
Abstract
Background and aims:
Acute kidney injury (AKI) is a key contributor to multiorgan dysfunction and mortality in ruptured abdominal aortic aneurysm (rAAA). Intra-abdominal hypertension and abdominal compartment syndrome (ACS), complications potentially resulting in AKI, can be prevented or managed with open abdomen treatment (OAT). Using consensus-based definitions, this study characterizes AKI in rAAA patients managed with OAT and examines the impact of abdominal wall closure on renal function.
Methods:
A single-center observational cohort study including all consecutive patients treated with OAT after open surgical repair for rAAA from September 2009 to January 2024. AKI was diagnosed and staged based on urine output (UO) and S-creatinine (SCr) as defined by the KDIGO classification, reassessed at closure of the abdomen and at discharge.
Results:
Seventy-three patients (mean age 73 years, 85% male) received OAT, prophylactically in 63 (85%) and due to ACS in 11 (15%). AKI occurred in 71 patients (97%) at a median of 2 (IQR, 2–3) days of admittance; 22 patients (30%) had stage 3 AKI, including 13 (18%) needing renal replacement therapy. The multivariable logistic regression showed SCr at admittance (p = .034) and perioperative diuresis (p = .018) as predictors of stage 3 AKI. The UO criterion diagnosed more patients than SCr alone (p = .001). Abdominal closure did not aggravate kidney function. In AKI stage 3, 90-day survival was 46% versus 80% in AKI stage 1 and 2 (p = .008). Forty-seven out of 51 survivors (92%) had resolution of their AKI before discharge.
Conclusions:
Defined by KDIGO, AKI developed in 71/73 (97%) of rAAA patients with OAT after surgical repair. UO was the most sensitive parameter. AKI was diagnosed at median 2 days of admittance and was transient in majority of survivors. There was no aggravation of kidney function at delayed primary abdominal closure.
Keywords
Context and Relevance
Acute kidney failure (AKI) is one of the main complications and contributors to mortality in patients with ruptured abdominal aortic aneurysms (rAAA). However, existing studies on AKI and rAAA apply inconsistent classifications and limited evidence exists regarding AKI in patients with rAAA undergoing open abdomen treatment (OAT). This study applied KDIGO consensus criteria to a high-risk patient population undergoing OAT to prevent or treat abdominal compartment syndrome following open rAAA repair. AKI was diagnosed in 71/73 (97%) of patients; stage 3 AKI occurred in 22/73 (30%) with significantly higher mortality (p = .008). Occurrence and significant predictors of AKI were observed early after admittance. Accurate use of consensus criteria increases AKI detection, may facilitate earlier diagnosis, and improve outcomes in rAAA patients.
Introduction
Acute kidney injury (AKI) is one of the main complications after ruptured abdominal aortic aneurysm (rAAA) and is associated with increased mortality.1–3 Severe AKI is linked to reduced long-term survival even after resolution.4–6 Previous studies of rAAA have reported incidence rates of 50%–74% for AKI and 15%–36% for severe AKI.2,7 The etiology of AKI following rAAA is multifaceted and includes prerenal factors, for example, circulatory shock, intraoperative suprarenal clamping or the application of aortic occlusion balloons,8–10 and renal factors such as nephrotoxic drugs and contrast agents. Pre-existing kidney disease, cardiac disease or hypertension, are associated with an increased risk of AKI and are frequent among these patients.11,12 Moreover, serious ischemic complications in the aftermath of rAAA are associated with acute renal insufficiency.12–15
Raised intra-abdominal pressure (IAP) is common among rAAA patients due to intra-abdominal edema and hematoma. 11 Intra-abdominal hypertension (IAH), defined as IAP over 12 mmHg, 16 can cause kidney injury. The combination of even moderate IAH and AKI has been associated with increased mortality.17,18 Several mechanisms contribute, such as a decline in renal perfusion pressure, reduced renal filtration, and compression of the renal parenchyma and vasculature. 16 If left untreated, IAH can lead to abdominal compartment syndrome (ACS), defined as sustained IAP ⩾ 20 mmHg and new onset of organ dysfunction or failure, 16 where the kidney often is the initial organ affected. 19 Current European guidelines state that IAP > 20 mmHg occurs in approximately half of the patients after rAAA and report the incidence of ACS to be 7%–20%. 9 In patients with rAAA, ACS may require open abdomen treatment (OAT).
Few studies examine AKI in patients with rAAA and OAT and existing studies on rAAA and kidney injury use inconsistent classifications, 20 such as Aneurysm Renal Injury Score (ARISe), 2 The Risk, Injury, Failure, Loss of kidney function and end-stage kidney disease (RIFLE),7,21 or Acute Kidney Injury Network (AKIN). 3
Since 2012, The Kidney Disease Improving Global Outcomes (KDIGO) consensus guidelines have been recommended, 22 including both urine output (UO) and serum creatinine (SCr) criteria, to more accurately diagnose and estimate the incidence of AKI.22,23
The primary aim of this study was to describe AKI by KDIGO among patients who, according to Clinical Practice Guidelines,9,16 require OAT after surgery for rAAA. A secondary aim was to investigate whether closure of the abdomen affects renal function.
Material and methods
Study design, inclusion, and ethics
This observational cohort study was conducted at a tertiary academic hospital in central Norway, with a population of 730,000 in a primary catchment area without population-based screening for AAA. In the period of September 2009 until January 2024, all consecutively treated patients who survived open surgical repair (OSR) for rAAA and received OAT were included. Only five patients were treated with OAT following endovascular aortic repair (EVAR); these were not included in the study. Patients included from 2009 to 2021 have been previously reported concerning OAT, but not with a focus on AKI. 24 The end of follow-up was November 2024, ensuring an observed 90-day follow-up for all included patients.
The Regional Committee for Medical and Research Ethics stated that the study did not fall under their legislation (255364), waiving informed consent, and the Department of Surgery’s research committee granted ethical approval. The study results are reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement 25 and can be found in the supplemental material.
Study population
The study population was identified by systematically searching for the procedure and diagnosis coding in the electronic hospital records and the Norwegian Vascular Surgery Registry (NORKAR), a national quality improvement registry which register all AAA operations prospectively.
Patients received 3000 IU heparin intravenously after aortic clamping and low-molecular-weight heparin 4000 IU was instituted 6 h postoperatively.
OAT was established prophylactically at the surgeon’s discretion when clinically suspected IAH at attempted closure of the abdominal wall or when ACS was diagnosed in the postoperative period. IAP was obtained routinely six times/24 h via trans-bladder pressure monitoring in the intensive care unit (ICU). 26
All patients received OAT with vacuum-assisted wound closure and mesh-mediated fascial traction27,28 with a continuous negative pressure of 25–125 mmHg and mesh-traction established at the first dressing change 24–48 h after primary surgery and received a second-generation cephalosporine intravenously as aortic graft protection.
