
Abstract
Procedural sedation and analgesia (PSA) is a core part of modern emergency department (ED) care allowing the rapid provision of important procedures. The safe delivery of a PSA service requires an appropriately staffed and equipped environment backed up by an ongoing system of training, audit and review. Topics covered in this review include: the evidence relating to the agents used; patient care before, during and after the procedure; the outcomes of ED PSA; and, the special considerations relating to PSA in children.
Introduction
The emergency department (ED) is a challenging clinical environment with a spectrum of disease from life threatening injury and illness to minor complaints. A significant proportion of patients will have a presenting complaint, that to be appropriately managed, will require a procedure or intervention that results in pain or discomfort, e.g. fracture reduction, wound closure or electrical cardioversion. Procedural sedation and analgesia (PSA) is a technique of administering sedatives or dissociative agents with or without analgesics to induce a state that allows the safe and comfortable delivery of these procedures whilst maintaining cardiorespiratory function. The ability to deliver this service is an important aspect of emergency medicine practice and is now part of the core training of emergency physicians in many countries.
The delivery of PSA in the ED is vital to the provision of high quality emergency care but has significant reported attendant risks. This has led to greater emphasis on training and monitoring, a safe clinical environment and the development of professional guidelines and standards. However, there remains debate and some controversy as to who, how and when ED patients should receive PSA. Key areas of debate include: the skill set and experience of clinicians administering drugs such as propofol, the use of end tidal CO2 monitoring, the need for fasting and the rate and definition of adverse events.
This review assimilates current state of the art evidence on ED PSA to provide the reader with an understanding of all aspects of this core ED activity.
Procedures
Equipment
ED PSA should be carried out in the resuscitation room, or in a separate similarly equipped area. The one exception to this may be for procedures where only Entonox™ (nitrous oxide and oxygen) is being utilised, in which case any clinical area of the ED may be used. 1 Use of a resuscitation room level facility should ensure the availability of resuscitation equipment, airway adjuncts, suction and appropriate monitoring equipment.
Training, credentialing and staffing
The availability of appropriately trained and experienced staff is central to the safe provision of PSA in the ED. Minimum safe staffing includes: one practitioner solely responsible for the safe and effective delivery of PSA, “the Sedationist”; one practitioner solely concerned with the procedure, “the Proceduralist”; and one additional member of staff to provide assistance and support. 1
All members of the team should be appropriately trained for their role. For doctors in training this may be built into the requirements of a wider rotation or training programme. However, each department is likely to require its own training scheme to ensure that permanent and sessional medical staff are competent and up-to-date. The introduction of such a credentialing scheme has been shown to improve adherence to good practice; however the effect may decay over time. 2 Therefore, a programme of regular education and update is required.
Audit and governance
All EDs should have a PSA governance system coordinated and led by a named physician. All areas of the process should be monitored including: pre-procedure assessment, procedure delivery and safe-discharge. Adverse events should be recorded and monitored.
Pre-procedure assessment
Before embarking on a procedure requiring PSA in the ED there are a number of important factors to consider. These include patient factors such as: airway evaluation, co-morbidities and fasting status. Also procedural factors such as the degree of urgency and target sedation depth need to be considered.
The aim of airway evaluation is to rapidly identify characteristics of a potentially difficult airway. A number of systems have been developed which can be used in the ED including LEMON (Look externally, Evaluate 3-3-2, Mallampati score, Obstruction of upper airways, Neck mobility) and HAVNOT (History, Anatomy, Visual clues, Neck mobility, Opening of the mouth, Trauma).3,4
A North American consensus document addressed the issues of fasting and the urgency of the procedure. 5 No evidence was found for pharmacologic pre-treatment with antiemetic drugs such as metoclopramide. The expert group recommended that the urgency and fasting status of the patient should both be considered, and then a decision was made about the target sedation depth. Whilst this approach seems reasonable it is potentially complex.
