
Abstract
A hernia through an intercostal space involving the bowel is rare but can result in strangulation of the bowel if not diagnosed promptly. We report a case of bowel herniation through the left 9th intercostal space after blunt trauma in a motor vehicle collision. A mass was present overlying the left lower anterolateral chest wall thought to be a haematoma, but it was eventually diagnosed as an intercostal hernia after CT imaging. The treatment for this injury included diagnostic laparoscopy to rule out other abdominal injuries and local repair of the defect. This report discusses the current literature regarding diagnosis and treatment of this rare phenomenon.
Introduction
Abdominal wall hernia of any sort is rare following blunt trauma (El-Charnoubi et al., 2010) and variants such as handlebar hernia (sustained when a patient strikes their abdomen against the handlebar of a motorcycle or bicycle) are even more so (Holmes et al., 2002). Intercostal herniation of abdominal viscera is rarely reported (Bobbio et al., 2008) and is usually associated with blunt force trauma causing diaphragmatic rupture followed by transpleural and intercostal herniation. We report a rare variant of the traumatic abdominal wall hernia where the abdominal viscera have herniated directly through the 9th intercostal space without preceding diaphragmatic rupture. This injury may be diagnosed on history and examination alone but is often overlooked until CT imaging (Unlu et al., 2007). Treatment often includes laparoscopy to exclude other abdominal injuries and to help delineate the extent of the hernia.
Case report
