
Abstract

A 13-year-old boy, with a history of full-thickness corneal laceration of the left eye caused by a knife 10 weeks earlier, presented to the eye clinic for a follow-up visit. Primary closure had been performed after the trauma and three weeks after the original injury, the patient developed a traumatic cataract and underwent surgical lens removal. Intraocular correction of the removed lens was deferred at the time of lensectomy due to the traumatic nature of cataract. Following lens removal, there was an increase in intraocular pressures, which was successfully treated with medications.
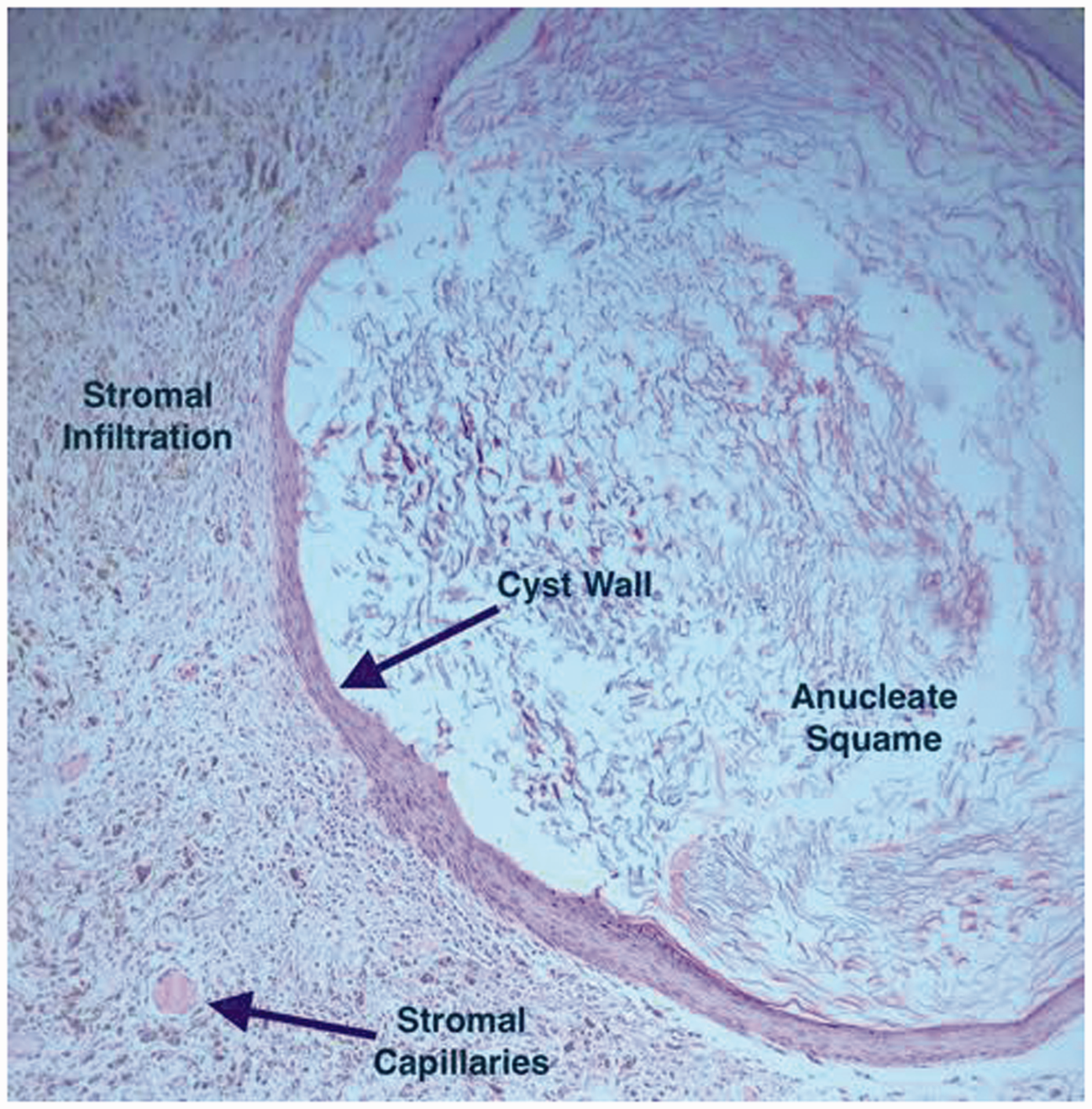
At this presentation, a translucent cystic lesion of the iris at 11 o’clock was present and there was fluffy white material in the anterior chamber of the left eye (Figure 1). Best corrected visual acuity was 20/200 in the affected eye and intraocular pressure was normal. The presentation was consistent with an inclusion cyst secondary to implantation of the skin tissue into the iris which is a highly vascular environment that promotes cell proliferation. There was also significant amount of keratin material floating freely in the anterior chamber. Sectoral iridectomy was performed and the cyst and keratin material were removed. Histopathological exam confirmed the diagnosis (Figure 2). The external layer of the cyst was formed with dermal stroma and basement membrane of the epithelial lining and the central core was filled with degenerated epithelial cells and keratinous squame. The management of iris inclusion cysts is challenging due to high risk of recurrence and several treatment approaches such as needle aspiration, endolaser photocoagulation, cryotherapy, local excision and en bloc resection have been proposed.
