
Abstract
Background
Retained intraocular foreign body (IOFB) is a specific subgroup of open globe injury which is often preventable with appropriate use of eye protection. We describe the spectrum of injuries resulting in IOFB, outcomes and complications following vitrectomy surgery and context specific risk factors which may influence outcomes at our hospital.
Methods
Retrospective cohort study of 43 consecutive cases of IOFB that underwent vitrectomy surgery.
Results
The median age was 34.6 years and 95.3% were male. The presenting visual acuities ranged from 6/6 (LogMAR 0.00) to Perception of Light (PL) with a median of Hand Motions (HM) (Interquartile Range (IQR) 6/24-HM). Hammering metal was the most common cause of injury (44.2%); 72% of injuries occurred while performing premeditated high-risk activities. The foreign body was metallic in 76.7% of cases and penetrated the cornea in 69.8% of cases. Lens injury occurred in 65.1%. The retina was impacted in 36 cases (83.7%), four of which impacted the macula. Macula impact was associated with poor visual outcome (p = 0.049, Fisher’s exact). Four cases (9.3%) had endophthalmitis. The median final visual acuity was 6/24 (IQR 6/9–6/60). Visual acuity improved in 63.4.0%. Ten cases (23.8%) were worse than 3/60. Better presenting vision was associated with better visual outcomes (p = 0.049, Fisher’s exact). The Ocular Trauma Score predicted outcomes well in better prognosis categories but underestimated final visual outcomes in the poor prognosis category. Central corneal scarring contributed to reduced visual outcomes.
Conclusion
The majority of IOFB injuries are preventable with appropriate use of eye protection. Visual outcomes are better than other causes of open globe injury. Resource constraints contribute to suboptimal final visual outcomes.
Background
Open globe injuries account for 63.7% of eye injuries presenting to the ophthalmology unit at Groote Schuur hospital. 1 Physical assault is the commonest cause accounting for 73.5% of cases and visual outcomes are often poor. All eyes undergo primary repair where possible but in most cases secondary procedures such as vitrectomy are not performed because of poor prognosis, the presence of good vision in the other eye and resource constraints. In a recent review, 79% of these eyes ended up blind (visual acuity less than Snellen 3/60) and only 12.6% obtained better than Snellen 6/12. 1
Open globe injuries with retained intraocular foreign body (IOFB) are a specific subgroup of open eye injury categorised independently in accepted eye trauma classification systems. 2 They frequently occur during occupational or recreational activities and are usually preventable with the use of appropriate protective eye wear. It is recognised that the visual prognosis of these injuries is potentially better than other causes of open eye trauma. The small fragment frequently causes localised damage to the eye structures and if the central macula is unaffected, these eyes may regain good visual function. The foreign material is usually removed by vitrectomy to reduce risks of infection, on-going inflammation and toxicity. Reconstructive surgery for best possible visual outcome (e.g. corneal transplantation to remove corneal scarring) may be limited by resource constraints. We reviewed the cases of posterior IOFB treated with vitrectomy surgery in our unit with the aim of describing the spectrum of injuries resulting in IOFB, the nature of the foreign material and the visual outcomes and complications following vitrectomy surgery. We also aimed to identify independent factors which may be associated with final visual outcomes and the effect of limited resources for corneal transplantation. We are not aware of any publications of this type from Southern Africa.
Methods
We conducted a retrospective cohort study of consecutive patients undergoing vitrectomy surgery to remove retained intraocular foreign material between February 2007 and June 2015. Cases were identified using the hospital ICD10 coding system as well as surgical log books of vitreoretinal consultants.
At presentation, the mechanism of injury was recorded. Visual acuity was measured using a Snellen chart or determination of Counting Fingers (CF), Hand Motions (HM) or Perception of Light (PL) if the Snellen chart could not be seen. All visual acuities were converted to LogMAR format for statistical analysis. An arbitrary LogMAR of 4 was assigned to PL vision and 5 for No Perception of Light (NPL). Vision of PL and NPL were excluded from the calculation of median visual acuity but were included in categorical analyses. 3
All eyes received a thorough slit-lamp examination and documentation of extent of injury. Lens injury was defined as visible injury to the capsule or lens on slit-lamp examination. The Ocular Trauma Score (OTS) 4 was determined for each eye using visual acuity and the presence of a relative afferent pupil defect, retinal detachment or endophthalmitis. This assigned each patient to Categories 1 (poor prognosis) to 5 (good prognosis) and predicted likely visual outcomes. The entry site of the foreign material was categorised according to recognised trauma terminology.