The patients had standard intensive care therapy to maintain a mean arterial pressure (MAP) > 65 mmHg and all patients had mechanical ventilatory support in the early phase of OAT. Loss of consciousness before surgery, systolic blood pressure at admittance, and episodes of MAP < 65 mm Hg for a duration ⩾ 15 min were recorded throughout the stay at the ICU to assess the effect of hypotension.
AKI assessment and definitions
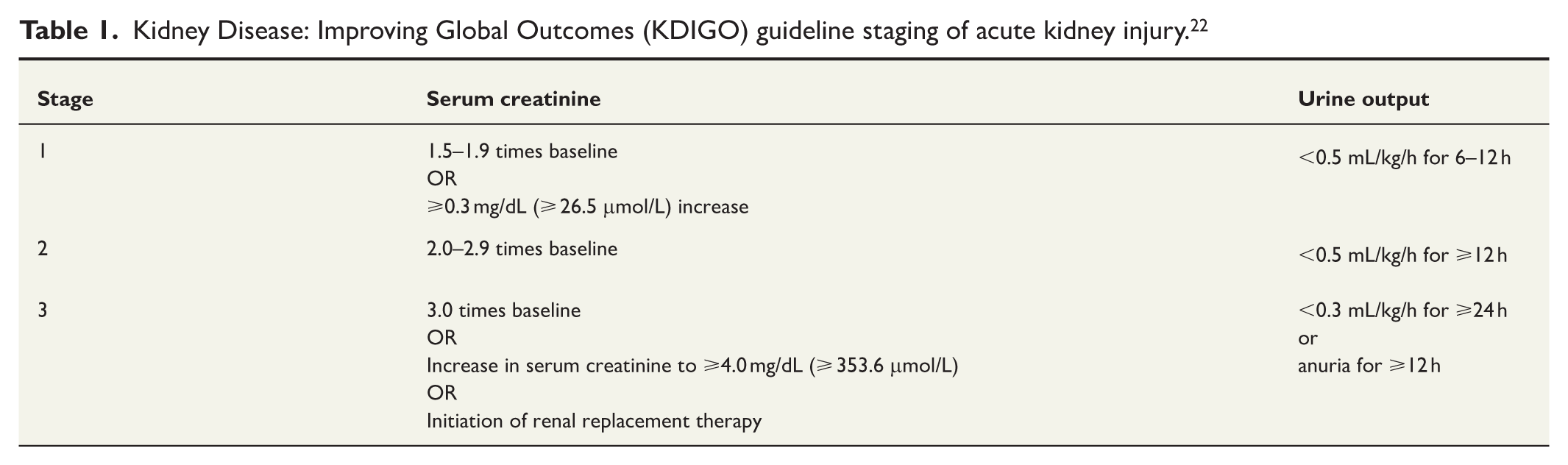
AKI was diagnosed according to KDIGO guidelines (Table 1) as any of the following: increase in SCr 1.5–1.9 times from baseline, increase in SCr by ⩾ 26.5 μmol/L or UO < 0.5 mL/kg/h for 6 h (Stage 1), increase in SCr 2.0–2.9 times baseline or UO < 0.5 mL/kg/h for ⩾ 12 h (Stage 2), increase in SCr 3.0 times baseline or SCr to ⩾ 4.0 mg/dL (⩾ 353.6 µmol/L) or initiation of renal replacement therapy or UO < 0.3 mL/kg/h for ⩾ 24 h or anuria for ⩾ 12 h (Stage 3). All patients were diagnosed at peak AKI. Throughout the ICU admittance, hourly UO and daily SCr were assessed, and the average hourly UO was calculated for any consecutive 6 and 12 h.
Kidney Disease: Improving Global Outcomes (KDIGO) guideline staging of acute kidney injury. 22
Baseline SCr concentration was defined as the last SCr measured 365 to 1 day before the index event, in accordance with KDIGO guidelines. 29 If no such measure existed, SCr obtained at admittance was used to diagnose AKI.
Resolution of AKI was defined as a combination of UO > 0.5 mL/kg/h for 12 h and/or SCr returning to less than 1.5 times baseline. UO data from the first 24 h after closure was available for 37 of 56 patients. Only SCr could be obtained after transferal from the ICU. Kidney function at discharge was defined as the last obtained SCr during hospitalization. Patients’ need for long-term renal replacement therapy (RRT) was evaluated no earlier than 90 days after discharge.
Abdominal compartment syndrome (ACS) was defined as sustained IAP ⩾ 20 mmHg and new onset of organ dysfunction or failure. 16
Data collection
Data on demographics, comorbidities, treatment, length of stay, complications, mortality, and all data from the perioperative phase and intensive care stay were retrieved from the electronic hospital records (Doculive EPR, Siemens, Cerner Corp./Picis 8.0/8.2, Picis Clinical Solutions, Inc./Helseplattformen Epic Hyperspace®). Data, including UO and SCr, were recorded prospectively, and case records were reviewed retrospectively. All data were manually validated and verified.
Statistical analysis
Depending on the distribution of data, continuous variables are reported as the median and interquartile range (IQR) or mean and standard deviation, and categorical variables as numbers and percentages. The independent samples T-test or Mann–Whitney U test were used to compare continuous variables, and the chi-square test or Fisher’s exact test was used to compare proportions. Wilcoxon signed-rank test was used to compare changes in SCr over time. When examining changes in SCr at the time of closure of the abdomen, patients on RRT were excluded. A p-value < .05 was regarded as statistically significant, and all p-values were two-sided. No corrections were done for multiple testing. Multivariable logistic regression was used to explore the etiology and risk factors of AKI stage 3, with all continuous variables modeled as linear predictors and R2 calculated ad modum McFadden.
Statistical analysis was performed using SPSS Statistics version 29.0.1 and version 30 (IBM Corp., Armonk, NY, USA) and R version 4.3.3 (R Core Team, 2025).
Results
Patient population
In the study period, 220 patients were treated for rAAA, of whom 56 (25%) had EVAR and 164 (75%) had OSR. Seventy-three patients had OAT after OSR and were included in the study. Prophylactic OAT was established in 62/73 (85%), and the remaining 11/73 (15%) resulted from ACS. Figure 1 shows the flowchart of the study population.