A large clinical literature review identified only one reported case of aspiration during ED PSA, among 4657 adult and 17,672 paediatric cases described in the literature. They concluded that there is no evidence to support routine fasting prior to ED PSA. 6
Sedation depth is a further consideration. Deeper levels of sedation are associated with increased rates of adverse events.7,8 Conversely, deeper levels of sedation have also been found to be associated with increased patient satisfaction. 9 Even once a target sedation depth has been chosen, such a target may be hard to achieve, especially if rapid onset agents such as propofol are used. 10 Other factors such as alcohol intoxication or variation in response to pain between patients may also make achieving an agreed sedation target difficult. Notwithstanding these challenges, the sedationist and proceduralist will need to decide on the most appropriate level of sedation. This target should be clearly communicated to all members of the clinical team involved in the sedation procedure.
Monitoring
Methods for monitoring patients during PSA can be divided into physiological and observational processes. Traditionally, the monitoring of physiological changes during procedural sedation includes three-lead ECG, pulse oximetry to record oxygen saturations, respiratory rate and measuring non-invasive blood pressure at regular intervals.
A number of randomised, controlled trials in the last decade have shown ETCO2 monitoring to be useful in the early recognition of hypoventilation and providing advanced warning of hypoxic events. 11 Abnormalities in capnography, however, are frequently transient and have not been shown to be related to adverse outcome or the requirement for intervention. In 2012, the Royal College of Anaesthetists and the College of Emergency Medicine published new guidelines in the UK, which included a recommendation for the routine use of end-tidal carbon dioxide (ETCO2) monitoring on all patients undergoing procedural sedation in the ED. 1
The American Society of Anesthesiologists describes sedation as a continuum, from alert to minimal, moderate and deep sedation; culminating in general anaesthesia. Observational monitoring allows the physician to assess the depth of sedation, to avoid over-sedation and the inadvertent induction of general anaesthesia. 12
Another commonly used observational monitoring tool is the modified Ramsay sedation scale. This scores the patient between 1 and 6. A score of 1 represents agitated or restless, a score of 2 represents co-operative and oriented, through to a score of 6 which is unresponsive. 13
None of the commonly used sedation scales has been validated for use in the ED.14,15
Pharmacologic agents for PSA
ED PSA was first described in North America using agents such as diazepam, chloral hydrate and pethidine (meperidine)-promethazine-chlorpromazine.16–18 Over the past 25 years, agents previously reserved for use in anaesthesia and intensive care medicine have been increasingly used in ED PSA.
The ideal agent should provide analgesia, amnesia and anxiolysis, whilst preserving airway reflexes, and maintaining cardiorespiratory stability. Moreover, it should have rapid onset and offset; be reversible, titratable and have a large therapeutic index. There is no single ideal agent. Combinations of agents are often used to achieve the desired effect, but this may increase the unpredictability of the response. The procedure, the patient, the operator's experience and the environment influence the choice of agent. The following section describes the most common agents and the evidence pertaining to their ED use in both adults and children.
Opioids
Opioids are powerful analgesics with some sedative properties. They produce respiratory depression and have minimal cardiovascular effects. Fentanyl is utilised in procedural sedation due to its rapid onset and short duration of action. It is 100 times more potent than morphine.
