
Abstract
Background and aims:
A large variation in surgery rates can be indicative of its overuse. In Finland, surgeries for carpal tunnel syndrome (CTS) and ulnar nerve disorder (UN) are common, but regional differences in their incidence rates remain unexplored. This study examined how the incidence rates of these surgeries vary across hospital districts in Finland to evaluate regional consistency.
Methods:
We compared regional age- and sex-adjusted incidence rates per 100,000 person-years based on data from Finland’s Care Register for Health Care for CTS and UN surgeries from 2010 to 2021, calculated relative to population size as reported by Statistics Finland. The study included 21 hospital districts in Finland.
Results:
During the 4-year period from 2018 to 2021, the difference between the lowest (99.6 cases per 100,000 person-years (95% confidence interval (CI) 80.7–122)) and the highest (351 cases per 100,000 person-years (95% CI 336–367)) adjusted incidence rates for CTS surgery was 3.5-fold, with a median adjusted incidence rate of 213 cases per 100,000 person-years. Over the same period, the difference between the lowest (1.04 cases per 100,000 person-year (95% CI 0.03–5.78)) and the highest (81.9 cases per 100,000 person-years (95% CI 73.2–91.5)) adjusted incidence rates for UN surgery was up to 79-fold, with a median adjusted incidence rate of 17.8 cases per 100,000 person-years.
Conclusions:
Surgery for CTS shows up to a 3.5-fold variation across Finland’s hospital districts. Although less common in absolute numbers, surgical treatment rates for UN vary up to 79-fold among these regions. Such significant variations are unlikely to be attributed solely to differences in population morbidity. Instead, the findings indicate that the criteria for performing these surgeries vary considerably across the Finland’s hospital districts, suggesting a potential overuse in certain areas.
Keywords
Context and relevance
Large regional variation in surgery rates for carpal tunnel syndrome (CTS) and ulnar nerve disorder (UN) indicate a “grey area” in clinical decision-making, where some regions operate on less severe cases while others use stricter criteria. This variation raises concerns about the overuse of surgery, particularly for milder cases where the benefits are uncertain, yet the risks remain consistent. This study revealed notable regional variation in CTS and UN surgery incidence rates across Finland, unlikely to align with population needs. The findings suggest substantial variability in surgical criteria, pointing to potential overuse in some regions. To improve resource utilization, healthcare providers should address system pressures contributing to overuse and ensure patients have sufficient information to make informed decisions.
Introduction
Carpal tunnel syndrome (CTS) and ulnar nerve disorder (UN) in cubital tunnel or Guyon’s canal are common compression neuropathies that are typically initially managed non-surgically, but surgery is offered to patients that fail a trial of non-surgical treatment or present with severe typical symptoms.1,2 While the evidence base for UN surgeries is more limited, the effect of carpal tunnel release for CTS has been evaluated in numerous randomized trials.2–5 Trials show that the mean benefit of surgery over non-surgical management of CTS is modest; surgery consistently provides greater symptom relief than splinting or other conservative treatments, but symptoms seem also to improve over time in non-surgically managed groups. In this context, decisions regarding surgical intervention may be considered preference-sensitive, meaning that treatment choices depend substantially on patient preferences and clinician judgment rather than on unequivocal effects in contrast to drastically effective care where treatment benefits are large and utilization should be relatively uniform.6–8 Surgical treatment rates may also be supply-sensitive, whereby utilization is influenced by the availability of healthcare resources such as specialist workforce, diagnostic capacity, or operating room access rather than by underlying clinical need. 6 Preference- or supply-sensitive services can exhibit substantial regional variation even when population morbidity is relatively homogeneous, as would be expected between adjacent regions within countries such as Finland.
Substantial regional variation without clear justification typically signals overuse. 8 Overuse, defined as the provision of medical services where potential harms exceed the benefits, 9 adversely impacts patients and healthcare systems alike. This issue is driven by a combination of demand- and supply-side factors, including patient and clinician beliefs and systemic pressures within healthcare delivery. 10 CTS and UN surgeries are prime examples of cases where a 2.5- to 5-fold regional variation has been observed in countries such as Sweden and France, with only partially explainable reasons,11,12 indicating that overuse can occur in high-incidence areas. In Finland, while national-level data on CTS and UN surgery rates has been documented, 13 regional differences in their delivery remain unexplored. The aim of this study is to examine the regional variations of CTS and UN surgeries across Finland.
Methods
This was a nationwide retrospective observational register study. We obtained the data from the Finland’s Care Register for Health Care, encompassing the period from 1 January 2010 to 31 December 2021. The register is maintained by collecting standardized information from hospitals, health centers, and other care providers, who submit data each year according to a manual specifying content and reporting procedures. 14 Data provision is mandatory for all healthcare units in Finland. The extracted data included, for each inpatient hospital stay, the date of surgery, patient age and sex, hospital, municipality of residence, and all primary and secondary diagnoses and operation codes.
During the study period, the Finnish healthcare system was divided into 21 hospital districts (Fig. 1). The geographical location of each hospital was determined using hospital codes, which were matched with publicly available data on all hospital districts in Finland, obtained from Statistics Finland.
