
Abstract
Genital gender-affirming surgery is a crucial yet often overlooked component of gender-affirming care for transgender individuals. Genital gender-affirming surgery is a rapidly evolving field, and it is not uncommon for surgeons — sometimes without prior experience in gender-affirming care — to encounter transgender individuals in clinical practice; hence, it is essential that all healthcare providers possess a foundational understanding of gender-affirming procedures and individual’s needs.
Research has shown that genital gender-affirming surgery significantly improves the quality of life for transgender individuals by aligning their physical characteristics with their gender identity. It can offer substantial satisfaction, both aesthetically and functionally. For transwomen, genital gender-affirming surgery enables them to wear underwear aligned with their gender identity, facilitates sexual function and the potential for vaginal intercourse. For transmen, it provides a more masculine appearance in the groin area, allows for penetrative intercourse with a reconstructed penis (neophallus), and in some cases enables urination while standing when combined with urethral lengthening.
Today, a wide range of surgical options exists for both transwomen and transmen. Thorough preoperative counseling is essential when selecting the most appropriate reconstructive method. Advances in plastic, reconstructive, and microsurgery continue to expand these options, offering greater personalization and improved outcomes. While genital gender-affirming surgery is complex and often irreversible, individuals are generally highly satisfied with the results, particularly when they have realistic expectations prior to surgery.
The aim of this narrative review is to provide an overview of genital gender-affirming surgery from a Nordic perspective. In the Nordic countries, gender-affirming care is highly centralized and integrated into publicly funded healthcare systems. The care programs across these countries share many similarities and are largely comparable in structure and approach.
Keywords
Terminology
Introduction
Gender dysphoria is a persistent condition in which an individual’s gender identity is incongruent with the sex assigned at birth. For individuals with gender dysphoria, their physical appearance does not align with their experienced or expressed gender identity. Gender identity itself can be conceptualized on the normative scale from masculine to feminine, encompassing both cisgender and transgender identities (F64.0 in the International Classification of Diseases, 10th Revision (ICD-10) classification). It can also exist outside this normative framework, referred to as non-binary gender identity (F64.8 in the ICD-10 classification). Although gender dysphoria, historically referred as transsexualism or transgender identity, has traditionally been categorized into psychiatric disorders chapter F in the ICD-10, in version International Classification of Diseases, 11th Revision (ICD-11) it is no longer classified as a disease. 1
Genital gender-affirming surgery is a rapidly growing field that involves several surgical disciplines: reconstructive plastic surgery, urology, gynecology, and sometimes colorectal surgery. The procedures are carried out to relieve gender dysphoria resulting in improving general health through achieving genital appearance and function aligned with the gender identity of the individual. While evidence on the impact of genital surgery on health-related quality of life (HRQoL) remains limited, studies on top surgery have demonstrated improvements in HRQoL following the procedure, although long-term data are scarce.2,3
In non-specialist settings, knowledge about genital gender-affirming surgery remains limited. However, as the transgender population continues to grow, surgeons and other healthcare professionals are increasingly likely to encounter transgender individuals in clinical practice.
In the Nordic countries, genital gender-affirming surgery is highly centralized to university hospitals and is frequently regulated by laws and official guidelines. Although legislation in the Nordic region has become more liberal in allowing individuals to change their legal gender through personal application, genital gender-affirming surgery still requires a formal diagnosis of transsexualism.
The aim of this article is to provide a comprehensive overview of gender-affirming genital surgery for general surgeons, with a particular focus on the Nordic healthcare context, where publicly funded systems, national guidelines, and evolving legal frameworks regulate access to and delivery of care.4,5
History
Genital reconstruction procedures for male-to-female and female-to-male transgender individuals present unique surgical challenges that have continued to evolve since their respective origins in the 19th and 20th centuries.
Feminizing genital surgery was performed as early as the 1930s, although the initial results were not successful. Following the Second World War, significant advancements in vaginoplasty were made in Denmark, where surgeons such as Warnerkros and Bolk performed some of the first gender-affirming vaginoplasties. Their approach included the removal of the testicles, creation of a neovagina, and even early attempts at uterus transplantation. Although the transplantation was unsuccessful, these efforts marked an important milestone in in the development of gender-affirming surgery in the 20th century.6,7
In the mid-1950s, Georges Burou, a gynecologist in Casablanca, and Sir Harold Gillies, assisted by Ralph Millard in England, introduced the modern technique of penile skin inversion, replacing previously used neovaginal grafting methods. 8 The creation of neoclitoris from the glans penis and the development of a more aesthetically refined vulva represented major advancements during the 1970s. Alternative techniques using flaps or intestinal segments were also developed, particularly for individuals who had unsuccessful penile inversion procedures. Pioneers like Burou, who worked discreetly in Casablanca, played a pivotal role in advancing these surgical methods. Their contributions significantly improved the well-being of gender-affirmed individuals by refining surgical techniques. Today, this legacy remains essential for any surgeon interested in performing vaginoplasty. 9
Technical advances in feminizing genital surgery have thus made it possible to safely construct neovagina, vulva, and clitoris for transfeminine individuals. These techniques enable vaginal intercourse, seated voiding, and the potential for sexual pleasure and orgasm, particularly when a portion of the glans penis and its associated sensory nerve bundle is preserved.
Current masculinizing genital surgery techniques are a more recent development and typically involve complex procedures such as tissue transfer from other parts of the body and the use of microsurgical techniques. Although complete penile reconstruction remains challenging, particularly in achieving a functional complication-free urethra, there is also a long history of penile reconstruction. The first documented gender-affirming phalloplasty is somewhat obscure, but early reports include one from Russia in 1936 by Bogoratz, 10 and another by Sir Harold Gillies in 1946. Gilles performed the first known phalloplasty specifically for gender-affirming purposes, rather than post-traumatic reconstruction, using a pedicled skin tube technique, originally developed for the treating war injuries during the First World War. 11 Further reports of gender-affirming phalloplasty appeared in the Netherlands in the late 1950s. 12 A major modern breakthrough came in the 1980s with the introduction of the radial forearm free-flap technique by microsurgery pioneer Professor Koshima, that is now considered the gold standard for phalloplasty. 13
Methods
A comprehensive literature search was conducted to identify relevant articles for this overview. The searches were carried out in collaboration with an information specialist to ensure a systematic and rigorous approach. Databases were queried using selected MeSH terms and keywords related to gender-affirming genital surgery (formerly referred to as sex reassignment surgery). Only articles published in English were considered, with no restrictions on publication year. The selection criteria focused on original research, review articles, and relevant clinical guidelines.
Legislation in the Nordic countries
The criteria for undergoing gender-affirming genital surgery vary across the Nordic countries. While legal gender can be changed by application to the relevant authority in most Nordic countries, gender-affirming genital surgery requires a thorough evaluation period at a specialized psychiatric unit and a diagnosis on transsexualism. Legal gender must be aligned with experienced gender through self-identification. The age limit to change legal gender is 18 years in most of the Nordic countries, though, for example, in Norway individuals aged 16 and older can change their legal gender through an online application.
