
Abstract
Background and aims:
Perioperatively used, topically administered tranexamic acid (TXA) has attracted increasing interest in plastic surgery, and several studies have compared the effectiveness and safety of topical and intravenous (IV) administration. Topical TXA has been reported to have an equal or superior effect in reducing postoperative bleeding and transfusion requirements, with no increase in reported adverse events. Although prophylactic topical TXA is believed to result in cost savings, cost-effectiveness analyses concerning the use of TXA in breast surgery have not yet been reported.
Methods:
This single-center, retrospective cohort study calculated the costs for all patients who underwent reduction mammaplasty between 2019 and 2021 at Jorvi Hospital, Finland. We compared postoperative complications and total healthcare costs associated with surgery between two groups: patients who received topical TXA perioperatively (TXA group) and patients who did not receive TXA (non-TXA group). Total costs were analyzed, including both the intraoperative and postoperative periods. All costs were calculated in euros, based on the 2020 Helsinki University Hospital (HUS) rates.
Results:
In 328 breast reduction surgeries, the leading postoperative costs were caused by reoperations, and additional ward stays due to complications. The cost of TXA irrigation itself was negligible compared with the other expenses. The median postoperative costs were €414 in the non-TXA group and €335 in the TXA group, and the mean postoperative costs were €874 in the non-TXA group and €453 in the TXA group (p = 0.002). In the non-TXA group, 11 patients (6.1%) underwent reoperation for hematoma and four (2.2%) for other wound-healing complications. In contrast, in the TXA group only one (0.7%) patient required reoperation for hematoma and one (0.7%) for wound-healing complications.
Conclusion:
This study demonstrates that the application of this low-cost drug may reduce the overall costs associated with reduction mammaplasty.
Introduction
Reduction mammaplasty is a commonly performed, quality-of-life–improving procedure in public health care in Finland and many Western countries, and its cost-effectiveness has been demonstrated, with a low cost per quality-adjusted life year (QALY). 1 Postoperative hematoma is a clinically significant adverse event following this procedure and may be associated with reduced patient well-being, increased morbidity, and higher healthcare costs due to the need for emergency reoperation. Previous studies have shown that topical TXA reduces postoperative bleeding.2–4
In Finland, health care is primarily the responsibility of regional authorities that organize and fund services. Public health care is financed through taxation, patient fees, and employer contributions. In addition, private health insurance and donations may contribute, but their role is minor. 5 Healthcare funding has undergone changes in recent years, but still taxes remain the primary source of funding. Patients are charged small, heavily subsidized fees for certain services, such as doctor visits, inpatient days, and examinations. These fees are regulated by law and have maximum limits. 6 There is also an annual ceiling on patient fees, after which most services are free of charge. The provider of the services (municipality or well-being services county) is responsible for implementing the fees, and these must not exceed the actual costs and must remain reasonable.7,8 It should be noted that the costs reported in this article do not correspond to the amounts paid by patients, but rather represent the costs invoiced by the hospital to the municipality (Table 1).
Patient characteristics, postoperative outcomes and resource utilization.
