
Abstract
Background:
Robotic-assisted transabdominal preperitoneal repair (rTAPP) is increasingly used for inguinal hernia. However, evidence on its implementation in district hospitals and its integration into resident training programs remains limited. The aim of this study was to assess a real-world implementation of rTAPP in a public district hospital.
Methods:
Patients with inguinal hernia who underwent rTAPP between May 2024 and May 2025 were included. Perioperative outcomes, quality of life (QoL), and recurrence within the first 6 months were assessed. Implementation was analyzed across three consecutive phases to evaluate changes in operative performance and trainee involvement. QoL was measured using the 5-level EQ-5D version (EQ-5D-5L) in a subset of patients with available pre- and postoperative data.
Results:
A total of 120 patients underwent rTAPP. There were no conversions to laparoscopic or open surgery. Postoperative complications were observed in 8 (6.7%) patients and were limited to Accordion grade I–II events. The median length of postoperative stay was 20 h. One patient (0.8%) experienced hernia recurrence within 6 months. In contrast with phase 1, resident surgeons performed rTAPP in phases 2 (15%) and 3 (12.5%). Mean operative time decreased from 86 min in phase 1 to 74 and 77 min in phases 2 and 3, respectively (p = 0.041) without a significant difference in postoperative complications. Paired EQ-5D-5L data demonstrated significant postoperative improvement in pain/discomfort, daily activities, and overall health score.
Conclusion:
Robotic-assisted inguinal hernia repair can be safely implemented in a district hospital setting with favorable short-term outcomes. Structured introduction of rTAPP allowed rapid involvement of surgeons without compromising perioperative safety or efficiency.
Introduction
Robot-assisted inguinal hernia repair is widely considered safe and feasible. However, evidence for clinical advantages over conventional laparoscopic repair remains inconsistent. Prior comparative studies have reported higher costs and longer operative times for robot-assisted transabdominal preperitoneal repair (rTAPP) than for laparoscopic transabdominal preperitoneal repair (TAPP).1–3 A systematic review from 2021 found lower complication rates with rTAPP compared with open and laparoscopic repair, but longer operative times. 4 De Angelis et al. 5 report lower recurrence rates after robotic inguinal repair compared to its laparoscopic counterpart, as well as less use of opioids than after open surgery. More recently, a Danish randomized trial demonstrated shorter operative times for rTAPP than laparoscopic TAPP. 6
The high acquisition and maintenance costs of robotic platforms may limit implementation in publicly funded hospitals. In Norway, hospitals face increasing pressure to reduce costs while maintaining surgical capacity and resident training. 7 Implementation of robotic platforms has traditionally been built upon selective training of a limited number of surgeons aimed at expediting the learning curve through increased surgical volume. At the same time, such approach may reduce training opportunities for other surgeons and affect workforce sustainability. No previous studies have examined the generalizability of simultaneous rTAPP training within a consultant workforce in its implementation phase.
This study aimed to evaluate the implementation and short-term outcomes of rTAPP in a district hospital setting. We hypothesized that the learning curve for rTAPP would be short in a unit with established experience in laparoscopic inguinal hernia repair despite the large number of surgeons involved in training on the robotic platform.
Methods
Patients, study design, and data collection
This prospective single-center cohort study was conducted at Ringerike Hospital (Hønefoss, Norway), part of Vestre Viken Hospital Trust, serving around 87,650 residents with 112 inpatient beds. All patients undergoing primary rTAPP for inguinal hernia between May 2024 and May 2025 were identified from the institutional hernia registry and included in this study (Data Protection Officer ID: 24/07718-3). In the same time period, some patients underwent open repair (Lichtenstein) and laparoscopic total extraperitoneal repair (TEP). Patients undergoing open surgery had recurrent hernias, previous abdominal surgery, and higher American Society of Anesthesiologists (ASA) grades, which, in some cases, precluded general anesthesia. As for the laparoscopic TEP, these were mostly attributed to the transition phase from laparoscopy to robot. In fact, no TEP has been performed at our institution since March 2025.