In all the Nordic countries, the national ID numbers are gender-specific. Therefore, before genital surgery can be planned, the individual′s ID number must correspond with their experienced gender identity, that is, a feminine ID number for transwomen and a masculine one for transmen. In some of the Nordic countries, an additional document from the Ministry of Health or a similar authority, is required to perform gender-affirming surgery. 13 The previous requirement for mandatory sterilization of transgender individuals prior to accessing gender-affirming care and surgery has been luckily abolished in all the Nordic countries.
Feminizing genital surgery
Feminizing gender-affirming surgery is performed to construct a vulva and vagina. This procedure involves the removal of the penis (penectomy) and testicles (orchiectomy), with the genital skin being used to create labia and a vaginal canal (Fig. 1A). The conventional technique, known as penile inversion vaginoplasty, involves inverting the penile skin to form a neovaginal canal (Fig. 1B). Reconstruction of the canal may utilize various tissue sources, including penile skin alone, a combination of penile and scrotal skin grafts, or skin grafts harvested from other donor sites. 14
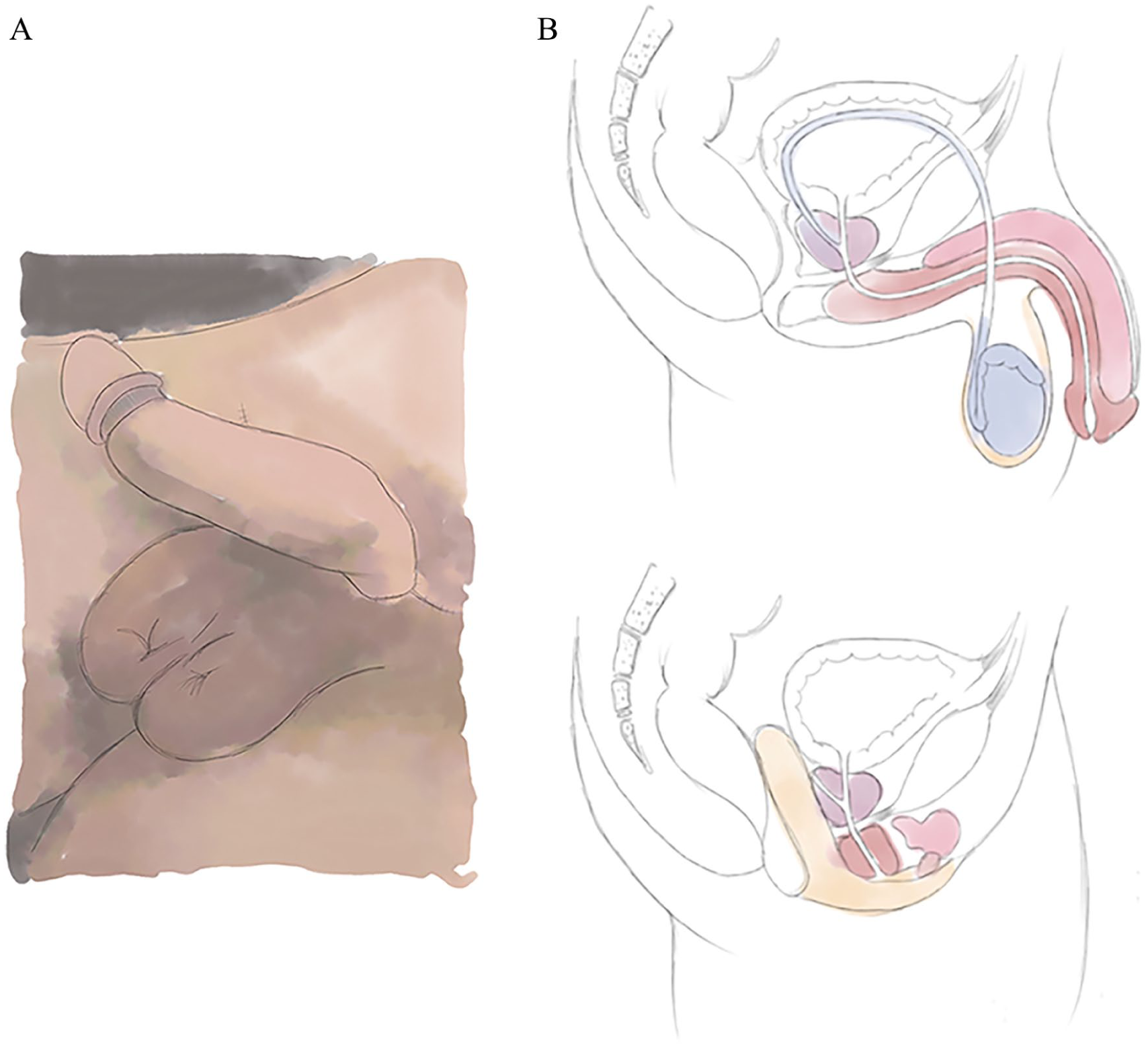
(A) Feminine appearance of genitalia following vaginoplasty. (B) Vaginal canal located between the rectum and prostate in the pelvis of a transfeminine individual after penile inversion vaginoplasty.
During vaginoplasty, the genital area is surgically rearranged to form a vaginal canal, introitus and vulva (external genitalia), including the labial structures. A variation of this procedure, known as vulvaplasty, is designed to create a feminine-appearing external genital area with either a shallow vaginal canal or no vaginal canal at all. 15
Penile inversion vaginoplasty
Traditional vaginoplasty remains a suitable option for most individuals, although several alternative techniques for lining the vaginal canal are now available. Penile inversion vaginoplasty has been considered the gold standard for decades. The procedure involves removal of the testicles (orchiectomy) and erectile tissue (penectomy), while preserving a portion of the glans penis along with the dorsal sensory nerve bundle, which is later used to form the clitoris. A neovaginal cavity is dissected to the pelvic floor, posterior to the prostate and penile root, and anterior to the rectal wall. The resulting vaginal canal typically measures 12 to 20 cm in length and requires regular postoperative dilation with a dilator to prevent stenosis and scar contracture.
The skin of the penile shaft and scrotum is valuable in penile inversion vaginoplasty and is used to create the labia majora and minora (Fig. 1). The labia minora are typically created using preputial, hair-free skin to minimize the risk of hair growth near the clitoris and urethral opening. Various techniques are employed for lining the vaginal canal, using either penile skin alone or in combination with full-thickness scrotal skin grafts. Some surgical centers recommend preoperative laser hair removal of the penile root and scrotum to reduce postoperative hair growth within the vaginal canal.
Certain key anatomical structures of the male pelvis remain after vaginoplasty. To avoid incontinence, the prostate is typically left intact. As a result of feminizing hormone therapy and testosterone suppression, the prostate is usually reduced in size by the time of surgery and its growth tends to be slow in trans women. Prostate cancer in trans women is extremely rare, although a few cases have been reported.14,16
Sigmoid and ileal vaginoplasty
Some individuals lack sufficient penile and scrotal skin, often due to genital hypoplasia resulting from the early initiation of gender-affirming hormone therapy combined with puberty blockers. Previous genital surgeries, such as circumcision, can also contribute to limited skin availability. When available tissue is insufficient, it is typically still possible to construct the vulva and labia; however, the vaginal canal may be shallow, potentially limiting the ability to engage in receptive vaginal intercourse.