Opioids are commonly used in conjunction with other agents to provide analgesia and augment the sedative effects of other agents. There is extensive experience with fentanyl whilst newer, shorter acting agents such as alfentanil and remifentanil are less well described.19,20
Nitrous oxide
Nitrous oxide (N2O) is a colourless, sweet smelling gas that is highly soluble in plasma and excreted unchanged by the lung. It has analgesic and amnesic properties with a short duration of action and minimal side effects. It is contraindicated in patients with a potential gas filled space, such as a pneumothorax. Patients control the amount they inhale through portable pressurised cylinders containing 50% N2O concentration and 50% oxygen. It can be administered in concentrations up to 70% via anaesthetic circuits. A study in 762 children found no difference in adverse events or sedation depth when comparing 70% with 50% concentrations. 21
N2O can be a useful adjunct to many agents, particularly in children. It has been successfully used to enable manipulation of forearm fractures in children when used in combination with morphine. 22 However the combination of N2O with an opioid has also been found to result in increased vomiting and deeper sedation scores in children. 23
Midazolam
Midazolam is a rapid onset benzodiazepine that provides amnesia and sedation. It has no analgesic properties and has a half-life of 60 min. It can be administered orally, intranasally and intravenously. Intranasal midazolam has been found to be effective in children, 24 although one study found that this is less effective than intravenous midazolam/ketamine. 25 Adverse effects include respiratory depression and hypotension. It can be reversed with flumazenil. Hypoxia occurs rarely, even in the absence of oxygen supplementation, but subclinical respiratory depression may occur. 26
Experience with midazolam in the ED is extensive and it remains a safe and efficacious choice, often in combination with fentanyl.7,27
Methohexital
Methohexital is a rapid acting barbiturate with no analgesia properties. It can cause hypotension, airway compromise, bronchospasm and respiratory depression. The safe use of methohexital in EDs has been described for a variety of indications 28 with a similar safety profile to propofol. 29
Etomidate
Etomidate is an ultra-short acting hypnotic sedative with a rapid onset and offset and reported safety in the ED.30–32 It has no analgesic properties, minimal cardiovascular effects and has dose dependent respiratory depressive effects. In a study of 60 children, mostly undergoing manipulations, minor respiratory events were noted in over 30% of cases. None suffered a significant adverse event. 33 Etomidate may cause pain on injection and myoclonic jerking. Concerns regarding adrenal suppression after its administration may have diminished its use in the ED. 34
Propofol
Propofol is an ultra-short acting sedative with a rapid onset and short duration of action. It may cause apnoea, hypotension, loss of airway reflexes and pain on injection. 35 Propofol has traditionally been considered to have no analgesic properties, although this has been challenged recently. 36 Several papers have described the safe and effective use of propofol in the ED, although an increased risk has been reported in older patients and those with deeper sedation.37–40
Advocates of propofol point to faster post-procedure recovery times and associated shorter time to ED discharge compared to midazolam19,41–43 and compared to ketamine.44–47 It has been suggested that these reductions in time spent in the ED could lead to cost savings. 48
Ketamine
Ketamine is an N-methyl-
Ketamine has been found to be safe and effective for use in ED PSA in both paediatric 51 and adult populations.52–54 Laryngospasm, hypersalivation and vomiting are reported side effects.27,55,56
“Ketofol” – ketamine and propofol
There are theoretical reasons why combining the pharmacologic properties of these two agents may provide ideal sedation conditions with minimal adverse effects.
This novel combination has been reported to have advantages in terms of recovery times, satisfaction and reduction in vomiting when compared against both propofol and ketamine as single agents.57–61
Outcomes
A case may be deemed ‘successful’ when the level of sedation is adequate to allow the clinician to complete the painful or unpleasant procedure, cardiorespiratory function is preserved and no adverse events occur. 62 The Quebec guidelines for PSA in children further expand this to include patient experience, stating sedation failure is one in which there is unpleasant recall of the procedure or the patient requires physical restraint or in which the patient experiences a sedation-related adverse event resulting in abandonment of the procedure, a permanent complication or unplanned admission to hospital. 14 Technical difficulties can result in failure of the procedure, even if conditions produced by sedation are optimal. In the published literature, success is often poorly defined and assumed to be completion of the procedure without reference to patient satisfaction or recall.
Factors associated with failure to complete procedure
Most studies report success rates of above 95%53,63–67 with lower rates of success of 62% to 78% reported for reduction of dislocated hip prostheses.68–70 A large prospective observational study reported significant risk of failure for reduction of dislocated hip, as compared to shoulder reduction. The same study also reported increasing rate of failure in adult patients weighing >100 kg. 71
Many patients with dislocated prosthetic hips have medical comorbidities and given the risks of adverse events and relatively high failure rates in this population, further research is needed to identify patients unsuitable for attempted reduction in the ED. Age, level of sedation, ASA grade and seniority of physician do not appear to be associated with increased rate of failure.65,70–72
Patient recall and satisfaction
There is an inverse relationship between patient satisfaction with PSA and both patient recall and pain.9,73 Recall rates are generally reported at 4–8%40,46,73,74 with higher rates in patient controlled sedation 66 and at lighter levels of sedation. 65 Interestingly, the presence of a grimace or groan during the procedure was not found to be associated with recall or patient satisfaction but was associated with low levels of physician and nurse satisfaction. 73
In addition to information on adverse events, it is good practice to advise patients of the risks of failure to complete the procedure and of recall, when obtaining informed consent for PSA.