The primary endpoints were perioperative results, short-term recurrence, and patient-reported quality of life (QoL). To evaluate implementation, outcomes were compared across three consecutive periods (40 patients per period). In period 1, procedures were performed by consultant surgeons experienced in laparoscopic inguinal hernia repair. In periods 2 and 3, residents progressively participated as console surgeons under consultant supervision. Differences in case mix, operative time, and perioperative outcomes throughout periods were assessed.
Pre- and perioperative variables were entered into the registry by the operating surgeon. Postoperative data were collected by a research nurse. Complications and readmissions were retrieved from the electronic medical record. Follow-up was conducted by telephone; patients with suspected recurrence or persistent symptoms were evaluated at the outpatient clinic. Patients unable to complete telephone follow-up because of language barriers (not proficient in Norwegian or English) or cognitive impairment were excluded from follow-up analyses.
Definitions
Operative time was defined as the time from skin incision to closure. Hernia defect size was measured intraoperatively. Conversion was defined as an intraoperative change to conventional laparoscopy or open surgery. Intraoperative incidents were registered. Postoperative complications were defined and graded using the Accordion classification; severe complications were defined as Accordion grade >II. 8
Recurrence and QoL were assessed at follow-up. Health-related QoL was measured using the 5-level EQ-5D version (EQ-5D-5L) preoperatively and at 6 months after surgery. 9 This instrument was introduced in January 2025 and, therefore, was not available for patients operated earlier. Postoperative pain and sensory symptoms (e.g. numbness) were also recorded.
Implementation and surgical technique
The first robotic case was performed in May 2024. All consultant general surgeons and all residents were trained on the daVinci X platform within 12 months. During the first 12 months, 14 surgeons (consultants and residents) performed robotic procedures; nine performed rTAPP for inguinal hernia during the study period. The first four cases in May 2024 were proctored by an Intuitive Surgical proctor. A standardized rTAPP technique, similar to previously published reports, was adopted, taught, and used by all surgeons. 10 The procedure started by establishing pneumoperitoneum via the Veress needle. Ports were placed in a horizontal line approximately 20 cm above the pubic symphysis using three 8-mm robotic ports; an additional assistant port (11 mm) was used selectively. Dissection proceeded medially to 2 cm below the pubic symphysis and 2 cm lateral to the midline, followed by lateral dissection. The hernia sac and peritoneum were reduced to the level of the psoas muscle. A self-fixating mesh (Progrip™, 12 × 16 cm, Medtronic) was placed, and the peritoneal flap was closed. Fascial defect closure was not performed.
Statistics
Continuous variables were presented as mean ± standard deviation (SD) or median (range), depending on distribution. The latter was used for non-normally distributed continuous data, while means were applied for normally distributed data. Categorical variables were shown in frequency (percentage). Comparisons across periods were performed by using one-way analysis of variance (ANOVA) for normally distributed variables and the Kruskal–Wallis test for non-normally distributed variables. Post hoc testing was used to verify statistically significant ANOVA results; the two-sided Mann–Whitney U test was applied for pairwise comparisons of medians. Pre- and postoperative QoL outcomes were compared using paired t-tests. Categorical variables were compared using the chi-square or Fisher’s exact tests. A two-sided p-value < 0.05 was considered statistically significant.