1
The cyst did not recur within a 6-month follow-up period.
Patient’s left eye. Pearl cyst of the iris, traumatic scar and free-floating white material are indicated by arrows. Histopathological examination showing hypervascularity and pericystic infiltration of iris stroma predominantly with mononuclear lymphocytes and segmented neutrophils compatible with foreign body reaction to the inclusion cyst. The cyst wall consists of layers of epithelial cells and the central core is filled with degenerated cells.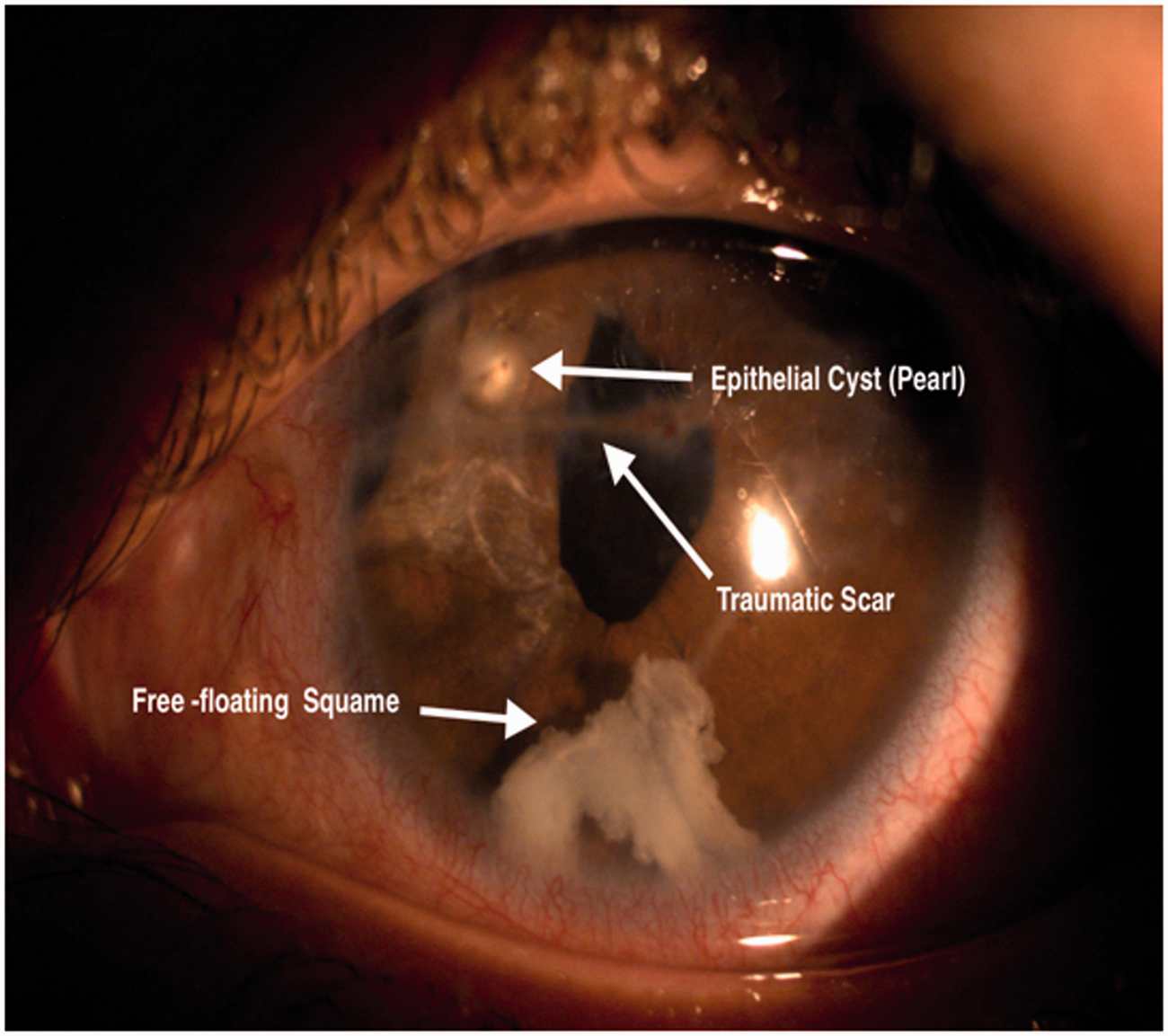
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.