
Abstract
The aim of this meta-analysis was to determine the effect and magnitude of effect of pre-injury warfarin on trauma patients. Studies comparing all trauma patients (nb. not head injury patients only) on pre-injury warfarin to all trauma patients not on pre-injury warfarin were included in the meta-analysis. The search was performed using Medline via the PubMed interface; no limits were placed on the language. Ten papers were found to be suitable for the meta-analysis. There were two case control studies and eight retrospective cohort (nested case control) studies. Significant heterogeneity was present as measured by the Q test (Q value = 126.366 df = 9, p = 0.000) and also the I2 test (I2 = 92.878). The preferred model for this meta-analysis was considered to be the Fixed effect model which produced a common OR 1.952 (95% CI; 1.888–2.018, p = 0.000). The results of this meta-analysis show that pre-injury warfarin does increase mortality in trauma patients by an odds ratio of nearly two.
Introduction
Anticoagulation is universally accepted as an additional risk factor for a potentially adverse outcome in trauma patients. Surprisingly, studies that have addressed the effect of anticoagulation on mortality in patients with blunt head injury have produced conflicting and varied results. A retrospective case control study was performed by Wojcik et al. 1 comparing 416 head-injured patients who were anticoagulated to a case-matched cohort of 416 head-injured patients who were not anticoagulated. The authors found that pre-injury anticoagulation did not have an adverse effect in terms of mortality or length of hospital stay. A nested case control study by Howard et al. 2 compared 537 elderly patients on warfarin who sustained a fall from standing to 2254 elderly patients not on warfarin who sustained a fall. Pre-injury use of warfarin had an adverse effect on survival (8.6% versus 5.7%). The majority of the patients died from head injuries. With regard to trauma in general previous published studies have also produced conflicting results. The aim of this meta-analysis was to determine the effect and magnitude of effect of pre-injury warfarin on trauma patients in general. The second aim of this study was to determine whether dataset size had any confounding effect on the odds ratio for mortality in trauma patients.
Methods