In such cases, alternative surgical options are available. A segment of bowel, typically from the sigmoid colon or ileum can be used to construct the vaginal canal (Fig. 2). The bowel wall closely resembles vaginal mucosa, offering a smooth appearance and texture, along with natural mucous production and lubrication. However, sigmoid vaginoplasty presents certain challenges, including odor, excess mucous production, and an increased risk of vaginal prolapse. 17 In addition, diversion colitis can occur.18–20 The sigmoid segment can be harvested either laparoscopically or through a small para Pfannenstiel incision in the left lower abdomen.21,22 This procedure is performed in collaboration with a colorectal surgeon, who harvests the bowel segment. The reconstructive plastic surgeon then inserts the segment into place. The bowel segment remains vascularized through preservation of a segmental artery from the left colon.
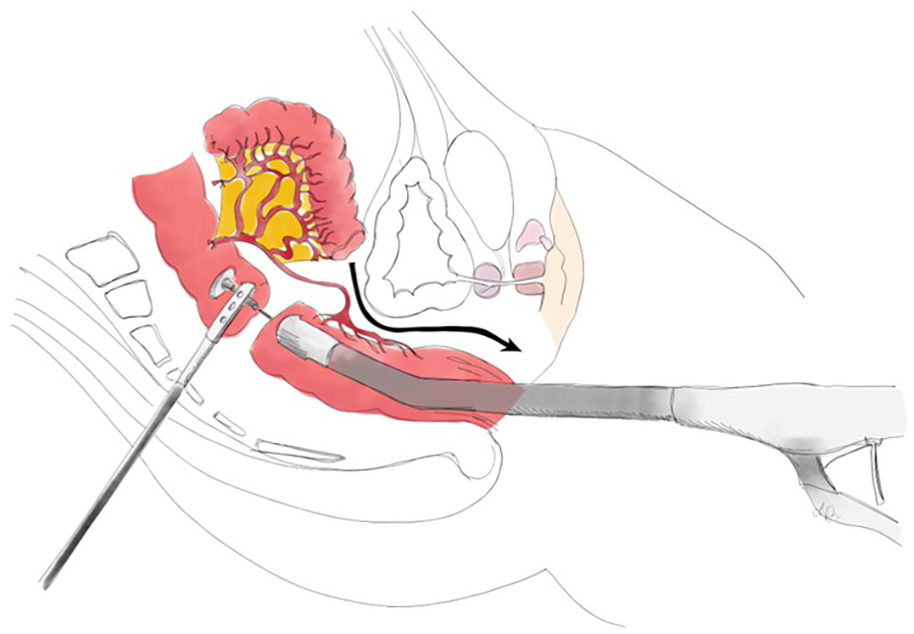
Sigmoid vaginoplasty where bowel segment is harvested laparoscopically and transferred to pelvis to create vaginal canal with mucous lining.
Bowel-based vaginoplasty is generally not the first-line option due to its invasiveness and the significant resources it requires. In the Nordic countries, it is typically reserved for cases where no other viable options exist, or when a previous vaginoplasty has failed, and the individual seeks a second attempt.
It is worth noting that bowel flaps are not used exclusively in transgender individuals. They are part of the broader reconstructive plastic surgery repertoire and are employed in a variety of clinical contexts, including the treatment of vaginal atresia and reconstruction of the esophagus and larynx.23,24
Peritoneal vaginoplasty
Peritoneal vaginoplasty may be a viable option for individuals who lack sufficient genital skin and require a deeper vaginal canal. It can be considered in cases of genital hypoplasia or for revision surgery when the original vaginal canal is shallow or non-functional. 25 Peritoneal tissue can be harvested using open, laparoscopic, or robot-assisted techniques. 26 A pedicled peritoneal flap may be used to create a vaginal canal by pulling it through an opening located posterior to the urinary bladder. Alternatively, the tissue can be applied as a graft. The method is relatively new and not yet in use in the Nordic countries for total vaginal reconstruction, but has been used in Stockholm for partial reconstructions.
Vulvaplasty (zero-depth or shallow vaginoplasty)
Vulvaplasty is a commonly used term for feminizing surgery in which a vaginal canal is either not created or is shallow. Some transfeminine individuals choose to undergo vulvaplasty alone and may experience significant relief from gender dysphoria, even though only the external genitalia (vulva) are feminized. 15 This procedure typically includes orchiectomy, penectomy, and the creation of a feminine-appearing genital region with labia, a neoclitoris, a urethral opening, and a vaginal introitus. Vaginal intercourse is however not possible. Vulvaplasty can be a suitable option for individuals who experience severe dysphoria related to their external genitalia, but who are either not interested in the postoperative dilation required to maintain a neovaginal canal or do not desire vaginal intercourse. 27 In addition, some individuals choose this option due to concerns about potential rectal or urethral complications associated with vaginoplasty.15,28
Orchiectomy
Orchiectomy is typically performed as part of vulvo-vaginoplasty in transfeminine individuals, but can also be carried out as a standalone procedure. Common indications include adverse effects of anti-testosterone therapy and a desire to discontinue hormone blockade through the permanent removal of the testicles. Some individuals remain uncertain about which type of gender-affirming surgery they wish to pursue, but are still motivated to undergo orchiectomy. 29 For these individuals, a staged approach to feminizing surgery, with orchiectomy as an initial step, may be beneficial. Orchiectomy is usually performed as day case procedure, through a small incision along the scrotal raphe to minimize scars in the genital area.30,31 Orchiectomy also facilitates wearing feminine clothing and underwear. 32 After surgery, transfeminine individuals no longer require testosterone-blocking medication that can have side effects such as hot flashes, weight gain, and reduced libido. 33 In addition, there is limited research on the long-term use of these medications for gender-affirming purposes.
Masculinizing genital surgery
Removal of internal female reproductive organs
The first stage of masculinizing genital surgery often involves the removal of internal female reproductive organs, that is, the ovaries and uterus, and in many cases, also the vagina. This procedure is typically performed using laparoscopic technique, except for vaginectomy, which is carried out via a vaginal approach or using a robot-assisted technique. The removal of internal reproductive organs and sterilization is a legal requirement in some of the Nordic countries (e.g. Finland) to qualify for masculinizing genital surgery.
Hysterectomy and oophorectomy are usually performed by a gynecologist as a separate procedure prior to masculinizing genital surgery. Vaginectomy is also a separate procedure, which may follow hysterectomy and is typically also performed by gynecologists.
