
Abstract
Injury to the kidney is relatively common in significant abdominal trauma with the majority of injuries being secondary to a blunt rather than penetrating mechanism. Iatrogenic injury is an important additional cause of renal vascular damage. Multidetector computed tomography (CT) is the reference imaging modality in patients with suspected blunt, penetrating or iatrogenic injury. It allows rapid acquisition of images that accurately identify and stage injury to the kidneys and other major organs. This review addresses clinical indications for imaging, injury classification and the subsequent management of renal trauma, focusing on the important role of the interventional radiology team, particularly in stopping life-threatening haemorrhage by transcatheter embolisation techniques.
Introduction
Renal injury is relatively common in significant abdominal trauma occurring in up to 10% of cases. The majority of renal injuries are the result of blunt as opposed to penetrating trauma with associated injuries to other organ systems being common. Iatrogenic trauma to kidneys is an additional important group of renal vascular injury to be considered. Multidetector computed tomography (CT) is the imaging modality of choice for grading renal injury whilst allowing pre-existing conditions and associated injuries to be identified. Grading of the injured kidney is most usually done with the American Association for the Surgery of Trauma (AAST) renal injury severity scale. This traditionally provides a framework for guiding management but does not include several important direct and indirect signs of renal injury which if present are readily detected by CT. These findings include perirenal haematoma size and active extravasation of contrast. The majority of injuries are classified as minor injuries. These and increasingly intermediate-grade injuries can be safely managed without intervention or surgery. The challenge to the trauma team is to accurately and rapidly identify those patients with major grade renal injury who require timely treatment by surgery or increasingly interventional radiology (IR). Haemorrhage remains a leading cause of early death in trauma patients and the IR team can offer definitive control of renal vascular bleeding in many cases. The concept of stopping traumatic renal haemorrhage by transcatheter embolisation is not new with small case series using autologous blood clot dating back to the 1970s. Since then there has been a general trend in trauma care towards less invasive management. This, accompanied by significant advances in IR techniques and technology and supported by a growing body of evidence has resulted in a shift away from open surgical management of patients with high-grade renal injury towards transcatheter embolisation even in the face of haemodynamic instability.
Incidence and mechanism of injury
Renal trauma occurs in between 1% and 3% of all trauma cases (Santucci et al., 2004). In significant blunt and penetrating abdominal trauma, the kidney is damaged relatively often, despite some degree of local anatomical protection. It is the most commonly damaged retroperitoneal organ being injured in up to 10% of cases of significant abdominal injury (McAninch and Santucci, 2002). The vast majority of cases (approximately 90%) result from blunt trauma, commonly road traffic accidents and falls, with penetrating injuries, principally from stab and gunshot wounds, being less common (Santucci et al., 2004). This does not include an important subgroup of renal injury caused as a result of medical interventions including renal biopsy, partial nephrectomy and renal access procedures. Iatrogenic injury is a significant cause of renal vascular injury. Injury to other major organs is common in significant blunt and penetrating renal trauma; however, more than 90% of isolated renal injuries are classified as minor and are self-limiting (Santucci et al., 2004).
Clinical features
Haematuria is an important sign of renal injury, being present in up to 95% of cases (McAninch and Santucci, 2002). However, its presence or degree does not necessarily correlate well with injury severity as was first described by Bright et al. (1978) in 1978. Indeed, haematuria may be absent in cases where renal pedicle or pelviureteric junction damage has been sustained. Macroscopic haematuria may be absent, or indeed transient, and performing urine analysis to assess for microscopic haematuria is essential. Accurate identification of the mechanism of injury, evaluation for the presence of associated injuries and dynamic assessment of the haemodynamic status of the patient with significant renal injury is mandatory.
Imaging
Indications
Specific indications for imaging in renal trauma
Modalities
Multidetector CT examination is the reference standard imaging modality in patients with suspected renal trauma or indeed any significant blunt abdominal trauma (Santucci et al., 2004). Modern scanners, which should ideally be located in close proximity to the trauma resuscitation room, can acquire whole body images in a matter of seconds. This allows minimal interruption to the ongoing resuscitation efforts of the trauma team and underpins a shift away from the concept of the trauma patient being too unstable to undergo CT examination. A recent large multicentre study of 4621 blunt trauma patients demonstrated that the integration of whole body CT into early trauma care significantly increased the probability of survival (Huber-Wagner et al., 2009). The acquired images allow accurate identification and staging of kidney injury, information regarding pre-existing renal disease, assessment of the contralateral kidney and identification of injuries to other organs. This information coupled with the clinical status of the patient allows for timely decision making as to the need for interventional or surgical management.