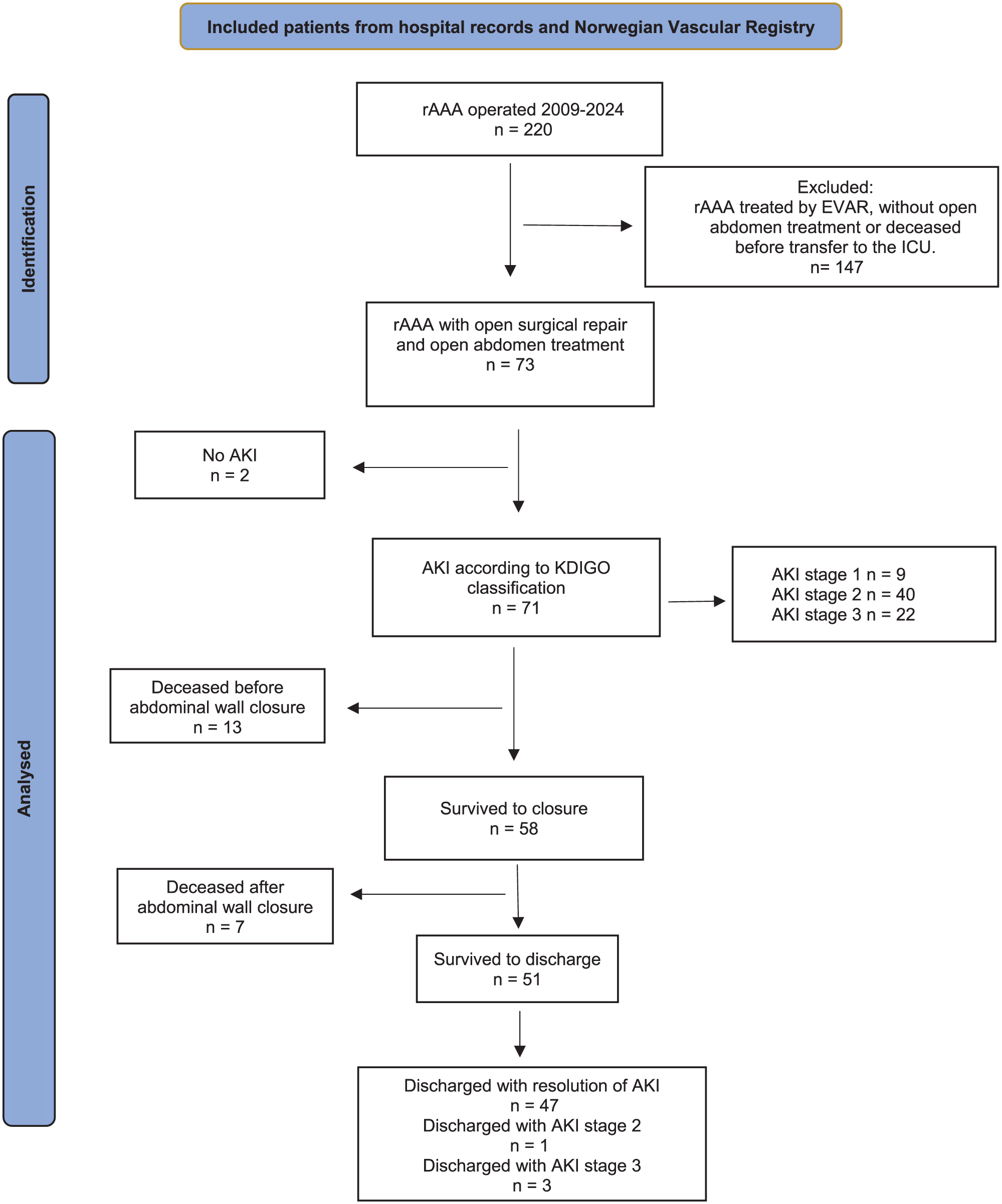
Flowchart of the study population. A total of 220 patients had surgery for ruptured abdominal aortic aneurysm (rAAA) during the study period, 73 patients had open surgical repair and open abdomen treatment and were included in the study.
The mean age was 73 (± 6.79) years, and 85% were male. The most common comorbidities were hypertension 28/73 (38%) and cardiac disease 30/73 (41%). Only one patient had known diabetes. Sixty-three (86%) patients had an infrarenal aneurysm; ten (14%) had a juxtarenal aneurysm and suprarenal clamping occurred in 20 (27%) of the patients. Table 2 presents the clinical characteristics of the study population.
Baseline characteristics of the 73 study patients grouped by KDIGO classification of AKI in combined stages 1–2 and stage 3.
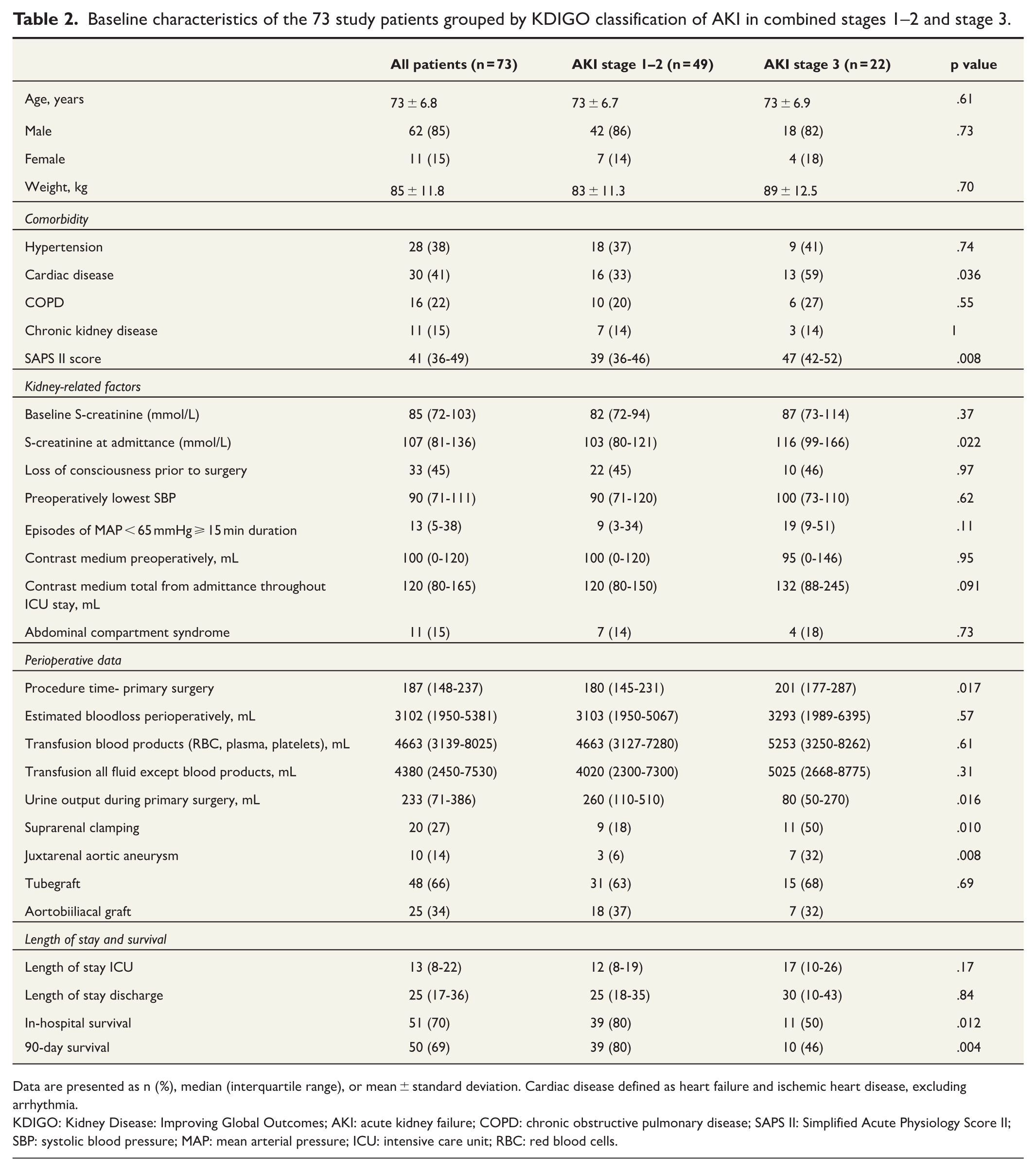
Data are presented as n (%), median (interquartile range), or mean ± standard deviation. Cardiac disease defined as heart failure and ischemic heart disease, excluding arrhythmia.