On suspicion of retained foreign material, all patients underwent a CT scan to confirm the diagnosis and localise the foreign material within the eye (Figure 1). All patients received systemic prophylactic antibiotics consisting of oral ciprofloxacin 750 mg b.d. and intravenous cefazolin 1 g t.d.s. for three days. Patients who had clinical endophthalmitis (hypopyon or severe vitritis) at initial presentation had vitreous sampling for microscopy and culture and received intravitreal vancomycin 1 mg and ceftazidime 2 mg at the time of primary repair.
CT scan demonstrating metallic IOFB in the left eye.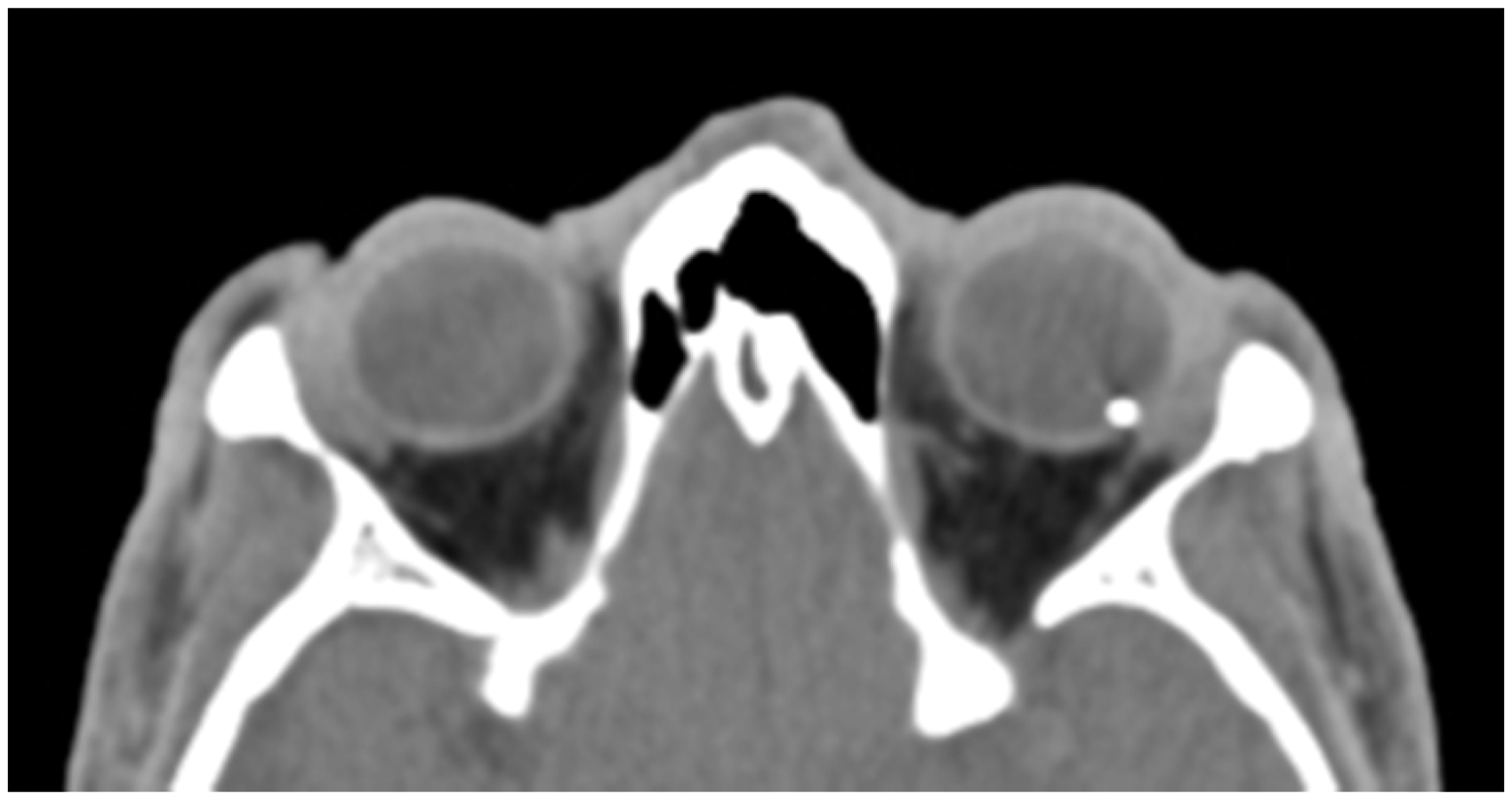
Informed consent for surgery was obtained from all patients. All surgery was performed under general anaesthesia. Where possible, a vitrectomy to remove the foreign material was performed at the time of primary repair. Alternatively patients underwent primary repair alone, with intraocular antibiotics if clinical endophthalmitis was diagnosed. A vitrectomy was performed a few days later to remove the foreign material and manage the associated intraocular injuries.