Results
Perioperative outcomes
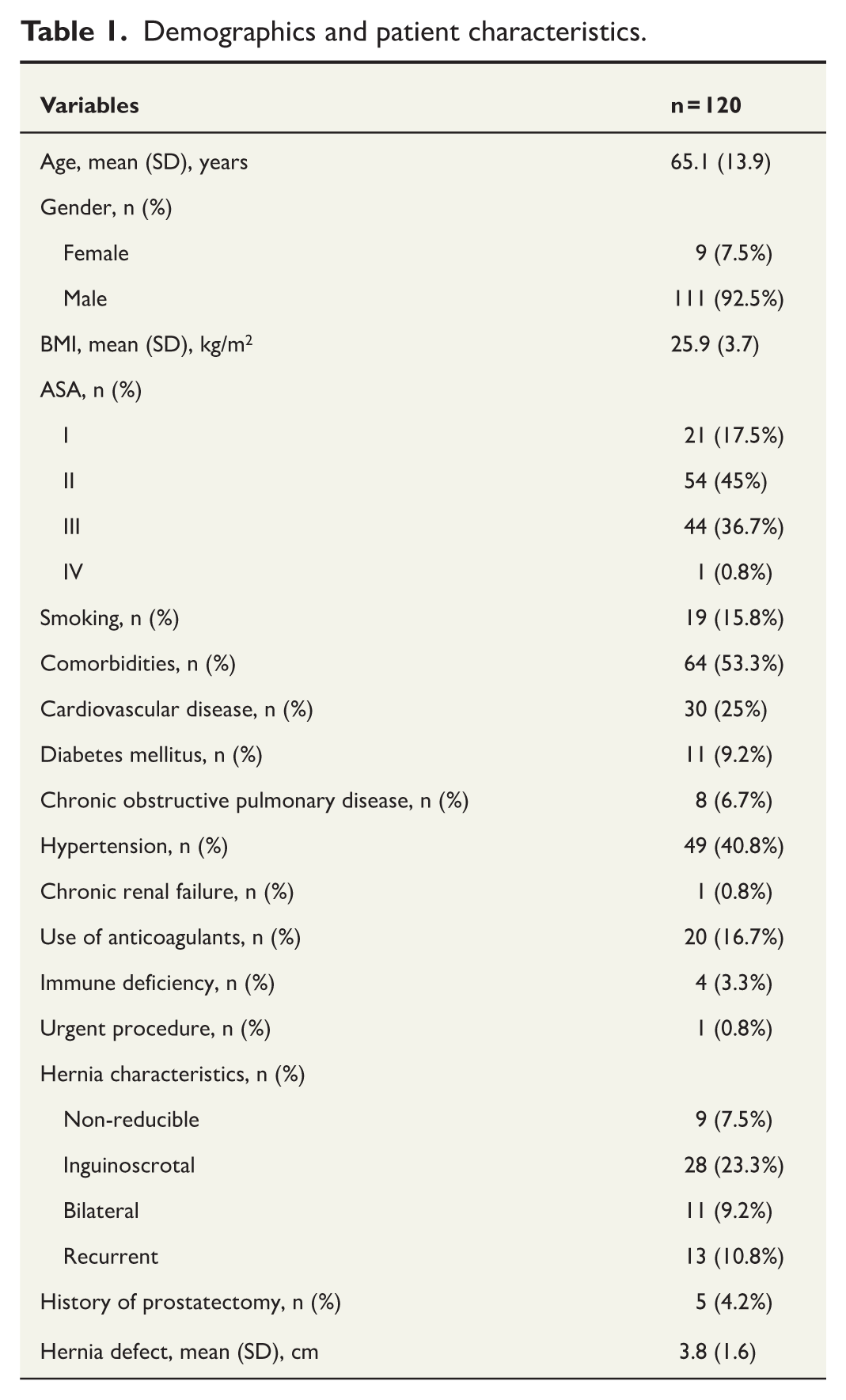
A total of 144 inguinal hernia repairs were performed during the study period. Of these, 120 (83.3%) patients underwent rTAPP, while 16 (11.1%) and 8 (5.6%) were operated by Lichtenstein repair and TEP, respectively. In the rTAPP population, the majority were men (92.5%) with a mean age of 65 years (Table 1). Inguinoscrotal hernia was present in 28 patients (23.3%), and 13 patients (10.8%) underwent repair for recurrent hernia. Bilateral hernia repair was performed in 11 (9.2%) cases.
Demographics and patient characteristics.