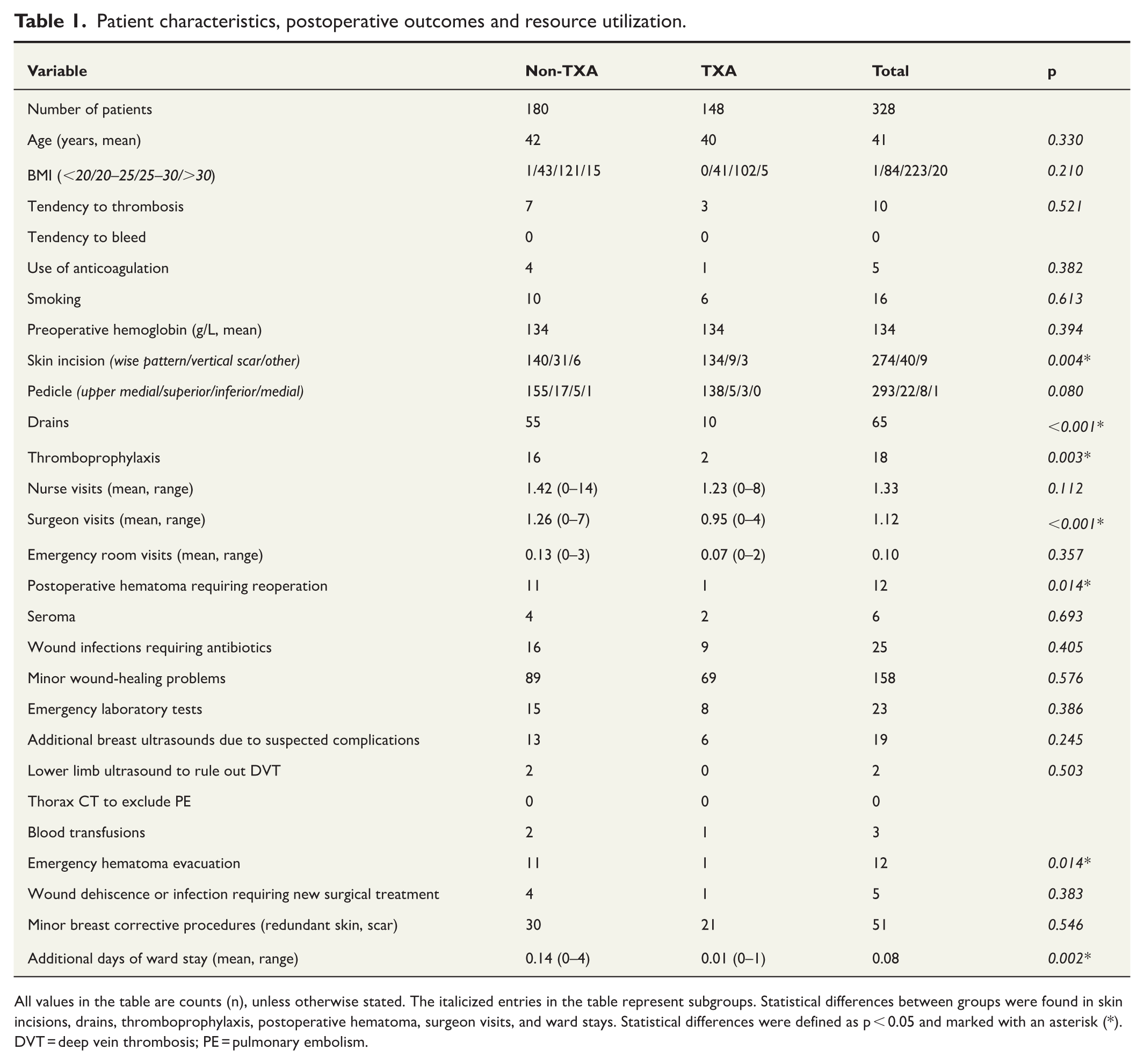
All values in the table are counts (n), unless otherwise stated. The italicized entries in the table represent subgroups. Statistical differences between groups were found in skin incisions, drains, thromboprophylaxis, postoperative hematoma, surgeon visits, and ward stays. Statistical differences were defined as p < 0.05 and marked with an asterisk (*). DVT = deep vein thrombosis; PE = pulmonary embolism.
The present cost analysis aims to focus on potential differences in expenses between reduction mammaplasty patients treated with topical TXA and those not treated with TXA. We aim to quantify baseline and additional costs of reduction mammaplasty, acknowledging confounding factors, and to assess the possible cost benefits associated with reduced postoperative bleeding following topical TXA administration.
Methods
This retrospective study covered the period between 2019 and 2021 and included patients who underwent solely bilateral reduction mammaplasty at HUS Jorvi Hospital in Finland. The real total cost of reduction mammaplasty consists of pre-, intra-, and postoperative care costs. The preoperative period was excluded from the analysis because the preoperative evaluations were similar across all patients, independent of TXA administration. In this report, we thus refer to total costs as intra- and postoperative costs. Data collection was performed at the beginning of 2025, and the patients were retrospectively followed using postoperative patient medical records. We applied the cost model used during the study period from 2019 to 2021. Pricing information was obtained directly from the 2020 internal rates of HUS, which serve as the basis for invoicing patients’ regions of residence.
Patient demographic data, as well as details concerning intraoperative and postoperative follow-up visits, treatments, and complications, were collected retrospectively from patient medical records. The two study groups consisted of patients whose wounds were rinsed with topical TXA (TXA group) and patients who did not receive TXA, either topically or systemically (non-TXA group). For clarity, patients who received systemic TXA (IV or oral) were excluded from the study. The results were compared between the two main study groups. Other exclusion criteria were unilateral reduction mammaplasty or operations that included other simultaneous surgical interventions.
In the TXA group, the TXA solution was applied intraoperatively directly to the wound just before closure. The solution had a concentration of 20 mg/mL and was prepared by diluting 1000 mg (10 mL) of TXA in 40 mL of sodium chloride. It was then divided equally between both breasts (25 mL per breast). The solution was used to irrigate the surgical wound, either while still open or partially closed, depending on the surgeon’s preference. Patients in the non-TXA group had their wounds irrigated with saline solution or not irrigated at all.
According to publicly funded healthcare billing principles, intraoperative costs are calculated as a fixed fee based on the procedure; individual expenses incurred during surgery are not billed separately, and the duration of the operation does not affect the overall cost. Under this billing system, the use of tranexamic acid on the surgical wound during surgery does not, according to the HUS price list, increase the total procedural cost. However, when reporting actual expenditures, it is important to specify the cost of tranexamic acid at HUS. The product used, Tranexamic acid Orion® 100 mg/ml, 5 mL ampoule, cost €1.60, and the required saline diluent—either sodium chloride 0.9% B. Braun® 100 mL (€0.49) or sodium chloride 0.9% Fresenius Kabi® 2 × 20 mL (€0.42)—was used at HUS in 2020.