The initial search was performed in November 2011 week 3 and updated in August 2013 week 2. Medline was used via the PubMed interface; no limits were placed on the language. The key words Trauma AND Warfarin were used. The final search from August 2013 generated 695 citations; all titles were reviewed for relevance. Fifty-one abstracts of the 695 abstracts were submitted for further review. Thirty-nine full papers were analysed further. Ten papers were suitable for the meta-analysis. A second search was performed using the terms Trauma AND Anticoagulation AND Mortality. The initial search was performed in November 2011 week 3 and updated in August 2013 week 2. The final search in August 2013 generated 299 citations, after de-duplication four new abstracts were reviewed for relevance. Four full papers were analysed, none were suitable for the meta-analysis. Cross-referencing did not identify any additional studies. See Figure 1 for PRISMA flow chart.
PRISMA flow diagram.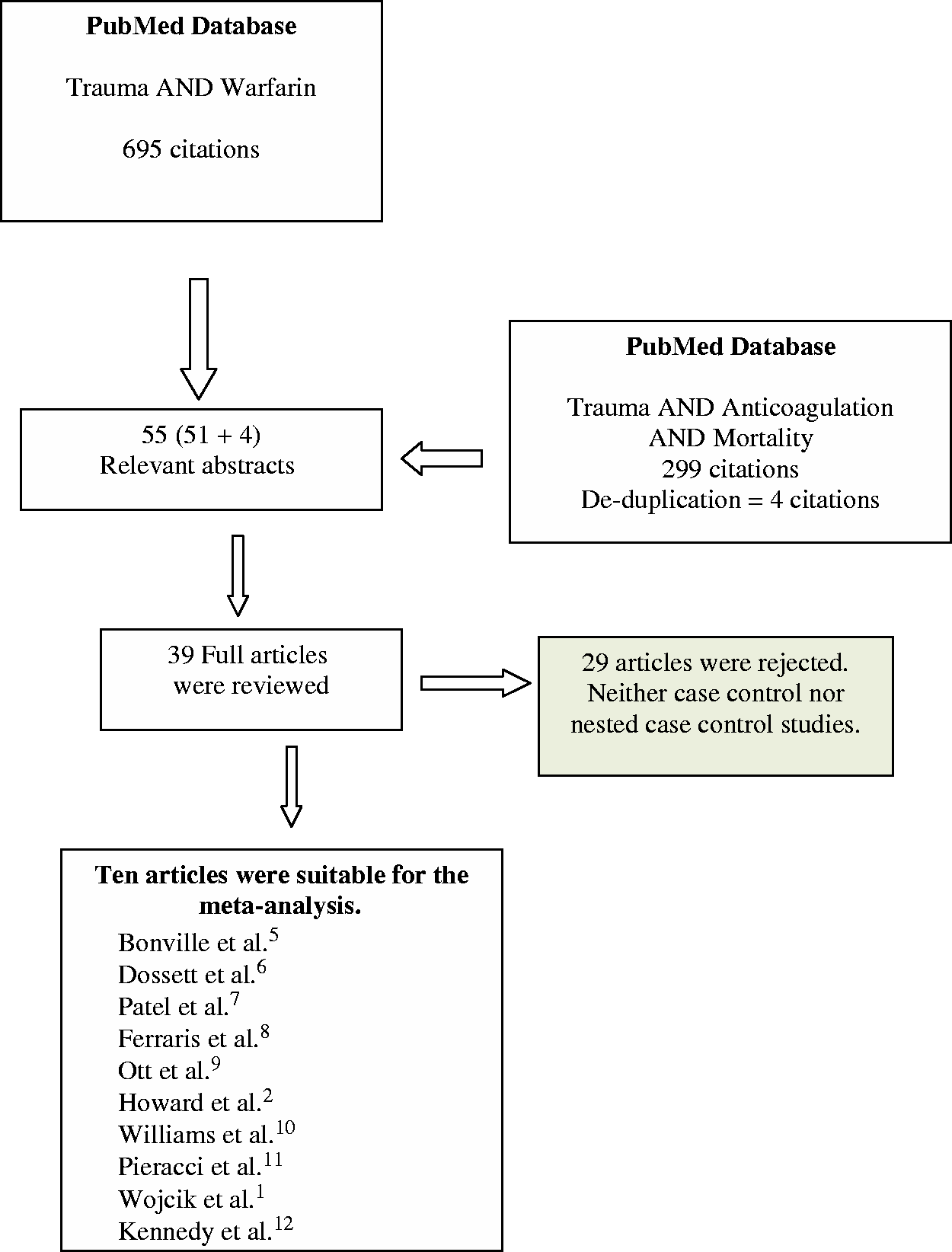
Selection criteria were broadly based upon MOOSE methodology.
3
Inclusion criteria were
Case control studies comparing mortality rates of adult trauma injury patients on warfarin versus mortality rates of trauma patients not on warfarin (Level III studies). Cohort studies of adult trauma patients with a nested case control group comparing mortality rates of patients on warfarin against mortality rates of patients not on warfarin (Level III studies). When possibly the subset of patients with head injuries were removed from the data set in view of the fact that this meta-analysis has been previously performed by Batchelor et al.
4
No lower limit was placed on the size of the study groups in either the case control or nested case control studies. Appraisal of the full papers was made by both authors. No formal grading of papers was undertaken.
Heterogeneity between studies was performed using the Q test and the I2 test. Statistical analysis was performed using Comprehensive Meta-analysis version 2 (meta-analysis.com; Biostat Inc, NJ 07631, NJ, USA). Articles were eligible for inclusion from any language provided that they were published in peer-reviewed journals. Year range: 1950 to the current year (2013).
Exclusion criteria
Case series of anticoagulated trauma patients. Cohort studies which did not separate out warfarin anticoagulation from other potential clotting abnormalities. Cohort studies including only patients with head injury. Case control or nested case control studies where it was not possible to separate out the subgroup of patients on warfarin from other subgroups e.g. Aspirin or Clopidogrel.
All of the abstracts and full papers reviewed were in English language and therefore problems with translation were not encountered. Abstracts from proceedings were not included in the search strategy neither was a search for unpublished data performed. Contact was not made with authors of any of the studies, the data were extracted directly either from the abstract or the full text.
