
Abstract
Computed tomography is the undisputed gold standard in the imaging of acute trauma, despite the introduction of focused assessment with sonography for trauma and magnetic resonance imaging. However, the role of computed tomography is far wider than just polytrauma imaging: its high spatial resolution, short scan times and very high sensitivity and specificities make computed tomography useful in the diagnosis of subtle injuries, as well as providing a general overview of other compartmental injuries. Three-dimensional reconstructions illustrates complex injury patterns clearly, aiding surgical planning and permitting accurate orthopaedic hardware follow-up. This article outlines some of the basic properties of computed tomography using examples from musculoskeletal trauma, to illustrate to clinicians what computed tomography can and cannot do for their practice.
Why do non-radiologists need to know about computed tomography?
By 2007, one in every seven patients presenting to the Emergency Department (ED) in the United States had a CT scan (Larson et al., 2011b). This number continues to rise exponentially, despite the introduction of other imaging technologies like ultrasound (US), and in particular focused assessment with sonography for trauma (FAST) and magnetic resonance imaging (MRI). An estimated 70 million CT scans are performed annually in the United States, so although a detailed knowledge of CT physics is not necessary for clinicians, an understanding of the basic principles and terminology are useful (Larson et al., 2011b). Clinicians interested in a more detailed review of the technology are advised to consult the following: Flohr et al. (2005) and Alisy-Roberts (2008).
Key principles and terminology used in CT
What is CT?
CT is an extension of plain film radiography (X-rays) and shares the same benefits of rapid image acquisition and superb bony detail. However, plain film radiographs have poor soft tissue resolution and display the three-dimensional (3-D) human body as a two-dimensional (2-D) image. Consequently, further detail is lost by superimposition of overlying structures upon one another. In the late 1960s, British physicist Godfrey Hounsfield came up with the idea of using a rotating X-ray source linked to newly discovered computers. Therefore in CT, the ionising radiation source rotates inside the gantry (‘doughnut’), with an arc of X-ray detectors opposite. The patient passes through the lumen of the gantry on a motorised table, before powerful computers rapidly reconstruct the complex array of X-ray data to create a series of staggered axial (transverse) images (‘slices’) through the patient. This made CT the first fully digital imaging modality, with the benefits of remote viewing and easy storage.
The first clinical scanner was used in London in 1972 and revolutionised medical imaging overnight. For this seminal discovery, Godfrey Hounsfield was awarded the 1979 Nobel Prize for Medicine and a knighthood (Hounsfield, 1979). Crucially for its use in trauma, as an X-ray-based technique, there are no contra-indications to CT, unlike MRI (e.g. any patients with ferrometallic implants or foreign bodies) and US (obesity, excess bowel gas), although care is needed to avoid excessive or unjustified radiation exposure (Brenner and Hall, 2007). Consequently, CT is used safely and widely in adult, paediatric and obstetric patients (Larson et al., 2011a).
As a digital technique, each CT image is made up of thousands of tiny pixels (picture elements). Each pixel (or the 3-D equivalent voxel), which forms the grey CT image, is shaded according to the average attenuation of the X-ray beam as it passes through the different tissues within that voxel (Alisy-Roberts, 2008). These relatively different attenuations are quantified as Hounsfield Units (HU) by the computer. HU range from –1024 (darkest shade, for air), through 0 (for water), to +3071 (lightest shade, for bone/metal), so that 4096 shades of grey are possible per image. Assessing the HU of different tissues, allows radiologists to differentiate similar looking tissues from each other (e.g. fat versus muscle, blood versus free fluid). However, the human eye can only differentiate 50 shades of grey, so CT images must be windowed, limiting the displayed range of HU, in order to show maximum tissue detail (Figure 1; Alisy-Roberts, 2008).