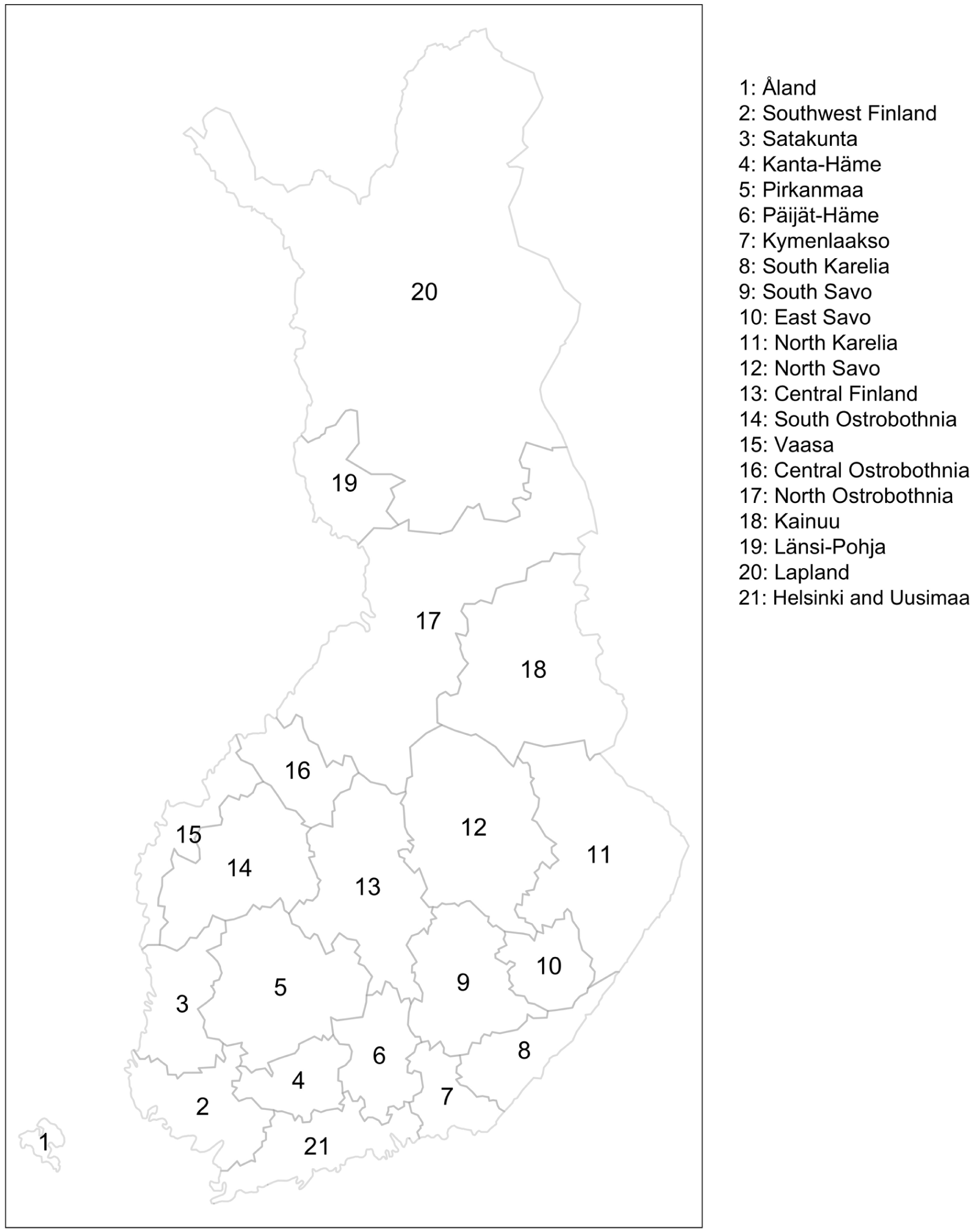
Hospital districts of Finland in 2019.
CTS and UN surgeries were identified using primary NOMESCO procedure codes (Finnish version) 15 in conjunction with International Classification of Diseases, 10th Revision, (ICD-10) diagnosis codes. CTS surgeries were included if the patient had the procedure code ACC51 or ACC59 (release of the median nerve) paired with the diagnosis code G56.0 (CTS) during the same operation. UN surgeries were included if the patient had the procedure code ACC53 or ACC59 (release of the ulnar nerve) along with the diagnosis code G56.2 (UN). Specific UN diagnoses such as Guyon’s canal syndrome and cubital tunnel syndrome were not distinguished. Only patients aged 18 years or older were included in the analysis.
Statistics
The primary outcome of this study was the age- and sex-adjusted incidence rate of surgery (per 100,000 person-years). We calculated annual age- and sex-adjusted incidence rates (per 100,000 person-years) using the mean adult population (age ⩾ 18 years) of each Finnish hospital district as the population at risk, based on publicly available data from Statistics Finland. 16 Age and sex adjustments were performed using the direct standardization method: crude incidence rates for each age and sex category were multiplied by the corresponding proportions of the standard Finnish population, categorized by year, sex, and 1-year age intervals. The results were summed to obtain the adjusted incidence rates for the total population.
To assess trends in clinical practice over time, we calculated and reported mean age- and sex-adjusted incidence rates for three time periods: 2010–2013 (reference period), 2014–2017, and 2018–2021. We modeled these mean adjusted incidence rates using Poisson regression, with 2010–2013 serving as the baseline. Incidence rate ratios (IRRs) with 95% CI were estimated using the exact method, comparing each subsequent period to the baseline. 17
To investigate factors contributing to the regional variability in adjusted incidence rates, we conducted Spearman correlation analyses with 95% CIs. Specifically, we examined (1) the relationship between adjusted incidence rates in 2018–2021 and those in the historical reference period (2010–2013), and (2) the association between adjusted incidence rates in 2018–2021 and the mean population size of each hospital district in the same period.
We obtained a dataset containing a map of Finland with hospital district boundaries from the publicly available R package SHP2019. 18 All analyses were conducted using R for Mac, version 4.3.2 (R Foundation for Statistical Computing, Vienna, Austria). Data cleaning was performed using the tidyverse package, and the function epi.conf() from the epiR package was used to calculate the adjusted incidence rates. Spearman correlation coefficients were computed using the SpearmanRho function from the DescTools package.
Ethics, registration, data-sharing plan, funding, and disclosures
This study received approval from the Finnish Institute for Health and Welfare (THL/1800/5.05.00/2019). Informed consent was not required because the data were retrospective and anonymized. Data were obtained from Finland’s Care Register for Health Care, with patient confidentiality protected in line with applicable data-protection laws. All study procedures adhered to ethical guidelines outlined in the Declaration of Helsinki.