A 28-year-old man presented to our emergency department (ED) following a motor bike accident at 60 km/h. The patient suffered no loss of consciousness and walked away unassisted from the accident. His main complaint on presentation to the hospital was pain on the left side of the chest. On examination, bruising and a 10 cm mass on the left anterolateral lower chest wall thought to be a haematoma were evident. CT scan of the chest and abdomen revealed herniation of the left colon between the 9th and 10th ribs with an associated fracture of the 10th rib (Figure 1). There was also a fracture of the left L1 vertebral transverse process.
Axial CT image with the left intercostal hernia clearly visible.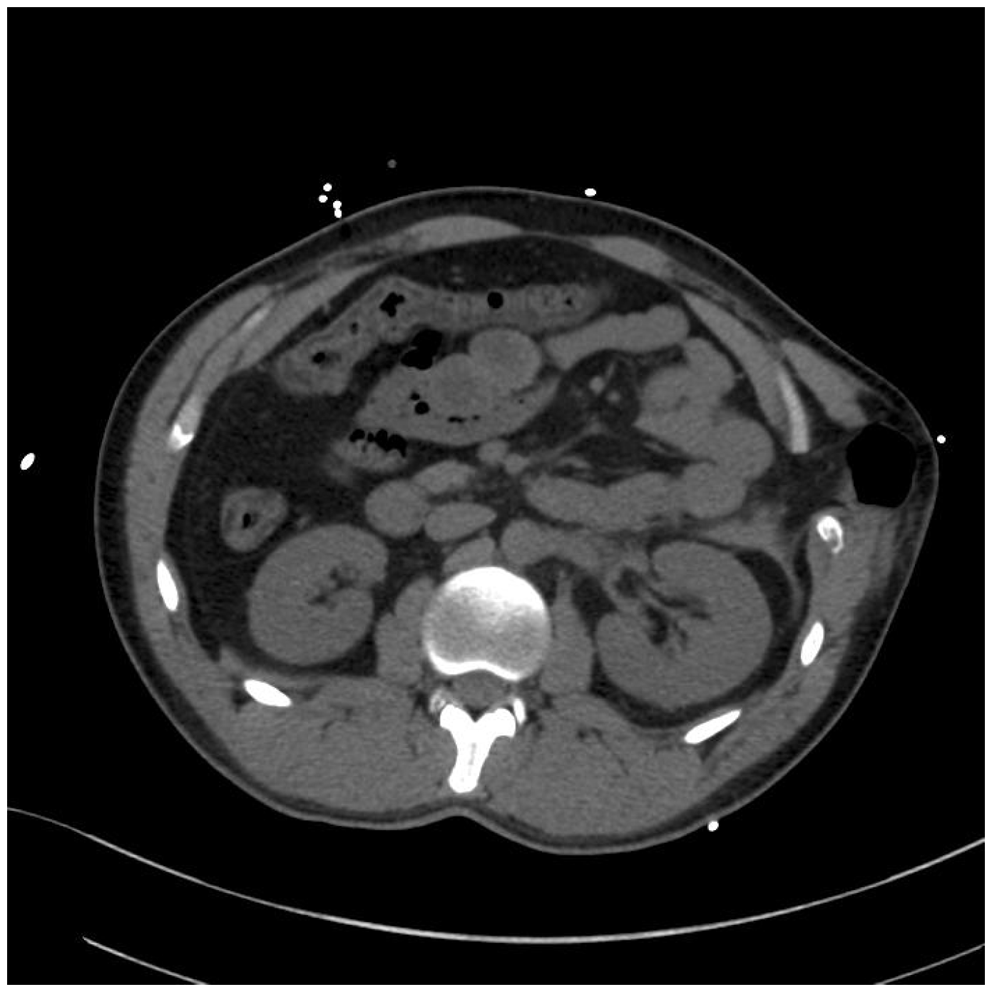
The hernia was irreducible and concern about possible associated intra-abdominal visceral injury prompted the decision for urgent surgery. The hernia reduced spontaneously on administration of muscle relaxant for general anaesthesia. The patient was positioned in the semi-right lateral position and diagnostic laparoscopy identified a haematoma in the colonic mesentery and a 1-cm colonic serosal tear at the splenic flexure which was oversewn with 3/0 monocryl. In the left upper quadrant, there was a cone-shaped defect of size 7–8 cm in the lateral thoracoabdominal wall (Figure 2).
Thoracoabdominal wall defect at laparoscopy.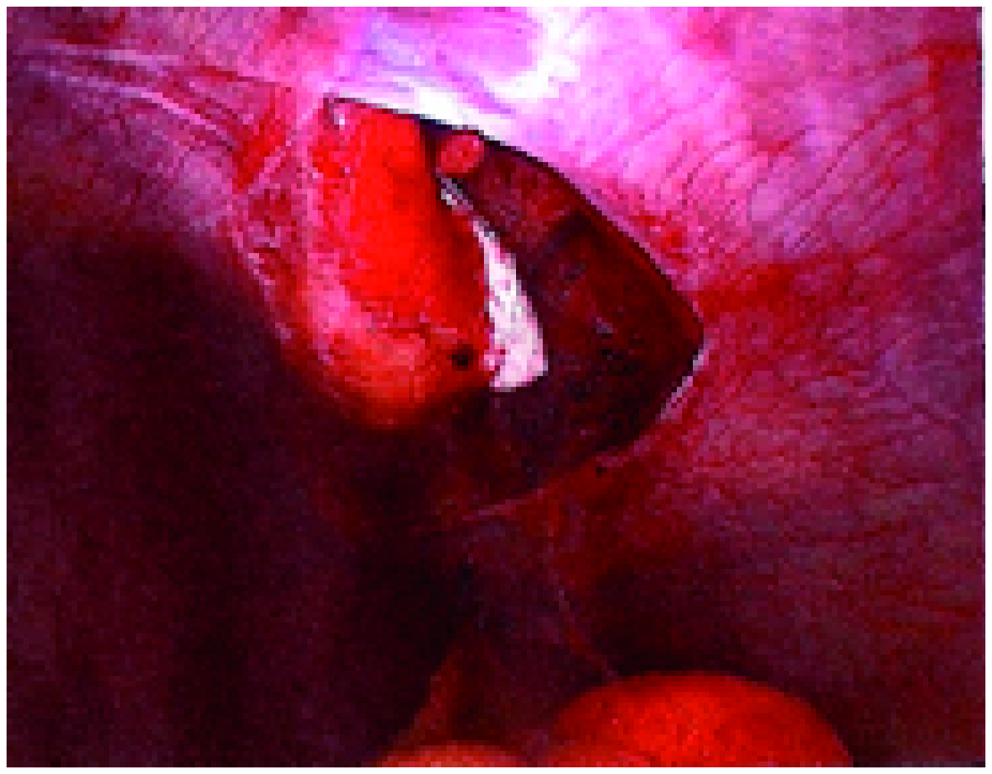
Laparoscopic repair was not attempted due to the degree of tissue loss from the thoracoabdominal wall. An incision was made over the site of injury in line with the rib and the fractured tip of the tenth rib was debrided with some of the surrounding damaged muscle. The remainder of the 10th rib was secured to the 9th by encircling 0-gauge loop non-absorbable monofilament polybutester sutures. The injured muscles were closed in layers. There was evidence of significant shearing injury to the subcutaneous fat, and the skin was closed with clips. Post-operatively, pain control was achieved by a paravertebral block. The patient recovered slowly without incident and was discharged on the eleventh day after injury.