Adverse events
There is considerable variation in the definition of adverse events associated with PSA. The World Society of Intravenous Anaesthesia (SIVA) International Sedation Task Force was set up to establish definitions and terminology in order to improve the reporting of sedation related adverse events across disciplines. A consensus document was published with intervention and outcome based definitions. 75 Sedation-related events are common, adverse events requiring interventions are less common and adverse outcomes, such as aspiration requiring intubation or cardiac arrhythmia requiring treatment, are exceptionally rare.76,77
Accepting the variable definitions of adverse events used in individual studies, there are certain factors associated with an increased rate of these events.
Age
A large prospective observational study reported age >50 years old to be associated with increased risk of adverse airway and respiratory events (odds ratio (OR) 2.3, 95% confidence interval (CI) 1.3–3.5, p < 0.001). 8 A smaller study reported a marginally significant increase in the rate of hypotension in the over 65 age group. 72 In contrast, a large observational study undertaken by the authors of this review did not show an association between increasing age and the risk of adverse events. 7
ASA class
There is strong evidence from several large prospective observational studies that higher American Society of Anaesthesiologist physical status class is associated with a higher risk of complications.39,64,78 Although a recent study, looking solely at PSA for dislocated hip prostheses did not find an association between ASA and complications. 70
Depth of sedation
Increasing level of sedation is associated with increasing risk of sedation related events.7,8 Two cases of aspiration have been reported both in elderly women meeting recommended fasting criteria who were sedated to a depth of general anaesthesia.8,76
Time of day
Procedures carried out during the hours of 20:00–07:59 are associated with higher rates of complications than those conducted during the day following multivariable logistic regression analysis in a large prospective observational study. 7 The reasons for this association are not clear. Possible contributory factors include: different patient mix during these times; different staff mix; fatigue and cognitive factors.
Recovery and safe discharge
The patient should remain in a clinical area with the same level of facilities and monitoring as required during the procedure, until level of consciousness and vital signs return to pre-procedural levels.
1
A safe-discharge check list is described in Figure 1. Reassuringly, most serious adverse events occur during the procedure. In a large registry of 1367 paediatric sedations, 92% of adverse events occur during the procedure and no primary serious adverse events occurred beyond 25 min from administration of final sedating agent, thus advocating a 30 min post-sedation observation period in this population.
79
Suggested pre-discharge checklist for use following procedural sedation and analgesia (PSA).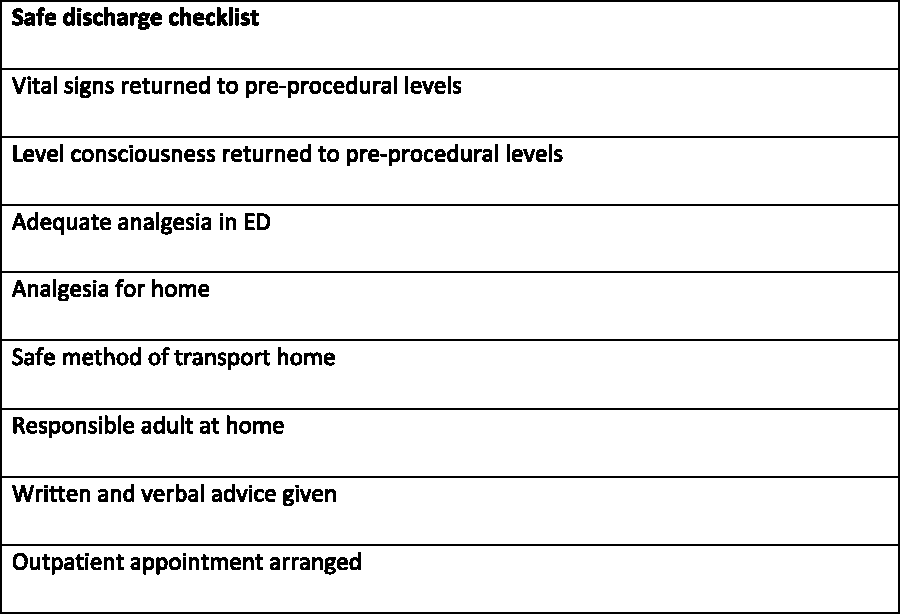
Reported times from end of sedation to discharge from the ED vary considerably with most studies reporting times of >60 min.63,80,81 This reflects findings from a nationwide survey into standards of practice in UK EDs 82 and is likely to represent adequate time for physiology to return to baseline and a wide safety margin for detection of serious adverse events.