Finnish data-protection legislation restricts public access to the dataset used in this study. Access is limited to authorized individuals under strict privacy protocols to ensure the confidentiality and security of patient information.
Results
Overall incidence rate in Finland
The nationwide adjusted incidence of CTS surgery remained stable at 201 (95% CI 197–205 or 206) per 100,000 person-years from 2010 to 2012 before peaking at 220 (95% CI 216–225) per 100,000 person-years in 2013 (Fig. 2). Following this peak, the adjusted incidence generally declined, reaching 161 (95% CI 157–164) per 100,000 person-years in 2021.
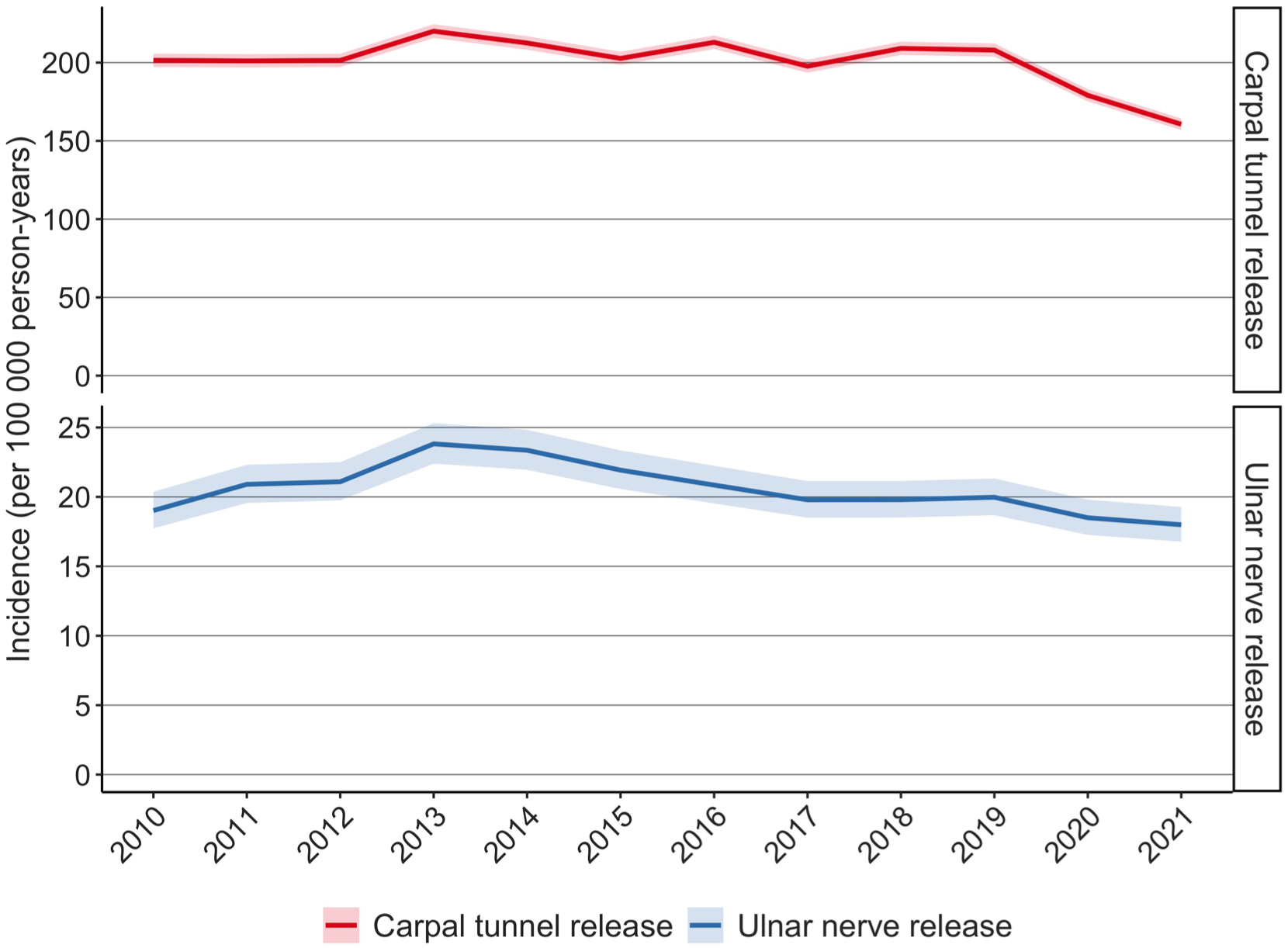
The nationwide incidence rates (per 100,000 person-years) of surgeries for carpal tunnel syndrome and ulnar nerve disorder in Finland from 2010 to 2021.
The nationwide adjusted incidence of UN surgery increased from 19 (95% CI 17.7–20.4) per 100,000 person-years in 2010 to 23.8 (95% CI 22.4–25.3) per 100,000 person-years in 2013. After 2014, it gradually declined, reaching 18 (95% CI 16.8–19.3) per 100,000 person-years in 2021.
Regional adjusted incidence rates of CTS surgery
The CTS surgery–adjusted incidence rates in 2018–2021 ranged from 99.6 (95% CI 80.7–122) cases per 100,000 person-years in Åland to 351 (95% CI 336–367) cases per 100,000 person-years in North Karelia (Fig. 3). The difference between the highest and the lowest adjusted incidence rate was 3.5-fold. The median adjusted incidence rate across the regions was 213 cases per 100,000 person-years. Comparing the 2018–2021 CTS surgery–adjusted incidence rates to those from 2010–2013, the trend showed a mixed pattern: in seven regions, there was a 1%–19% increase in the adjusted incidence rates, and in 14 regions, there was a 1%–40% decrease in the adjusted incidence rates (Table 1).