Different windowing (to show different tissues preferentially) and multi-plain reformats (to show different anatomical plains) used for computed tomography (CT) image analysis. (a) Sagittal whole spine CT image (bone windows) showing fracture of C7 spinous process (arrow), multiple thoracic vertebral body fractures (*) and a sternal fracture (arrowhead). (b) Axial image through the lower thorax (lung windows) showing small bilateral pneumothoraces (arrows). (c) Axial image of male pelvis at S1 following a gunshot wound (soft tissue windows). There is a comminuted fracture of left iliac crest with bony and metal fragments (arrow) next to a large pelvic haematoma (*), which is displacing contrast-filled intact iliac vessels. Note the simultaneous assessment of bony and vascular injuries.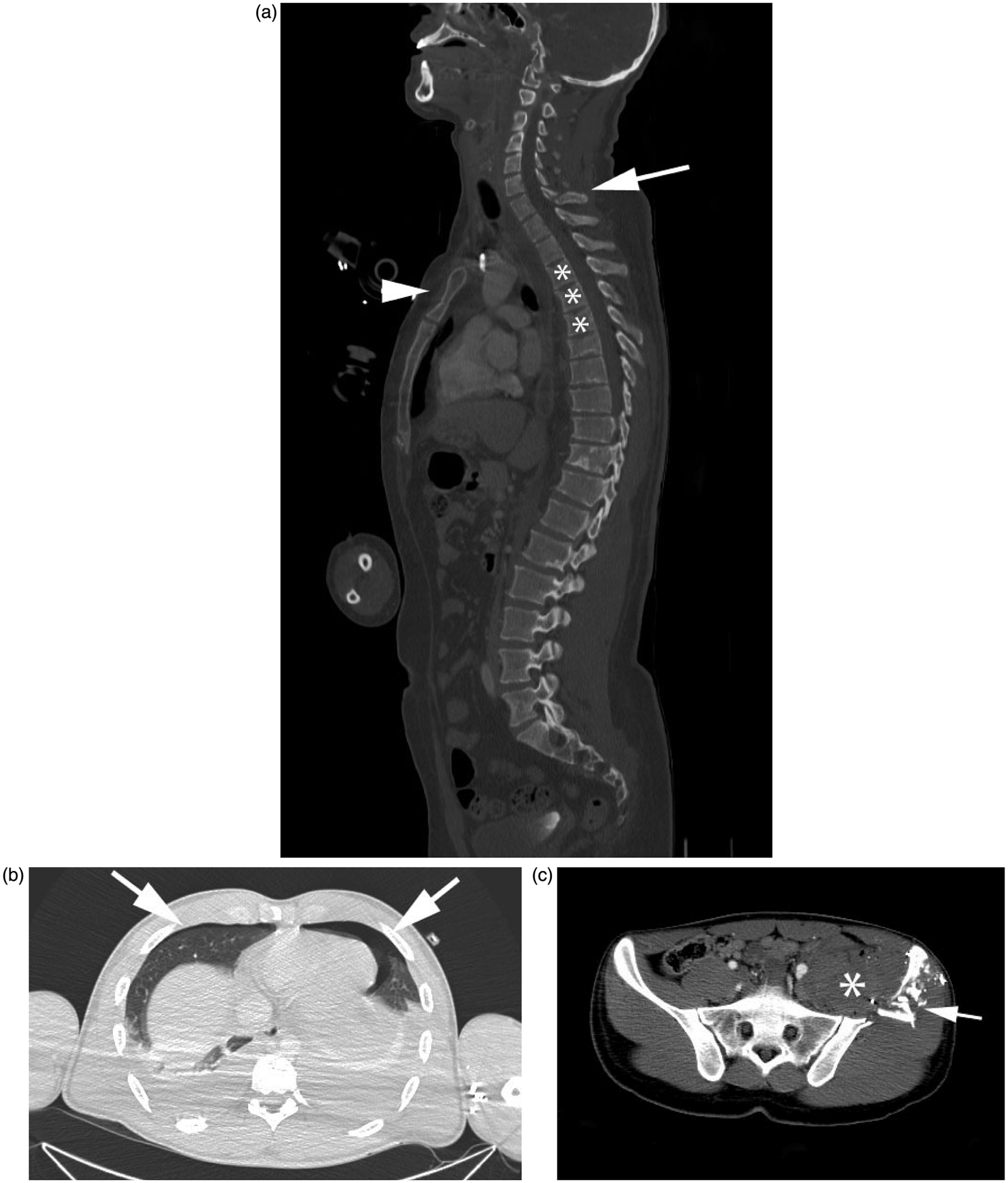
Spiral CT
Further advances in electronics allow modern CT scanners to image patients in a continuous block (so called spiral or helical CT), compared to the initial staggered single sections. This has the benefit that all tissue is imaged, reducing the chance of missing anything significant between non-imaged slices. Unfortunately, this means that there are >1500 slices for the radiologist to review for a whole body CT trauma scan!
Initially, spiral CT caused a large increase in patient radiation dose (as more of the patient was imaged), but the dose continues to be reduced with new CT protocols, so that by 2004 the patient had 17% less radiation dose with a spiral CT than the same study with single slice CT, despite acquiring more information (Ptak et al., 2003). This reduction is thought to be due to reducing overlap between scanned areas.
Multi-detector CT
The depth of X-ray detector rows has also increased rapidly (from 1 up to 328 rows currently), so that much larger blocks of tissue can be imaged during each X-ray source rotation (multi-detector CT, MDCT, which is the current standard). Consequently, scan times have decreased from over 30 min that the first clinical CT scanner in 1972 took to produce an axial slice (brain) scan, to a modern scanner which can image the whole body in a few seconds (Figure 2). This is particularly useful for trauma patients who might be haemodynamically unstable, or unable to lie still (age/pain). This reduces breathing/movement artefact in the images and reduces the need for sedation. In comparison, an MRI brain scan alone takes around 20 min.
A modern 128-slice computed tomography (CT) scanner at our institution. This dedicated Emergency Department (ED) scanner performs a whole body trauma scan (slices at 0.75 mm intervals), with IV contrast to show vascular and visceral injuries, in 105 s. The actual scan time is only a fraction of this time (45 s) but is delayed by the time taken for IV contrast to be circulated around the arterial and venous systems (60 s). Note integrated resuscitation and patient monitoring facilities, as well as the automated IV contrast injector on the left.