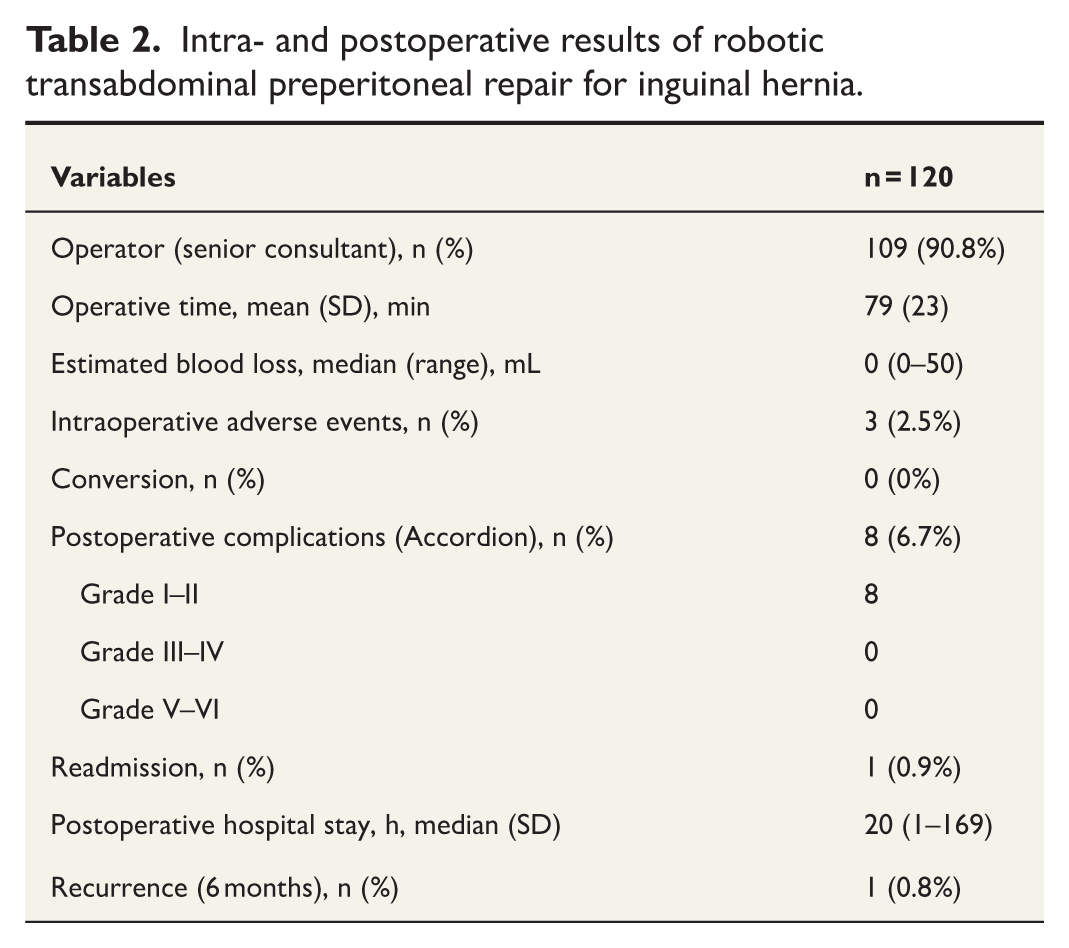
Senior consultant surgeons performed 109 (90.8%) procedures, while 11 (9.2%) procedures were performed by resident surgeons under supervision (Table 2). No conversions to laparoscopic or open surgery occurred. Intraoperative adverse events occurred in three (2.5%) patients, including bleeding (n = 2) and a peritoneal tear unrelated to the dissection area (n = 1). Postoperative complications were observed in 8 (6.7%) patients and were limited to Accordion grade I–II events. These included urinary tract infection or urinary retention (n = 4), hematoma/seroma (n = 2), and minor cardiac events (n = 2). The median postoperative hospital stay was 20 h.