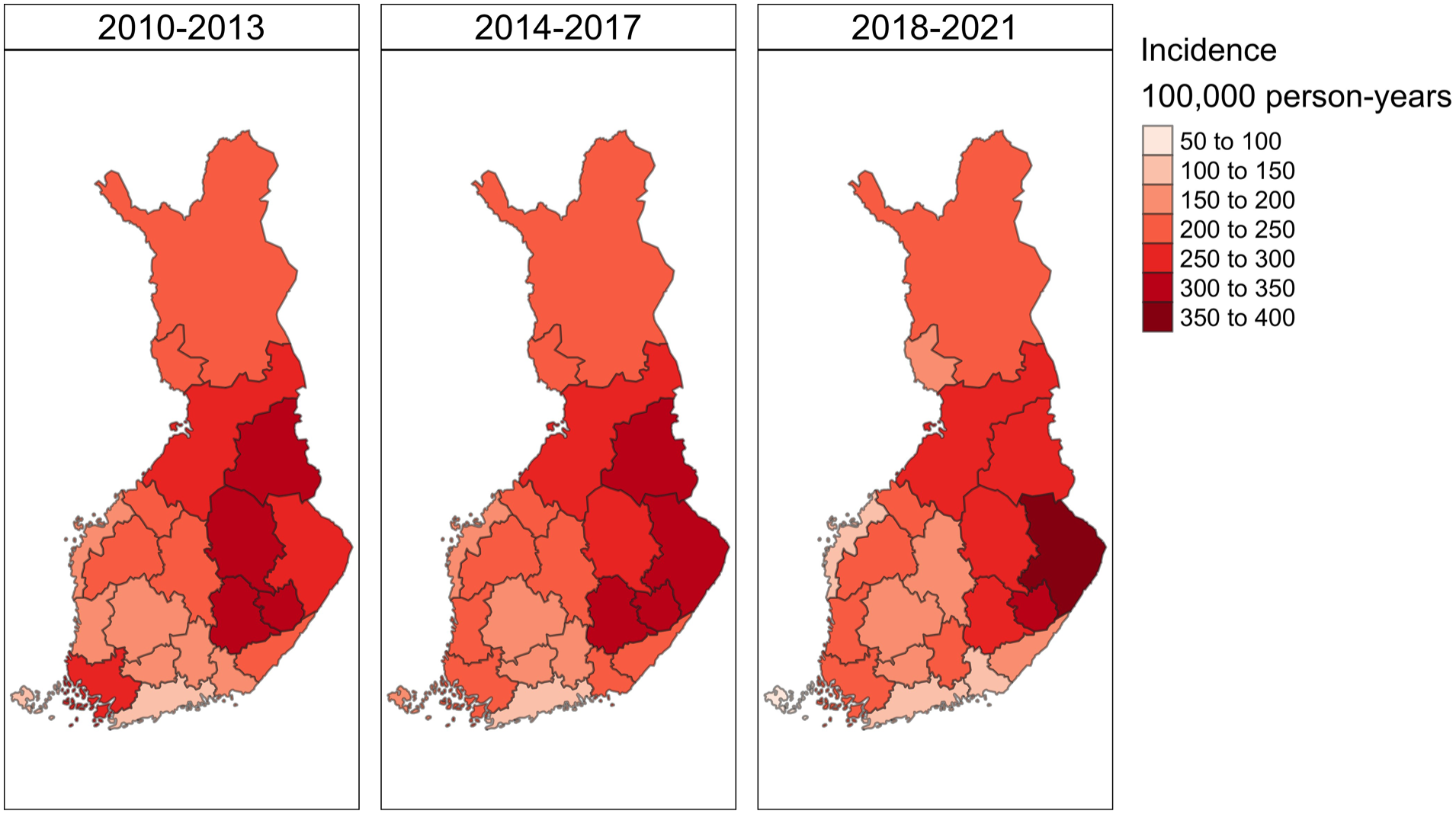
A map of Finland divided into 21 hospital districts, illustrating age- and sex-adjusted incidence rates (per 100,000 person-years) of carpal tunnel syndrome surgery for the periods 2010–2013, 2014–2017, and 2018–2021.
Carpal tunnel syndrome surgery–adjusted incidence rates (per 100,000 person-years) for 2018–2021, along with adjusted incidence rate ratios and percentage changes comparing 2010–2013 to 2018–2021 across Finnish hospital districts.