KDIGO: Kidney Disease: Improving Global Outcomes; AKI: acute kidney failure; COPD: chronic obstructive pulmonary disease; SAPS II: Simplified Acute Physiology Score II; SBP: systolic blood pressure; MAP: mean arterial pressure; ICU: intensive care unit; RBC: red blood cells.
When diagnosed with ACS (n = 11, 15%), the main pathophysiological findings at decompressive laparotomy were bleeding, edema, and bowel ischemia in six (55%), three (27%), and two patients (18%), respectively. Time of decompression was within 24 h of admittance in eight (73%) patients, within 48 h in two (18%) patients and in one (9%) patient after 9 days.
Acute kidney injury
AKI occurred in 71/73 (97%) of the study population. In patients with a prior measurement of SCr (n = 47, 64%), there was a significant elevation in SCr at admittance, from baseline median 85 μmol/L to 109 μmol/L (p = .001).
Patients were diagnosed with peak AKI at a median of two (IQR 2–3) days of admittance, and resolution occurred at a median of 5 days (IQR 2–13). In patients surviving until discharge, resolution occurred in 47 of 51 (92%) of patients (Figure 1). The patients without resolution all had RRT during their hospitalization.
After the closure of the abdominal wall, SCr was followed for two consecutive days in 54 of 58 patients (93%), with a fall in SCr from a median of 79 to 77 μmol/L (p = .67). Eleven (19%) of these patients were extubated and discharged from ICU before closure of the abdomen and another 14 (24%) within ⩽ 48 h of closure of the abdomen. No patient had worsening of KDIGO staging in the first 24 h after closure (Figure 2).
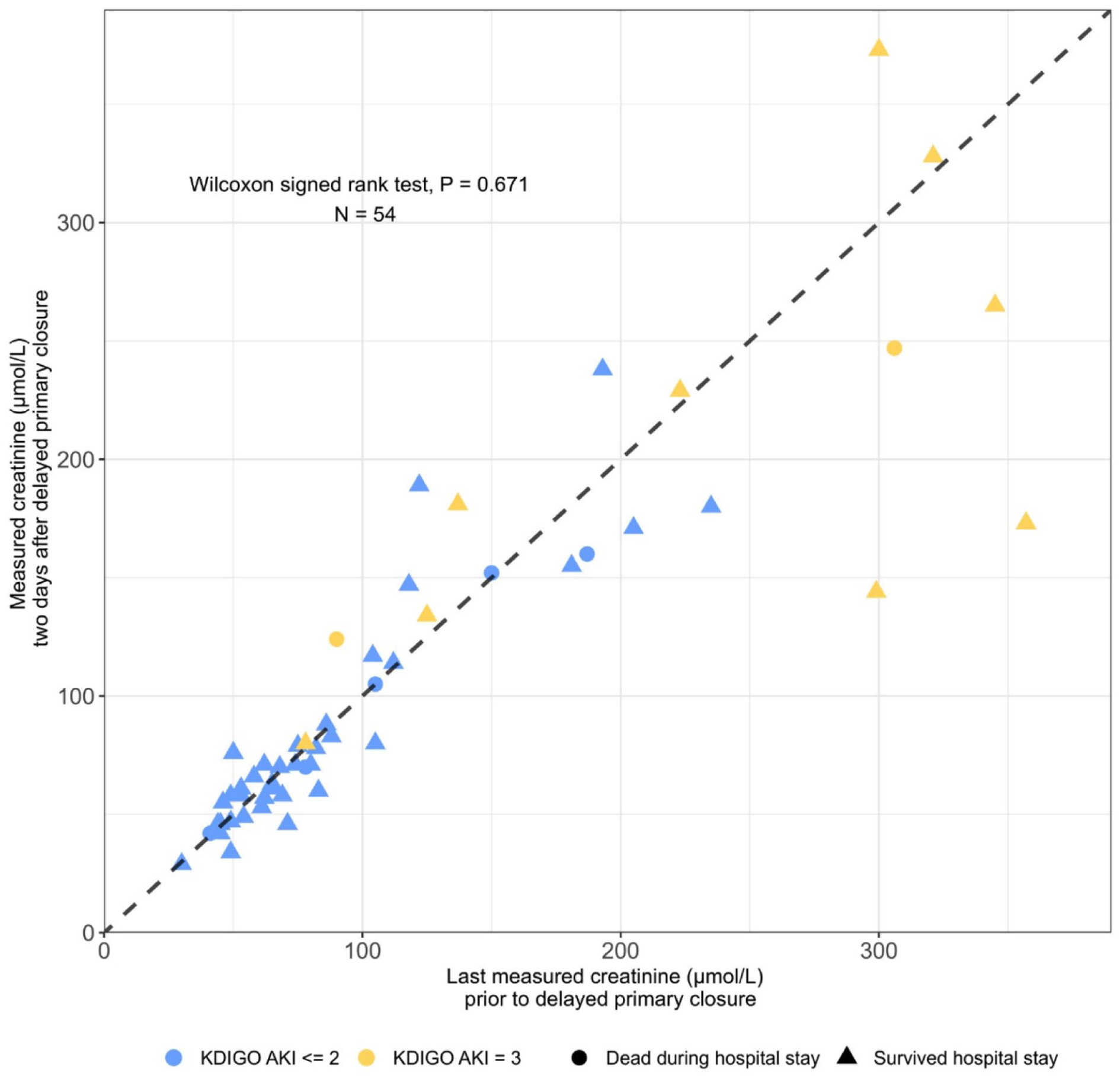
Scatter plot of distribution of S-creatinine the day prior to delayed primary closure and 2 days after delayed primary closure of the abdominal wall, according to KDIGO classification and survival.