The examination should be tailored to the injured patient and as such it is not possible to prescribe a universal protocol that suits all cases or institutions. Most scans will be performed as part of an assessment for abdominal trauma, which in the stable patient usually involves acquisition of images in the portal venous phase post-administration of intravenous contrast. This will image the kidneys in the late cortical or early nephrogenic phase, allowing identification of parenchymal injury. In the haemodynamically unstable patient, imaging in the arterial phase is recommended allowing active bleeding to be identified. If there is suspicion of an injury to the collecting system on the initial images (and the patients clinical condition will allow it), a delayed excretory-phase scan can be performed to assess for urinary contrast extravasation.
Other imaging modalities have a very limited role in the initial assessment of the acutely injured kidney. The use of intravenous urography in this setting is largely historical. Ultrasound may be utilised by a member of the trauma team in the resuscitation room as a part, the controversial triage tool Focused Asssessment by Sonography in Trauma which does not involve dedicated assessment of the kidneys. Ultrasound is certainly less sensitive at identifying free retroperitoneal fluid and solid organ injury than CT. Catheter angiography is occasionally used as a first-line diagnostic tool, but is more usually performed as part of a transcatheter embolisation procedure following CT.
Injury classification
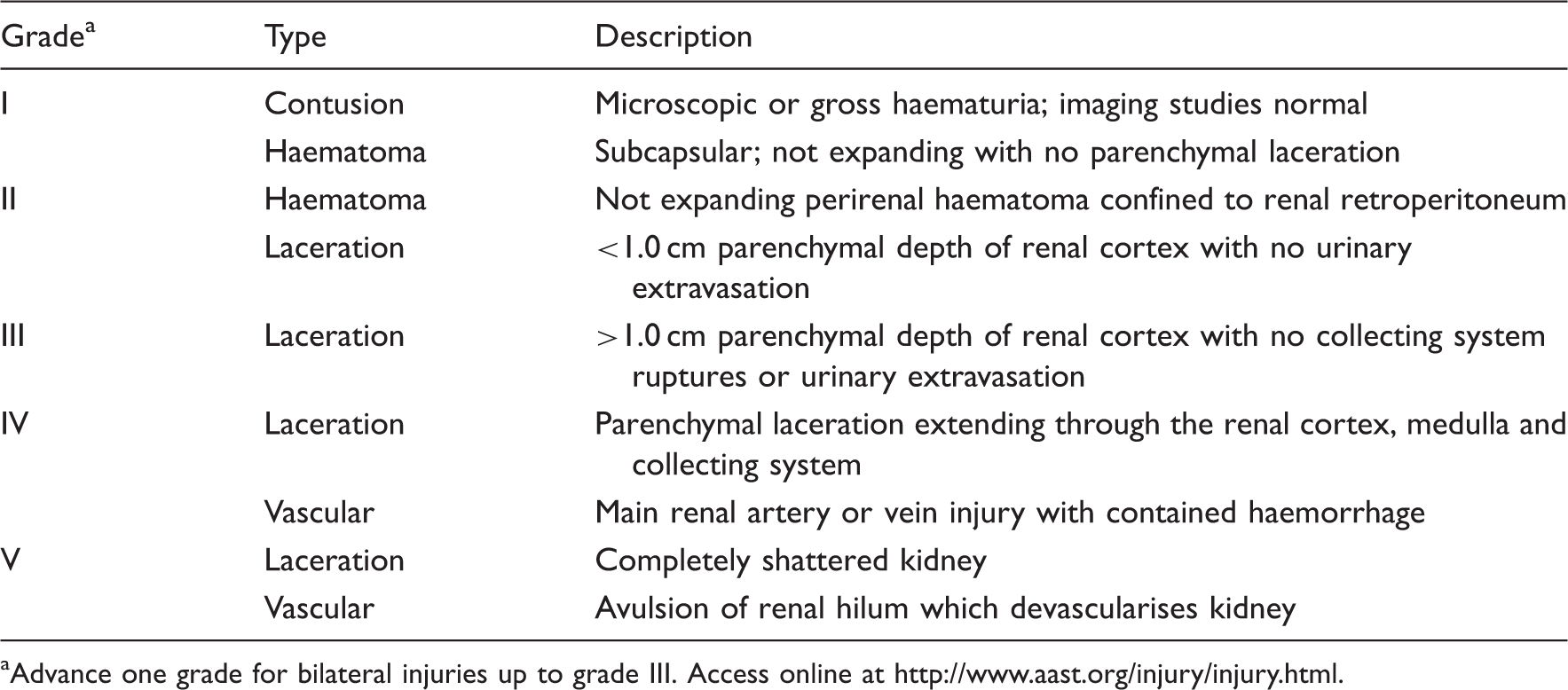
Over two decades ago, the AAST organ injury scale for renal trauma was published (Moore et al., 1989). This scheme is an anatomic description of kidney damage which is scaled from one (least severe) to five (most severe). It is outlined in Table 2 and some examples are illustrated in Figure 1. The scale allows the classification of renal injury into categories upon which decisions regarding patient management can be based. Studies have validated its clinical use (Santucci et al., 2001; Kuan et al., 2006; Tasian et al., 2010); however, in the 20 years or so since their publication, the management of renal trauma has significantly changed. As in the management of blunt trauma to other solid organs, there has been a shift towards non-operative management (Santucci and Fischer, 2005). This has in part been driven by significant advances in the quality and acquisition time of CT images, coupled with a surge in transcatheter embolisation techniques and technology. The key features of the AAST organ injury score, principally