Statistical analysis
The data were analyzed using IBM SPSS Statistics (Version 29). Categorical variables were compared between the TXA and non-TXA groups using Pearson’s chi-square test, Fisher’s exact test, and the Fisher–Freeman–Halton test, as appropriate. Ordinal and continuous variables were analyzed using the Mann–Whitney U test, as the assumption of normality was not met. All tests were two-tailed, and a p value of <0.05 was considered statistically significant.
Results
A total of 328 patients were included in the study. Of these, 180 patients were not treated with TXA (non-TXA group), while 148 patients received topical TXA before wound closure (TXA group) (Fig. 1). The demographic data are illustrated in Table 1.
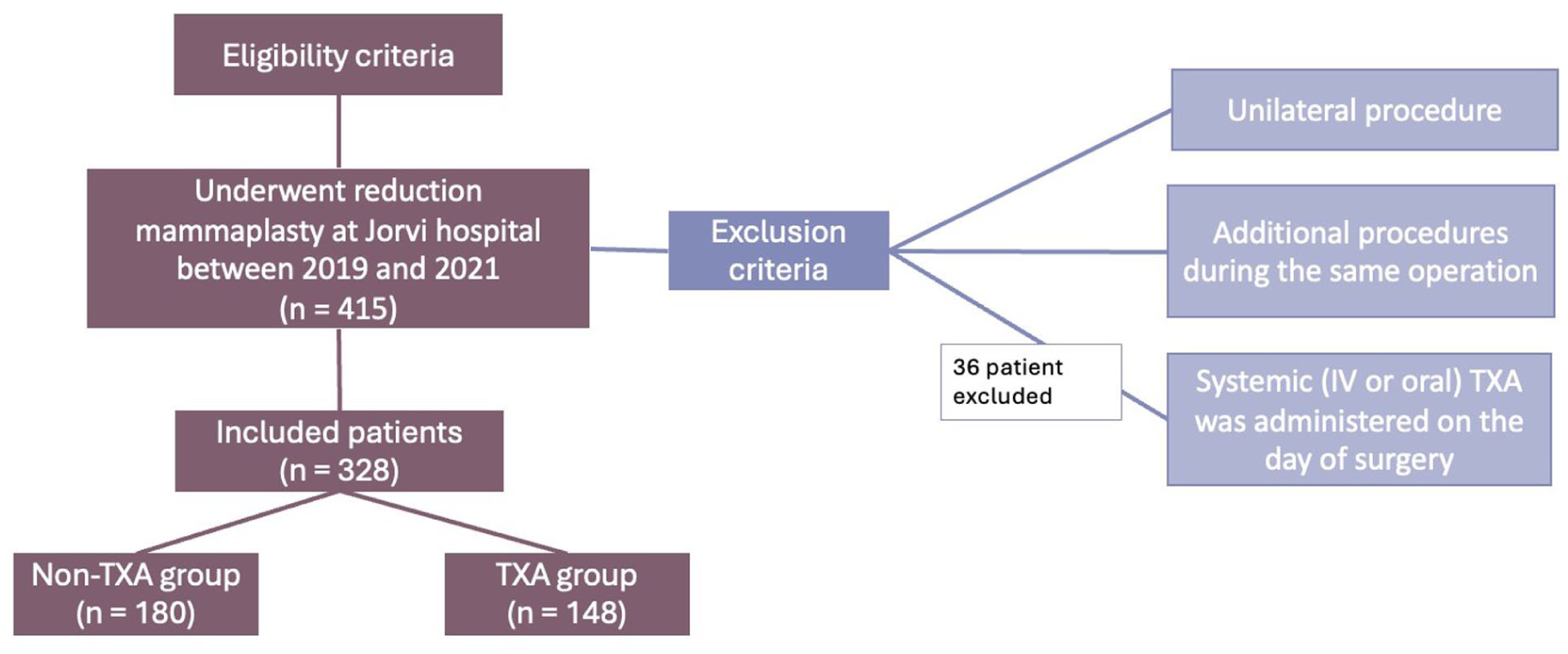
Flowchart of patient selection criteria.
The cost of reduction mammaplasty in the HUS hospital district, in the plastic surgery unit, was €4277 per elective procedure in 2020. This value was standardized for all patients, even though the price varied slightly between different years. The postoperative costs were divided into baseline and additional costs. Standard postoperative costs comprise one visit with a wound care nurse and one or two surgeon outpatient clinic visits. Postoperative costs were compared between the study groups (TXA versus non-TXA). Table 2 summarizes the events leading to these costs. The postoperative costs were significantly higher in the non-TXA group after surgery. The median postoperative costs were €414 in the non-TXA group and €335 in the TXA group, and the mean postoperative costs were €874 in the non-TXA group and €453 in the TXA group (p = 0.002).
Postoperative costs that may increase the total cost of reduction mammaplasty.