Intra- and postoperative results of robotic transabdominal preperitoneal repair for inguinal hernia.
Recurrence and QoL
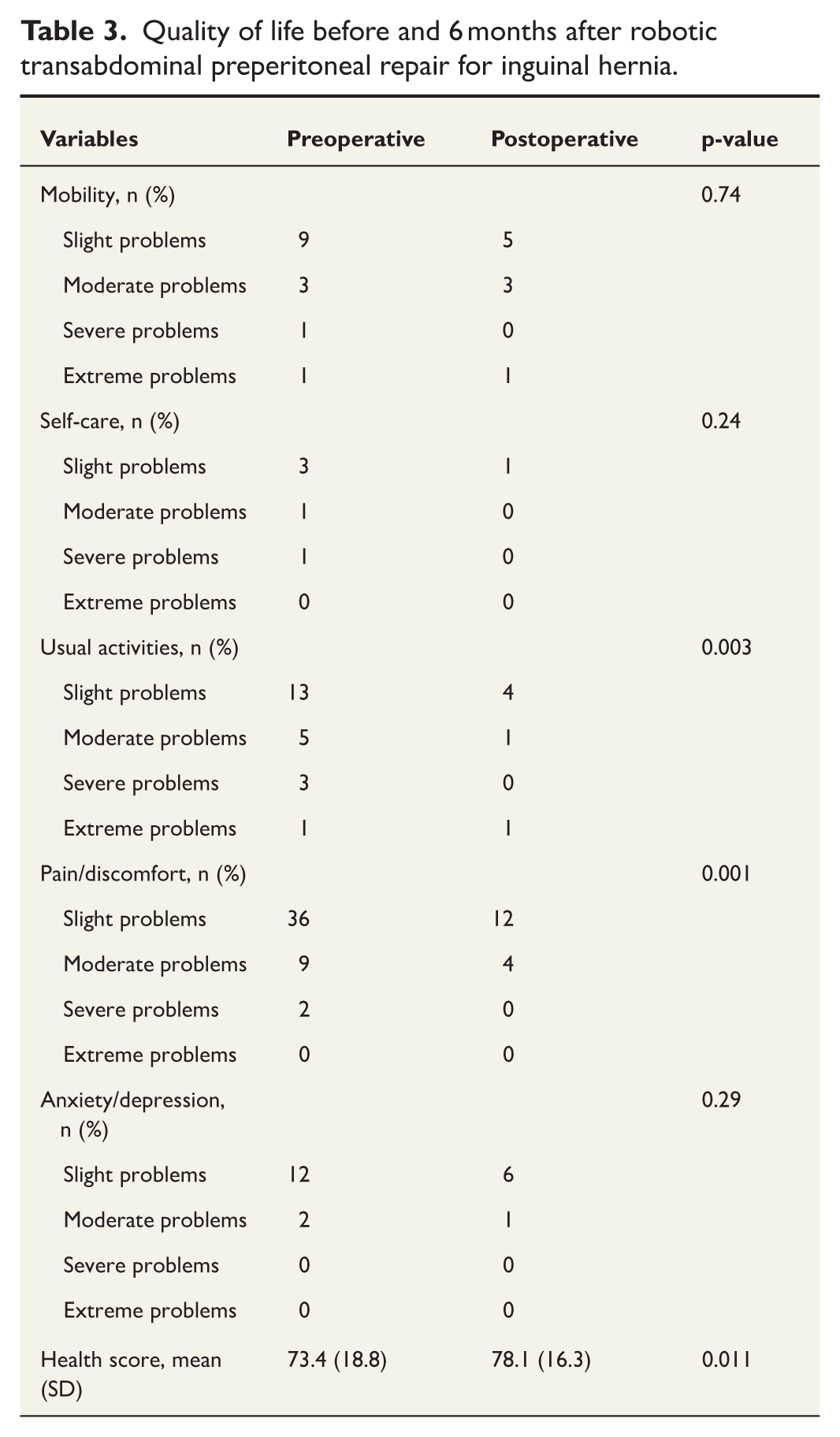
One patient (0.8%) experienced hernia recurrence within 6 months after surgery. Postoperative pain was reported by nine patients, while seven reported numbness in the operation area. Data on pain and numbness were missing in four patients. Paired pre- and postoperative EQ-5D-5L data were available for 60 patients. Significant postoperative improvements were observed for daily activities and pain/discomfort domains (Table 3). Mean self-reported health score significantly increased from 73.4 to 78.1 (p = 0.011).