Many transmasculine individuals do not undergo gender-affirming genital surgery. In such cases, it is important to counsel them to actively seek cervical cancer screening, as they are not routinely invited to national screening programs due to having masculine ID number.34,35
Metoidioplasty
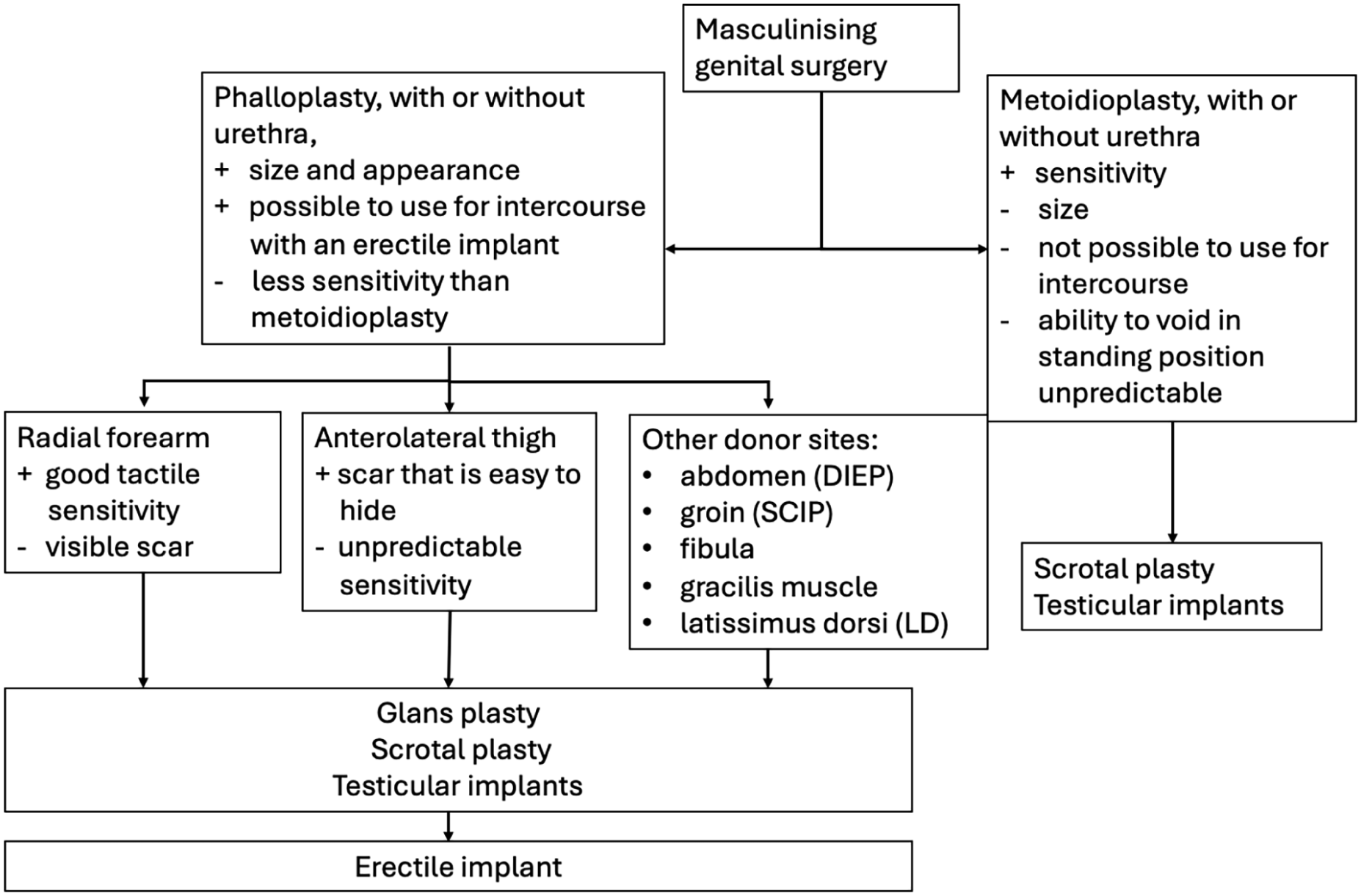
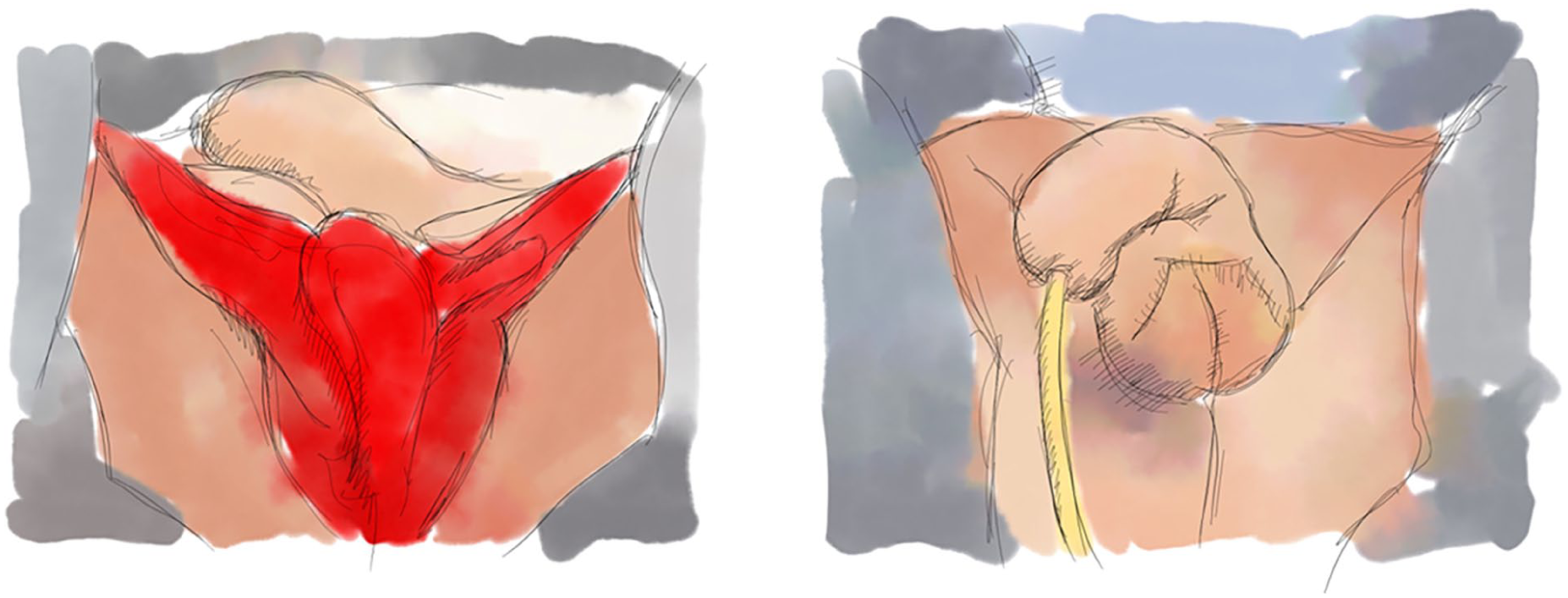
Masculinizing genital surgery is broadly divided into two approaches: metoidioplasty and phalloplasty. Testosterone therapy induces clitoral hypertrophy, causing the clitoris to resemble a glans penis. Metoidioplasty takes advantage of this effect and combines it with surgery in which the crura of the clitoris are released from beneath the pubic bone, allowing the entire clitoris to be protracted. 36 Metoidioplasty may be performed with or without urethral lengthening and is usually combined with a scrotoplasty (Fig. 3).37,38 Compared with phalloplasty, metoidioplasty is technically simpler and associated with fewer risks. The resulting neopenis is typically 3 to 8 cm in length. 39 The ability to void in standing position or engage in penetrative intercourse is unpredictable. However, metoidioplasty offers several advantages, including preserved tactile and erogenous sensation of the glans penis (formerly the hypertrophied clitoris), 40 minimal scarring, and no donor site morbidity. Individuals considering metoidioplasty must receive thorough preoperative counseling to ensure realistic expectations and reduce the risk of postoperative dissatisfaction.