Injuries to the lens necessitated lens removal, with or without placement of an artificial lens at the same procedure. All vitrectomies were performed by vitreo-retinal consultants operating under the Eibos® wide-angled viewing system. If the lens had been removed, the foreign material was most frequently extracted through the anterior chamber via a limbal incision (see video). If the lens was preserved, then the material was removed through a sclerotomy in the pars plana. Retinal injuries or detachments were treated appropriately with laser retinopexy and intraocular tamponade. Foreign material recovered from the eye was sealed in an envelope for possible future medico-legal proceedings.
Patients were discharged on dexamethasone/chloramphenicol topical treatment and systemic anti-inflammatory treatment. Follow-up was conducted at Groote Schuur hospital eye outpatients or by the referring doctor for patients from rural areas. The study was approved by the Human Research Ethics Department of the University of Cape Town (HREC REF: 666/2015).
All data were collected in Epidata® and transferred to STATA 12 5 for analysis. The Fisher’s exact test was used to analyse categorical variables. Wilcoxon rank-sum test was used to compare medians. A p-value of less than 0.05 was considered statistically significant.
Results
We reviewed 43 consecutive cases of ocular trauma with retained foreign material between February 2007 and June 2015. Forty-one patients (95.3%) were male. The median age was 34.6 years (range 7 years–60 years), and the right eye was involved in 23 cases (53.5%). The presenting and final visual acuities are shown in (Figure 2).