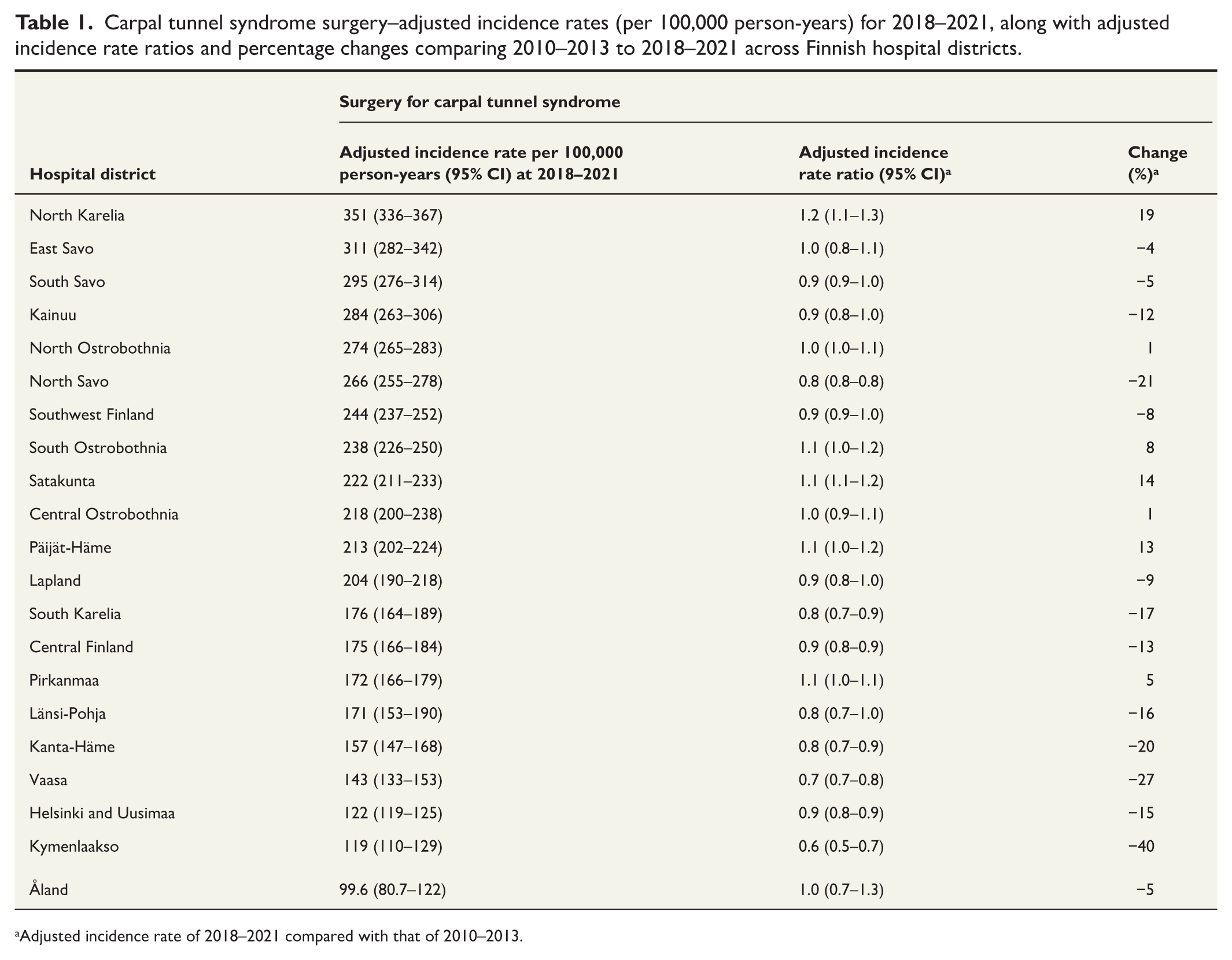
Adjusted incidence rate of 2018–2021 compared with that of 2010–2013.
Regional adjusted incidence rates of UN surgery
The UN surgery adjusted incidence rates in 2018–2021 ranged from 1.04 (95% CI 0.03–5.78) cases per 100,000 person-years in Åland to 81.9 (95% CI 73.2–91.5) cases per 100,000 person-years in Lapland (Fig. 4). The difference between the highest and the lowest adjusted incidence rate was 79-fold. Åland and Lapland notably deviated from the rest of the regions, with incidence rates clearly outside the overall range. When excluding these two outliers, the second highest adjusted incidence rate was 33.6 (95% CI 29–38.9), and the second lowest was 10.6 (95% CI 8–13.7), resulting in a reduced difference of approximately 3.2-fold. The median adjusted incidence rate across the regions was 17.8 cases per 100,000 person-years. Comparing the 2018–2021 UN surgery adjusted incidence rates to those from 2010–2013, the trend also showed a mixed pattern with an increase of the adjusted incidence rates between 6% and 149% in 7 regions and a 7%–81% decrease in 14 regions (Table 2).
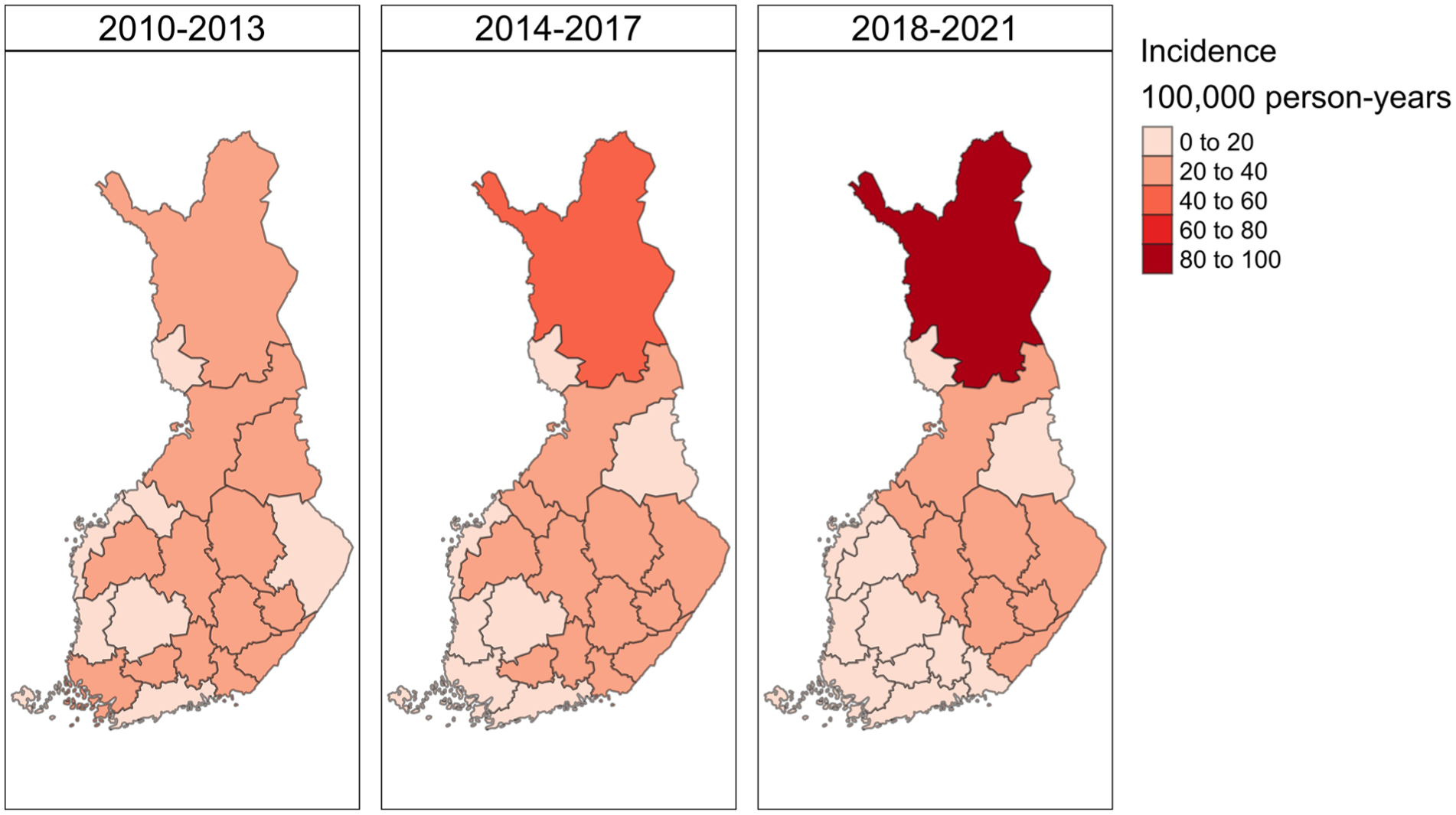
A map of Finland divided into 21 hospital districts, illustrating age- and sex-adjusted incidence rate (per 100,000 person-years) of ulnar nerve disorder surgeries for the periods 2010–2013, 2014–2017, and 2018–2021.