KDIGO classification
All patients were diagnosed and staged by the SCr and UO criteria in the KDIGO classification. By including the UO criterion, significantly more patients were diagnosed overall (p = .001), and significantly more patients were classified as stage 2 (p = .001) (Table 3).
Acute kidney injury defined by KDIGO criteria (including both S-creatinine and urine output criteria) in comparison to classification by only S-creatinine or urine output criterion, among 73 patients treated with open abdomen after ruptured abdominal aortic aneurysm.
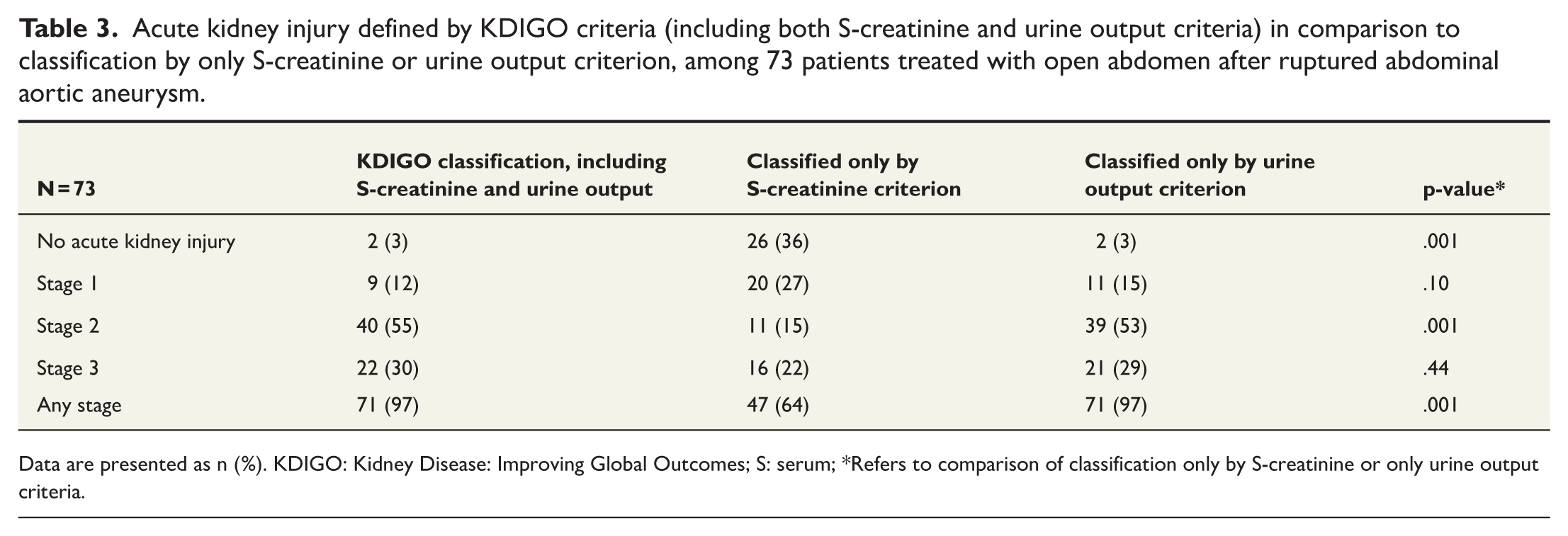
Data are presented as n (%). KDIGO: Kidney Disease: Improving Global Outcomes; S: serum; *Refers to comparison of classification only by S-creatinine or only urine output criteria.
AKI stage 3
AKI stage 3 occurred in 22/73 (30%) patients, with 13 (18%) receiving RRT. Four (18%) of the patients with AKI stage 3 had OAT due to ACS. Stage 3 patients had significantly more cardiac disease (p = .037), juxtarenal aneurysms (p = .006), higher SCr at admittance (p = .022), suprarenal clamping (p = .006), lower perioperative urine production (p = .015), and higher SAPS II score (p = .010) than the remaining study population. Concerning markers of hemodynamical instability, no difference was seen between the groups in loss of consciousness (p = .97) or preoperatively lowest systolic blood pressure (p = .62). Table 2 and Figure 3 display more details. Fourteen (64%) of the 22 stage 3 patients survived to closure of the abdomen and of the 11 (50%) patients who survived to discharge eight had had resolution of AKI after a median of 20 (IQR 7–24) days. The remaining three patients were discharged with stage 3 including two requiring long-term RRT.