Distributions of visual acuity at presentation and final follow-up. CF: counting fingers; HM: hand motions; PL: perception of light; NPL: no perception of light.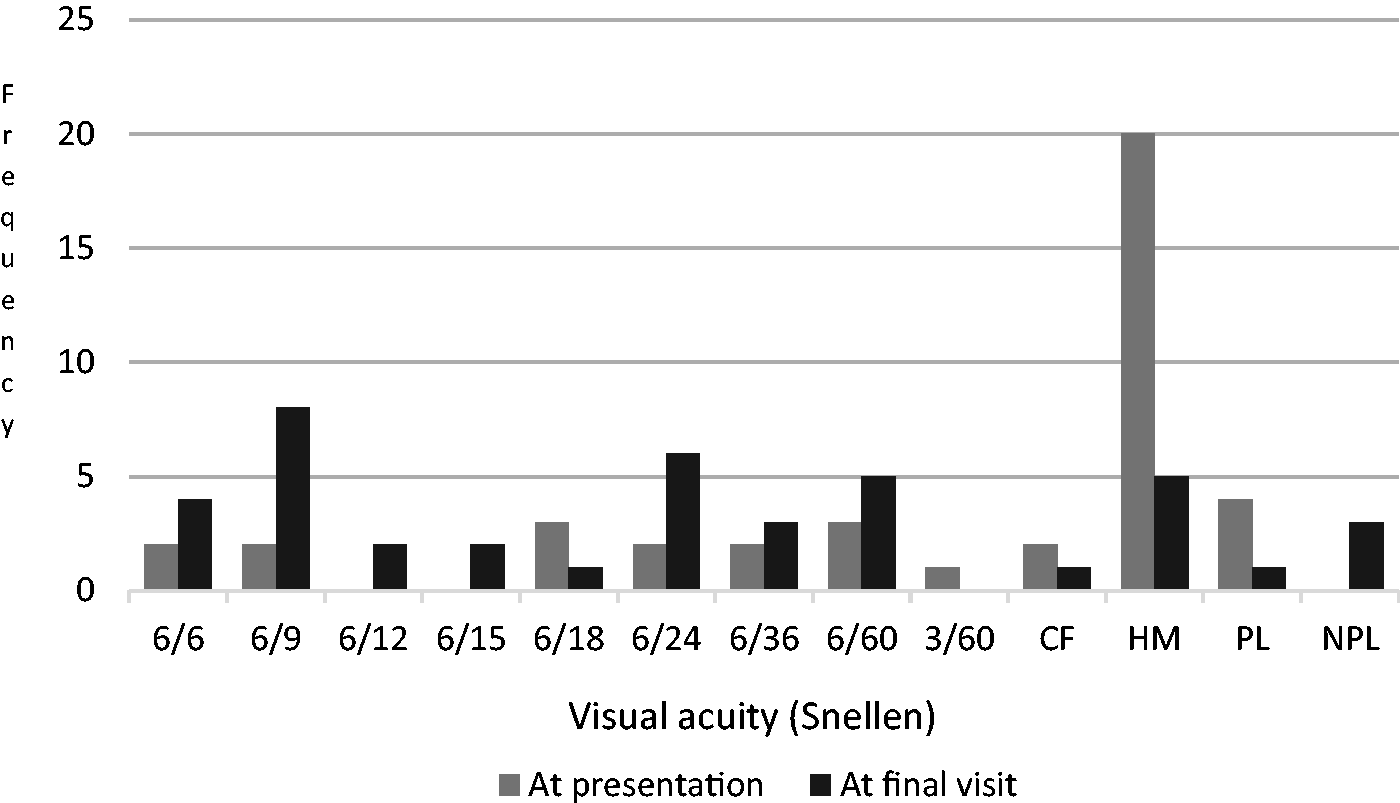
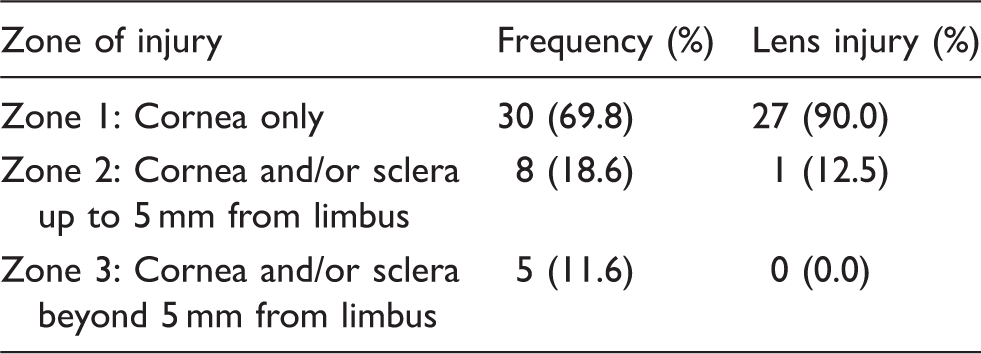
Entry site and lens injury.
The mean OTS Category was 3.2. Four cases (9.3%) had clinical endophthalmitis at initial presentation.
The most common mechanism of injury was hammering which accounted for 19 cases (44.2%). A total of 31 cases (72.1%) occurred in an environment where protective eye wear should have been used, e.g. using a hammer, grinder, nail gun or jack-hammer. No patients reported using protective eye wear at the time of the injury. Interpersonal violence was responsible for seven cases (16.3%). Five patients (11.6%) were unsure of the origin of the foreign body or suffered other accidental injuries, e.g. shattered light bulb.
The median time from injury to first procedure was three days (range: same day to 509 days). This delay was most commonly a result of late presentation and delayed access to busy emergency theatres. In eight patients (18.6%), the delay from injury to surgery was 10 or more days. Of these, two patients were initially misdiagnosed with uveitis, five had delayed presentation and one patient initially absconded and returned later; 29 eyes (67.4%) had removal of the foreign body at the first procedure; 14 (32.6%) had primary repair followed by vitrectomy to remove the foreign material. The mean time to second procedure was 3.7 days following primary repair.
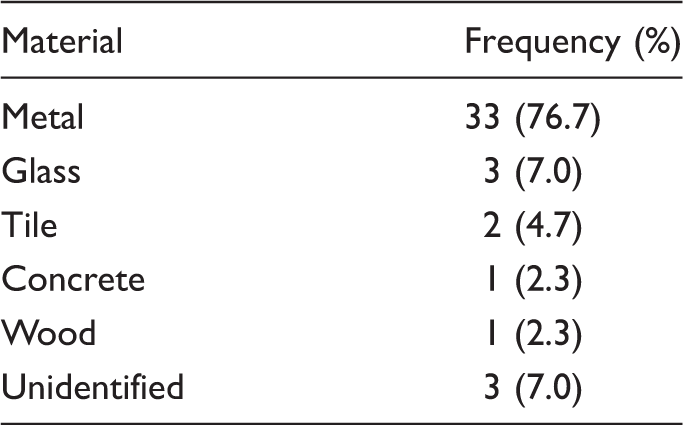
Nature of foreign material.
Tamponading agent.