Multi-planar reformats
Modern scanners acquire tissue data as isotropic voxels, meaning cubes of data that are equal in all three spatial axes (0.6 mm3). Consequently, extremely high resolution images are formed, which can be viewed simultaneously in axial, coronal and sagittal plains (known as multi-planar reformats – MPRs, Figure 2). Usefully, CT data can be easily reformatted retrospectively in any anatomical orientation (unlike MRI), so that complex comminuted or subtle intra-articular fractures can be assessed in the plain of the joint or fracture, for the benefit of the radiologist and surgeon. Viewing images in different plains has been shown to help diagnosis and triage of complex injuries for immediate surgery, assessing the fracture pattern and the relationship to other key structures such as vessels, nerves and tendons (Magid et al., 1990).
Three-dimensional reconstructions
Modern viewing software allows coloured 3-D volume or surface-rendered images to be produced in real time, which can be rotated and viewed at any angle. These images allow removal of overlying soft tissue (or plaster cast), so that only the areas of interest are shown (Figure 3). This is useful for ‘busy’ anatomical areas such as the acetabula, knees and ankles, where overlying structures can make assessment difficult.
Three-dimensional (3-D) volume-rendered image of the same patient as Figure 2(c), after removal of soft tissues, showing the fracture pattern (arrow) and intact pelvic vessels.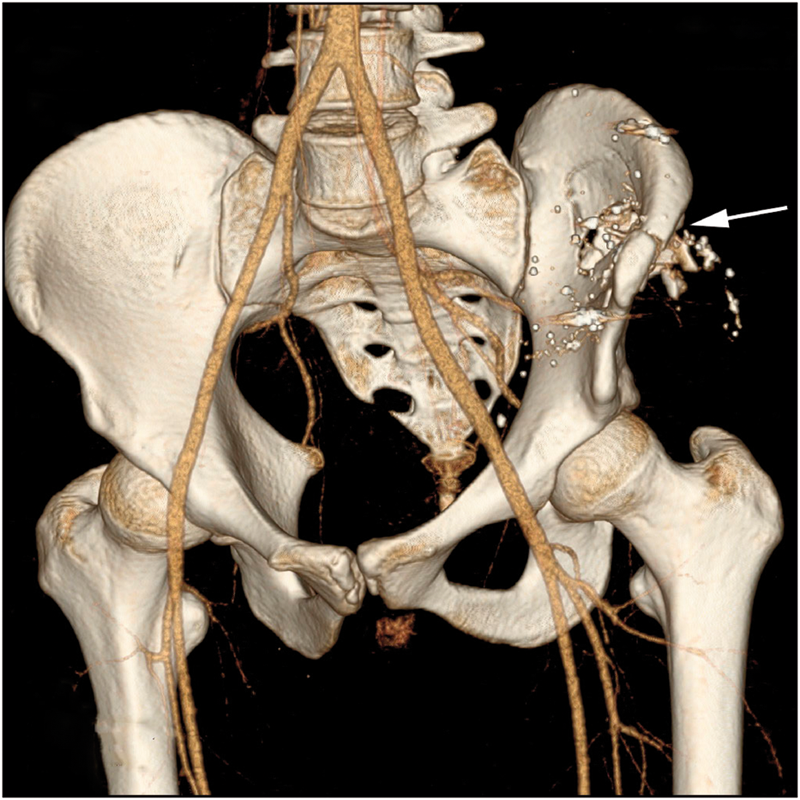
The use of MPRs and 3-D rendering has caused a substantial improvement in injury identification compared with axial CT imaging, altering the timing and treatment of injuries. For example, 30% of acetabular fractures had their management altered after viewing the MPRs, compared with the initial management based on the axial CT findings alone (Scott et al., 1987).
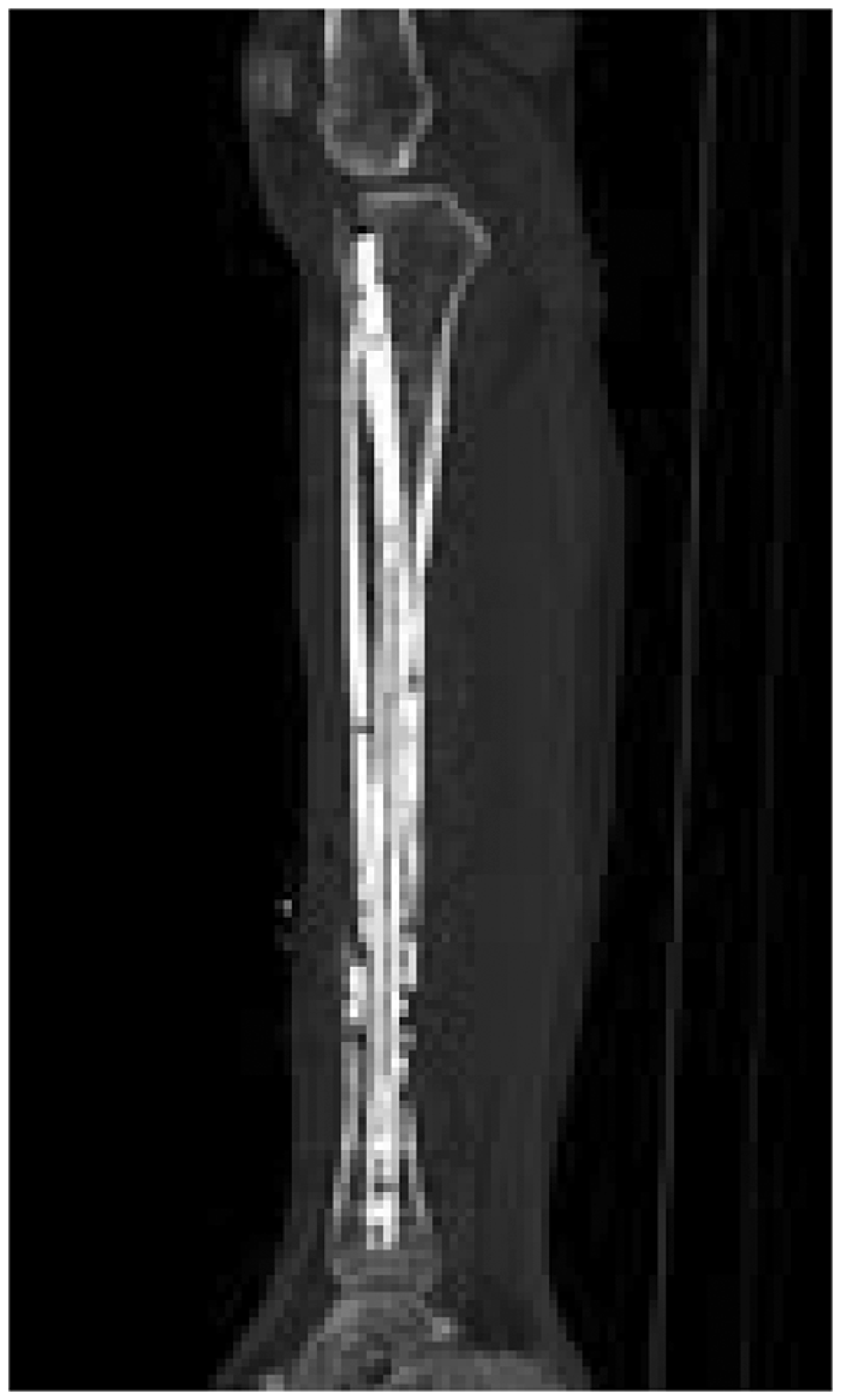