Results
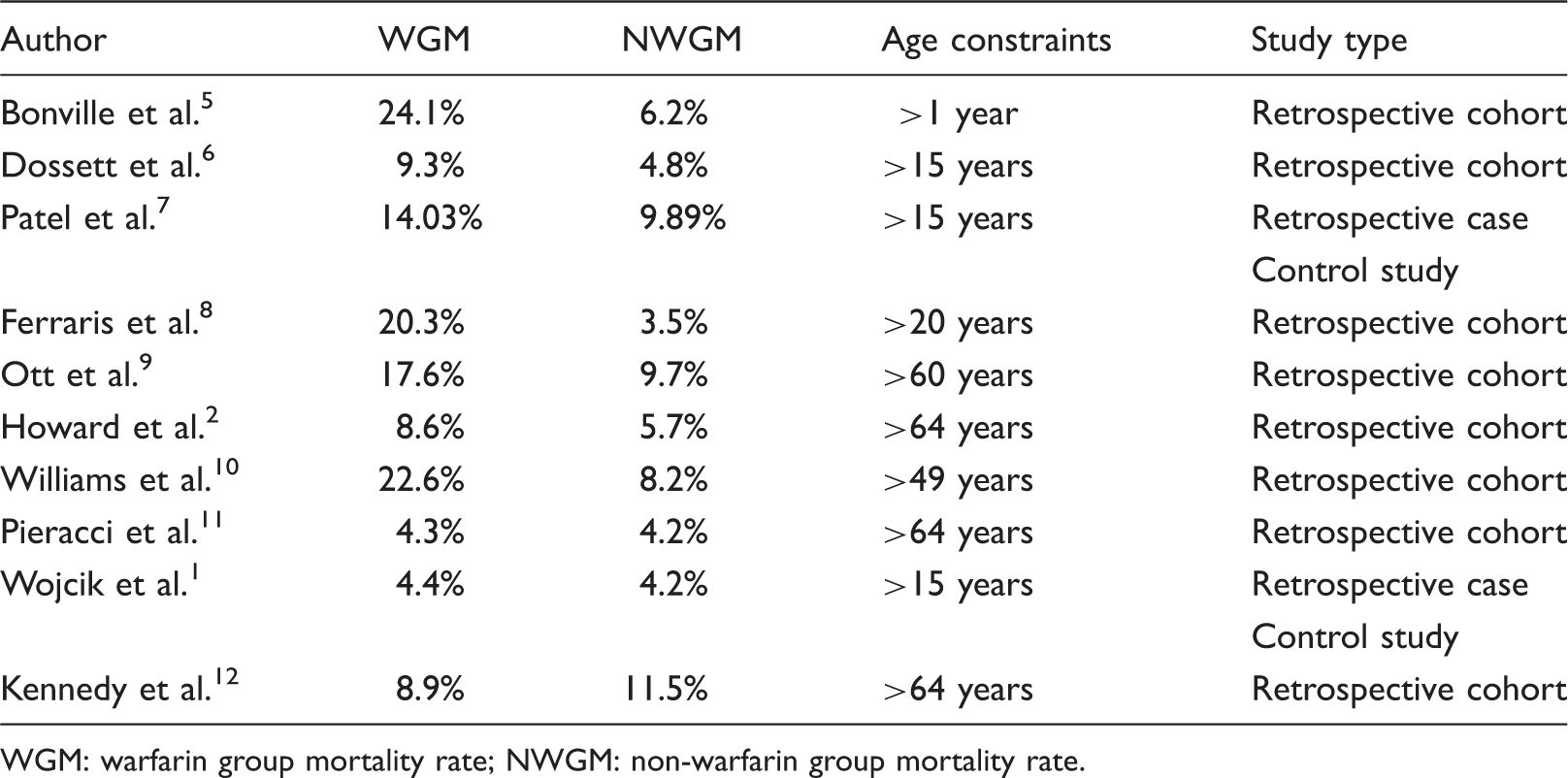
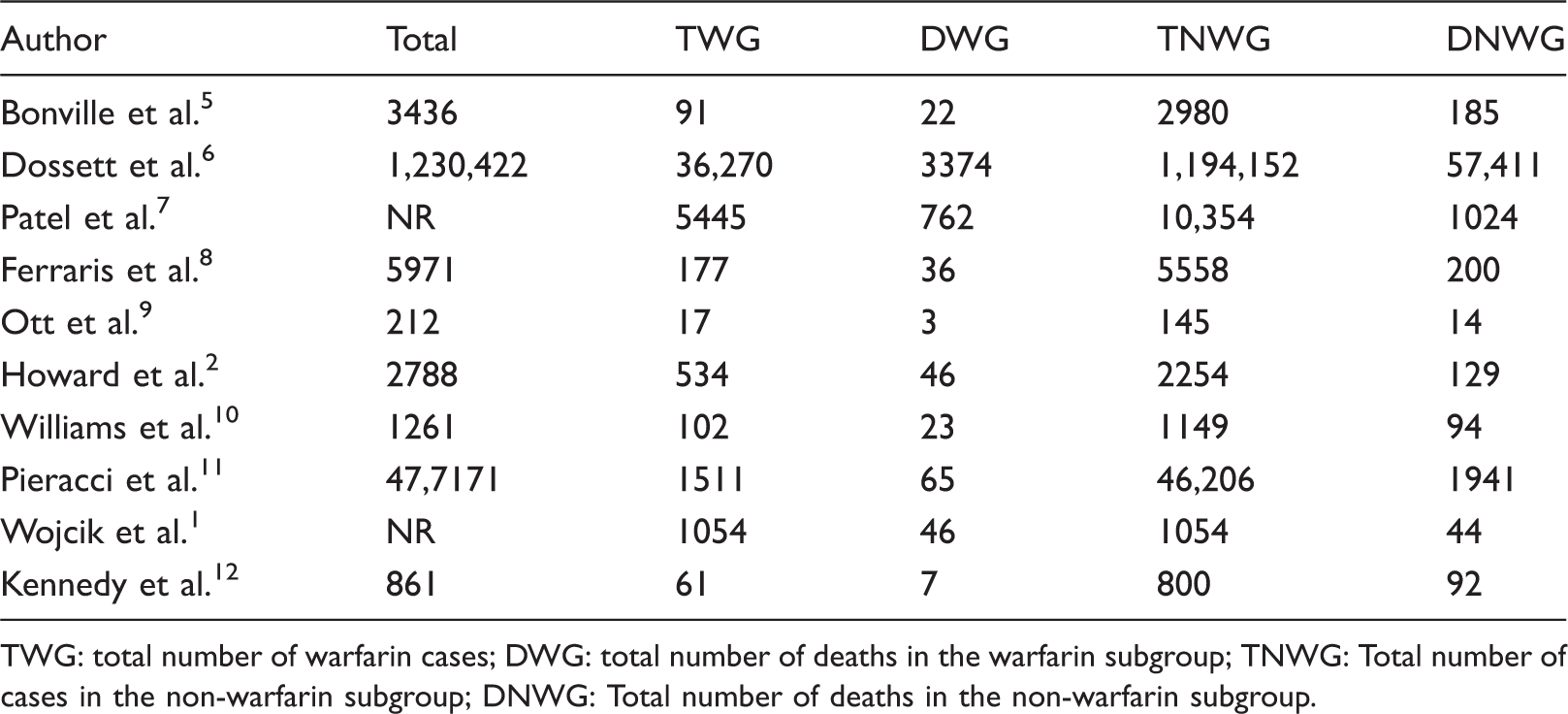
Ten papers were found suitable for the meta-analysis. There were two case control studies and eight retrospective cohort (nested case control) studies (Table 1). The size of the cohorts is shown in Table 2. The mean or median ISS values for the two study groups are shown in Table 3. The Forest plot for the unadjusted odds ratios is shown in Figure 2. The study by Bonville et al.
5
was a retrospective review of all trauma patients over the age of 1 year. Patients taking antiplatelet agents with or without warfarin were removed from the analysis (n = 365). A total of 1136 patients had intracranial haemorrhage. The study by Dossett et al.
6
utilized all patients over 15 years of age in the National US trauma data bank for the period 2002–2007. Data were available to compare all trauma patients (i.e. non head injury and head injury combined) on warfarin versus all trauma patients not on warfarin. Data were not available to study the cohort of patients over the age of 60. The study by Patel et al.