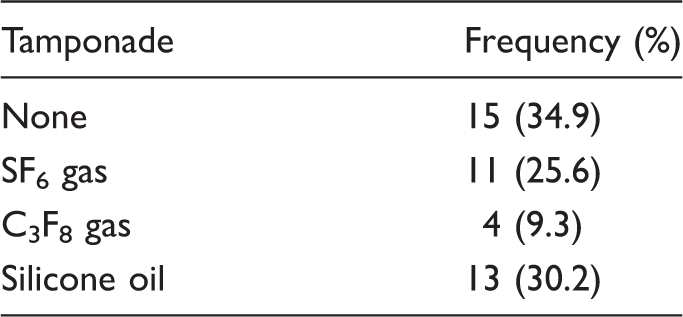
Follow-up data were available in 41 cases. The median follow-up period was 5.1 months (range 1 week–6.4 years). Six cases (14.3%) developed retinal detachments, five cases (83.3%) of which resulted in poor visual outcomes; 13 cases (31.7%) underwent further rehabilitative surgery to remove the silicone oil, remove corneal sutures and insert secondary intraocular lenses. Of the 13 cases with silicone oil tamponade, 8 (61.5%) had removal of oil by the end of the study. The mean time to removal of silicone oil was 6.9 months (range 2.1–11.7 months); 9 (22.0%) retained their natural lens at the end of follow-up, 15 (36.6%) were pseudophakic and 19 (46.3%) were aphakic. Of the aphakic patients, 9 (47.4%) improved with optical correction. Final visual outcomes are shown in Figure 2, and change in visual acuity is shown in Figure 3.
Change in visual acuity (logarithmic scale). CF: counting fingers; HM: hand motions; PL: perception of light; NPL: no perception of light.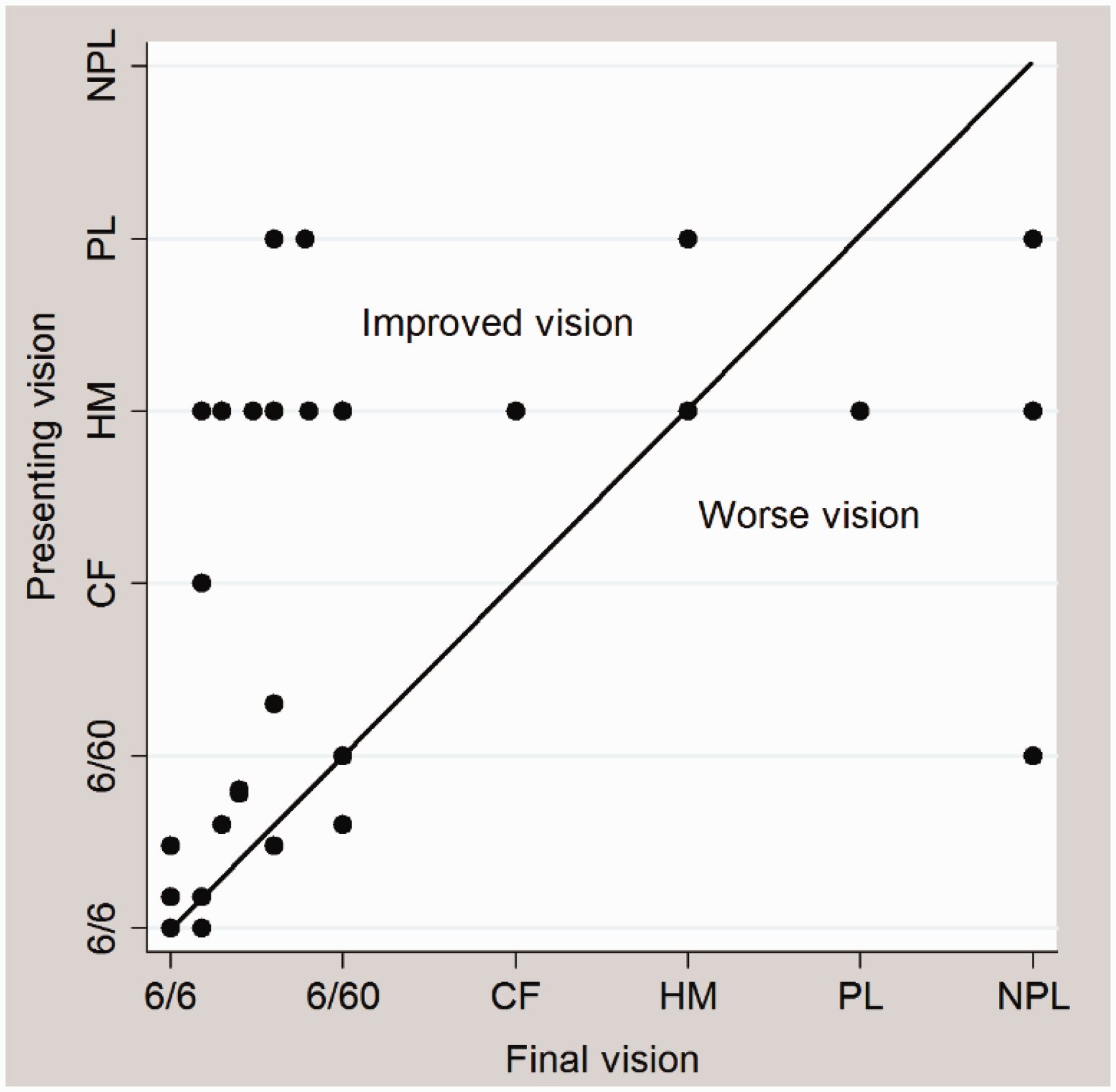
Excluding PL and NPL outcomes (four cases), the median final visual acuity was 6/24 (IQR 6/9-6/60). In patients with follow-up of longer than one month (n = 31), the median final acuity was 6/18 (IQR 6/9-6/48). Overall, 25 cases (61.0%) improved over the follow-up period. Better presenting visual acuity was associated with improved final visual outcome (p = 0.049 Fisher’s exact); 16 (39.0%) had central corneal scarring which was felt to contribute to reduced vision at the end of follow-up. Hammering injuries did not have a significantly different outcome to non-hammering injuries (p = 0.77, Wilcoxon rank-sum). Macular impact resulted in a poor outcome, with three of the four cases achieving less than Snellen 3/60 (p = 0.049, Fisher’s exact). Three of the four endophthalmitis cases achieved better than Snellen 6/60. Patients in the primary removal group had a better median final acuity (Snellen 6/15, IQR 6/9-6/48) than those who had a delayed vitrectomy (Snellen 6/24, IQR 6/18-HM) (p = 0.14, Wilcoxon rank-sum test). However, there were more patients (n = 3) with PL or worse vision in the primary removal group than the delayed vitrectomy group (n = 1).