Other uses of 3-D reconstruction are in assessing orthopaedic hardware (e.g. arthroplasties, plates and screws). Previously, these patients posed great difficulties for imaging, as they are unsuitable for MRI and US (due to the metal). The metal causes large ‘streak’ artefact on CT (Figure 4), obscuring the fine details that were needed to be seen. Using 3-D reconstruction and metal-smoothing algorithms, modern CT is now significantly better at showing non-union, loosening and displacement unseen with plain film (Figure 5; Ohashi et al., 2005). It is essential that referring clinicians mention the presence of metal hardware before a CT scan, so that the streak-reducing algorithm can be applied.
Large streak artefact caused by computed tomography (CT) scanning of a metallic intra-cranial aneurysm clip, which was not mentioned on the request card. The streaking obscures anatomical detail making accurate interpretation impossible. A sagittal computed tomography (CT) image of a tibial intra-medullary nail imaged using streak-reduction algorithm software allowing assessment of both the metal hardware as well as demonstrating the surrounding anatomical detail.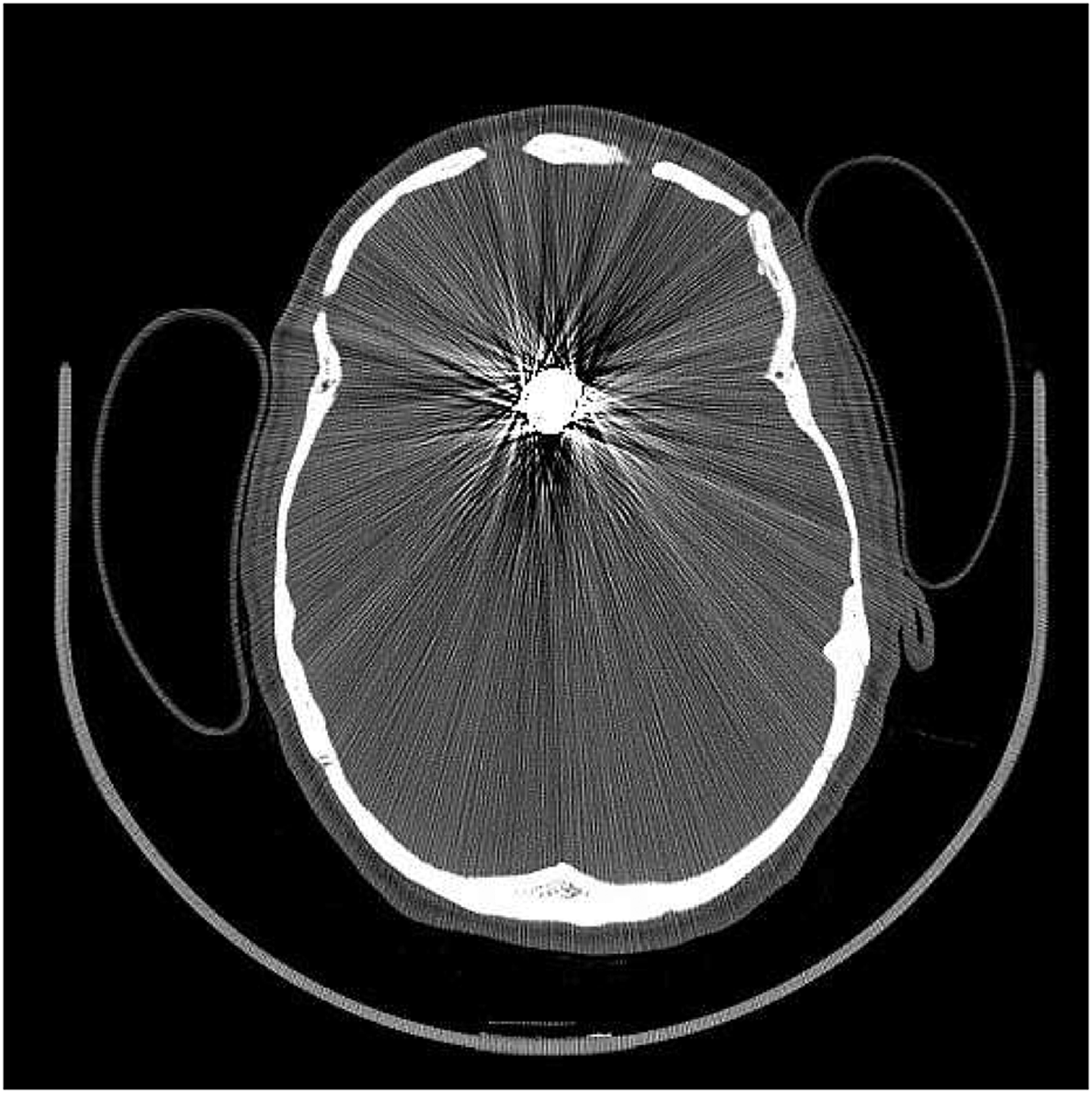
3-D recons can reduce patient radiation dose – particularly useful for paediatric patients or ‘repeat visitors’ such as alcoholics or connective tissue disorder patients, who undergo repeated imaging over a long time period (Fayad et al., 2005).
CT in major trauma: the doughnut of life
A key concept in major trauma is that serious injuries need to be detected allowing their definitive treatment without delay – the ‘golden hour’ principle (ATLS, 2008). Delay in recognition of these injuries, resulting in a delay in their treatment has been shown to increase mortality (Tien et al., 2007a). In patients requiring a laparotomy for isolated abdominal injuries, it is estimated that for every 3 min spent in the ED there is a 1% increase in mortality (Clarke et al., 2002). Diagnosis of injuries therefore needs to be accurate (high sensitivity) but also quick. CT fits this role perfectly, currently unmatched by any other modality.