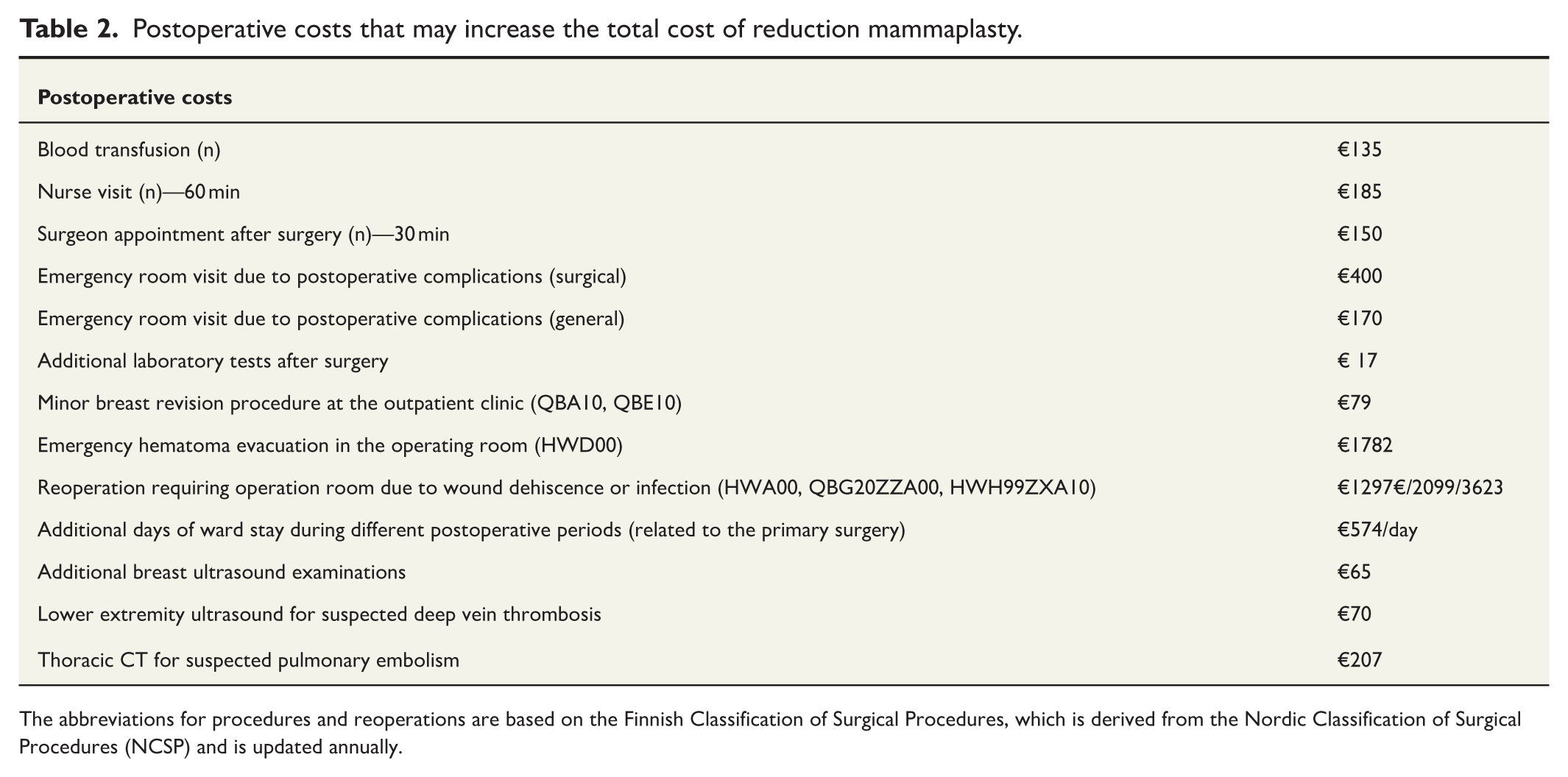
The abbreviations for procedures and reoperations are based on the Finnish Classification of Surgical Procedures, which is derived from the Nordic Classification of Surgical Procedures (NCSP) and is updated annually.
Total costs and cost categories of postoperative treatment
The total cost consisted of the surgery itself plus postoperative costs related to the primary reduction mammaplasty or to any reoperation resulting from it (Table 2). The average total costs were €4961, being €5151 among non-TXA patients and €4730 among TXA patients.