Quality of life before and 6 months after robotic transabdominal preperitoneal repair for inguinal hernia.
Implementation phases
Patient demographics and baseline characteristics were comparable between periods (Table 4). A higher proportion of inguinoscrotal hernias was observed in period 3, although this difference did not reach statistical significance (35 versus 15 versus 20%, p = 0.09).
Outcomes of robotic transabdominal preperitoneal repair for inguinal hernia in three consecutive time periods.
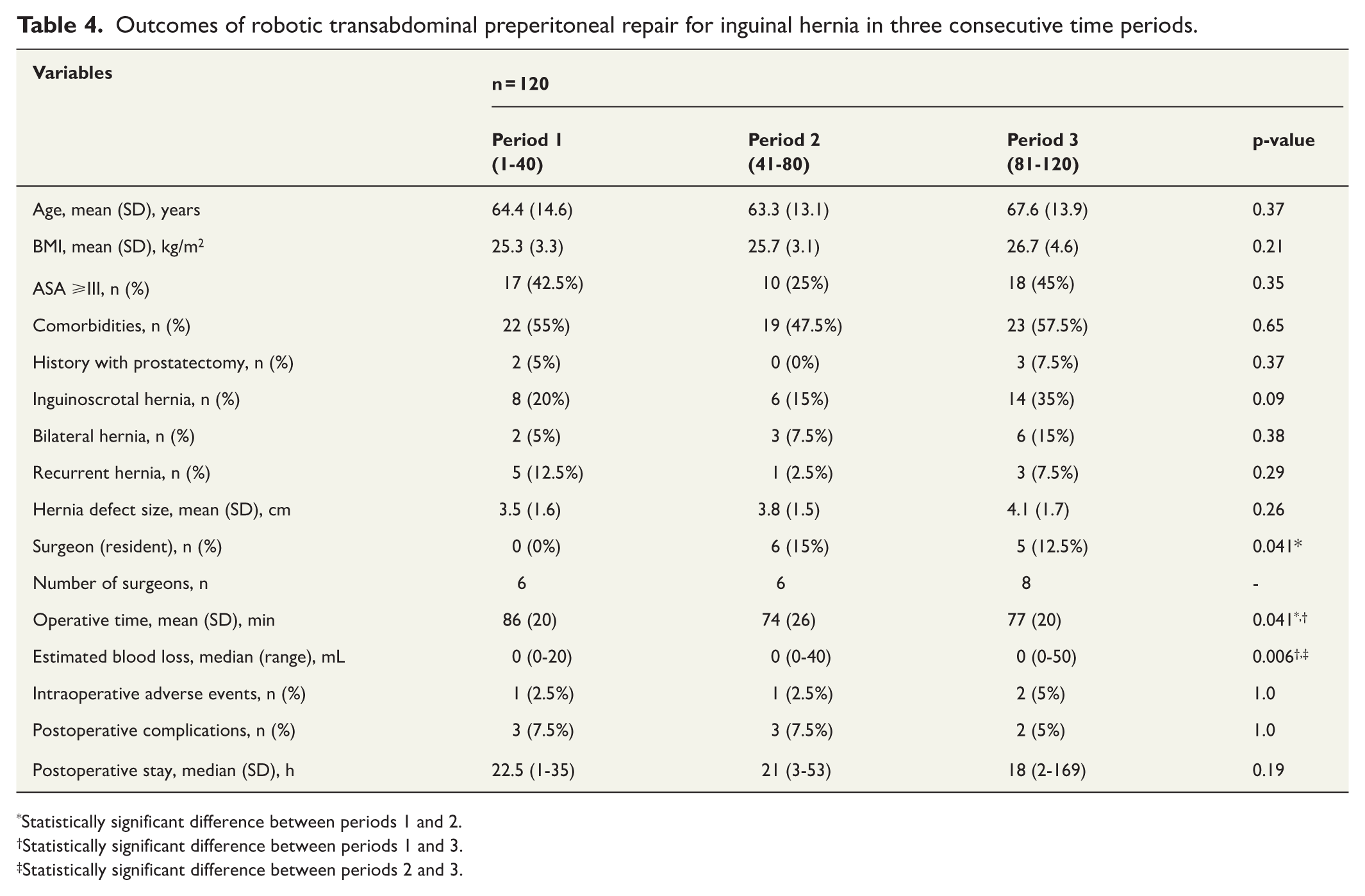
Statistically significant difference between periods 1 and 2.