parenchymal laceration depth and major vessel injury, are readily identified by multidetector CT. However, modern scanners are capable of demonstrating several features of renal injury which are not included in the AAST score. These include active contrast extravasation, perirenal haematoma size and laceration size, and complexity. These findings are important risk factors significant for renal vascular injury associated with the need for urgent intervention to arrest bleeding, increasingly by transcatheter embolisation (Nuss et al., 2009). Other findings indicative of renal vascular injury that may be identified on arterial phase CT imaging include the presence of pseudoaneurysm (PSA) or arteriovenous fistula (AVF). This has led to the proposal to substratify AAST grade 4 injuries into 4a and 4b based on the absence or presence of additional risk factors such as active contrast extravasation, with the former likely to be managed non-operatively and the latter with embolisation or open surgery (Dugi et al., 2010). A further CT finding reported to be associated with the need for transcatheter embolisation is that of discontinuity of Gerota's fascia (Fu et al., 2010).
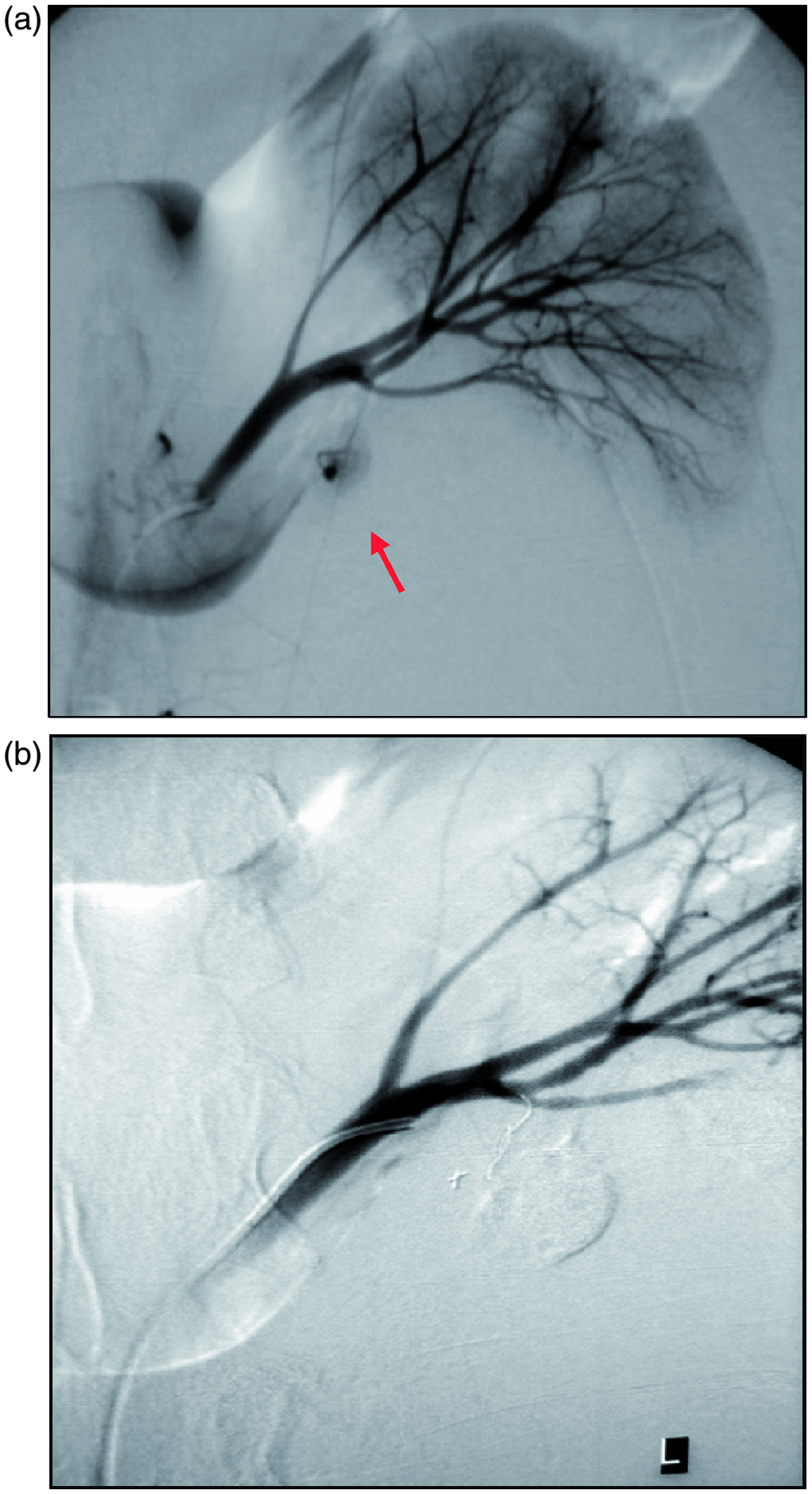
(a) A 3D reformatted image from a CT examination of a patient who fell from a height onto his left side. The left kidney is displaced medially by perirenal haematoma. There is extravasation of contrast indicative of active bleeding (arrow). Note the associated fractures of the left 11th and 12th ribs (arrowheads). (b) An axial slice from the CT examination demonstrates significant left perirenal haematoma displacing the left kidney. There is extravasation of contrast indicative of active bleeding (arrow). (c) Selective left renal artery angiogram demonstrates active bleeding from lower pole arterial branch (arrow). (d) Super selective coil embolisation (arrow) and identification of a further area of active bleeding (arrow head) which was also successfully treated by embolisation with coils. The AAST renal injury severity scale aAdvance one grade for bilateral injuries up to grade III. Access online at http://www.aast.org/injury/injury.html.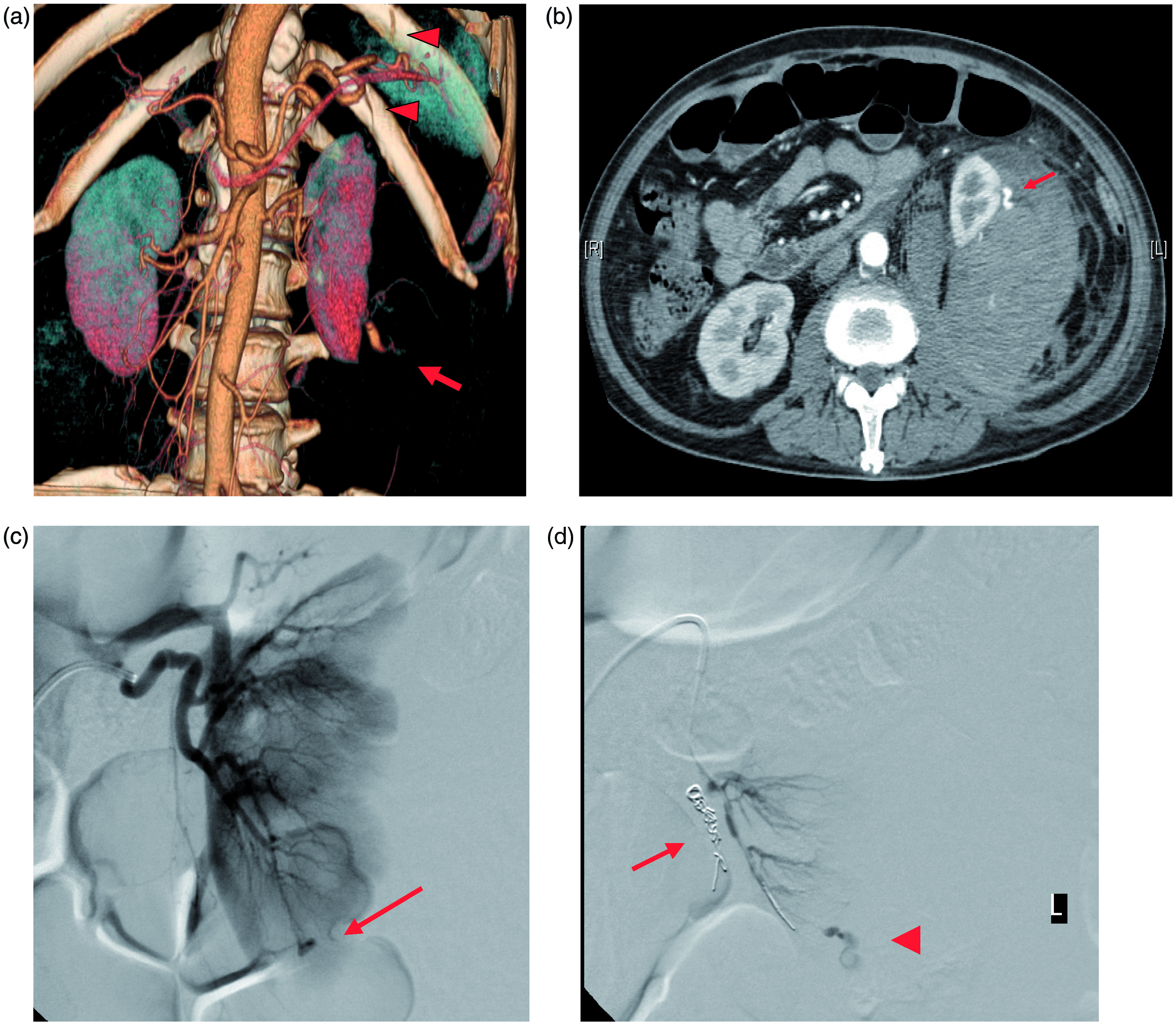
Management
The vast majority of renal injuries are minor and self-limiting (Santucci et al., 2004). Intermediate-grade injuries are increasingly managed expectantly without IR or surgical intervention. Traditionally, high-grade injuries were treated by open surgery with renal salvage/reconstructive surgery or nephrectomy. In some cases, the decision to proceed to urgent laparotomy may be due to the recognition of