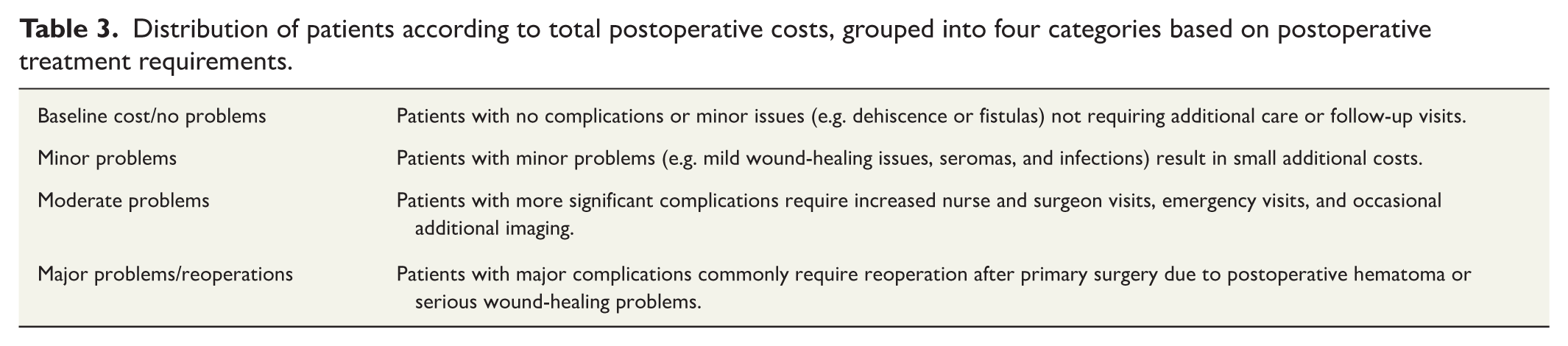
To obtain a rough overview of how total costs, based on postoperative needs, were distributed among patients, we divided the cohort into four groups (Table 3). Fig. 2 summarizes the main results of the study. The topical TXA group predominated in the baseline “no complications” category, whereas the non-TXA group predominated in the major complications and reoperation category. The need for reoperation due to complications, such as postoperative hematoma, accounted for the largest increase in total costs.
Distribution of patients according to total postoperative costs, grouped into four categories based on postoperative treatment requirements.
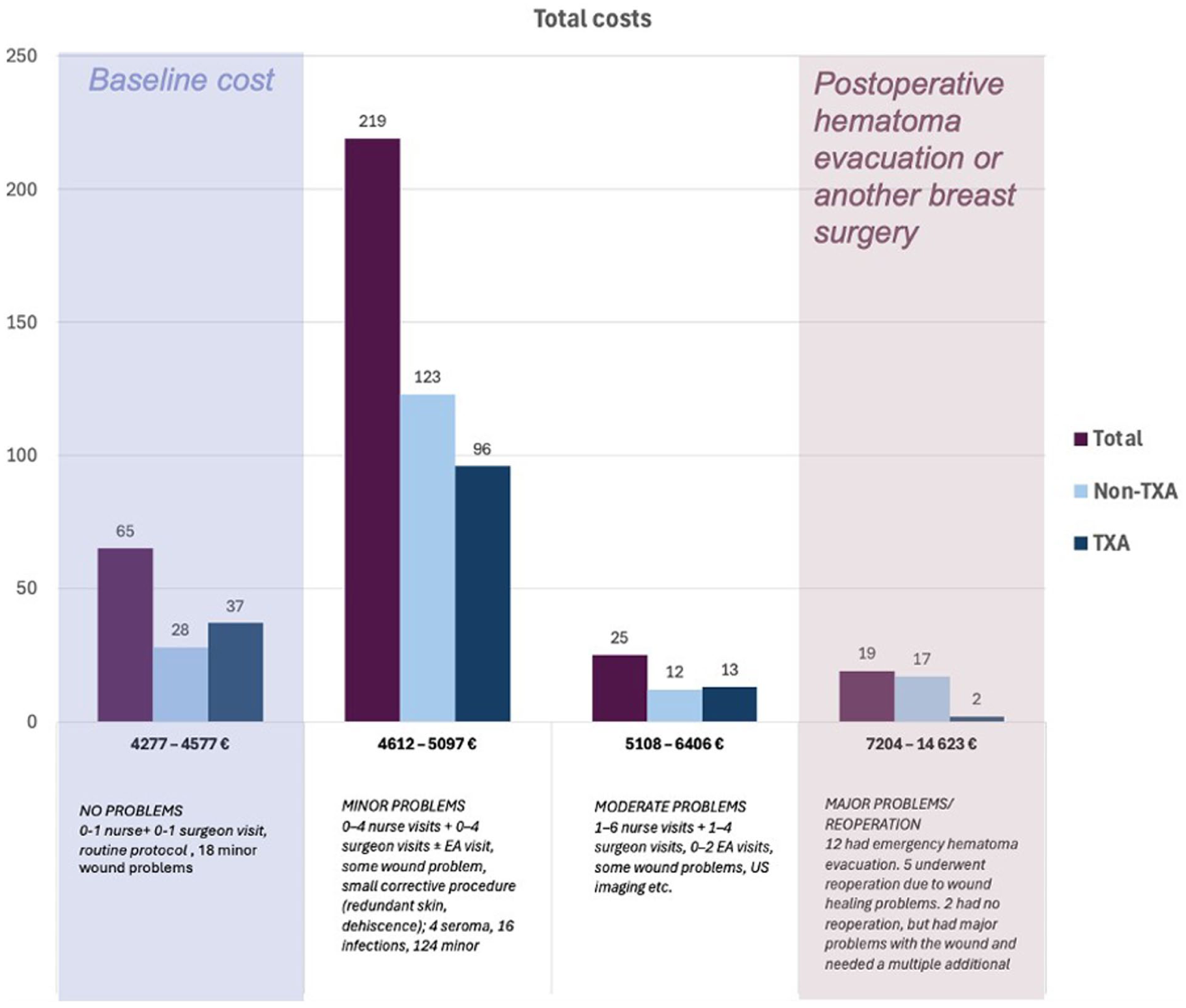
Distribution of total healthcare costs following reduction mammaplasty.
