
Abstract
Coronary artery occlusion following a blunt trauma is a rare complication. We report a case of a 56-year-old man who experienced an intermediate code trauma following a motor vehicle accident. The patient had a visible ‘seat-belt sign’ and complained of chest pain. Initial electrocardiogram showed mild ST segment elevation accompanied by elevation of cardiac enzymes. Echocardiogram and cardiac magnetic resonance imaging were consistent with right ventricular systolic dysfunction. Coronary angiogram revealed 100% occlusion of proximal right ventricular marginal branch. The patient was managed medically. This case presents a rare case of right ventricular marginal occlusion following blunt chest trauma.
Introduction
The medical literature contains 77 reported cases that fulfilled the WHO criteria for myocardial infarction after blunt chest trauma (BCT) since 1974. 1 The spectrum of blunt cardiac injury (BCI) ranges from asymptomatic myocardial bruise to cardiac rupture and death. The incidence of BCI following blunt thoracic trauma has been reported to be 20%–76%. 2 BCI can lead to conditions such as cardiac free wall rupture, septal rupture, coronary artery injury, cardiac failure, complex arrhythmias and minor electrocardiography (ECG) or cardiac enzyme abnormalities.2,3
We report the case of a man who sustained BCT in a motor vehicle collision (MVC), resulting in a unique case of total occlusion of a proximal right ventricular (RV) marginal branch. The case underscores the importance of electrocardiography and cardiac enzyme abnormalities in risk stratification of BCT cases and describes alternative therapeutic options for its management.
Case report
A 56-year-old man presented to the Ronald Reagan UCLA Emergency Department as an intermediate code trauma following a MVC. He was a restrained backseat passenger and significant passenger space intrusion to the driver’s side was noted. The patient reported diffuse abdominal and chest wall pain upon arrival to the resuscitation suite. Chest wall pain was worse with inspiration and palpation of sternum and ribs, but he denied any chest pressure, jaw pain, back or left arm pain. He was hemodynamically stable and had a visible seatbelt