Scrotoplasty is performed using two rhomboid cutaneous flaps from the labia majora to construct a single-pouch scrotum, providing the anatomical structure necessary for the later implantation of testicular implants.
In some Nordic countries, for example, Norway and Denmark, metoidioplasty is the preferred option available to individuals seeking masculinizing genital surgery. The procedure can be performed with or without urethral lengthening, depending on the individual’s preferences and clinical eligibility. In most cases, metoidioplasty is also combined with the insertion of testicular implants, either as a one-stage or two-stage procedure.
Phalloplasty
Phalloplasty refers to masculinizing genital reconstruction in which tissue is used to create a phallus, typically transferred from another part of the body using local, pedicled, or free-flap techniques. The procedure can be performed with or without urethral lengthening—the latter referred to as “shaft-only” phalloplasty.
Phalloplasty is often performed using a two-team approach, allowing the donor flap to be raised simultaneously while the recipient site, including vessels and nerves, is prepared for tissue transfer. Several techniques have been described in the literature, with the free radial forearm flap and anterolateral thigh (ALT) flap being the most commonly used. Both can be combined with urethral lengthening.
There is considerable variation in flap techniques used for phalloplasty across the Nordic countries.
Radial forearm flap phalloplasty
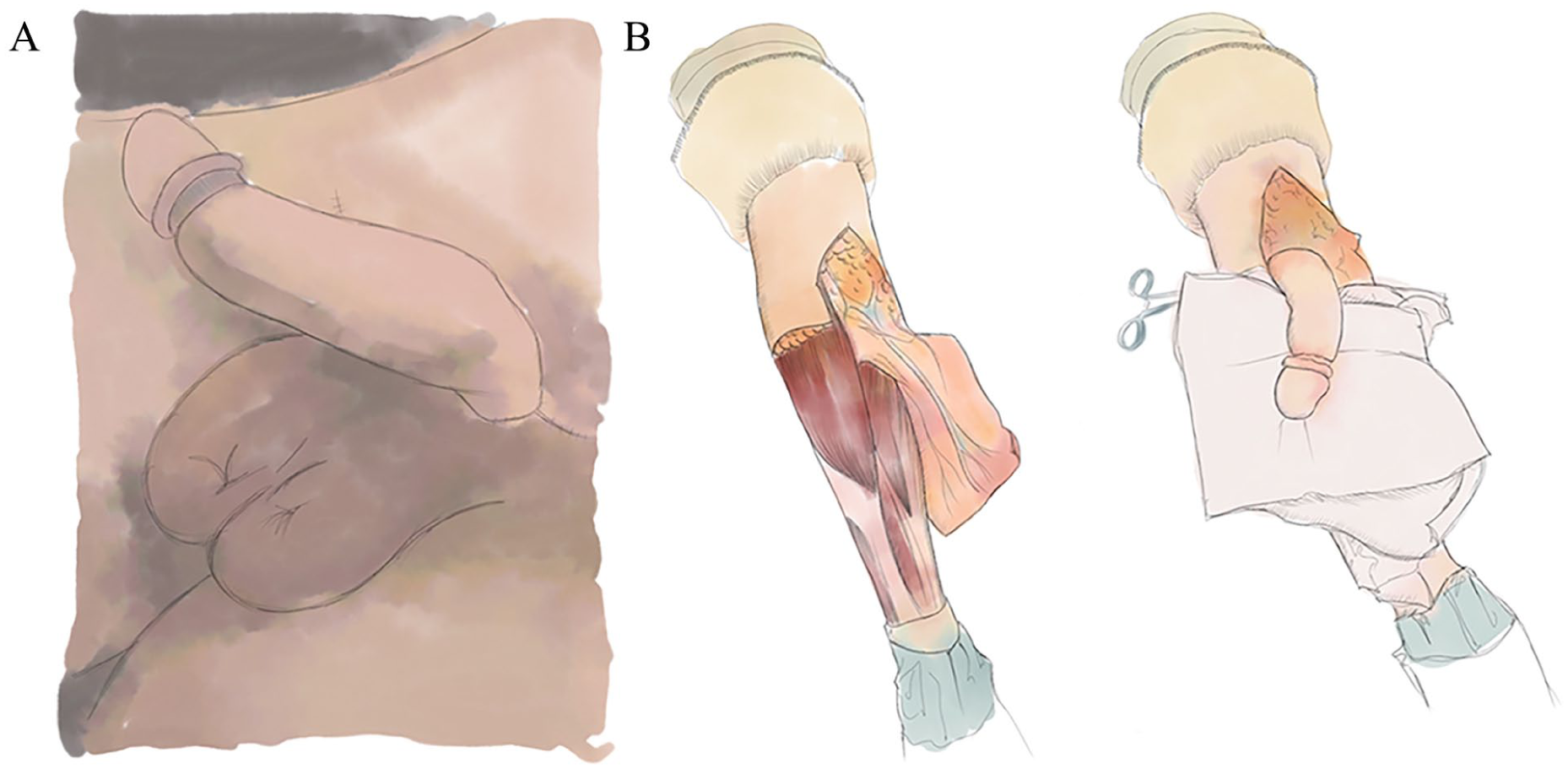
The radial forearm flap is one of the most widely used free flaps in reconstructive plastic surgery (Fig. 4). The radial forearm flap is a fasciocutaneous flap harvested from the volar (anterior) aspect of the forearm. It is perfused via incorporation of the radial artery, providing reliable vascular supply (Fig. 5). Due to its thin and pliable characteristics, the flap is particularly well suited for complex reconstructions in regions requiring delicate contouring and flexibility, such as the head and neck, genital, and upper extremity areas. Since the 1980s, it has also served as the gold standard for gender-affirming phalloplasty. 41 It offers several key advantages: the skin is thin, soft, and pliable, with excellent tactile sensitivity due to the presence of multiple antebrachial sensory nerves located in the subcutaneous layer. These nerves can be included in the flap and co-apted to the ilioinguinal and dorsal clitoral nerves to provide erogenous sensation to the neophallos.42,43 Following preoperative laser hair removal, the radial forearm flap becomes hair free and has highly reliable vascularity. Prior to surgery, an Allen’s test must be performed to confirm sufficient blood flow through the ulnar artery to the palmar arch, ensuring safe harvest of the radial artery.