The ulnar nerve disorder surgery–adjusted incidence rates (per 100,000 person-years) for 2018–2021, along with adjusted incidence rate ratios and percentage changes comparing 2010–2013 to 2018–2021 across Finnish hospital districts.
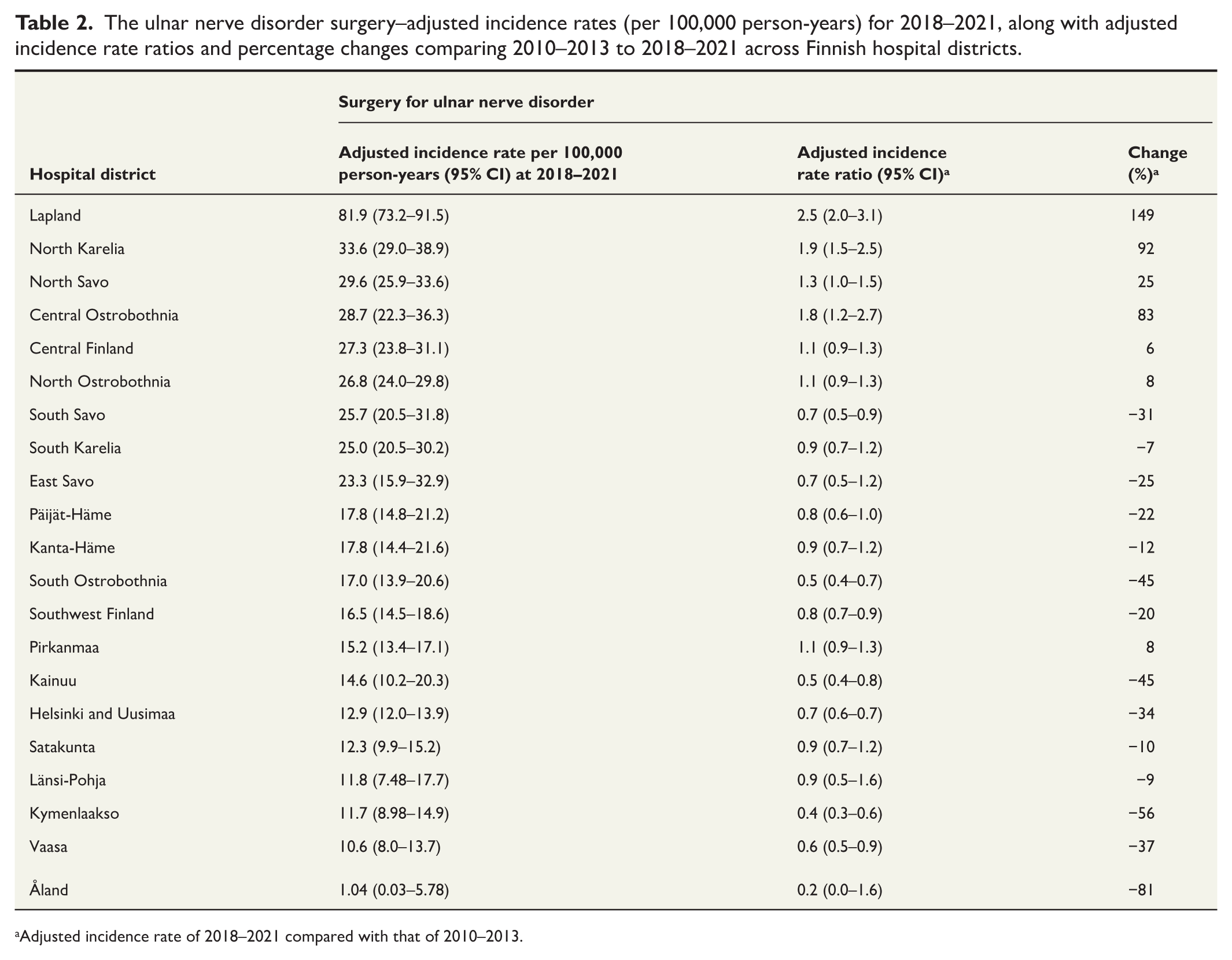
Adjusted incidence rate of 2018–2021 compared with that of 2010–2013.
Contributing factors
The correlation between population size and adjusted incidence rates was weak, with a Spearman rank correlation coefficient (rho) of −0.06 (95% CI −0.48 to 0.38) for CTS surgery and 0.07 (95% CI −0.37 to 0.49) for UN surgery (Supplemental Fig.1). In contrast, the correlation between the adjusted incidence rates in 2018–2021 and the historical adjusted incidence data from 2010 to 2013 was moderate to strong, with a rho of 0.83 (95% CI 0.63–0.93) for CTS surgery and 0.46 (95% CI 0.04–0.74) for UN surgery (Supplemental Fig. 2).