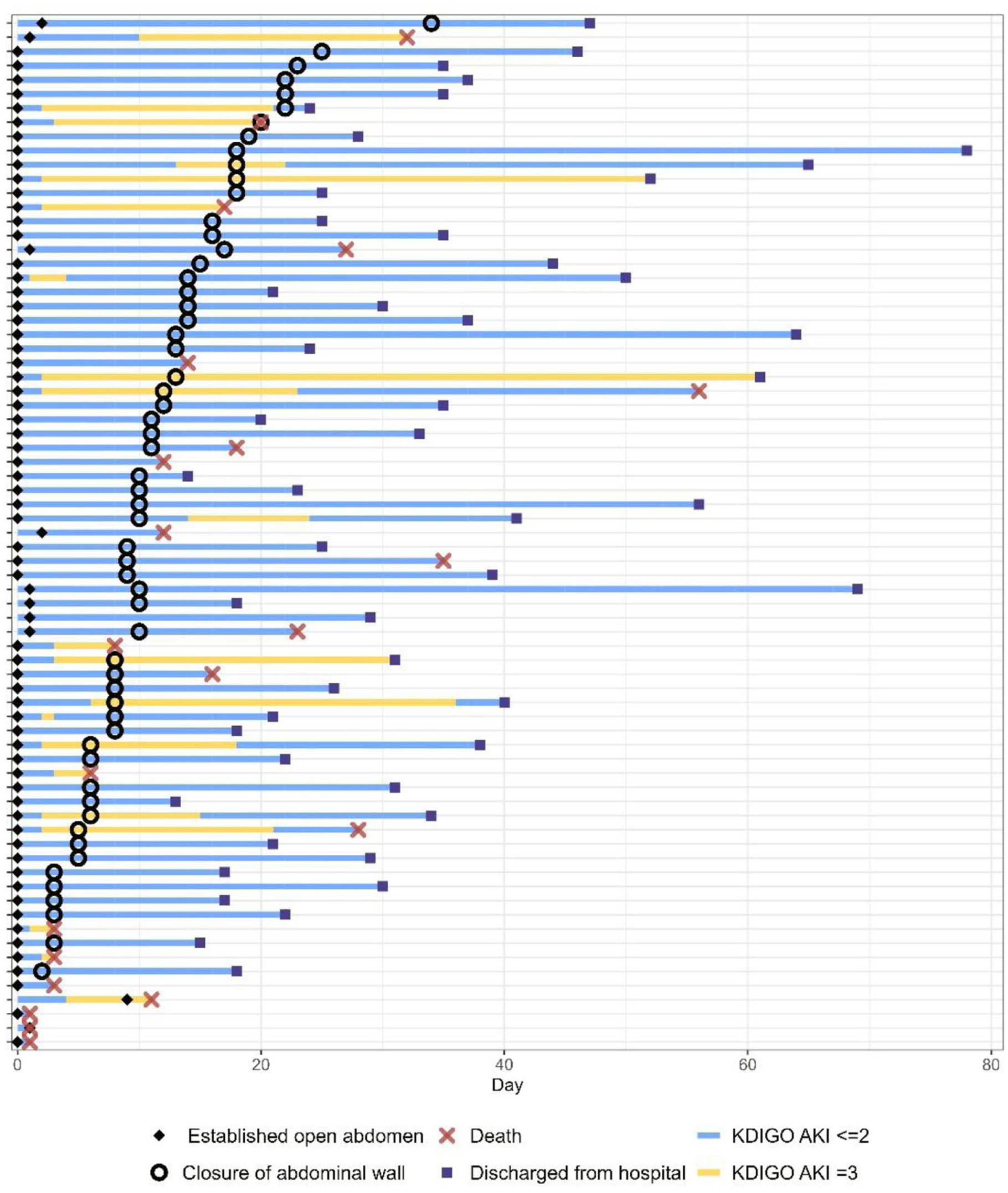
Swimmer Plot with all study patients. AKI is described by KDIGO stage throughout the hospital admittance and includes the timeline for open abdomen treatment in addition to survival.
To further explore the etiology and risk factors of AKI during OAT, a multivariable logistic regression was performed with AKI stage 3 constituting the outcome. Statistically significant predictors from the univariate analyses were included, in addition to sex and age (Table 4). SCr levels at admittance (OR 1.24, CI 1.02–1.51, p = .034) and perioperative diuresis (OR 0.67, CI 0.48–0.93, p = .018) were associated with KDIGO stage 3. The model explained 39% of the variance (McFadden R2) (Table 4).
Multivariable logistic regression to describe predictors of KDIGO AKI stage 3.
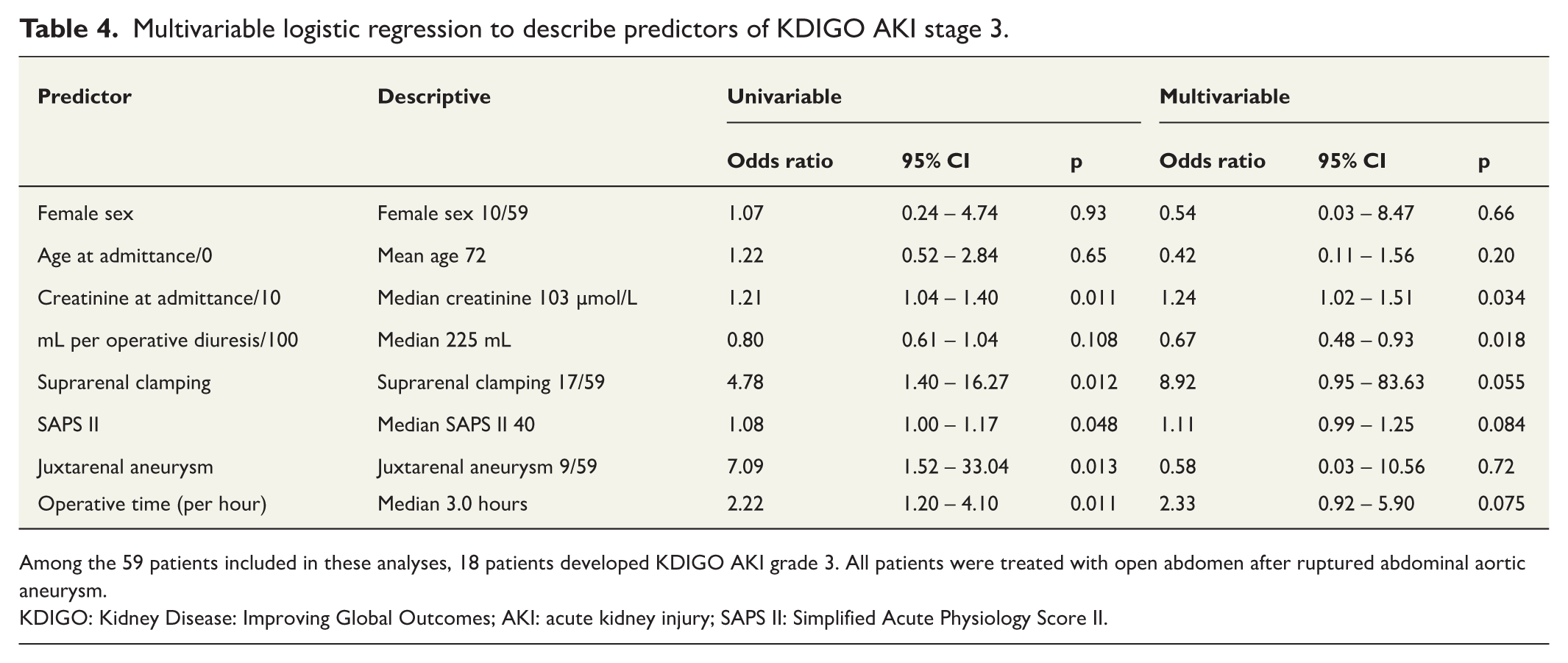
Among the 59 patients included in these analyses, 18 patients developed KDIGO AKI grade 3. All patients were treated with open abdomen after ruptured abdominal aortic aneurysm.