coexisting severe injuries to other major organs needing surgical intervention or dictated by limited local access to IR services. The move away from surgical management of isolated high-grade renal injuries has not just been the pull resulting from improved imaging with multidetector CT, better critical care services and advances in IR, but also the poor outcomes following open surgical management. A large proportion of patients undergoing exploratory laparotomy for renal trauma underwent nephrectomy (Wessels et al., 2003), and high morbidity and mortality rates have been reported (Edwards et al., 2009). Nephrectomy in the setting of trauma has also been shown to be associated with a higher incidence of renal failure than other therapeutic modalities (Starnes et al., 2010). Avoidance of iatrogenic nephrectomy is the obvious benefit of non-surgical management of isolated renal injury.
Transcatheter embolisation has been shown to be a safe and effective therapy to control active renal vascular bleeding secondary to blunt and in selected cases penetrating trauma (Dinkel et al., 2002; Bent et al., 2008; Breyer et al., 2008). This is also the experience at our institution where a series of patients have undergone successful embolisation of acute renal haemorrhage following both blunt and penetrating trauma (Figure 1(a)–(d)). More recently, Brewer et al. (2009) reported the safe and effective urgent embolisation of grade 5 renal trauma in haemodynamically unstable patients. Furthermore, intermediate-term follow-up showed no significant adverse events, with no reported complications of refractory hypertension, altered renal function, new urolithiasis, chronic pain, urine leak, AVF or PSA (Stewart et al., 2010). Several studies have evaluated the effects on renal function and morphology of transcatheter embolisation in the setting of trauma, demonstrating preservation of renal function and parenchyma (Chatzioannou et al., 2004), preservation of glomerular filtration rates evaluated by dynamic scintigraphy (Morita et al., 2010) and late functional and morphological improvements in embolised renal units (Mohsen et al., 2007).
The principle role of the IR team in the management of both blunt and penetrating renal traumas is to stop life-threatening haemorrhage. This concept is not new. Renal artery embolisation was first described in 1964 (Edling and Ovenfors, 1964) and small published series of cases using autologous blood clot to successfully arrest traumatic renal haemorrhage date back more than three decades. (Chuang et al., 1975). Since then there have been significant advances in IR equipment, technology