7
was a 2:1 case-matched control study using a refined dataset from the National US Trauma data bank for the period 2002–2006. All trauma patients were included in the cohort i.e. head injury and non head injury. The study by Ferraris et al.
8
(Level III study) was a cohort study (nested case control) of adult trauma patients on warfarin against the remaining cohort of patients who were not on warfarin. In total 562 patients (∼10%) in the control group were on aspirin. It was not possible to extract the cohort of patients over 60 years of age from the entire cohort. All trauma patients were included in the cohort i.e. head injury and non head injury. The study by Ott et al.
9
was a retrospective cohort of trauma patients over 60 years using the Level trauma database at Michigan. General trauma patients and those with negative CT head were included in the cohort. This was a small study (Table 2), however it was included for completeness. The study by Howard et al.
2
was a retrospective cohort study (nested case control) using the database from the Level 1 trauma centre in Pennsylvania. Only patients over the age of 64 years who sustained a fall from standing were included. As a consequence a significant number of patients had severe head injuries (25.9% warfarin group, 22.1% non-warfarin group).
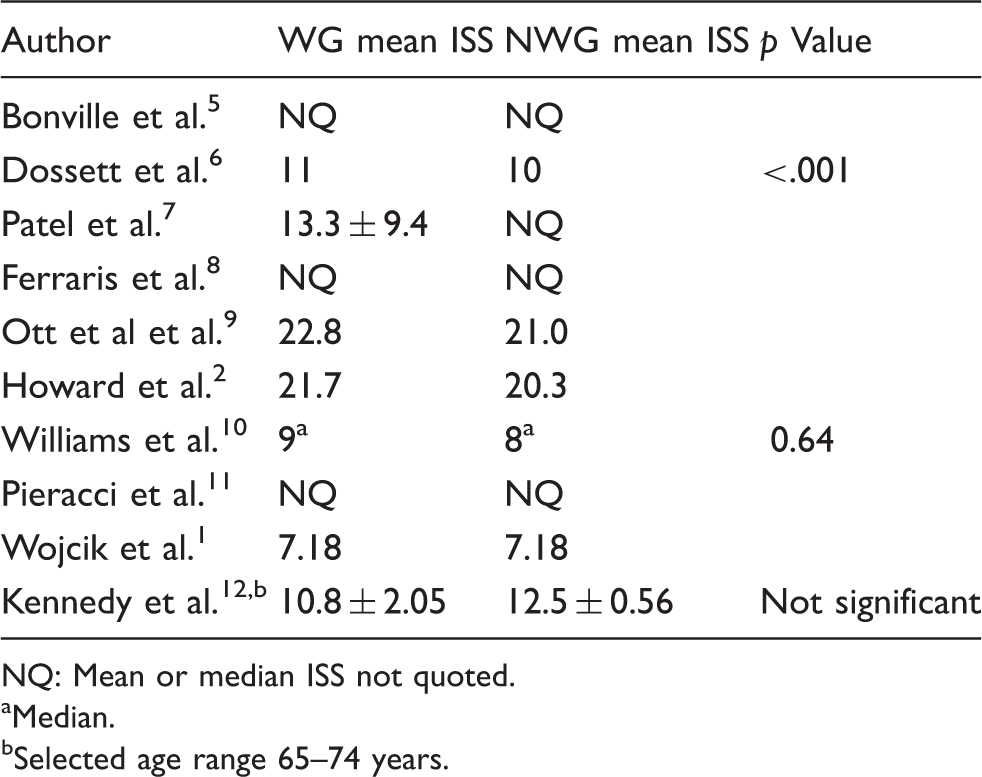
Forest plot and the unadjusted odds ratios for the 10 studies in the meta-analysis. Salient features of the nine studies. WGM: warfarin group mortality rate; NWGM: non-warfarin group mortality rate. Size of the cohort studies and the size of the individual