(A) Postoperative result following radial forearm flap phalloplasty, including scrotoplasty and glans sculpting (coronaplasty). (B) Intraoperative view showing harvesting of the radial forearm flap from antebrachium and in situ tubularization of the flap.
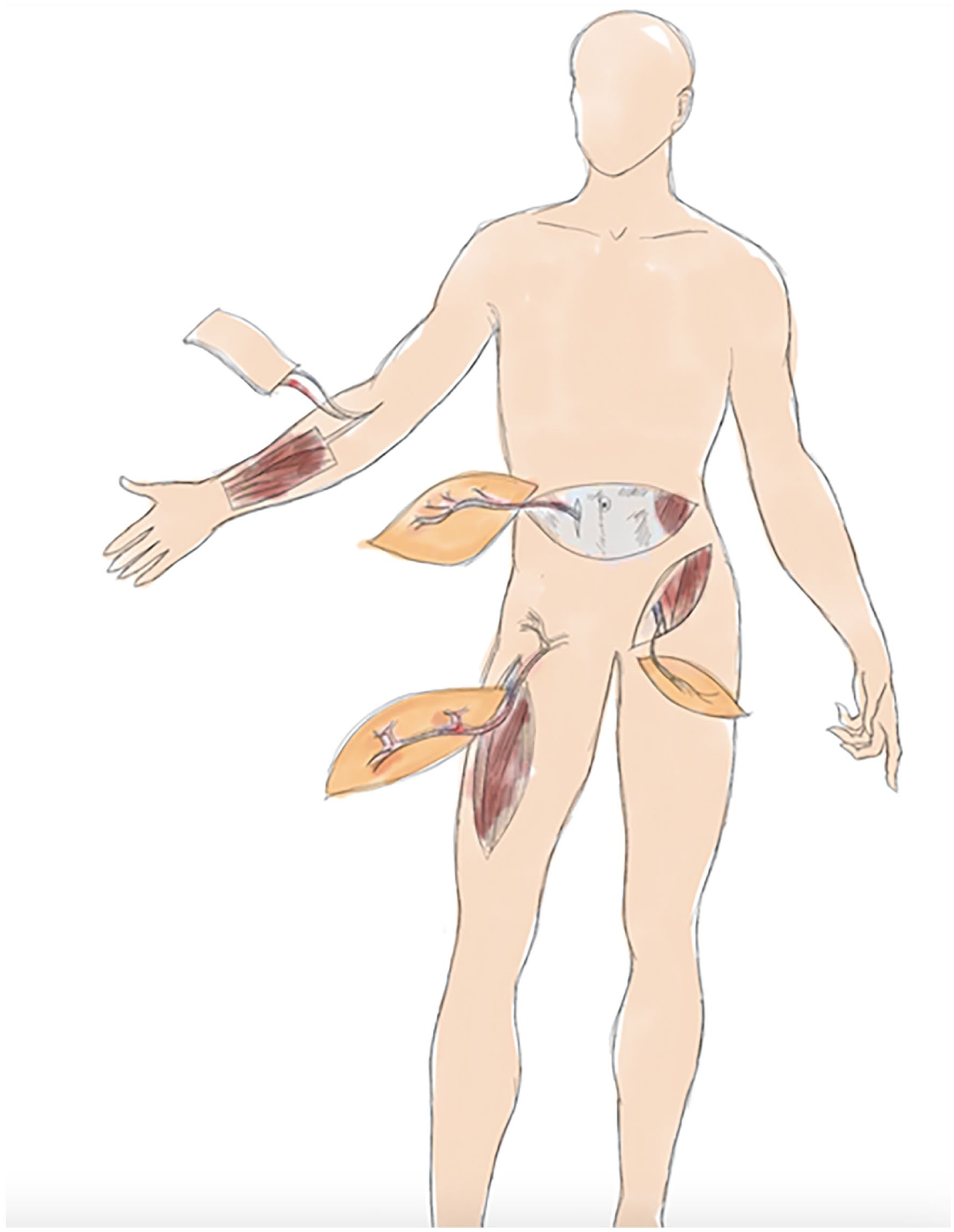
Donor sites for phalloplasty flaps include the radial forearm, deep inferior epigastric perforator (DIEP) flap from the lower abdomen, superficial circumflex iliac artery perforator (SCIP) flap from the groin, and anterolateral thigh (ALT) flap.
From a microsurgical perspective, the radial artery has a favorable caliber for anastomosis with recipient vessels. Common recipient vessels in the genital include the inferior epigastric arteries and the medial branches of the femoral artery, such as the pudendal artery. Venous anastomosis is typically performed between the cephalic vein—included in the flap—and the great saphenous vein. In some cases, the concomitant veins of the radial forearm flap must be anastomosed separately to ensure sufficient venous outflow from the flap. Nerve coaptation is performed using microsurgical suturing techniques combined with tissue glue. Restoration of tactile sensation after nerve coaptation generally takes several months, and may take up to 2 years to fully develop. The radial forearm flap is a favorable option for phalloplasty, as it allows for the harvest of multiple (typically 2–3) antebrachial nerve branches, enabling the creation of a neophallus with the potential for good sensory innervation.
The primary drawback of the radial forearm flap technique is the donor site, typically a 12 × 16 cm area on the volar aspect of the forearm, which is covered with a split-thickness skin graft (Fig. 5). This site can result in a large, visible scar and may lead to functional limitations, reduced mobility, and pain at the scar, particularly around the forearm and wrist. Accidental injury to the superficial branch of the radial nerve can also cause numbness in the thenar region of the hand. The donor site often requires intensive rehabilitation after wound healing to prevent chronic scarring and neuropathic pain. 44 Recent studies suggest that outcomes can be improved using staged grafting, full-thickness skin grafts, or dermal matrix substitutes.45,46 In addition, the appearance of the donor site, due to its large rectangular shape, may be socially stigmatizing. As a result, many individuals choose to cover the area with a tattoo for aesthetic reasons.
ALT flap phalloplasty
The ALT flap is a fasciocutaneous or musculocutaneous flap based on perforators from the descending branch of the lateral circumflex femoral artery (LCFA). It is harvested from the anterolateral aspect of the thigh, typically centered along a line connecting the anterior superior iliac spine (ASIS) to the lateral border of the patella. This flap is another workhorse in reconstructive microsurgery and serves as a valuable option for individuals seeking phalloplasty, particularly for those concerned about visible donor site scarring on the forearm.45,47 ALT flap-based phalloplasty provides good volume and form, and in most cases, the flap can be transferred to the genital region as a pedicled flap. 46 ALT phalloplasty can be performed in several ways: as a single flap (“shaft-only” phalloplasty), as a single flap including a urethral segment 48 or using a multi-flap technique where different flaps are combined to construct the phallos and urethra, often incorporating a thin radial forearm flap. 49 In some cases, the pedicle length of the flap’s vascular supply (i.e. the LCFA and its accompanying veins) is insufficient for tension-free transfer, requiring conversion to a free flap with microsurgical anastomosis. 50 The ALT flap is generally not recommended for individuals with more than one inch of subcutaneous fat in the lateral thigh area, as this may result in an overly bulky neophallus and technical difficulties with tubularization of the flap.