and techniques. There is now a wide range of embolic material available in the armamentarium of the IR and the advent of coaxial microcatheter systems allows superselective catheterisation of segmental arteries allowing accurate delivery of embolics. This results in effective arrest of bleeding from renal artery branches whilst preserving nephrons. The challenge to the trauma team is to accurately and rapidly identify those patients whose renal injury would benefit from transcatheter techniques and to ensure timely referral to the IR team.
The IR team should forge strong links with the trauma team and ideally provide a 24-h-a-day service with a rapid response time. At our institution, eight IRs, all offering embolisation for acute bleeding, with the support of dedicated IR radiographers and nurses provide a comprehensive service with a 30-min response time. The IR theatre should ideally be located in close proximity to the CT Scanner and trauma resuscitation room minimising delay. Timely referral is essential to ensure optimal outcome. Delay in time to achieve embolisation has been shown to be an important factor in patient survival in a series of patients undergoing arterial embolisation to control pelvic fracture haemorrhage with development of coagulopathy being cited as an important reason for poor outcome (Agolini et al., 1997). More recently, Howell et al. (2010) reported that in haemodynamically unstable trauma patients undergoing therapeutic catheter-based IR procedures, delay to IR beyond 60 min was independently associated with a twofold increase risk of mortality. Furthermore, for every hour delay, the risk of mortality increased by nearly 50%. Once in the IR theatre, access is obtained to the arterial system usually via the Common Femoral Artery at the groin. CT angiography often negates the need for flush aortic angiography as the source of bleeding has already been identified providing a ‘roadmap’ for the IR to proceed directly to selective catheterisation of the bleeding vessel. Angiography may demonstrate active extravasation of contrast indicative of unrestrained active bleeding, presence of a PSA or AVF. Renal arteries are end arteries and therefore there is no need to consider collateral supply as in other vascular territories such as the gastro- duodenal-pancreatic arcade. Superselective catheterisation minimises ischaemic damage secondary to embolisation. Embolisation is most frequently with coils, however, we have used Gelfoam (spongiostan) or liquid embolics such as glue (N-butyl cyanoacrylate) in selected cases, for example, where the patient has developed a coagulopathy.