subgroups. TWG: total number of warfarin cases; DWG: total number of deaths in the warfarin subgroup; TNWG: Total number of cases in the non-warfarin subgroup; DNWG: Total number of deaths in the non-warfarin subgroup. Mean or median ISS values for the warfarin (WG) and non-warfarin (NWG) subgroups. NQ: Mean or median ISS not quoted. Median. Selected age range 65–74 years.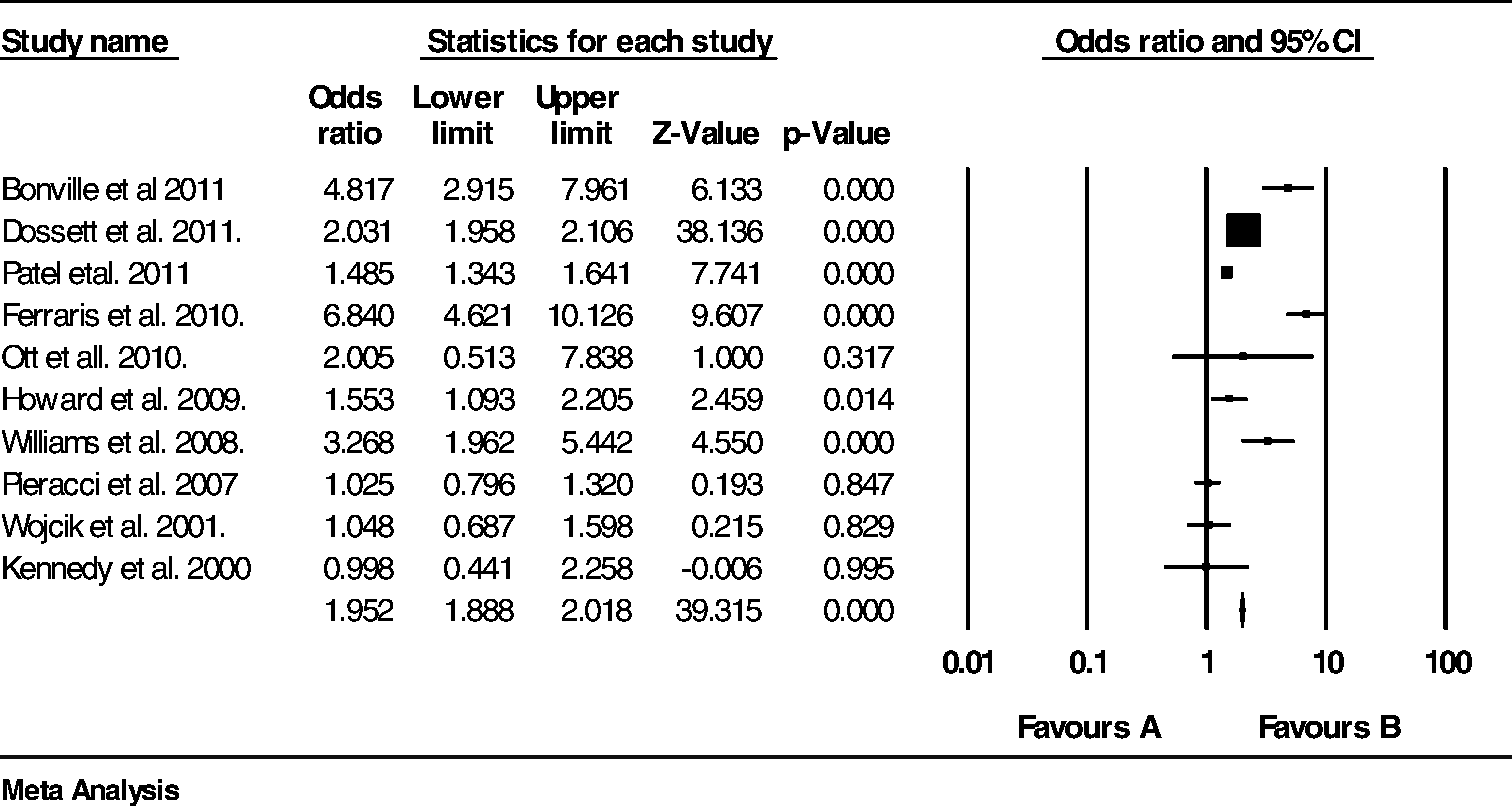
The study by Williams et al. 10 was a retrospective cohort study of patients aged 50 years or older using the trauma database at Alameda County Medical centre for the period 2000–2005. 4 All trauma patients were included in the cohort i.e. head injury and non head injury. The study by Pieracci et al. 11 was a retrospective cohort study using the New York State database for the period 2004. Only patients over the age of 64 years who sustained a fall from standing were included in the cohort. All trauma patients were included in the cohort i.e. head injury and non head injury. A total of 2536 patients had intracranial haemorrhage. The study by Wojcik et al. 1 was a retrospective case-matched control study using the Pennsylvania Trauma Outcome Study database during the period 1995–2000. The subset of patients with head injuries were removed from the analysis (416 patients were in the warfarin group and 416 patients were in the non-warfarin groups). The study by Kennedy et al. 12 was a retrospective cohort study (nested case control) using the Level 1 trauma database in Pennsylvania for the period 1993–1995. All trauma patients were included in the cohort i.e. head injury and non head injury.