As illustrated previously, CT provides excellent anatomical detail, as well as showing clinically significant visceral, vascular and retroperitoneal injuries unseen on clinical examination, plain films and FAST, in a very short time frame (Gaarder et al., 2009; Miller et al., 2003). Trauma CT scanning is significantly faster than traditional trauma imaging with plain films and FAST, as well as substantially more accurate (Wurmb et al., 2011). Prompt trauma CT scanning in major trauma has been shown to be an independent predictor for patient survival and is recommended as the new gold imaging standard, with no demonstrable adverse effects (Huber-Wagner et al., 2009). This includes haemodynamically unstable patients, once viewed as contra-indicated to CT, as it allows the cause of their instability to be identified and definitively treated (Huber-Wagner et al., 2009).
Another understated benefit of CT is that a normal CT is an excellent excluder of serious or significant injury. Therefore, a normal CT trauma scan provides a very high reassurance of no significant injury, allowing early and safe hospital discharge, with significant associated cost savings (Salim et al., 2006).
Surprisingly, although whole body CT (‘trauma scan’) is accepted as the gold standard for the imaging of major trauma, the current eighth edition of the Advanced Trauma Life Support manual (ATLS) mentions the use of plain film X-rays, namely anteroposterior (AP) chest (CXR) and pelvis (PXR) during the primary survey. CT is mentioned as a secondary survey adjunct alongside FAST (ATLS, 2008). These recommendations do not reflect the huge advances in CT technology and ED availability described previously. We expect that the ATLS guidelines will be updated in-line with accepted contemporary trauma practice, where there has been a move towards early whole body CT scanning at the expense of plain films and FAST (RCR, 2011; Wurmb et al., 2011). Skipping plain films before trauma CT results in no loss of diagnostic information, but results in a 40% time saving (Rieger et al., 2002). When prompt CT scanning is planned in the ED, serious consideration should be given to omitting the ATLS standard 3 or 5 film plain X-ray ‘trauma series’, which adds delay, cost and radiation exposure.