Statistically significant difference between periods 1 and 3.
Statistically significant difference between periods 2 and 3.
All procedures in period 1 were performed by senior consultant surgeons. Resident surgeons performed 15% and 12.5% of procedures in periods 2 and 3, respectively (p = 0.041). Mean operative time decreased from 86 min in period 1 to 74 and 77 min in periods 2 and 3, respectively (p = 0.041). Median estimated blood loss increased across periods but remained clinically negligible. The incidence of postoperative complications and length of hospital stay were similar in the three periods.
Discussion
This prospective cohort study demonstrates that rTAPP can be safely implemented in a district public hospital with favorable short-term outcomes. The proportions of recurrent and inguinoscrotal hernias treated in this cohort were comparable to those reported in the literature (Table 5).3,11–15 The complexity of the procedures increased during the study period, correctly demonstrating the institutional learning curve. Perioperative results, complication rates, and early recurrence were within the ranges reported in previous studies, despite the involvement of multiple surgeons and progressive inclusion of residents. Patient-reported QoL improved following surgery in the subset of patients with available paired EQ-5D-5L data. While EQ-5D-5L is not hernia-specific, and data were available for only half of the cohort, the observed improvements in pain/discomfort and daily activities demonstrate patient recovery after rTAPP. There is no reason to expect significant differences in QoL for the patients treated before January 2025; however, we will need long-term outcome data to support our findings.
Studies addressing the implementation of robotic transabdominal preperitoneal repair for inguinal hernia and their main findings.
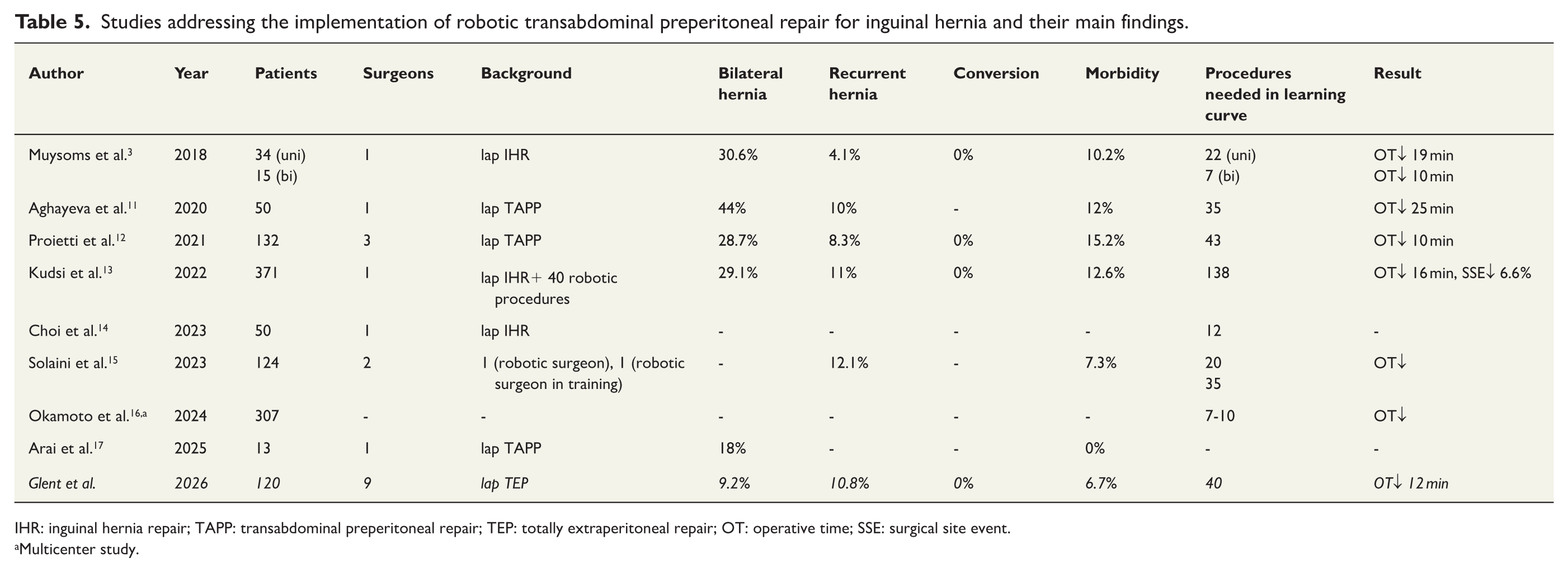
IHR: inguinal hernia repair; TAPP: transabdominal preperitoneal repair; TEP: totally extraperitoneal repair; OT: operative time; SSE: surgical site event.
Multicenter study.
Several studies have demonstrated comparable results for laparoscopic TEP/TAPP and rTAPP.2,3,5 Possible advantages of rTAPP compared to its laparoscopic counterpart are the possibility for direct visual guidance and instruction peroperatively when training residents. Improved surgical dexterity and good visualization may help reduce cognitive stress and facilitate learning. 9 Furthermore, a double console greatly facilitates resident involvement during surgery. The double console was available in our hospital from period 3. During the study period, 83.3% of all inguinal hernia repairs were done robotically. We believe that the implementation of rTAPP was facilitated by our dedicated transition from laparoscopy to robotics, allowing for a high case volume and shortening our institutional learning curve.