KDIGO: Kidney Disease: Improving Global Outcomes; AKI: acute kidney injury; SAPS II: Simplified Acute Physiology Score II.
Complication and survival
In the total study population, 34 (47%) patients suffered a total of 44 ischemic complications—18 episodes of bowel ischemia and 26 of lower limb ischemia—and 7 (10%) patients suffered both ischemic complications.
In total, 58/73 (80%) patients survived until the closure of the abdomen. In-hospital survival was 70% (51/73), and the 90-day survival was 69% (50/73). Among patients treated prophylactically with OAT, the 90-day survival was 74% (46/62), and if ACS had occurred, 36% (4/11) (p = .029).
The in-hospital survival in patients with AKI stage 3 was 50% (n = 11) versus 80% (n = 39) in patients with stages 1 and 2 (p = .012). The corresponding 90-day survival was 46% (n = 10) and 80% (n = 39), respectively (p = .004) (Table 2). There was no difference in survival in stage 3 patients related to prophylactic OAT versus ACS (p = .096) (Table 5).
Patients grouped by reason for open abdomen treatment, among 73 patients treated with open abdomen after open surgical repair for ruptured abdominal aortic aneurysm.
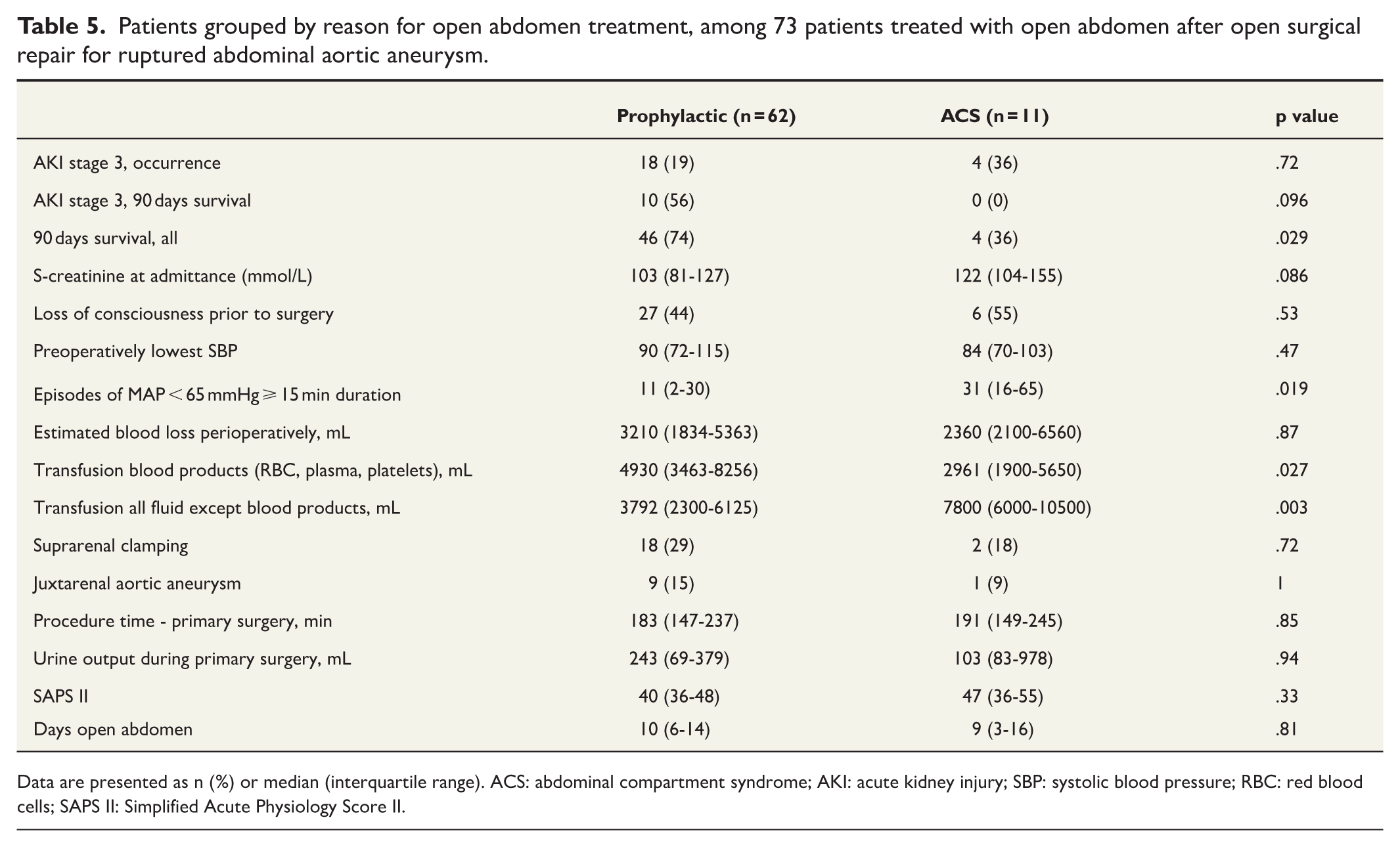
Data are presented as n (%) or median (interquartile range). ACS: abdominal compartment syndrome; AKI: acute kidney injury; SBP: systolic blood pressure; RBC: red blood cells; SAPS II: Simplified Acute Physiology Score II.
Suprarenal clamping (n = 20) was associated with stage 3 AKI in 11 (55%) with a 90-day survival of 55%, and stage 1–2 AKI in 9 (45%) with a 78% 90-day survival. In infrarenal clamping (n = 53), stage 3 AKI occurred in 11 (21%) and stage 1–2 AKI in 40 (75%), with corresponding 90-day survival 36% and 80%. Two patients (4%) had no AKI, one survived. Survival in AKI stage 3 was no different in supra-versus infrarenal clamping (p = 1.00), nor in the groups “suprarenal clamping and AKI stage 3” versus “infrarenal clamping and AKI stage 1-2” (p = .12).
Discussion
AKI was present in 97% (71/73) of patients with OAT after rAAA. There was a significant increase in the prevalence of AKI when including both UO and SCr criteria, with peak diagnosis at median 2 days post-admittance. No signs of kidney function deterioration were observed upon closure of the abdominal wall. Patients with AKI stage 3 (n = 22, 30%) had lower 90 days survival than those with less severe AKI (p = .004) and patients with ACS had lower survival than those with prophylactic OAT (p = .029) Among the survivors, 92% (47/50) had resolution of AKI at discharge.