Discussion
While national-level incidence rates of CTS and UN surgeries in Finland over the past decade showed a relatively mild initial increase followed by a comparable decrease, this pattern provides only a descriptive picture about the overall situation in the country. Beneath these averages, there were large regional differences with CTS and particularly with UN surgery. Over the past decade, trends within regions were heterogeneous, with some districts experiencing consistent increases or decreases in both CTS and UN surgeries, while others demonstrated divergent patterns. In addition, CTS and UN surgery rates did not mirror each other; regions with high CTS surgery rates were often different from those with high UN surgery rates.
Given the large variation in CTS and UN surgery rates across Finnish regions—and prior research showing that patient and surgeon preferences for CTS surgery may diverge19–21—we interpret these procedures, in the Finnish context, as examples of preference-sensitive care. 6 Although our data do not explain the underlying reasons for the regional variation, the disparities between CTS and UN surgery rates suggest that this is not simply due to some surgeons being universally eager to operate on entrapment neuropathies, but may instead reflect differing perceptions or approaches to these specific diagnoses. Supply-side explanations would seem less likely in Finland: all hospital districts are served by regional hospitals, specialist training is nationally standardized, and the number of specialists in each region is planned at the national level to meet demand.6,22 Notably, our study districts with large urban centers—such as Helsinki-Uusimaa and Pirkanmaa—presumed to have higher densities of surgeons, did not exhibit the highest incidence rates, further supporting the view that variation reflects preference sensitivity rather than resource availability. However, findings from Sweden—where a 2.5-fold regional variation in CTS and UN surgeries has been reported 11 —suggest that even in well-organized, high-income health systems, variation may still reflect regional differences in access, diagnostic capacity, and surgical availability. Surgical treatment rates in Finland—with approximately 60% of CTS patients undergoing surgery 13 —are comparable to Sweden’s, where rates ranged from approximately 50% to 80% across counties. The Swedish study concluded that regional variation could not be fully explained by demand-side factors alone and pointed to supply-side dynamics as likely contributors. Given the similar magnitude and persistence of regional variation in Finland, it is plausible that differences in capacity, resource allocation, or institutional norms may still influence surgical decision-making—despite structural efforts to equalize supply. Therefore, while we view preference-sensitive care as the primary explanatory framework, we acknowledge that supply-side influences may also contribute to the observed variation.
Furthermore, the notably high surgical rates in some Finnish regions—especially when compared to international figures, such as in the United Kingdom where only 26%–28% of CTS patients underwent surgery between 2010 and 2013 23 —raise concerns about potential overuse in high-incidence areas, rather than underuse in others. This observation highlights a central issue: increased utilization of surgery may yield negligible overall population benefits if surgical indications are expanded to include milder or atypical symptoms. In such cases, the benefits of surgery tend to decline, while the risks and morbidity associated with surgery remain largely similar as with severe symptoms where benefits are larger (Fig. 5). This concern is supported by prior research on musculoskeletal care: Rudolfsen et al. 24 demonstrated that regions with higher treatment rates tended to treat patients who were healthier at baseline and experienced smaller improvements in outcomes. In the context of CTS and UN, there is a gray zone between clear benefits for patients with severe typical symptoms and no benefits for those with atypical mild symptoms. In this gray zone—where preference-sensitive care takes place6,7—treatment decisions are strongly influenced by individual preferences, and the balance between benefits and risks may often be perceived differently by clinicians and patients. Expanding surgical indications in the gray zone increases the risk of crossing a threshold where the harms outweigh the benefits. The large variation in surgery rates suggests that a substantial part of decision-making in current CTS and UN surgery practice in Finland occurs in this gray zone.
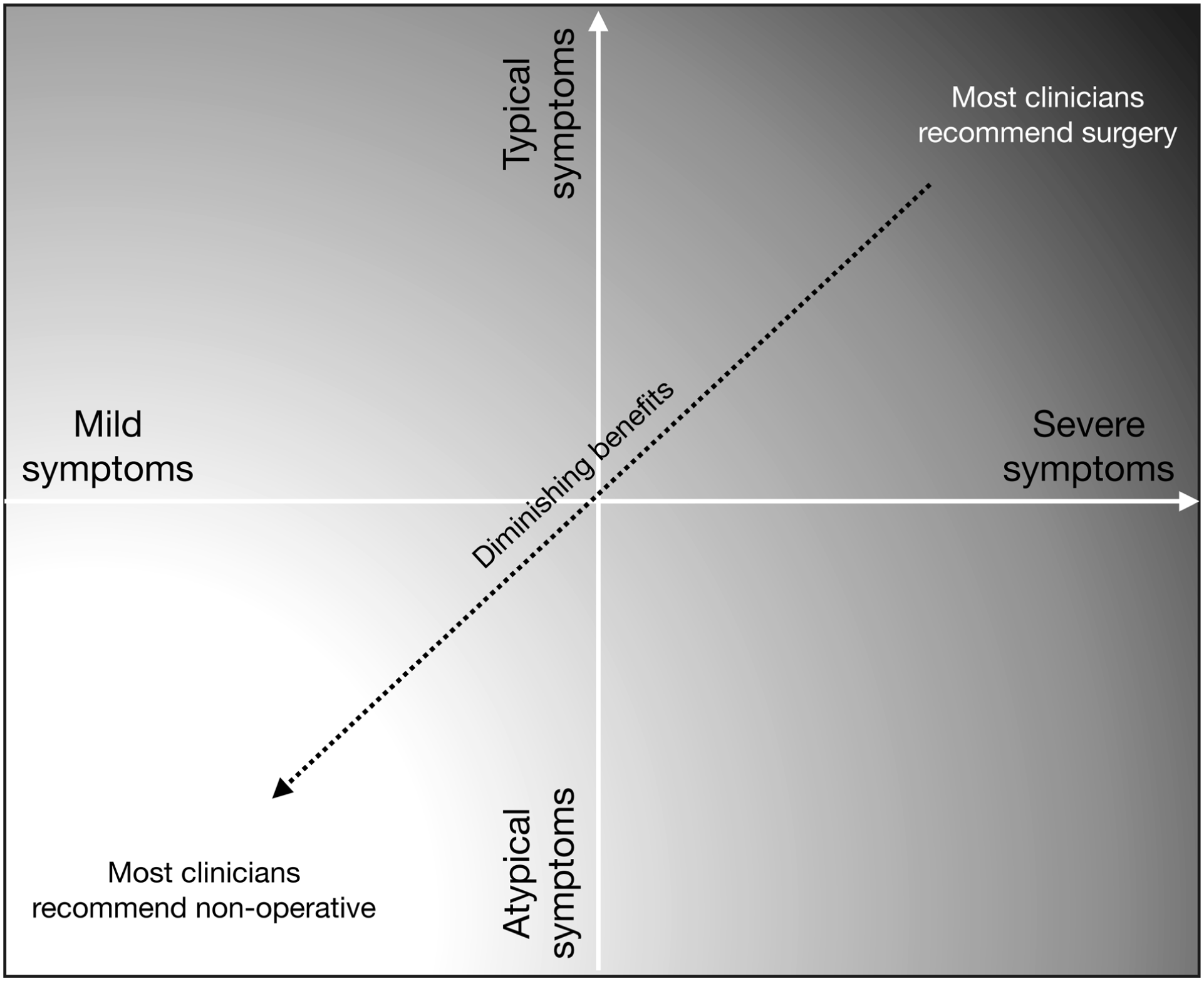
Theoretical framework behind regional variation in the use of surgery beyond population needs.