An inevitable consequence of the shift away from the management of renal trauma by nephrectomy is the need to be recognised and manage complications related to the injured kidney. The need to perform follow-up imaging in patients with renal trauma is controversial, but it is probably unnecessary for blunt renal injuries of grades I to III (Malcolm et al., 2008). However, complications after renal trauma are reported to occur in between 3% and 33% of cases (Al-Qudah and Santucci, 2006) and can be immediate, early or late. Immediate complications most commonly relate to renal vascular injury as discussed above. Early complications are usually defined as occurring within 4 weeks of trauma and include urinary extravasation and urinoma formation, perinephric collections and secondary haemorrhage often due to PSA or AVF. Extravasation of urine is the most common complication of renal trauma (Matthews et al., 1997). Delayed phase excretory CT imaging may demonstrate active leak of urine from a disrupted collecting system. The majority of these patients can be treated expectantly with only a small proportion requiring intervention. The IR can provide urinary diversion in these cases by performing nephrostomy tube insertion and in selected cases, antegrade ureteric stenting and/or image-guided percutaneous drainage of urinomas. Delayed haemorrhage is a serious complication of renal trauma and most often due to PSA or AVF. When clinically suspected, these are readily identified by CT imaging and can be effectively treated by selective transcatheter embolisation most often with coils or N-butyl cyanoacrylate glue (Miller et al., 2002; Cantasdemir et al., 2003; Yazdi and Moharramzadeh, 2008). Both PSA and AVF can present months or years following injury (Chazen and Miller, 1997). Late complications include hypertension, hydronephrosis and calculus formation. ‘Page kidney’ is a term applied to hypertension secondary to renal compression which in the setting of trauma may be due to perirenal haematoma or urinoma or scarring of the renal capsule. This phenomenon was first described by Page (1939) in 1939 and the first clinical case reported in 1955 by Engel and Page (1955) in a young patient with hypertension cured by removal of a calcified subcapsular haematoma.
Other considerations
Iatrogenic injury
Iatrogenic injury is an important cause of kidney trauma, being the most common cause of significant renal vascular injury (Mohsen et al., 2007; Mavili et al., 2009). This is supported by an analysis of all renal artery embolisations performed at our institution over the past decade. In this series, renal vascular injury requiring percutaneous transcatheter embolisation in the acute setting was three times more common secondary to iatrogenic than a combination of both blunt and penetrating traumas. Renal biopsy was the most common cause of injury (Figure 2(a)–(c)), with partial nephrectomy and renal access procedures being other causes. Figure 3 (a) and (b) demonstrates successful selective embolisation in a patient who became haemodynamically unstable in the immediate post-operative period following partial nephrectomy. Catheter or CT angiography demonstrated active contrast extravasation, PSA, AVF or a combination of these, with PSA being the most common finding. These lesions are safely and effectively treated with transcatheter embolisation with superselective embolisation ensuring minimal damage to the kidney.