Differences in postoperative complications between the two groups
There were significant differences between the TXA and non-TXA groups regarding the development of postoperative hematoma and need for emergency hematoma evacuation surgery (p = 0.014), with a higher incidence in the non-TXA group (11 of 180 patients, 6.1%) compared with the TXA group (1 of 148 patients, 0.7%). The absolute risk reduction (ARR) for postoperative hematoma was 5.4%, corresponding to a number needed to treat (NNT) of 19. 9
The total number of revision surgeries due to wound-healing problems or infections was limited, with five patients requiring reoperation. Of these, four were in the non-TXA group (2.2%), and one was in the TXA group (0.7%), resulting in numbers too small to allow reliable statistical comparison between the groups (Fig. 3). There were no notable differences between groups when comparing the incidence of postoperative seroma, wound infections, or other minor wound-healing problems (ns).
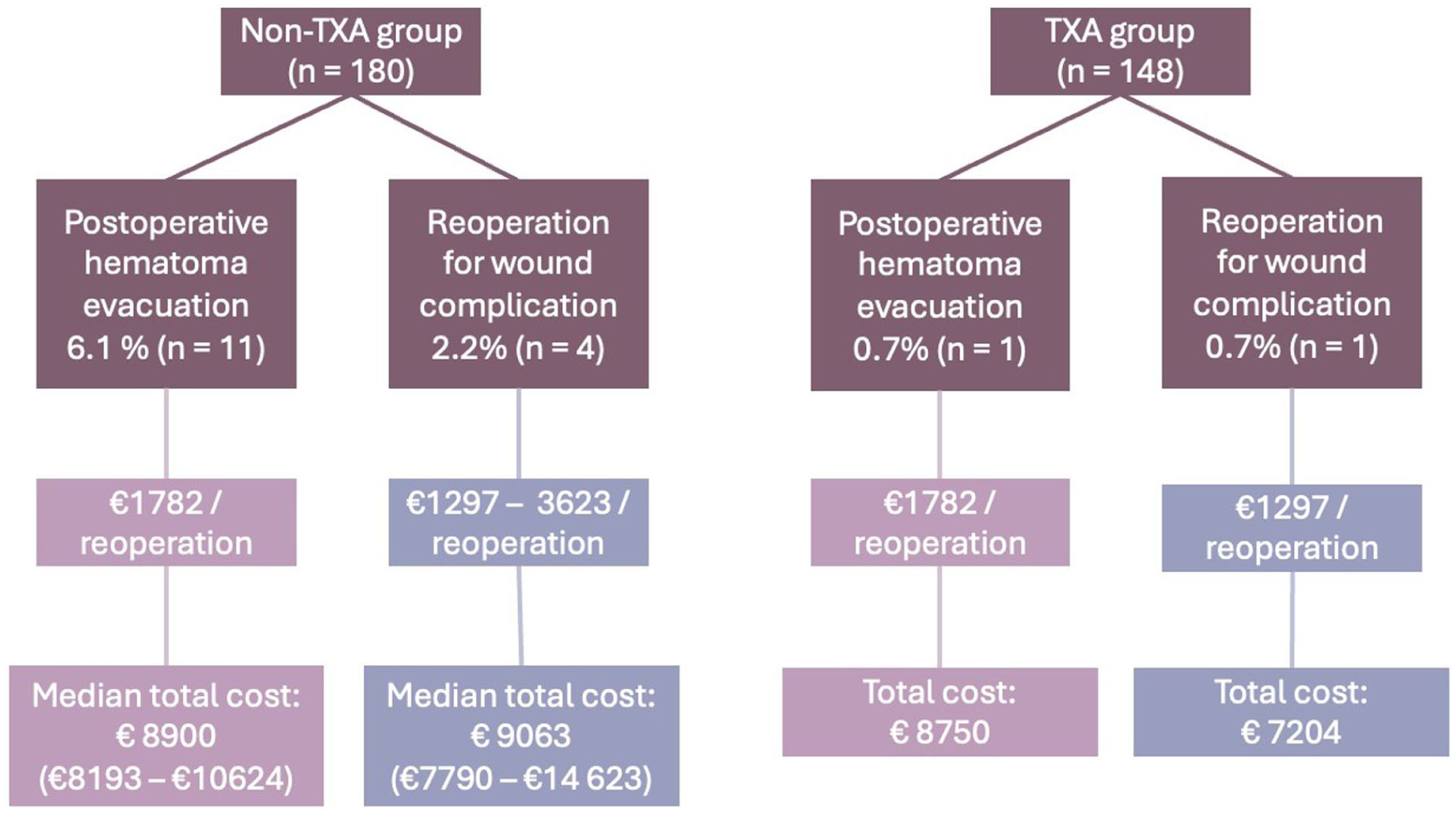
Reoperations were required due to postoperative hematomas or wound complications in the TXA versus non-TXA groups.