Discussion
Abdominal intercostal hernia (AIH) is uncommon. There are several reports of intercostal hernias involving the lungs but few that describe a hernia that contains abdominal contents (Balkan et al., 2001). Bobbio et al. (2008) described a hernia that protrudes through the intercostal space involving a diaphragmatic defect as a transdiaphragmatic intercostal hernia, which differs from an AIH, when abdominal viscera gain entry to the intercostal space without an associated diaphragmatic defect – this best describes the injury in this case.
There are a number of potential mechanisms that can cause a hernia to develop through the intercostal space. Kurer and Bradford (2006) hypothesized that a hernia through the intercostal space involving abdominal contents was caused by penetrating or blunt thoraco-abdominal injuries which involve rib fractures. Ganci and Orgill (1996) went further and described a variant called the ‘autopenetrating hernia’ characterized by a small abdominal wall defect secondary to a focal blunt injury. They suggested that the mechanism involved the driving of a jagged edge of a fractured rib or costal margin through the deeper tissues creating a local tissue defect. In our case, the motorcycle handlebar appears to be the source of the focal blunt injury and the disruption of the muscular and fascial layers from the blunt injury is in line with the generation of the local tissue defect.
Dimyan et al. (1980) originally proposed the term ‘handlebar hernia’ to describe any abdominal hernia occurring when a person hits the handlebar of a motorcycle or bicycle with force. The force of a handlebar often does not penetrate the soft tissues but causes disruption of the muscular and fascial layers (Holmes et al., 2002). Not all intercostal herniae are caused by blunt-force trauma and cases resulting from chronic cough (Khan et al., 2006) from predisposing conditions such as chronic obstructive pulmonary disease (Sharma and Duffy, 2001) are reported. Our patient had no such predisposing features.
The ED clinical history and examination did not diagnose the hernia, almost certainly due to the low level of clinical suspicion because of AIH’s low incidence. Francis and Barnsley (1979) suggested that the presence of a reducible soft tissue swelling in the thoracic wall following trauma should be enough to suspect a hernia and that if the hernia size increased with inspiration and decreased with expiration, then abdominal contents should be suspected rather then lung within the hernia. As in this case, clinical findings and chest radiography are not always diagnostic. Biswas and Keddington (2008) reported a patient who presented to a minor surgery clinic for excision of a chest wall lipoma 1 year after a motor vehicle collision. Examination at that stage revealed a reducible defect apparently containing bowel and the diagnosis was again confirmed by CT. It is invaluable in both early diagnosis in trauma and pre-operative planning (Chen et al., 2005).
Traumatic AIH is usually found inferior to the seventh rib on the left side, as the liver presumably prevents visceral herniation on the right. Fractures of the 8th–12th ribs should raise concerns of associated abdominal visceral injury and a CT scan is important to aid in assessing splenic, renal and diaphragmatic injuries (Kurer and Bradford, 2006).
In high-impact/diffuse injuries, the rate of associated intra-abdominal injury approaches 60% and exploratory laparotomy or laparoscopy is essential (Tiong et al., 2007) and militates to transabdominal repair of the defect. Focal injuries are associated with fewer intra-abdominal injuries and a clinical decision can be made as to whether exploration is required. A surgical approach for treatment was necessary in this patient as the inclusion of bowel within the hernial sac placed him at risk of a significant bowel injury and need for resection.
Conclusions
Traumatic AIHs whilst rare can have serious consequences and should be treated immediately. Diagnosis is not often made until after CT scanning and it is recommended that a low threshold for imaging is warranted in cases of trauma. Surgical intervention is usually indicated for repair, and should be coupled with laparoscopy or laparotomy to rule out hollow viscus injury in all but the most straightforward injuries.