A limitation of this flap is that it typically contains only one sensory nerve, the lateral femoral cutaneous nerve, which can be isolated and harvested for nerve coaptation. 51 The donor site on the thigh is closed using a split-thickness skin graft, and while the resulting scar may be aesthetically unappealing, is generally easily concealed under boxer shorts or trousers.
ALT flap phalloplasty may require additional liposuction at a later stage to achieve a more proportional phallus volume. Coronaplasty (shaping of the glans penis) is typically deferred and performed as a second stage procedure.
Other phalloplasty options
Additional flap options are available for phallus construction. Choosing the most appropriate technique requires a careful assessment of each individual’s priorities and physical characteristics, along with thorough counseling on the expected outcomes associated with each available option (Fig. 6).
Pathway to choose masculinizing genital surgery.
Preferences regarding tactile sensation and donor site scarring are crucial considerations when selecting a flap for phalloplasty. An ideal flap should have at least one identifiable sensory nerve suitable for coaptation with recipient nerves in the genital region. In addition, the flap must have reliable perfusion and vessels of adequate caliber to allow for successful microsurgical anastomosis of both artery and vein(s).
Flaps that meet these criteria include the free latissimus dorsi flap, 52 free fibular flap 53 —which may include fibular bone to facilitate erection—and the pedicled superficial circumflex iliac artery perforator (SCIP) flap. In addition, the deep inferior epigastric perforator (DIEP) flap, which involves harvesting skin and subcutaneous tissue from the lower abdomen, is a well-established option in reconstructive plastic surgery and can also be used for phalloplasty (Fig. 5).
In Finland, there is a tradition of more than 20 years of performing phalloplasty using the so-called triple flap method. In this technique, urethral lengthening is achieved using a superficial circumflex iliac perforator artery (SCIP) flap harvested the from groin, while the shaft of phallos is constructed using bilateral gracilis muscle flaps covered with split-thickness skin grafts. A potential outcome of this method is a paradoxical erection phenomenon, caused by muscle contraction when the motor nerves of the gracilis muscles are preserved. 54
There is considerable variation in flap techniques used for phalloplasty across the Nordic countries. In Norway for example, phalloplasty has previously been offered using a variety of techniques, including both free flaps and local flaps. In recent years, however, phalloplasty has not been performed routinely. This is primarily due to limited surgical capacity and a relatively high rate of complications and patient dissatisfaction.
Scrotoplasty, coronaplasty and testicular and erectile implants
The aesthetic outcomes of metoidioplasty and phalloplasty can be enhanced through additional genital reconstruction to achieve a more natural appearance of the male external genitalia. Scrotoplasty is typically performed using two rhomboid cutaneous flaps harvested from the labia majora, which are sutured together to form a skin pouch resembling the scrotum (Fig. 3). From the embryological perspective, the labia majora and scrotum share the same origin, making this technique particularly effective in creating a natural-looking scrotum with thick, hair-bearing skin. Scrotoplasty is performed first, and the implantation of silicone testicular implants is carried out later as a separate surgical procedure, once the scrotal tissue has healed and is ready to accommodate the implants. 55
Testicular implants are typically made of silicone and can be implanted as a standalone procedure or during the same operation as the placement of an erectile device, such as a silicone rod or an inflatable pump system. 56 Risks of testicular implants include infection, migration, extrusion, or patient dissatisfaction with size or symmetry. Selection of appropriate implant size and symmetry of the neoscrotum are important for optimal outcomes. Implants come in size 17 and 27 cc.
Erectile implants are typically placed in the neophallus following phalloplasty, where sufficient bulk and internal support can accommodate the device. These implants enable rigidity sufficient for penetrative intercourse, a goal for many individuals undergoing genital reconstruction. Inflatable implants provide a more natural appearance and the ability to control rigidity. Malleable (semi-rigid) implants are mechanically simpler but remain firm at all times. Implantation is typically delayed for 6–12 months after phalloplasty to allow for full healing and tissue stabilization. Erectile devices are associated with potential complications, including prosthesis infection, malrotation, and erosion through the phallos. 57
Coronaplasty (also referred to as glansplasty) (Fig. 7) is an aesthetic refinement performed to enhance the natural appearance of the phallus. The glans penis is typically sculpted using the Norfolk technique, which is combined with a split-thickness skin graft to create a defined sulcus coronalis. 58

Norfolk coronaplasty involves elevating the skin edge of the glans corona and reconstructing the sulcus coronalis using a split-thickness skin graft.
Complications of genital gender-affirming surgery
Gender-affirming genital surgery is a subspeciality of reconstructive surgery that involves operating on physiologically healthy and well-functioning genitalia using irreversible techniques. Most individuals undergoing these procedures are young and somatically healthy, making the tolerance for major complications extremely low. Given that these surgeries aim to improve quality of life rather than address urgent medical conditions, surgical safety and precision are paramount.
Common complications associated with genital surgery include general surgical issues such as wound infections, postoperative bleeding, hematoma, and wound dehiscence. Hypergranulation is a frequent feature of wound healing in genitalia, where conditions may be moist. 59 Despite the proximity of the surgical field to the urinary tract and anal opening, severe infectious complications are rare, owing to the rich vascular supply of the genital area. Even larger cases of wound dehiscence typically respond well to conservative management, provided that dressing changes are appropriately performed and local infections are treated with antibiotics.