Seven eyes (17.1%) were blind (Snellen < 3/60) at the end of follow-up. Three had macular impact injuries and four developed poor prognosis retinal detachments. A further three cases had poor vision when last seen but were lost to follow-up early with gas or silicone oil in situ and may have improved on longer follow-up.
The OTS accurately predicted good visual outcomes in those patients with a Category 5 OTS (favourable features) and was reasonably accurate in the Categories 4 and 3. In Category 2 (worst prognosis), visual outcomes were better than expected (See Figure 4).
Predicted and final visual outcomes by presenting OTS category. CF: counting fingers; HM: hand motions; PL: perception of light; NPL: no perception of light; OTS: ocular trauma score.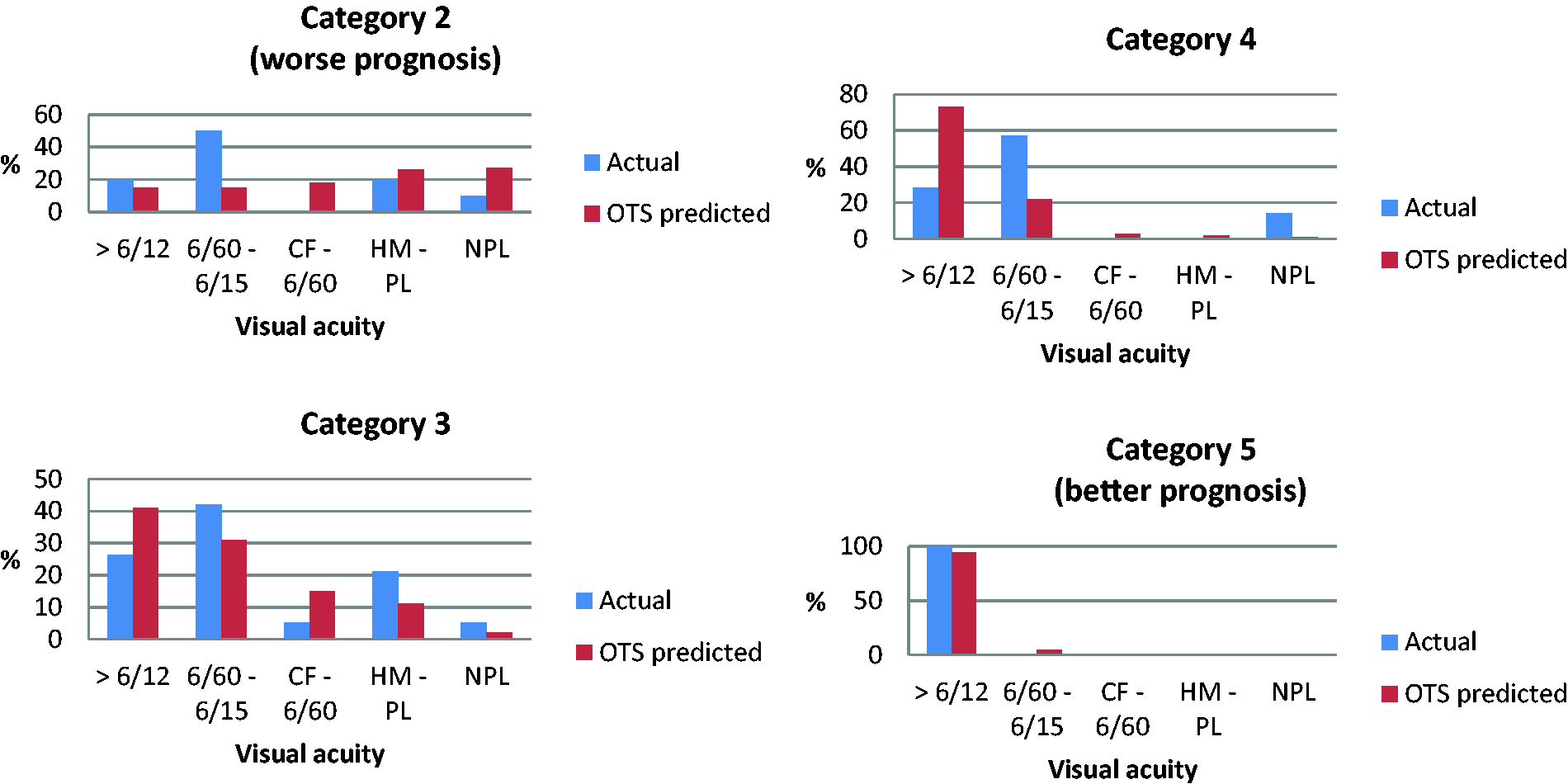
Discussion
This study highlights that open globe injuries with retained intraocular foreign material are potentially preventable in the majority of cases with the appropriate use of protective eye wear; 72% of cases occurred whilst performing a premeditated high-risk activity where protective eye wear should have been used. No patients reported using protective eye wear.
Intraocular foreign bodies contribute only 2% of open globe injuries presenting to our hospital in contrast to international reports of around 28%. 6 This reflects the high rate of interpersonal violence which accounts for 73.5% of open globe injuries in our unit 1 and which infrequently causes IOFB. Seven cases (16.3%) of IOFBs were caused by interpersonal violence in this series. The most common cause of IOFB was hammering metal (44.2%) which is consistent with other reports.6–8 A further 27.9% of our cases occurred while grinding, using a nail gun or jack-hammer. The most common foreign material was metallic (76.7%) which is a similar finding to others.6,7