AKI occurrence and classification
In this study, the occurrence of AKI is higher than reported in previous studies on populations with rAAA and OSR without OAT. Kopolovic et al. 3 found 76% by the use of AKIN criteria, the same as van Beek et al. 7 found applying RIFLE criteria. The incidence of severe AKI and the frequency of RRT do not differ considerably.2,3,7,10,15 Van Beek et al. 7 found 36% severe AKI according to RIFLE criteria in the population with OSR while Ambler et al. 2 found severe AKI at 43% using ARISe criteria. Due to variability in AKI classification and differences in patient populations, comparisons are challenging. Several confounding factors exist, one being that hemodynamically unstable patients are at increased risk of AKI and at the same time more likely to be considered in need of prophylactic OAT.
Previous studies have shown that oliguria contributes to identifying patients with worse outcomes of AKI, more than SCr alone.5,30,31 In this study, the UO criterion raised the sensitivity for AKI, indicating that UO measurements are important for the early detection of AKI. Wlodzimirow et al. 23 demonstrated that excluding UO from the RIFLE classification delayed the diagnosis and underscored the incidence and severity of AKI. Although a sensitive marker of kidney function, oliguria is a normal physiological response to hypovolemia and does not necessarily signify kidney injury. 32 The lack of clarity in KDIGO guidelines on how to record UO and low clinical applicability outside the intensive care unit are other factors affecting the clinical usefulness of the criteria.33–35 However, early prediction of severe AKI has the potential to improve survival in patients with rAAA. The median interval of 2 days to AKI diagnosis observed in this study highlights the importance of the immediate postoperative period. The high sensitivity of the urine output criterion underscores its potential in early recognition and intervention.
Clinical markers included in the multivariable regression analysis predicted only 39% of the variance in stage 3. New biomarkers, such as tissue inhibitor of metalloproteinase-2 (TIMP-2) and insulin-like growth factor binding protein 7 (IGFBP7), are promising for earlier detection and studies show biomarker-guided treatment to reduce the need for RRT.5,32,36 However, their appropriate clinical use remains undefined, and research to develop therapeutic drugs have not yet been successful.5,32
Intra-abdominal hypertension, rAAA and AKI
The increased SCr at admittance indicates that the kidney’s compensatory mechanisms were exhausted early after aortic rupture. Hypovolemia secondary to severe hemorrhage, high age, and pre-existing comorbidities are all possible contributors to the elevated SCr.5,37 IAH is another potential factor, suggested by the surgeon’s choice to establish prophylactically OAT in 85% of the study patients while the remaining patients developed ACS. Decompressive laparotomy can protect kidney function, as shown in the prospective multi-center study by de Waele et al., 38 with improved urine output and respiratory function after decompression in ACS patients.
Ambler et al. 2 found preoperative SCr to be a predictor of severe AKI in rAAA without OAT and in this study higher SCr at admittance was associated with AKI stage 3 in the multivariable regression analysis. However, the retrospective study design does not allow conclusions regarding the causality of AKI; it cannot determine whether excessive bleeding, IAH, pre-existing vulnerability, or low renal reserve are the most important contributing factors, neither assess whether abdominal decompression prevented progression to more severe AKI in some cases. Although AKI stage 3 had lower survival in this study, the fundamental drivers for mortality could be common risk factors rather than the severe AKI itself.
Prolonged OAT is resource-demanding and bears the risk of complications such as graft infections or entero-atmospheric fistula formation.9,39 Renal function at delayed primary closure is seldom reported in the literature. In this study, SCr measurements and urine production showed no decline after abdominal closure, suggesting either a timely closure or a potential to close the abdomen safely earlier in some patients. Unfortunately, post-closure IAP measurements were not obtained and could possibly have shed further light on the association between abdominal closure, IAH, and kidney function.
Compared to Ersryd et al.’s 11 national population-based study, the proportion of patients treated with prophylactic OAT in this cohort appears high. This can indicate over-treatment or reflect a difference in clinical practice and institutional focus on ACS and OAT. Notably, AKI was diagnosis at a median of 2 days post-admittance, aligning with the timing of ACS in 10 of 11 cases. Whether a more restrictive OAT approach could have led to additional cases of AKI stage 3 remains unanswered. Likewise, the lack of a non-OAT comparison group precludes conclusions regarding the possible effect of prophylactic OAT in preventing severe AKI.
The strength of this study is the excellent internal validity due to the prospectively registered patients, with no missing patients identified when comparing the different registries. Furthermore, most variables were defined and registered prospectively, such as UO throughout the ICU stay and daily SCr measurements.
Limitations are relatively few included patients, with results prone to type II statistical errors and limited statistical power, as seen in the multivariable logistic regression where factors known to predict AKI were not associated with the outcome. The generalizability of the study is affected by the lack of a non-OAT comparison group and not including patients treated with EVAR. EVAR for rAAA may have a lower incidence of AKI6,15 although the European Society for Vascular Surgery 2024 Management Guidelines of Abdominal Aorto-iliac Artery Aneurysm do not conclude on the matter. 9
Some data, such as baseline SCr, perioperative urine output, and daily IAP measurements before and after closure of the abdomen, were incomplete for some patients. A prospective, multi-center study could illuminate unanswered questions concerning rAAA, OAT, and AKI.
Conclusion
Most patients treated with OAT after rAAA developed AKI when diagnosed by KDIGO classification, and the UO criterion significantly increased the number of patients diagnosed. No aggravation of kidney function at delayed primary closure could signify a potential for earlier closure of the abdominal wall.
Considering the high incidence of AKI, all measures to protect kidney function seem warranted from admittance. Further valuable insight into the dynamics of intra-abdominal hypertension and kidney function in patients with rAAA can be gained by prospective, multi-center studies.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261438658 – Supplemental material for Incidence and outcome of acute kidney injury in open abdomen treatment following open surgery for ruptured abdominal aortic aneurysm
Supplemental material, sj-docx-1-sjs-10.1177_14574969261438658 for Incidence and outcome of acute kidney injury in open abdomen treatment following open surgery for ruptured abdominal aortic aneurysm by Henriette Fagertun, Knut A. Rise Langlo, Pål Klepstad, Skule Mo, Tor-Arne Hegvik, Linn Åldstedt Nyrønning, Martin Björck and Arne Seternes in Scandinavian Journal of Surgery
Footnotes
Acknowledgements
The authors thank Rolf Westly, HEMIT, for data extraction.
Author contributions
H.F., A.S., S.M., K.A.R.-L., and P.K. conceived the study. H.F. collected the data and drafted the manuscript. H.F. and T.-A.H. performed the statistical analysis. All authors critically revised the manuscript and approved the final version.
Clinical trial registration
N/A.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The main author received an unrestricted research grant from St Olav Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.