Several reports on rTAPP implementation originate from specialized or high-volume centers, often involving a limited number of surgeons.16–19 In contrast, the present study reflects routine clinical practice in a publicly funded district hospital, where both elective surgery and resident training are core responsibilities. One of the key findings of this study is that operative time decreased over successive implementation phases despite increasing resident participation. This suggests that structured training, standardization of technique, and early proctoring may mitigate the effects of lower individual case volumes per surgeon. Importantly, increased trainee involvement was not associated with higher complication rates, longer hospital stays, or increased short-term recurrence. The number of residents increased in periods 2 and 3 but remained overall low for the first 12 months of implementation. The residents included had previous experience with laparoscopic general surgery, including laparoscopic TEP, and were the most senior ones (n = 2) in the department. Privileged with good access to the robot, we focused early on resident training and aimed to include residents as early as possible.
This study has several limitations. Follow-up was limited to 6 months, precluding assessment of long-term recurrence. The absence of a comparator group prevents direct comparison with laparoscopic/open techniques, although this was not the focus of the study. In addition, QoL assessment was introduced midway through the study period, resulting in a substantial amount of missing data. Furthermore, EQ-5D-5L is a generic instrument for QoL assessment, thus not specific to patients with hernia. These factors limit the generalizability of the findings.
The strengths of the study include its prospective design, complete perioperative data capture, and evaluation of implementation across an entire surgical unit. Our findings suggest that rTAPP can be integrated into district hospital practice without compromising patient safety or surgeon training when a structured implementation strategy is applied.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.