The overall prognosis in the eyes with IOFB is considerably better than other open globe injuries presenting to our unit. In a recent review, 79% of open globe injuries from other causes ended up blind (Snellen < 3/60) and only 12.6% achieve Snellen 6/12 or better. 1 In our series of IOFB cases, seven eyes (17.1%) were blind at the end of follow-up (Snellen < 3/60) while 63.4% improved (Figure 3) and 34.2% achieved Snellen 6/12 or better. This compares favourably with other IOFB reports7,8 and is slightly better than a large series of 1421 eyes where 54.3% improved. 6
Sixty-one percent (25 cases) were judged to have visually significant corneal scarring. Further visual improvement may have been possible in 16 of these cases (64.0%) in a setting of unlimited corneal transplant resources. Resource constraints prevent corneal transplantation in the majority of cases, particularly if the other eye has normal vision. This does, however, negatively impact the final visual outcomes of our study. The remaining nine cases were unlikely to improve with corneal surgery because of the associated ocular injuries.
Other reports agree with ours that hammering is the commonest cause of IOFB.6,7 A series of 64 hammering injuries was reported by Valmaggia et al. 9 They describe exceptionally good outcomes in this subgroup with 82.8% of cases achieving Snellen 6/12 or better and the mean acuity of Snellen 6/12. They highlighted macular impact as the main poor prognostic factor. In our subgroup of 18 hammering-related injuries, the median final acuity was Snellen 6/24 (IQR 6/12-6/60). Two of these cases had macular impact and poor final acuities of CF and Snellen 6/60 respectively; 14 of the 18 cases had significant corneal scarring which we feel contributed to the poorer outcomes in our patients. We note with interest that the mean final acuity in the series by Valmaggia et al. 9 was obtained without any corneal transplantation.