(a) An axial slice from an arterial phase CT examination of a patient with a left Illiac fossa kidney transplant who companied of left-sided abdominal pain following a percutaneous biopsy procedure. It demonstrates a PSA in the anterior part of the transplant kidney (arrow). (b) Selective transplant renal artery angiography confirms the presence of a large PSA (arrow). (c) The right-hand image demonstrates successful selective embolisation. Images courtesy of Dr I McCafferty. (a) Selective left renal artery angiogram in a patient with significant hypotension immediately following partial nephrectomy demonstrating active extravasation of contrast from a descending ureteric arterial branch (arrow). (b) Successful superselective coil embolisation of the bleeding artery with excellent preservation of the remaining kidney.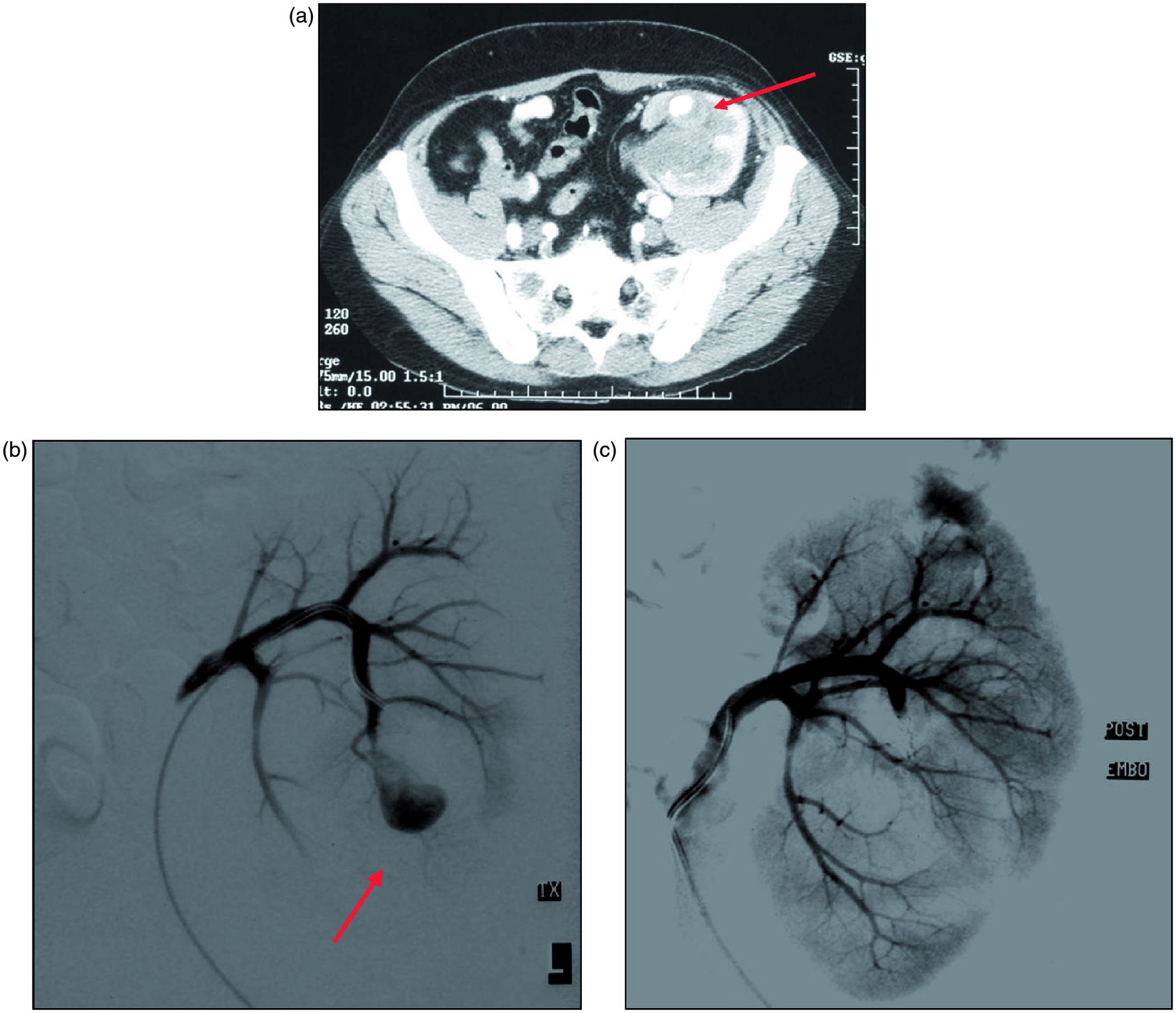
Injury in kidneys with pre-existing abnormalities
Pre-existing renal lesions (PERLs) seem to increase the vulnerability of kidneys in renal trauma (Santucci et al., 2004). They are found in a larger proportion of children suffering renal injury than adults, with one series reporting the existence of PERLs in 36% of children with blunt renal trauma (Onen et al., 2002). Renal lesions predisposing to injuries include hydronephrosis, for example, secondary to pelviureteric junction obstruction or stone, renal cysts, tumours and developmental renal anomalies such as longitudinal renal ectopia (e.g. pelvic kidney) or renal fusion (e.g. horseshoe kidney). These are often undiagnosed at the time of the injury. CT is the optimal examination to evaluate trauma to abnormal kidneys (Rhyner et al., 1984).
Transplant kidneys
Renal transplants are most commonly sited within the pelvis and therefore, like ectopic pelvic kidneys, are potentially more vulnerable to trauma. Iatrogenic injury, frequently secondary to percutaneous biopsy (Figure 2(a)–(c)), is an important cause of transplant renal vascular damage. Early recognition of these injuries, ideally with CT angiography, allows for timely referral for percutaneous embolisation or other transcatheter techniques. Figure 4(a)–(d) demonstrates the successful use of a covered stent-graft to exclude a PSA at the arterial anastomosis of a transplant kidney and serve to illustrate another tool in the armamentarium of the IR.