sign. He had no previous history of myocardial infarction or chest pain and reported riding his bicycle long distances several days prior to his injuries without any symptoms. He disclosed a past medical history of hypertension and hyperlipidemia.
On hospital Day 2, the patient was noted to have an elevated troponin. Subtle, less than 1 mm ST elevations in leads II, III, and aVF were identified on ECG (Figure 1). Troponin on admission was 2.2 and peaked at 20.8 on Day 2. Computed tomography angiogram at the time of admission showed no evidence of pulmonary embolus or dissection.
ECG on hospital Day 2 showing normal sinus rhythm with heart rate of 84 beats per minute. There are subtle, less than 1 mm ST elevations in leads II, III and aVF.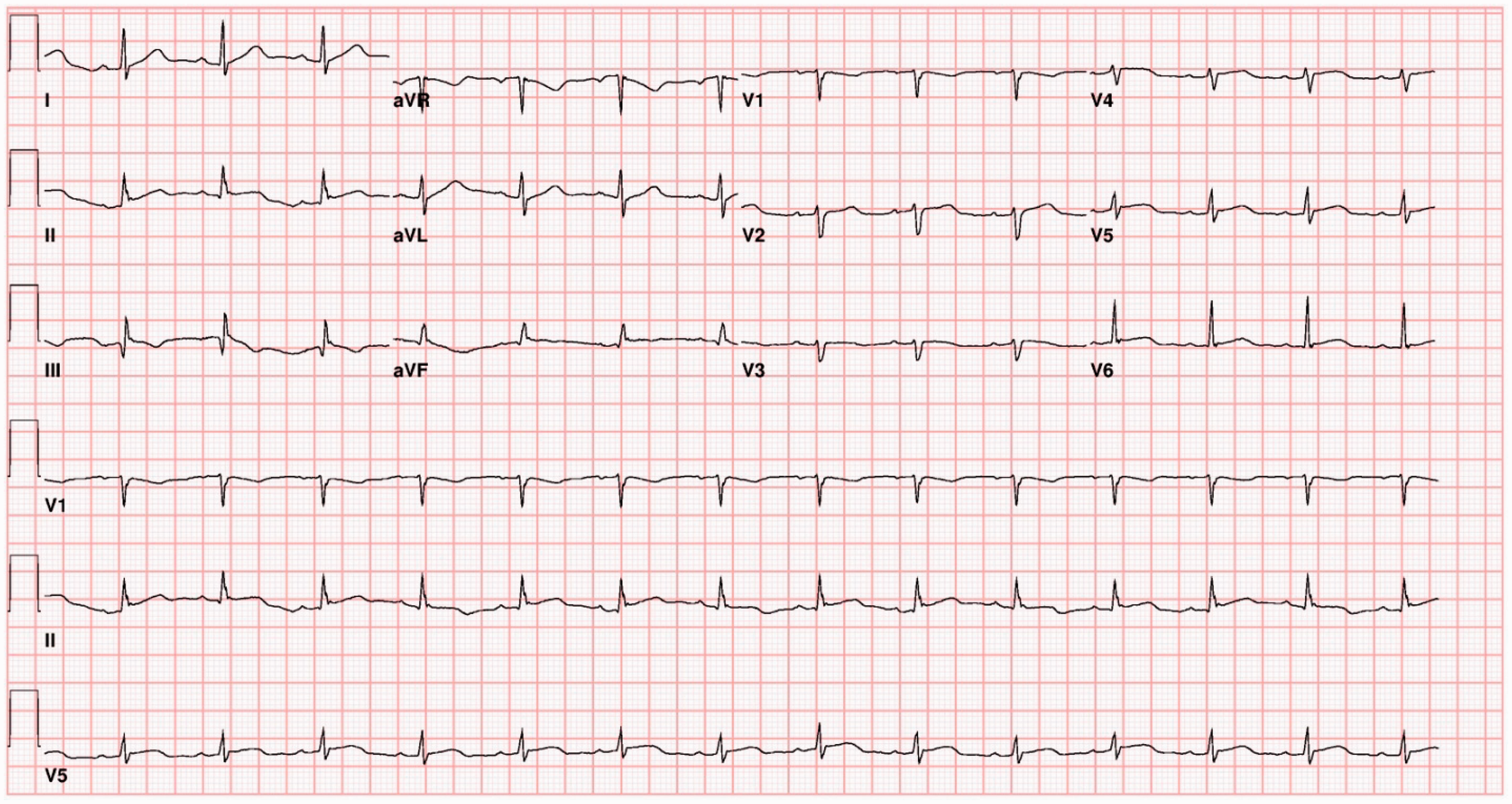
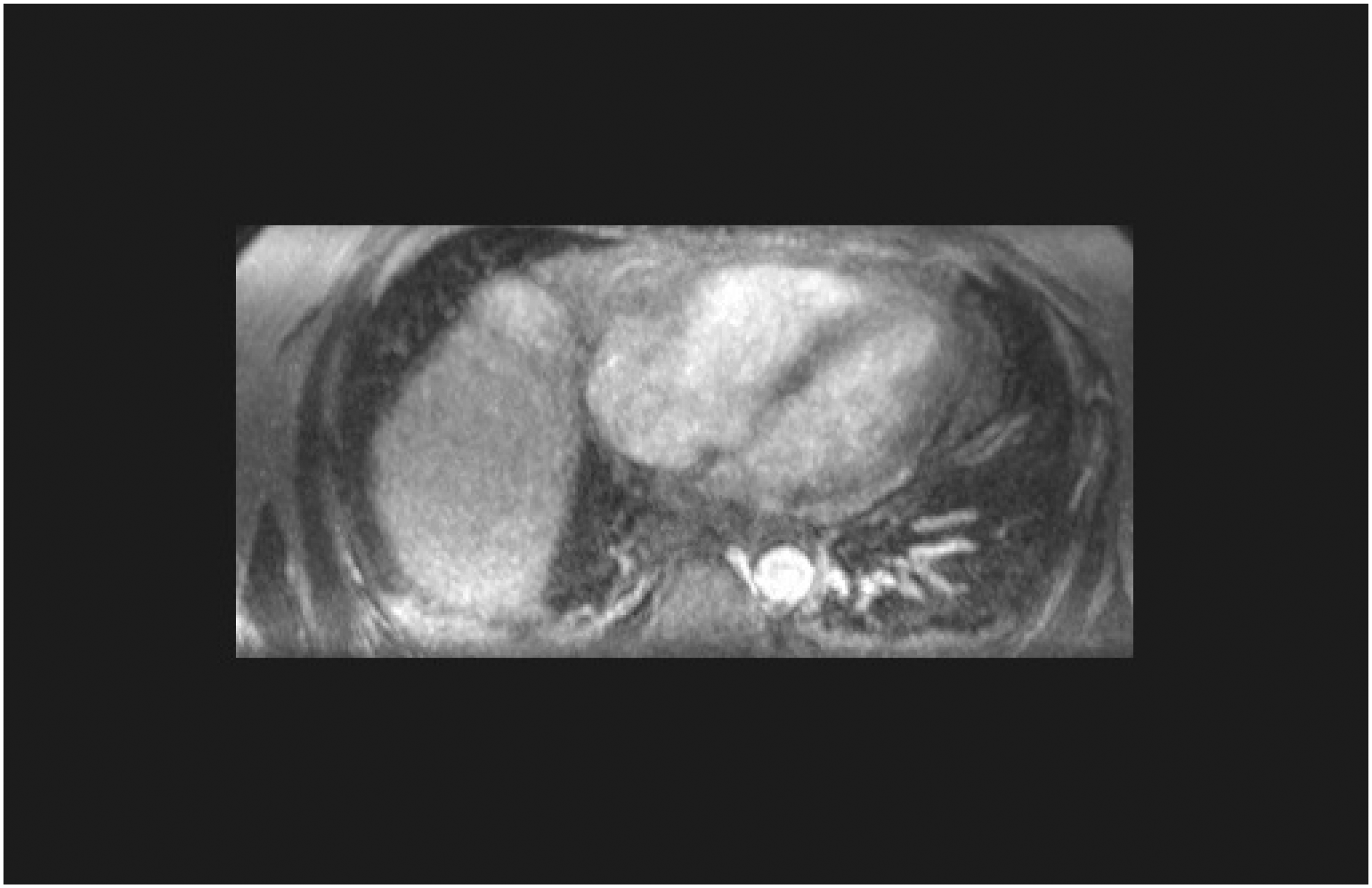
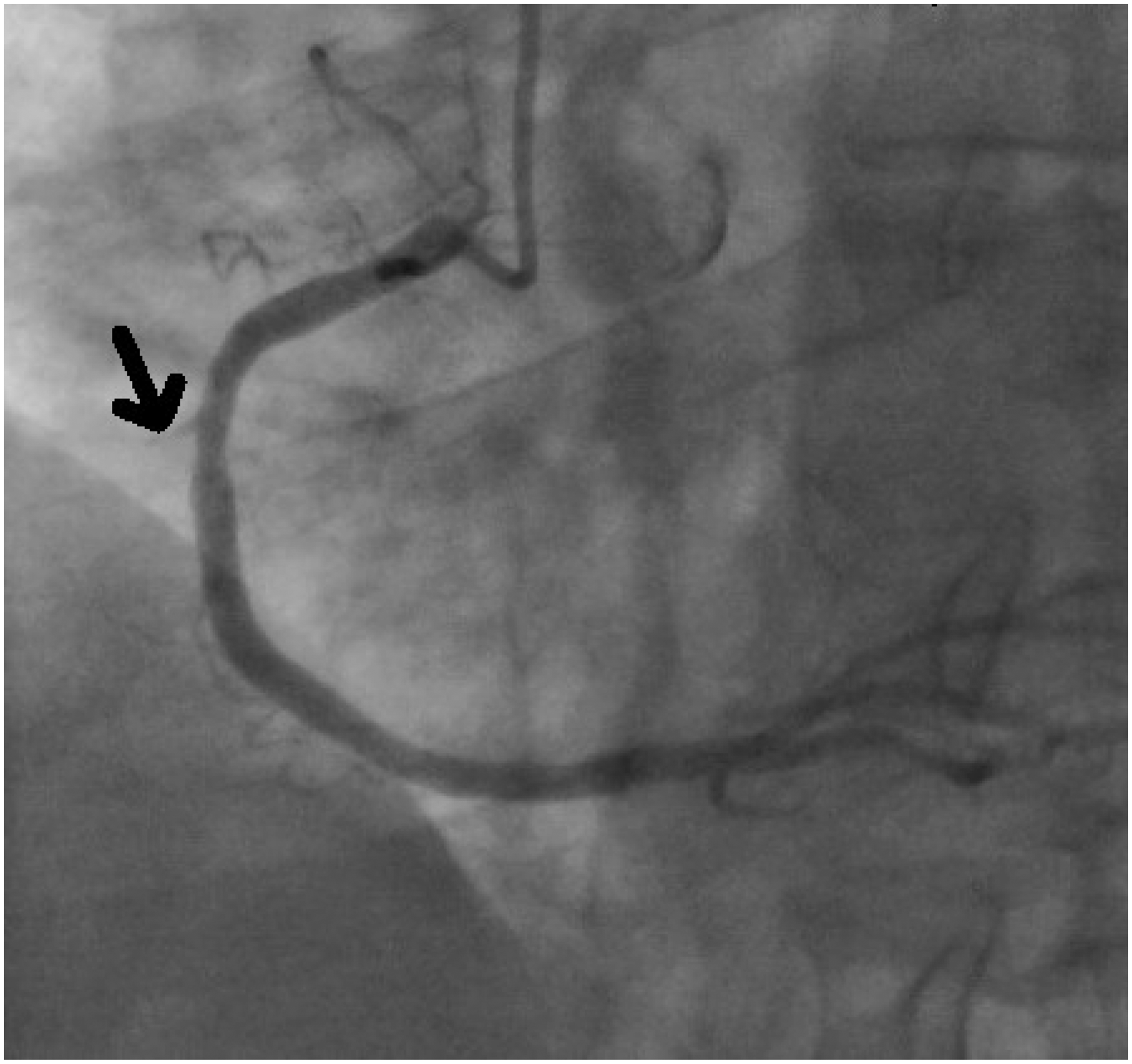
Echocardiogram on Day 2 showed normal left ventricular systolic function with left ventricular ejection fraction (LVEF) of 50%–55%, mildly decreased RV systolic function with RV enlargement. A hinge point was noted at the RV apex suggesting some wall motion abnormality. Both saline contrast bubble study and Definity study showed no obvious ventricular leak; there was also no evidence of pericardial effusion (Figure 2). Cardiac magnetic resonance imaging on the same day revealed mildly decreased right ventricular ejection fraction of 44.3%. Otherwise the right ventricle appeared normal with no wall motion abnormality to suggest myocardial ischemia, no evidence of aneurysm and no delayed hyperenhancement. The pericardium and mediastinum were unremarkable apart from some subcutaneous bruising and fluid surrounding the sternal fracture (Figure 3). Based on these findings of decreased RV function, the patient underwent a coronary angiogram, which revealed 100% occlusion of the proximal RV marginal branch and mild coronary atherosclerosis without obstructive coronary artery disease, including a 50% mid-left anterior descending coronary artery (LAD) lesion (Figure 4). No intervention was indicated given that onset of event was > 12 h from presentation, branch vessel appeared to be < 2.5 mm, and the patient was hemodynamically stable and asymptomatic.