The other clinical characteristics of our patients were similar to those reported in the literature. Entry sites were mainly corneal (69.8%)6,8 with a high rate of traumatic cataract (65.1%)6,10 A direct retinal injury occurred in 83.7%. Understandably, retinal impact at the macula results in a poorer visual prognosis. 9 Three of the four patients in our series with macular impact achieved less than Snellen 3/60 which was statistically significant (p = 0.049, Fisher’s exact). Ten eyes (24.4%) were less than Snellen 6/60 at the end of follow-up which is similar to the rate of 25% reported by United States Eye Injury Registry. 11 Seven eyes (17.1%) were less than Snellen 3/60. Others report less than Snellen 3/60 in 24% 7 and less than Snellen 1/60 in 50%. 6
Other factors associated with poor outcomes include poor presenting visual acuity, secondary infection (endophthalmitis), the presence of a relative afferent pupil defect and retinal detachment.6,7 Reported rates of endophthalmitis associated with these injuries vary from 0% to 16%.6,8,12 A large review of 1421 cases 6 found a lower rate of endophthalmitis, if primary repair of the entry wound was performed within 24 h. The median time from injury to primary repair in our study was three days and only 13 cases (30.2%) had primary repair within 24 hours. Reasons for this include a lack of private transport among poorer communities, delayed referral from community clinics and busy emergency theatres which serve all disciplines at Groote Schuur hospital. Four cases (9.3%) had clinical endophthalmitis at initial presentation in our series. This occurred in one case despite timeously referral and primary repair within 24 h. The other three cases presented between two and four days after injury. Where possible, improving patients’ access to care and streamlining access to emergency theatre may therefore help to reduce the incidence of this complication.
Although some advocate removal of the foreign body within 24 h,9,13,14 others support immediate primary repair and delayed vitrectomy with IOFB removal provided no signs of infection are present. Advantages of delayed vitrectomy include a more stable primary wound, clearer view for surgery, higher chance of vitreous separation from the retina and reduced risk of severe haemorrhage.6,7,12 A number of authors report that a delayed secondary procedure (for up to two weeks) is not associated with worse final visual acuity.6,7 We could not refute this finding. Although patients in the primary removal group had a better median final acuity (Snellen 6/15) than those who had a delayed vitrectomy (Snellen 6/24), this was not statistically significant (p = 0.14, Wilcoxon rank-sum) and there were more patients (three cases) with PL or worse vision in the primary removal group than the delayed vitrectomy group (one case). Selection of worse injuries (e.g. poor view through the cornea) for a delayed procedure may also have skewed these outcomes.
In the post-operative period, the development of a retinal detachment, particularly if associated with fibrosis (proliferative vitreoretinopathy, PVR), is strongly associated with a poor prognosis. The reported incidence of retinal detachment ranges from 10% to 46%7,8,10 and PVR occurs in about 25%. 8 Our retinal detachment rate was consistent with this. Six (14.6%) cases developed retinal detachments. However, five of these (83.3%) developed PVR with a poor outcome.
Baseline visual acuity and classification with the OTS have been used to predict final outcomes. 9 Better visual acuity at presentation is associated with better outcomes in some series6,8,14 and we showed similar results (p = 0.049, Fisher’s exact test). Of note is that injuries to the lens can produce profound visual loss which is imminently reversible. In our series, 21 of the 24 cases presenting with HM vision or worse had lens injuries, 14 (66.7%) of which improved with treatment. This may explain why final visual outcomes were better than predicted by the OTS. We found that 70% of Category 2 (severe injury) patients achieved Snellen 6/60 or better, where the OTS predicted only 30% would achieve this acuity. A similar finding was reported by Szijártó et al. 8
Limitations of our study include its retrospective nature and limited follow-up (less than one month) in 10 cases (24.4%). Most of these patients lived in rural areas and follow-up data were difficult to obtain. Some of these cases are likely to have improved as gas resorbed after surgery (two cases), silicone oil was removed (two cases) or with further lens implantation (six cases). However, complications such as retinal detachment may also have remained undocumented. The limited number of patients reduced the power of the study.
Conclusion
The preventable nature of the majority of these injuries with appropriate implementation of eye protection cannot be over emphasised. This study provides evidence and motivation for improved education regarding eye safety in all activities with potential for eye injury, whether in industry or recreational. With the use of modern vitreoretinal techniques, we achieved outcomes in keeping with international reports. Further improvements may be possible with improved resources.
Access to data
Data used in this study may be available from the corresponding author on request.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.