Postoperative follow-up and treatment requirements
Fifteen (4.6%) of 328 patients required additional ward stays due to reoperation after primary surgery. Reoperations were more frequent in the non-TXA group, resulting in significantly more additional postoperative ward stays (TXA group, 1 patient (0.7%); non-TXA group, 14 patients (7.8%); p = 0.002). Additional ward days varied from one to four days (1 day: 9 patients; 2 days: 2 patients; 3 days; 2 patients; 4 days: 2 patients). The cost per additional day in the ward was €574, resulting in total costs for these additional stays ranging from €574 to €2296. We did not include ward stay costs for patients who remained in the ward by prior agreement after primary surgery.
A total of 19 patients (13 non-TXA versus 6 TXA; ns) required additional postoperative breast ultrasound (US) due to suspected infectious abscess, seroma, or hematoma. In some cases, the indication for the additional US examination was the presence of a palpable lump or nodule in the breast. Three patients required two additional US examinations to confirm the diagnosis.
Two of the 328 patients underwent lower extremity ultrasound due to suspected postoperative deep vein thrombosis (DVT). In both cases, the diagnosis of DVT was confirmed, and both patients were in the non-TXA group. In one patient, the DVT occurred one month after surgery, with the causal relationship to the operation unclear. The other patient also had a postoperative hematoma and underwent evacuation in the operating room, which involved two successive surgeries. Intravenous TXA is typically administered upon diagnosis of a postoperative hematoma and was also given in this case. There were no suspected cases of pulmonary embolism (PE) in either study group; consequently, no patients required thoracic CT.
A total of three patients (0.9%) received blood transfusions after the primary surgery due to low hemoglobin levels (postoperative hemoglobin, 83–100 g/L, with a hemoglobin decrease ranging from 13 to 51 g/L). Two of those who required transfusions were in the non-TXA group and developed postoperative hematoma, whereas one patient was in the TXA group and did not develop a postoperative hematoma requiring evacuation.
A postoperative wound care nurse visit, 10–14 days after surgery, was part of the routine protocol during the study period. Only 27 of the 328 patients (8.2%) did not attend a postoperative nurse follow-up at the hospital; at least nine of these patients instead visited a local primary healthcare nurse. Most patients (n = 236, 72%) had only one routine wound care nurse visit. Additional follow-up visits were scheduled if wound-healing problems were detected. Overall, 65 patients (19.8%) required additional wound care nurse visits. Most of those patients had 2–5 additional visits, but a few required numerous visits (6 (n = 2), 8 (n = 1), 9 (n = 1), or 14 (n = 1)). There was no statistical difference in the number of nurse visits between groups. It is, however, noteworthy that the two most problematic patients, who experienced substantial wound-healing complications and required 14 and 9 nurse visits, respectively, were both in the non-TXA group.
Furthermore, 259 patients (79%) had one or two postoperative follow-ups with the surgeon, and these were counted as part of the baseline costs. Fifty-four patients had no postoperative follow-up visits (TXA, n = 35; non-TXA, n = 19). Fifteen patients had more than two visits to the surgeon’s outpatient clinic for additional follow-ups (three to seven visits). Two-thirds of the patients who required additional visits were in the non-TXA group (p = 0.001).
Twenty-nine of the 328 patients (8.8%) required a total of 36 emergency room visits (23 patients once, 5 twice, and 1 three times) due to concerns related to the primary reduction mammaplasty (10 from the TXA group and 19 from the non-TXA group). Two of these patients had an emergency visit with a general practitioner, while the others were treated in a surgical or acute care emergency department. During the emergency room visits, only two of these patients were diagnosed with postoperative hematoma. All other hematomas had been detected immediately after surgery, before hospital discharge. Remaining emergency room visits presented with infection (n = 11), seroma (n = 5), or wound-healing problems (n = 20).
Demographic comparison of the two study groups
There were no significant differences between the main study groups (TXA and non-TXA) in age, body mass index (BMI), smoking status, anticoagulation use, or tendency to develop thrombosis (Table 2). In this patient group, there were no significant comorbidities. There were a few parameters that differed between the two groups, including drain use, thromboprophylaxis use, and surgical incision technique. In the non-TXA group, there were significantly more patients who received drains (p < 0.001). The patients receiving drains also displayed slightly more frequent revisits to the nurse (27.7% versus 17.8%). The two study groups also differed with regard to thromboprophylaxis use. Patients in the non-TXA group received low-molecular-weight heparin (LMWH) significantly more often than those in the TXA group (p = 0.002). A total of 10 patients had a thrombosis predisposition; of these, six received postoperative thromboprophylaxis, and all were predefined as inpatients. None of them experienced a thromboembolic event postoperatively. No patients had a known tendency to bleed. Skin incision techniques varied between the study groups; the wise-pattern incision dominated in both groups, but vertical incision was more common in the non-TXA group than in the TXA group (p = 0.004). The upper medial pedicle was predominant in both groups.