It should be noted that the studies mentioned above all used dedicated ED CT scanners, as opposed to transporting an ill or unstable trauma patient to a radiology department, neither equipped nor staffed for resuscitation. However, many (e.g. 40% of US EDs in 2008) have their own purpose-built emergency CT scanners adjacent to or, in some cases, within the resuscitation room to speed up access (Fung Kon Jin et al., 2008; Thomas et al., 2008). Indeed immediate 24/7 access to CT is one of the requirements for a UK major trauma centre (RCR, 2011). Consequently, non-major trauma centres without these facilities can be bypassed with proven survival benefit (ACS, 2011). This allows immediate CT trauma scanning to guide resuscitation and definitive treatment as quickly as possible, whilst minimising wasted time and unnecessary patient movement and radiation exposure.
CT versus MRI versus FAST
The limited availability, long scan length and large contra-indicated patient group, mean that MRI is not indicated for acute trauma care (RCR, 2011). It will remain as a second-line tool for the foreseeable future but should be available to major trauma units when required (RCR, 2011).
FAST is a four-view US assessment for detection of free intra-abdominal fluid (Miller et al., 2003). Despite promising data from the early 1990s, FAST cannot compete with modern CT. Trauma patients need definitive exclusion of occult haemorrhage and head injury that are the two main causes of death, but are usually undetectable by FAST. Even if only isolated abdominal injuries are suspected, retrospective analysis of 11,118 patients with blunt trauma admitted to a Level 1 trauma centre in the United States showed that 34% of patients with significant visceral injury (liver, kidney, pancreas and mesenteric lacerations) did not have a haemoperitoneum, so could not be detected by FAST (Shanmuganathan et al., 1999). Using CT as the comparator, the sensitivity of FAST by non-radiologists (trauma surgeons and ED physicians) in the United States at detecting haemoperitoneum – which FAST is designed to detect – was 42%, resulting in significant under-diagnosis of abdominal injury (Miller et al., 2003). Even when performed by European specialist emergency radiologists (who perform US studies regularly), sensitivity improved to 62%, but still the authors concede that FAST cannot reliably exclude intra-abdominal bleeding and further imaging (CT) is needed (Gaarder et al., 2009).
Using common problem areas of pelvic and cervical spine fractures, we discuss briefly the benefits that CT scanning has in their detection and management.
Pelvic fractures
Pelvic fractures can be life-threatening emergencies with significant mortality. They are the commonest cause of treatable haemorrhagic deaths (Tien et al., 2007a), associated with exsanguinating haemorrhage from the iliac arteries (or their branches), the presacral venous plexus or simply from the large bulk of bone fractured. However, the majority of deaths in patients with pelvic fractures (mostly stable fractures) are due to associated visceral vascular injuries, rather than directly from the pelvis itself. Pelvic fractures are an indicator of significant blunt trauma and major injury elsewhere, particularly the brain, thorax and abdomen (Burgess et al., 1990).
Triaging a hypotensive patient with a pelvic fracture into a stable or unstable fracture pattern is crucially important in guiding whether pelvic angiography or laparotomy is needed first. The consequences of making the wrong choice are severe (up to 60% mortality or >2.5 times increased risk; Eastridge et al., 2002). An unstable pelvic fracture needs angiography before laparotomy, even in the presence of a confirmed haemoperitoneum. This is because unstable fracture injuries are associated with a pelvic haemorrhage source, which exsanguinate quicker and are worsened by laparotomy (Eastridge et al., 2002). Conversely, a stable fracture pattern suggests an abdominal source for hypotension and laparotomy is required first.
Case 1
An elderly man presented to the ED following a simple mechanical fall at home. He complained of lower abdominal pain. He was on warfarin for atrial fibrillation (AF) and had known peripheral vascular disease. A PXR was performed (see Figure 6(a)).