The pelvic floor is a complex anatomical region, with multiple physiological and sexual functions. When performing surgery in this area, there is a risk of urethral or rectal injury and risk for iatrogenic trauma to larger vessels. This risk is particularly relevant in vaginoplasty, where a critical step involves dissecting the neovaginal canal posterior to the penile root and prostate and anterior to the rectal wall. Recent studies show that the risk of both rectal and urethral injury during vaginoplasty ranges from 0.5% to 2%. 60 Most of these iatrogenic injuries can be successfully repaired, especially when identified intraoperatively. 61 However, if such injuries go unrecognized during surgery, there is an increased risk of developing rectovaginal or urethrovaginal fistulas. 62 A rectovaginal fistula may necessitate the creation of a temporary stoma to allow for healing, while vesicovaginal or urethrovaginal fistulas may require a temporary suprapubic catheter to allow the affected area to heal. 63 Fistulas often hinder the normal dilation protocol after vaginoplasty and may lead to severe vaginal stenosis and the need for revision surgery. 64
The neural structures of the clitoris and glans penis are also vulnerable to surgical complications. There is a risk of postoperative loss of tactile sensation and difficulty achieving orgasm following gender-affirming genital surgery, although the risk of complete loss of orgasmic function appears to be low. 65 To minimize these potentially avoidable and sometimes irreversible outcomes, it is essential to perform meticulous dissection of neural structures and to have detailed anatomical knowledge of the genital region. 66
Urethral complications in gender-affirming genital surgery include stenosis and fistula formation. In feminizing vaginoplasty there is a risk of meatal stenosis due to the shortening of the native urethra. In addition, there is a risk of iatrogenic fistula particularly at the bulbar level, where the urethra traverses the prostate when dissecting the vaginal cavity. 67
Urethral complication rates, particularly in phalloplasty, are relatively high, up to 50%. Therefore, individuals should be thoroughly informed during preoperative counseling about the risks and benefits of urethral lengthening.68,69 To avoid the high risks associated with urethral lengthening, shaft-only phalloplasty can be offered as an alternative. 70 At present in Nordic countries, only Finland provides phalloplasty with urethral lengthening as a standard procedure. In Sweden, urethral lengthening is provided only in terms of scientific studies and the rest of Nordic countries are even more restrictive. Some studies suggest that performing staged phalloplasty, in which the anastomosis between the native and reconstructed urethra is delayed until a second surgical stage, may help reduce the risk of late urethral stenosis and fistula formation. 71
Microsurgical complications in phalloplasty primarily include venous congestion and thrombosis, which can occur in either the venous or arterial side of the flap circulation. Due to these risks, phalloplasty flaps are closely monitored, typically hourly during the first 24 h, followed by progressively less frequent assessments. If thrombosis is suspected, immediate revision surgery is necessary to salvage the flap. Failure to restore circulation will result in complete or partial necrosis of the phallus.
Gender-affirming care can have significant and often irreversible implications for fertility. As many forms of gender-affirming genital surgery are sterilizing, fertility preservation counseling and options, such as sperm or oocyte cryopreservation, should be routinely offered and discussed prior to surgery. 72 All the Nordic countries offer this counseling before the debut of hormone treatment.
Clinical outcomes and patient-reported experiences
Gender-affirming surgery is a relatively new and evolving surgical subspeciality, encompassing a range of techniques for both top (chest) and genital procedures. For masculinizing or feminizing top surgery, as well as feminizing genital surgery (vaginoplasty), several well-established surgical approaches exist. However, masculinizing genital surgery remains particularly challenging. From a surgical perspective, achieving a safe and functional phalloplasty, without major complications at the recipient site or donor site, continues to be one of the most significant technical and clinical concerns of the field.
Several studies have been published investigating the impact of surgical treatment on long-term outcomes and HRQoL in individuals with gender dysphoria. Only a limited number of these are however prospective in design and report long-term follow-up data.73,74 Furthermore, the field has been criticized for a lack of evaluation tools and patient-reported outcome measures (PROMs) that are both well-adapted and validated specifically for populations with gender dysphoria.75,76 Historically, most PROMs used in gender-affirming care were developed for cisgender patients, often in the context of breast cancer or aesthetic surgery. In recent years, however, new instruments and questionnaires tailored to the unique experiences and needs of individuals with gender dysphoria have been introduced into both clinical practice and research settings.77,78
Detransition
A small minority of transgender individuals experience regret related to their gender identity or express a desire to detransition, a process that may involve social, medical, and/or surgical reversal of aspects of a previous gender-affirming transition. A Swedish study reported that 2.2% of individuals who had undergone gender-affirming surgeries later sought detransition or reversal procedures. 79 Similarly, a Danish national cohort study found a regret rate of 0.06% per person-year among individuals who had undergone gender-affirming surgeries. 80 In addition to identity-related regret, some individuals report dissatisfaction with specific procedures or outcomes that do not meet their expectations, whether aesthetic, functional or both. It is therefore essential to distinguish between a desire for detransition and dissatisfaction with surgical results or overall care. While case reports have described detransition following top surgery (e.g. breast reconstruction after gender-affirming mastectomy), genital detransition remains extremely rare, with only limited cases described in the literature to date.81,82
Although the overall rates of regret and detransition are low, these outcomes are clinically significant and underscore the importance of comprehensive preoperative assessment and ongoing postoperative support for individuals undergoing gender-affirming treatment.
Conclusions and future perspectives
Genital gender-affirming surgery is a relatively new and rapidly advancing subspeciality within reconstructive surgery. Its primary aim is to construct genital anatomy that aligns with an individual’s gender identity, thereby alleviating genital-related dysphoria. It is essential to recognize that gender identity is not strictly binary, as is often assumed within cisnormative frameworks, but rather exists along a spectrum. The role of the gender-affirming surgeon is not to serve as a gatekeeper, but to act as a professional and empathetic guide, supporting individuals throughout the process. A key responsibility of the surgeon is to provide comprehensive preoperative counseling, including a thorough discussion of potential complications, functional limitations, and realistic expectations regarding surgical outcomes. Clear, honest communication about the irreversible nature of most gender-affirming procedures is also critical to informed consent and long-term patient satisfaction.
Overall, genital gender-affirming surgery is associated with a low rate of severe complications and has been shown to significantly improve both psychological well-being and physical comfort. For many individuals, achieving congruence between their body and gender identity brings substantial relief and enables them to shift their focus toward broader life goals and future aspirations. While evidence already supports improvements in HRQoL following top surgery, the data specifically addressing long-term outcomes of gender-affirming genital surgery remain limited.
From the individual′s perspective, the gender-affirming care pathway, from initial referral to a diagnostic psychiatric outpatient clinic, through the initiation of hormonal treatment, and ultimately gender-affirming surgery, is often a lengthy multi-year process. Limited healthcare resources and a shortage of specialized healthcare professionals contribute to extended waiting times for surgical interventions. During this period, continuous psychological support and appropriate clinical follow-up are essential to safeguard mental health and promote overall well- being.
To date, the majority of published studies in the field of gender-affirming surgery are single-center and retrospective in design. Prospective, systematic follow-up remains limited, and follow-up durations are often insufficient to capture long-term outcomes or late-onset complications such as urethral stenosis following urethral lengthening or neovaginal stenosis due to inadequate adherence to dilation protocols.
The Nordic countries are currently at the forefront of care for individuals with gender dysphoria. Diagnostics services have been centralized, and national guidelines for both diagnosis and treatment have been developed to ensure standardized clinical pathways. In addition, national registers have been established to monitor treatment outcomes and support the ongoing quality assurance of gender-affirming care.
Looking ahead, key challenges include the ongoing refinement and development of safer surgical techniques, along with strategies to recruit and retain dedicated plastic surgeons and psychiatrists in the field. These efforts are critical to reducing waiting times and ensuring timely, equitable access to high-quality gender-affirming surgical care.
In the current global climate, where access to gender-affirming care is increasingly threatened by regressive political and legislative movements, it is more important than ever that the Nordic countries continue to uphold and advance the provision of gender-affirming treatments. By maintaining a commitment to evidence-based, compassionate, and equitable care, the Nordic region serves as a critical example of how to safeguard the rights and well-being of transgender and gender-diverse individuals.
Footnotes
Author contributions
Illustration drawn by Lucy Bai.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a research grant from Päivikki and Sakari Sohlberg Foundation.