(a) An axial image from an arterial phase CT examination of a patient who developed left-sided abdominal pain a month following left renal transplantation. It demonstrates a large left-sided perirenal haematoma (arrows) and abnormality at the arterial anastomosis (arrow head). Note the renal transplant in the right iliac fossa which had failed secondary to rejection. (b) Catheter angiography demonstrates a PSA in the region of the transplant artery anastomosis. (c) The PSA has been successfully excluded by the placement of a covered stent graft. (d) A 3D reconstructed image from follow-up arterial phase CT examination at 1 month demonstrates successful exclusion of the PSA with patency of the transplant renal artery. Images courtesy of Dr P Riley.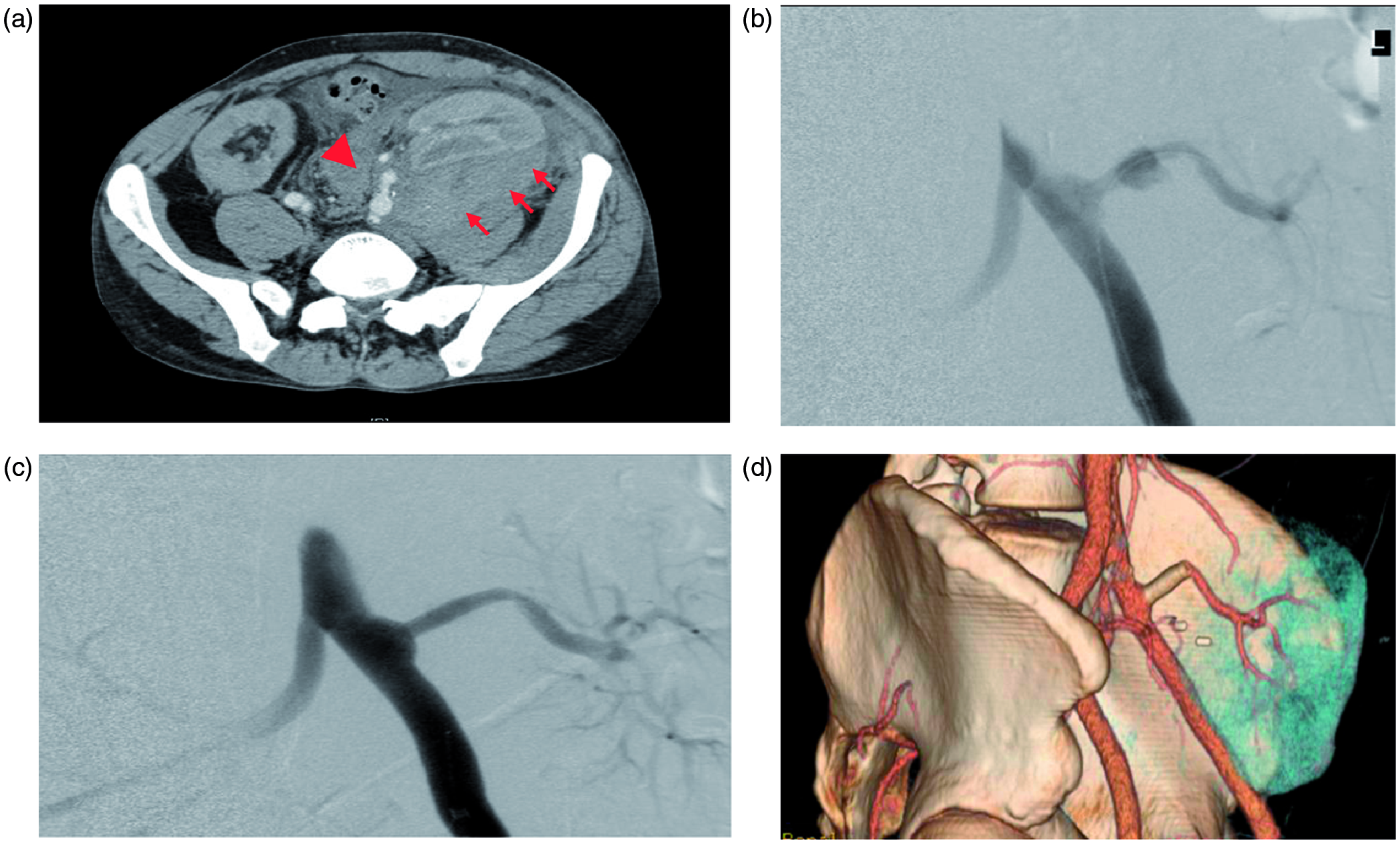
Conclusion
Haemorrhage remains a leading cause of early death in trauma patients. As with injury to other solid organs, transcatheter techniques can provide definitive control of acute renal bleeding. To optimise the outcome, this requires rapid identification and staging of renal injury and timely referral to IR. This, in turn, is dependent on the rapid acquisition of CT imaging during trauma resuscitation and close working relationships between the trauma and IR teams.