Case 1: computed tomography (CT) versus pelvis X-ray (PXR).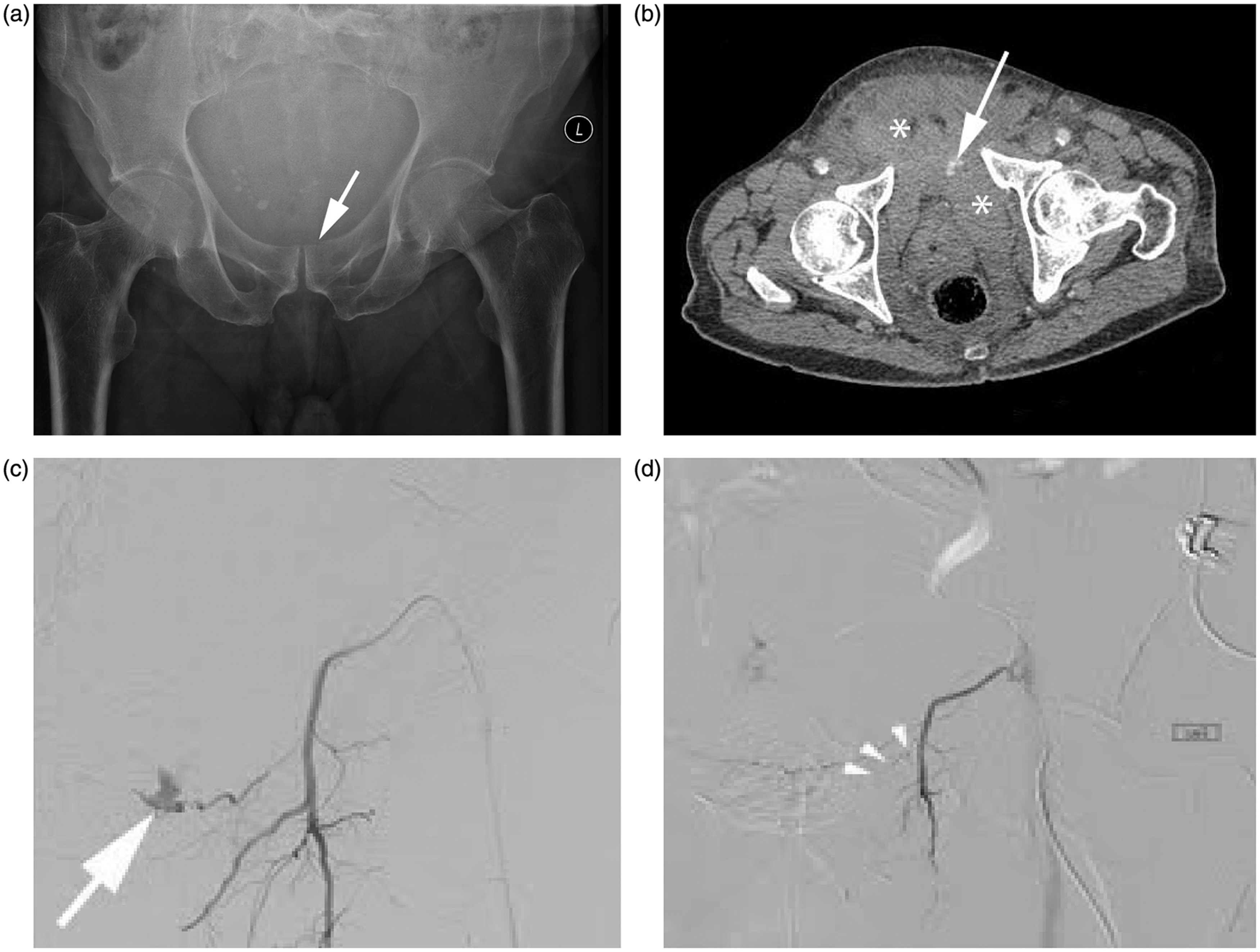
The ED junior interpreted this as showing acute urinary retention and the patient was catheterised. There was little urine output. Note the missed subtle step in left superior surface of superior pubic ramus (arrow) and absence of normal abdominal gas pattern. Over the next 4 h, the patient became progressively haemodynamically unstable. Upon senior review, fluid resuscitation was started and an urgent pelvic CT performed (see Figure 6(b)).
This single axial slice shows a large pelvic haematoma (stars) and a white contrast blush showing active extravasation (arrow).
The patient proceeded for urgent angiography that revealed the bleeding source (see Figure 6(c): arrow, ruptured aberrant obturator artery branch, a common anatomical variant).
This was successfully embolised (see Figure 6(d): metal coils, arrowheads) with a good patient outcome.
PXR only provides information regarding fracture pattern and not vascular or visceral injuries. Unfortunately, PXR has been shown in various studies to have a sensitivity as low as 68% in diagnosing both simple and complex pelvic fractures following blunt trauma (Guillamondegui et al., 2002). The same study showed that in patients having an initial PXR followed by CT scanning, the initial PXR diagnosis was changed in 69% of patients based on CT findings. Consequently, some EDs have replaced PXR altogether with CT, reducing time wastage and cost, as well as any unnecessary patient movement and relatively high radiation dose associated with PXR.
Cervical spinal fractures
The potential cost to the patient, the hospital and society of spinal cord injury is huge. In all, 55% of spinal injuries occur in the cervical region (ATLS, 2008). Therefore, ATLS assumes that all (major) trauma patients have an unstable cervical spine (c-spine) until proven otherwise, as >5% of patients experience onset or worsening of neurological symptoms after reaching the ED. Spinal immobilization is associated with various problems, including pressure sore generation, patient agitation and raised intra-cranial pressure, so prompt cervical spine clearance is essential. Patients who cannot be cleared clinically typically undergo three-view plain film imaging (AP, lateral and open mouth), but 5–8% of patients with fractures have normal X-rays (Blackmore et al., 1999). Admittedly, not all of these fractures may be clinically significant for spinal cord injury, but the vast majority (>85%) have been shown by CT to extend into the transverse foramina, with associated vertebral artery injury risk (Woodring et al., 1993). Relatively few patients (∼1.6%) following blunt trauma develop vertebral or carotid injuries (associated with a 60% risk of death or stroke), but these injuries too can be accurately detected on a standard trauma CT (Langner et al., 2008). This illustrates again how CT detects not just the primary bony injury but also the secondary, potentially treatable, occult vascular injury.