Discussion
This study describes the costs of reduction mammaplasty in Finland, identifies the sources of these costs, and demonstrates that an inexpensive and widely studied drug, tranexamic acid, may also reduce total surgical costs by decreasing hematoma formation and the need for reoperations. Cost-effectiveness studies on the use of topical tranexamic acid exist in other specialties, such as trauma 10 and orthopedics.11–13 Previous studies have shown significant cost-effectiveness with the use of topical TXA in orthopedic total hip and knee arthroplasty procedures by reducing blood transfusion rates.11–13 To our knowledge, no such cost-analysis studies of topical TXA have previously been conducted in plastic surgery breast procedures.
Postoperative costs primarily depend on wound healing and the occurrence of complications. Complications may occur independently or may be influenced by TXA use. Our results indicate that complications requiring reoperation have the greatest impact on total costs. Since the non-TXA group had significantly more reoperations, this resulted in substantially higher postoperative costs and, consequently, higher total costs compared with the TXA group. The most common reason for reoperation after breast reduction surgery was postoperative hematoma. The cost of preventing a single hematoma was calculated by multiplying the NNT of 19 by the cost of TXA solution ((€1.60 + €0.42) = €38.40 = €2.02), resulting in a cost of €38.40. 9 This cost is substantially lower than the cost of reoperating to evacuate a single hematoma, which amounts to €1782. We hypothesized that TXA reduces the risk of postoperative hematoma 3 and, as a result, decreases both reoperation rates and total costs.
There were differences between the study groups in the use of drains, thromboprophylaxis, ward stay following primary surgery, and skin incisions, which may be linked to changes in preoperative practices at Jorvi Hospital during the study period. Topical TXA was introduced to Jorvi’s hospital protocol in October 2020. Most of the non-TXA patients were operated on before that time, apart from a few exceptions. Reflecting the surgeon practices at that time, there was significantly more drain use in the non-TXA group. Interestingly, going back to the basic data, among patients who had drains, the cause of the extra wound care nurse visits was not drain removal. It is also noteworthy that drains are mostly removed by the primary healthcare nurses, and those visits were not included in our cost calculations. Carpelan and Kauhanen 14 demonstrated in a 2016 study that outpatient reduction mammaplasties produces significantly lower costs in comparison with inpatient procedures, largely due to ward-related costs. After that, surgical practice gradually shifted toward more outpatient-type surgery in the later years. In this regard, we excluded postoperative ward costs after primary surgery, as most of these stays were prearranged as inpatient care due to social factors or preoperative medical conditions. We included only ward stays due to complications, reoperations, or other conditions that required additional ward days. Another related finding was that surgeons more readily prescribed thromboprophylaxis to inpatients following major surgery, largely due to bed rest on the ward or a tendency toward thrombosis. Of the 12 hematomas observed, only one occurred in a patient who received thromboprophylaxis, and this case was in the non-TXA group. Thus, the difference in hematoma rates between the study groups could not be explained by differences in thromboprophylaxis use. Although skin incision styles varied between the groups, with more vertical scar incisions in the non-TXA group, this is unlikely to affect complication rates or costs, since previous studies have not found incision type to influence major complications. 15 In our previous study on reduction mammaplasty, no clear association was found between the use of drains, thromboprophylaxis, or skin incisions and the risk of hematoma formation. 3
Postoperative follow-up visits varied in practice according to the surgeon’s preference. When the number of follow-up visits exceeded two, this was assumed to be associated with postoperative healing problems. Although the non-TXA group had a higher number of follow-up visits, this did not substantially contribute to the mean difference in postoperative costs between the non-TXA and TXA groups, with the largest cost differences resulting from the need for reoperations.
Limitations of the study
This study did not assess QALYs or productivity losses, which are typically included in cost-effectiveness analyses. Patients in the non-TXA and topical TXA groups underwent surgery at different times during the study period, and follow-up visits were not standardized. Due to the retrospective design, the potential impact of changes in individual surgeon preferences and prevailing hospital practices during 2019–2021 could not be excluded. For less frequent secondary outcomes, such as reoperations due to infection, seroma, or thromboembolic events, the study was underpowered to detect clinically meaningful differences.
Conclusion
Complications leading to reoperation, particularly postoperative hematomas, had the greatest impact on healthcare costs in reduction mammaplasty. These complications were markedly less frequent in patients receiving perioperative topical TXA, suggesting that routine use of TXA is a simple, safe, and cost-effective intervention. Implementing topical TXA as part of standard care for reduction mammaplasty patients appears to be a recommended approach.
Footnotes
Acknowledgements
The authors would like to thank Mr. Timo Pessi for his assistance with the statistical analysis.
Author contributions
Krisztina Sipos is the corresponding author and was responsible for manual data collection from patient records and for writing the initial draft of the article. Susanna Kauhanen, Mervi Rautalin, and Kaisu Ojala supervised the work, provided advice, and reviewed the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by a research grant from Finska Läkaresällskapet and by grants from Helsinki University Hospital, Division of Musculoskeletal and Plastic Surgery Research Department (TuPla), and the Finnish Medical Foundation.
Ethical approval
This retrospective study did not require Ethics Committee or Institutional Review Board (IRB) approval and was approved through an institutional administrative decision by HUS (HUS/683/2025-13).