Echocardiogram on hospital Day 2 revealed normal left ventricular systolic function with LVEF of 50%–55% and mildly decreased right ventricular (RV) systolic function with RV enlargement. A hinge point was noted at RV apex suggesting some wall motion abnormality. Both bubble study and Definity study showed no obvious ventricular leak and no evidence of pericardial effusion. Cardiac MRI revealed mildly decreased right ventricular ejection fraction of 44.3%. Otherwise the right ventricle appeared normal with no convincing evidence of dysmotility to suggest a myocardial contusion. There was no evidence of aneurysm and no delayed hyperenhancement. The pericardium and mediastinum were unremarkable, apart from some subcutaneous bruising and fluid surrounding the sternal fracture. Coronary artery angiogram revealed a 100% occlusion of the proximal RV marginal branch (black arrow) and mild coronary atherosclerosis without obstructive coronary artery disease, including a 50% mid-LAD lesion. The RV marginal branch appeared to be < 2.5 mm.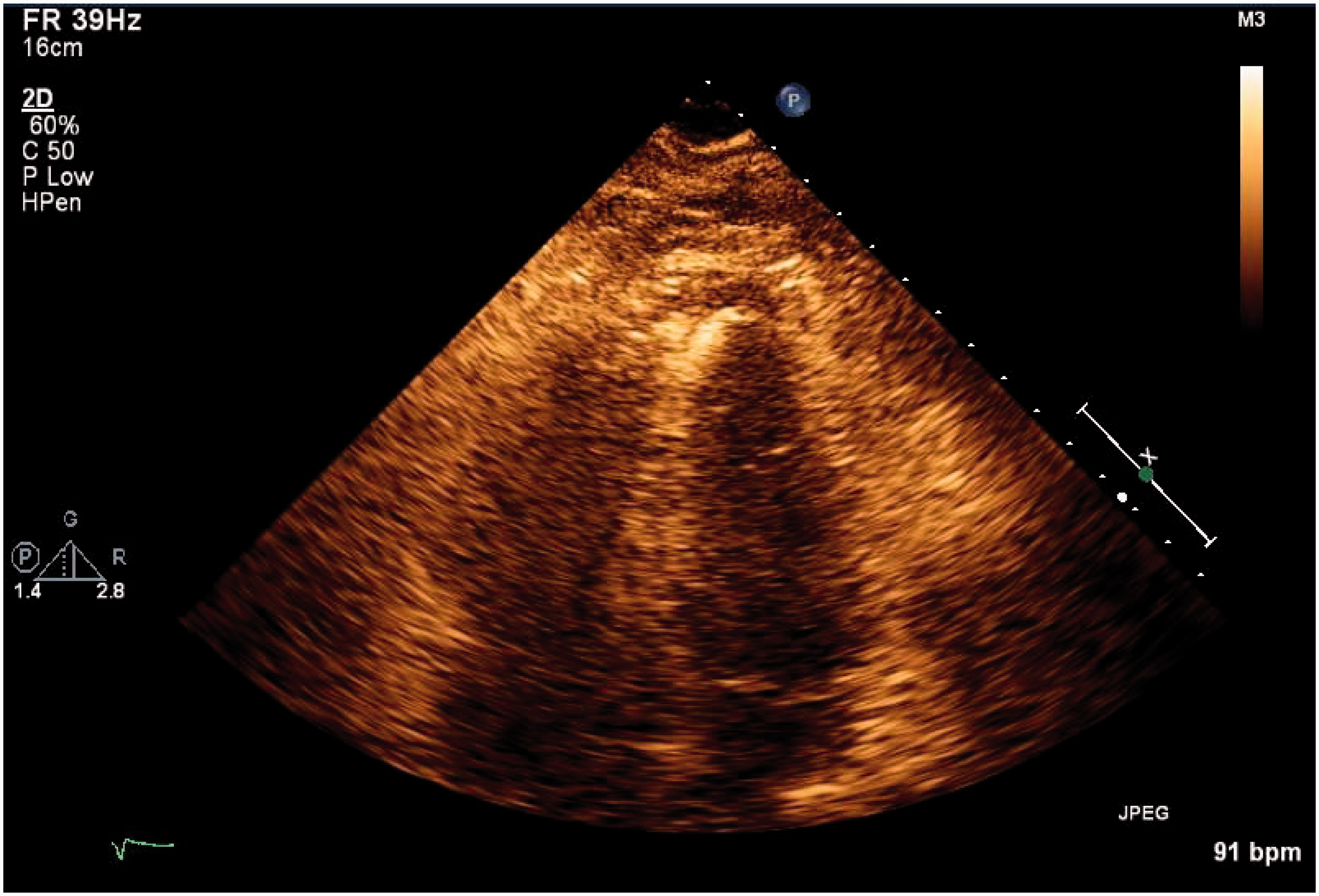
Cardiology consultants recommended lisinopril, metoprolol, aspirin and atorvastatin for prevention until further followup with his cardiologist. He was transferred from the intensive care unit to the floor in stable condition and continued to require physical therapy (PT). He was able to ambulate with PT and his pain was controlled with oral pain medication, and therefore, he was discharged on hospital Day 6.