To compound matters, 10% of patients with c-spine fractures have non-contiguous vertebral fractures and 25% have at least mild brain injury (ATLS, 2008). Consequently, CT seems like an ideal solution to prevent overlooking unstable fractures: CT sensitivity 98% versus 52% for plain films (Holmes and Akkinepalli, 2005), coupled with the benefit of detecting associated vascular, head and other bony injuries. Indeed, analysis on cost-effectiveness has shown that CT is more cost-effective than plain film for all c-spine-injured patients except young patients (<50 years) with low impact mechanisms (Blackmore et al., 1999). This last finding reinforces the value of limiting CT use (cost, radiation dose) for only those patients with a reasonable chance of spinal injury, rather than as a universal screening tool. Validated clinical rules exist for assessing alert patients’ need for imaging, such as the Canadian C-Spine Rule (CCS; Stiell et al., 2001).
Unfortunately, many potential c-spine-injured patients are either unreliable (drugs/alcohol) or obtunded as a consequence of major trauma. This means that clinical guidelines (such as CCS) cannot be used with certainty. Although CT is the undisputed gold standard for identifying bony injuries, it is inferior to MRI in viewing ligamentous and disk injuries. Consequently, many clinicians request an MRI of the cervical spine to exclude spinal soft tissue injury when the CT spine is normal, for fear of missing a significant injury. A well-designed study from Baltimore examined 1400 consecutive obtunded trauma patients with cervical spine CT followed by cervical spine MRI, in order to see the consequences of missed soft tissue injury on CT. Despite using 4 and 16 slice CT (compared with current modern standard of 64 slices), CT had a negative predictive value of 98.9% for ligamentous injury and 100% for unstable cervical spine injury (Hogan et al., 2005). So, although CT did not detect 100% of ligamentous injuries, those that were missed were shown to be clinically unimportant. These authors suggest therefore that MRI should be reserved for patients with positive or equivocal CT scans (Hogan et al., 2005).
CT and radiation: the good versus the bad
This article illustrates some of the uses and benefits of CT. However, the clear benefits and subsequent increased usage must be balanced against the high (ionising) radiation dose associated with CT. A whole body trauma CT (in 2007) mean dose was 22.7 mSv, compared with 5 mSv for an AP abdominal X-ray or 0.7 mSv for a PA CXR (Tien et al., 2007b). In the United Kingdom, CT is the second largest source (after radon gas released naturally from granite) of population radiation dose (Alisy-Roberts, 2008). The chance of cancer development due to radiation exposure is purely statistical (stochastic), but it rises linearly with increased exposure. Trauma CT scanning has been estimated to result in 11.7 additional fatal thyroid cancers per 100,000 patients scanned (Tien et al., 2007b). CT has been suggested to cause up to 2.0% of all cancers in the United States, due to high population scanning rates (Brenner and Hall, 2007). Surprisingly, a recent survey found that 91% of ED physicians in the United States did not believe that CT use increased the lifetime cancer risk and they also significantly underestimated likely patient radiation dosages (Lee et al., 2004). This highlights the importance of clinicians considering whether the scan is really needed and the value of discussion with a radiologist about potential alternatives.
Clearly, in major trauma patients, the benefits of CT scanning outweigh the potential risk of future carcinogenesis. Prompt CT is required to save the patient’s life then and there. However, what about less serious trauma or elective follow-up? These risks have been recently quantified for medium trauma (median injury severity score (ISS) score of 8) and showed that there is a six-fold greater risk of mortality from trauma not diagnosed on CT than from the lifetime increased cancer risk (Laack et al., 2011). Quantified, the risk of CT attributable death was 0.1%, which although significant (as not 0%) is very small. This risk was greatest in paediatric or pregnant patients (who have increased tissue radio-sensitivity) and decreased with age (Brenner and Hall, 2007).
One of the challenges for CT manufacturers is to reduce radiation dosages, which is happening with no change in diagnostic quality (Kalra et al., 2004). Equally, referring clinicians must consider each patient individually and decide exactly what questions need answering to avoid repeat scans, and they should seriously consider omitting plain films (e.g. PXR, C-spine series), if patients are going on to have CT scans (Guillamondegui et al., 2002; Smith and Hall, 2009).
Conclusions
There is a diverse range of usages for CT, which looks to expand with the growing use of CT-guided percutaneous/minimally invasive intervention (Cronin et al., 2011). CT remains the gold standard for the imaging of all major trauma, allowing precise identification of multi-system injuries. When available, whole body CT should be used promptly to guide resuscitation and further treatment, with demonstrable survival, cost and time-saving benefits.
CT can add real benefit to the diagnosis, planning and follow-up of musculoskeletal (MSK) patients. The importance of accurate, detailed request cards and good communication with the CT team is essential to allow the best CT images to be produced (such as 3-D reformats or orthopaedic hardware assessment).
CT image quality and scan time has improved so much that further refinements are likely to be small. Further, major advances are likely to involve reducing the patient radiation burden, image reconstruction speed and metal artefact.
The main limitation of CT is radiation dose. Dosages are reducing rapidly, but avoiding inappropriate imaging is the best way to reduce patient dose. Clinicians must be aware of the cumulative cancer risk especially for non-urgent or non-essential imaging, when other imaging modalities could be used. Discussion with a radiologist is recommended for any uncertainties.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.