Several prospective case series45,49,81 and one small randomised trial 47 report shorter recovery times with propofol compared to midazolam, though data on whether this translates to shorter length of ED stay are limited. Longer recovery times have been reported in older patients. 49 Patients suffering from an adverse event during the procedure take a longer time to recover and have a longer stay in the ED.49,83 These delays may be an indication that patients suffering from adverse events are more likely to have been deeply sedated. It may also be that after noting an adverse event, clinicians undertake a longer period of post-procedure observation in addition to the time required to deal with the actual adverse event.
Appropriate post-procedure written and verbal advice is mandatory. Although significant adverse events post-discharge are rare, a larger group of patients may experience some symptoms. In one study, 13% of adults undergoing PSA complained of symptoms including drowsiness and headache after discharge. 73 Paediatric studies have reported incidences of 15–42% of symptoms following discharge.79,84 The parents of children receiving ketamine for PSA should be warned of delayed adverse effects of gastrointestinal upset, sleep disturbance, nightmares and ataxia. All patients should be discharged home with a responsible adult.1,85
Procedural sedation in children
Procedural sedation in children is increasingly performed outside the operating theatre and by non-anaesthetists. A number of studies have suggested that it can be delivered safely by emergency physicians. In a large study carried out in the USA by the Paediatric Sedation Research Consortium examining 131,751 paediatric procedural sedation cases recorded by a variety of healthcare professions, there was no statistical difference between the different provider complication rates including emergency physicians, paediatricians, anaesthesiologists and intensivists.64,86,87
Psychological/distraction techniques can also be very important and may reduce the amount of sedative agent used. These should include taking the time to explain the procedure, what the child needs to do, what sensation they may experience and things they can do to help cope appropriate to the child's age. It is important to also consider the presence of a parent or guardian in the room as this may reduce some of the child's anxiety. Play specialists and other distraction techniques may also be of benefit. 88
There will still be times, however, when PSA is required. The type of sedative agent selected will be multi-factorial and may be affected by the age of the child, the level of anxiety, previous experience and the type of procedure to be performed. The pharmacological properties of the various available agents are discussed elsewhere in this review.
One emerging area is the use of propofol for paediatric PSA. 89 However, the use of this agent by non-anaesthetics in the paediatric age group remains controversial.
Conclusion
PSA is now a core part of the service delivered by a modern ED. In this review we have aimed to summarise current best practice based on the available evidence.
An appropriately equipped environment within the ED is essential. Individual staff competence cannot be assumed and there should be a system of training, education and credentialing. Many different agents are available and the final choice of agents and dose should take account of the planned procedure and desired depth of sedation. PSA can be particularly useful in children, but different techniques and strategies are likely to be required. Overall adverse event rates are low, but a robust clinical governance system overseeing PSA should be considered mandatory.
In the future, the role of patient controlled sedation may increase. 66 Other agents such as dexmedetomidine may be studied more in the ED context adding to the choices available. 90 Training and credentialing in ED PSA will continue to develop. An increased role for simulation and consideration of human factors and situational awareness is likely.
Properly organised and delivered PSA in the ED provides safe, effective and high quality treatment and care.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.