To improve resource utilization, healthcare providers can (1) address potential system-driven factors contributing to overuse, which may vary between the regions but could include regional guidelines (or lack of them), regulatory, or financial pressures, and (2) ensure that patients receive sufficient information about the effects of treatment options to actively participate in treatment decisions.10,19–21
As for the limitations of our study, while reporting surgeries to the Finland’s Care Register for Health Care is mandatory and ensures high coverage (92%–98%) and sensitivity (81%–92%), 25 we cannot exclude the possibility of our analysis being affected by inconsistencies or inaccuracies in the reporting of diagnosis and intervention codes. Irregularities might cause noise particularly with small populations, but our CIs suggest that random variation cannot be held responsible for the differences. In addition, since all UN surgeries were coded under a single classification, we could not distinguish the incidence rates for specific diagnoses (Guyon’s canal syndrome and cubital tunnel syndrome), but we suspect that vast majority are cubital tunnel decompressions. Furthermore, the overall number of surgeries performed in the country may have declined in 2020 and 2021 due to the COVID-19 pandemic, as many elective procedures were canceled or delayed. However, this should not have significantly influenced regional differences, as pandemic-related regulations were applied across all regions.
In addition, while it is possible that regional differences in disease burden contribute to variation in surgery rates, we believe this factor accounts for only part of the observed differences. We currently lack corresponding regional-level morbidity data, which limits our ability to directly assess its contribution to surgical variation. However, our interpretation is supported first by the observations that regional variation in surgical care across geographic areas is often not fully explained by variations in population morbidity; 7 and second by our correlation analysis, which indicates that hospital districts with high incidence rates at the beginning of the study period tended to maintain these elevated rates over time, suggesting that stable regional practice patterns may persist independent of changes in the underlying morbidity.
In addition, our study did not delve into an in-depth analysis of the differences in the risk factors associated with CTS surgery or UN surgery potentially influencing regional incidence rates, similarly as seen in other European countries.11,12 For example, diabetes exhibited some geographical variation in Finland prior to the 2000s. 26 In contrast, obesity showed minimal regional variation in Finland during the late 1990s and early 2000s. 27 Recent data indicate that both diabetes and obesity now display some regional disparities throughout Finland. 28 Further analysis of diabetes and obesity variations is needed to understand their contribution to the observed disparities in CTS and UN surgeries, though we anticipate they explain only a small fraction of the variation.
While we believe that access to surgical or non-surgical care is unlikely to be a major limiting factor in Finland, we acknowledge that we do not possess detailed numerical data on specialist density, waiting times, referral patterns, or diagnostic service availability at the regional level. As such, we are unable to directly assess the extent to which supply-side factors could influence regional surgery rates. Future studies incorporating these data are needed to evaluate this hypothesis more directly.
To conclude, this study revealed high disparities in the utilization of CTS and UN surgeries are unlikely to be explained by population needs. Instead, the findings indicate that the criteria for performing these surgeries vary considerably, suggesting a potential overuse in high-incidence areas. Identifying drivers behind the high utilization represents a potential gap that future research could address.
Supplemental Material
sj-docx-1-sjs-10.1177_14574969261458557 – Supplemental material for Regional variations in surgeries for carpal tunnel syndrome and ulnar nerve disorders: A registry-based study in Finland
Supplemental material, sj-docx-1-sjs-10.1177_14574969261458557 for Regional variations in surgeries for carpal tunnel syndrome and ulnar nerve disorders: A registry-based study in Finland by Vieda Lusa, Ville Ponkilainen, Anniina Laurema, Ville M. Mattila and Teemu Karjalainen in Scandinavian Journal of Surgery
Footnotes
Authors contributions
VP, AL, VMM, and TK made a substantial contribution to the concept of the work. VP made a substantial contribution to the acquisition and analysis of the data. VP and TK made a substantial contribution to the interpretation of data. VL drafted the article. VP, AL, VMM, and TK revised the manuscript critically for important intellectual content. VL, VP, AL, VMM, and TK approved the version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.