Significant heterogeneity was present as measured by the Q test (Q value = 126.362 df = 9, p = 0.000) and also the I-squared test (I2 = 92.878). Heterogeneity was predominantly due to the great variation in the size of the cohort studies. The preferred model for this meta-analysis was the Fixed effect model which produced a common OR = 1.952 (95% CI; 1.888–2.018, p = 0.000). The Random effect model was also evaluated and this produced a similar result; common OR = 1.997 (95% CI; 1.546–2.580, p = 0.000).
Discussion
The results of this meta-analysis has shown that pre-injury use of warfarin increases the unadjusted odds ratio of death in trauma patients by a factor of approximately two although the value for the common odds ratio was heavily influenced by the study by Dossett et al. 6
The results of this study show a similar impact on mortality when compared to a meta-analysis recently undertaken by Batchelor et al. 4 who compared the impact of anticoagulation on patients with isolated blunt head trauma. In this particular study, the pooled odds ratio for death was found to be 2.008 (95% CI; 1.634–2.467).
Significant heterogeneity was present as demonstrated by the high Q test and I2 test was predominantly due to the large differences in size between the cohorts. Despite this difference, seven out of the ten studies produced an odds ratio in the order of 1–2, although in four studies the results did not reach statistical significance.1,9,11,12 Thus, the magnitude of effect of warfarin on mortality was found to be independent of the size of the data set in this meta-analysis.
Significant variations in the age inclusion criteria were noted. Despite this variation, age does not appear to have been a compounding effect because there is no obvious relationship between high mortality rates and cohort studies, which included elder patients only. Equally studies which included patients of all ages and therefore potentially more patients with serious injuries did not have higher mortality rates compared to the studies which included elder patients only. With regard to the study by Bonville et al., 5 the only study to include patients under 15 years of age, it was not possible to remove the paediatric data for the purposes of this meta-analysis.
Mean ISS values were found to range from 7.18 to 22.8 for the warfarin group and 7.18 to 21.0 for the non-warfarin group. Interestingly, the two studies with the highest mean ISS levels (see Table 3)2,9 were not the same studies with the higher mortality rates (see Table 1).8,10 In only one study 1 was it possible to remove the subset of patients with head injuries. A sub meta-analysis on anticoagulated patients with isolated head injuries was not undertaken as this study has recently been published by Batchelor et al. 4 Mortality rates in the warfarin subgroup were found to range widely (4.3%–24.1%). This is in contrast to the mortality rates in the non-warfarin subgroup where the mortality rates were noted to cover a narrower range (3.5%–11.5%). The reason for the differences in these ranges is not entirely clear. The studies with the higher mortality rates in the warfarin group did not correspond to the higher mortality rates in the non-warfarin group. Therefore, the studies with the higher mortality rates did correspond to the studies with the higher odds ratios.5,8,10 The main limitation to this study as mentioned previously is the heavy weighting towards the Dossett study. 6 A further limitation to this meta-analysis is that apart from the two case control studies,1,7 the remaining studies were nested case control studies and although reasonably matched by ISS were not well matched in terms of the relative size of the control group. Despite this limitation there was reasonable concordance with regard to the magnitude of the unadjusted odds ratio for the majority of the studies.
Conclusions
The results of this meta-analysis have shown that pre-injury warfarin does increase mortality in trauma patients by an odds ratio of nearly two. This effect was found to be independent of the size of the dataset.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.