent/Patient consent
N/A.
Clinical trial registration
N/A.