Since discharge, the patient has been doing well with systolic blood pressure of 110–120 mmHg at home. He is making improvements with physiotherapy and is able to walk around a block and climb stairs without any cardiovascular limitations. He reports occasional cough and chest congestion but no fever. He also denies any shortness of breath, chest pain, lower extremity edema, orthopnea, paroxysmal nocturnal dyspnea, dizziness or lightheadedness.
Discussion
Coronary artery injury in a BCT is a rare complication accounting for only 3% of BCI cases. 2 Clinically significant cardiac injury occurs in approximately 5%–15% of patients with severe BCT. 4 The most commonly affected vessel in BCT is the LAD in 71.4% of the cases, 1 likely due to the vulnerable anatomic position in the anterior portion of the heart,1,4 followed by the right coronary artery in 19% of the cases most vulnerable at its origin perhaps due to acceleration/deceleration injury, followed by the left main artery in 6.4% of the cases and the left circumflex artery in 3.2%. 1
Mechanisms of BCI include1,5:
Direct precordial impact Crush injury resulting from compression Deceleration or torsion causing a tear in the heart at a point of fixation Hydraulic effect resulting in rupture, such as that seen during an abrupt abdominal compression that results in significantly elevated venous pressure that is transmitted to the right atrium or ventricle Blast injury.
Trauma leading to coronary artery damage and myocardial infarction after blunt trauma includes intimal tear, dissection, rupture of an existing plaque, spasm, vessel rupture and external compression from epicardial hematoma. 1
The most common finding associated with BCI is chest pain, 2 but this pain is often associated with thoracic trauma and not angina which makes the diagnosis of myocardial ischemia in BCI difficult for emergency physicians. Other clinical findings like thrill, murmur, rub or hemodynamic compromise should be considered when making the diagnosis of BCI. 4 In our patient’s case, RV marginal artery occlusion could theoretically have led to some degree of right heart failure. Fortunately for this patient, RV function was overall preserved. If he had developed RV failure, the most appropriate treatment is support with diuretics to promote euvolemia and forward flow. The data supports the use of electrocardiography and cardiac enzymes in the diagnosis of clinically significant cardiac complications after blunt cardiac trauma. 6 The electrocardiogram is useful to identify abnormalities including sinus tachycardia, bradycardia, conduction delays or atrial or ventricular arrhythmias which may be present in BCI. ECG changes are usually present at the time of admission or may be detected within the first 24 h after injury. Hence, at least a 24-h period of observation and ECG telemetry should be employed in patients suspected of having BCI. 2 The combination of ECG and cardiac troponin identifies reliably the presence or absence of significant BCI. Patients with an abnormal ECG and troponins need close monitoring for at least 24 h. 7
Echocardiography assists in the diagnosis of non-cardiac injuries, including aortic rupture, intracardiac thrombi, pericardial effusion and pleural effusion which can be associated with BCI.8,9 There are different therapeutic approaches for treating acute myocardial infarction after blunt thoracic trauma. Percutaneous angioplasty with or without stent placement is the most utilized therapeutic choice and has excellent results in terms of vessel revascularization and reversal of ST segment disorders. In cases of severe bleeding, coronary bypass is indicated. 10
Conclusion
Coronary artery occlusion is a rare but potentially fatal complication of BCT. The patient’s only complaint could be chest pain, which can be due to chest wall trauma and not angina. This makes the differentiation of the diagnosis of myocardial infarction from coronary artery occlusion difficult. ECG changes and cardiac enzyme elevation are very important markers for BCI but sometimes can be delayed for up to 24 h after injury. Echocardiography is also very useful to assess cardiac function. The most utilized treatment of choice is percutaneous angioplasty with or without stent placement. This report emphasizes the importance of proper evaluation, early diagnosis and prompt intervention in a case of BCI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.