
Abstract
Trauma point-of-care ultrasound in the form of the Focused Assessment with Sonography for Trauma (FAST) exam and its evolution into extended FAST have significantly enhanced the diagnostic power of evaluation and resuscitation of the trauma patient; however, these modalities still have limitations in evaluating mediastinal and cardiac pathology. This report demonstrates a case of point-of-care transesophageal echocardiography in the diagnosis of blunt thoracic aortic injury in an unstable patient involved in a motor vehicle collision.
Introduction
The miniaturization and portability of point-of-care ultrasound have led to significant change in care for unstable patients in the trauma bay. With the inception of the focused assessment with sonography for trauma (FAST) exam in the early 1990s, 1 and the subsequent evolution into the extended FAST (e-FAST) exam, 2 the presence of hemoperitoneum, hemopericardium, hemothorax, and pneumothorax may all be rapidly diagnosed non-invasively at the bedside using ultrasound. These exams are recommended as adjuncts to the primary survey by the American College of Surgeons in routine advanced trauma life support (ATLS) training programs, 3 and care is routinely influenced by their findings (e.g. a laparotomy should generally be prompted by intraperitoneal free fluid in an unstable patient).
Despite the accuracy, utility, and proven benefit of the e-FAST examination, there are anatomical limitations in its scope. For example, the inability to image the retroperitoneal space for hemorrhage has been noted to be a shortfall of this modality. 2 Blunt thoracic aortic injury (BTAI) and imaging of mediastinal structures in general also remain out of the scope of surface ultrasound techniques that comprise the e-FAST exam. With the adoption of point-of-care transeosphageal echocardiography as a valuable adjunct in both emergency medicine and critical care,4,5 BTAI is amenable to bedside diagnosis if sufficient training and tools are available in a resuscitation environment.
In this case report, we describe the point-of-care diagnosis of BTAI using transesophageal echocardiography (TEE) in a young woman after blunt trauma.
Case history
A 41-year-old female presented to a community hospital emergency department after having been struck by a car at unknown speeds while riding her mobility scooter. She was previously known for a metabolic disorder with associated spastic diplegia, bilateral sensorineural hearing loss, cerebral palsy, strabismus, and a remote L1 burst fracture sustained from a mechanical fall.
Upon initial assessment at the community hospital, she was found to be tachycardic and normotensive. With an initial GCS of 7, she was intubated for airway protection. After performing the primary and secondary surveys, which included a negative FAST exam, a pelvic binder was applied as well as a Sager™ emergency traction splint to the right leg given a clinically obvious femur fracture. The patient was then urgently air transferred to our tertiary care trauma center.
The patient deteriorated during transfer, arriving at our center in shock with a heart rate of 143, a blood pressure of 80/60, though maintaining oxygen saturations of 96% via endotracheal ventilation. Resuscitation with blood products and crystalloid was initiated. Bilateral chest tubes were empirically placed, yielding no significant air or hemothorax. A repeat FAST redemonstrated absence of free fluid in the peritoneum. Chest X-ray revealed a widened mediastinum. Secondary survey did demonstrate multiple abrasions, palpable bony deformities to the inferior orbits bilaterally, as well as swelling and bluish discoloration of the head and neck in a picture resembling SVC obstruction. Given the ongoing shock with narrow pulse pressure despite resuscitation, a point-of-care transesophageal ultrasound probe was inserted to interrogate the mediastinum.
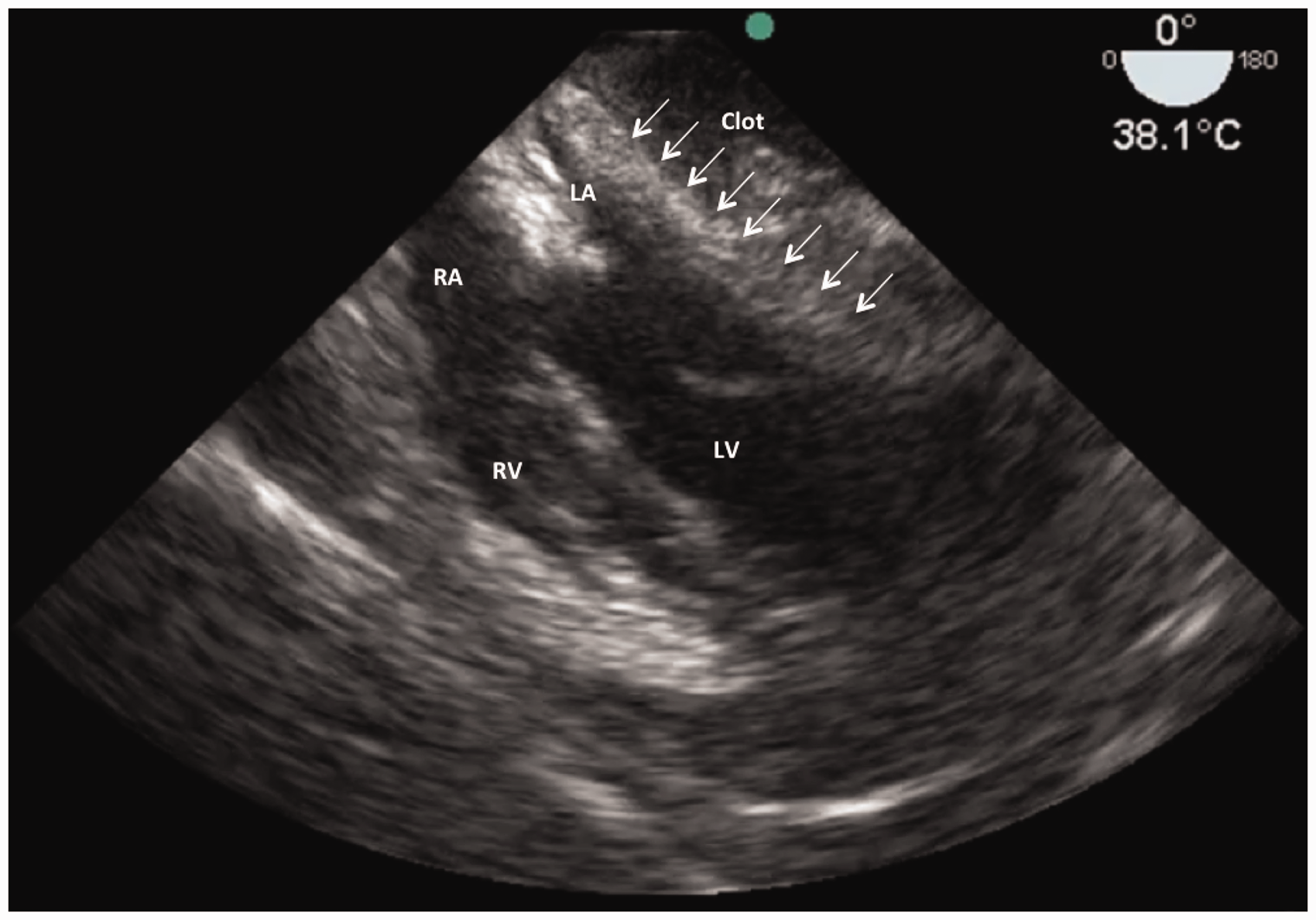
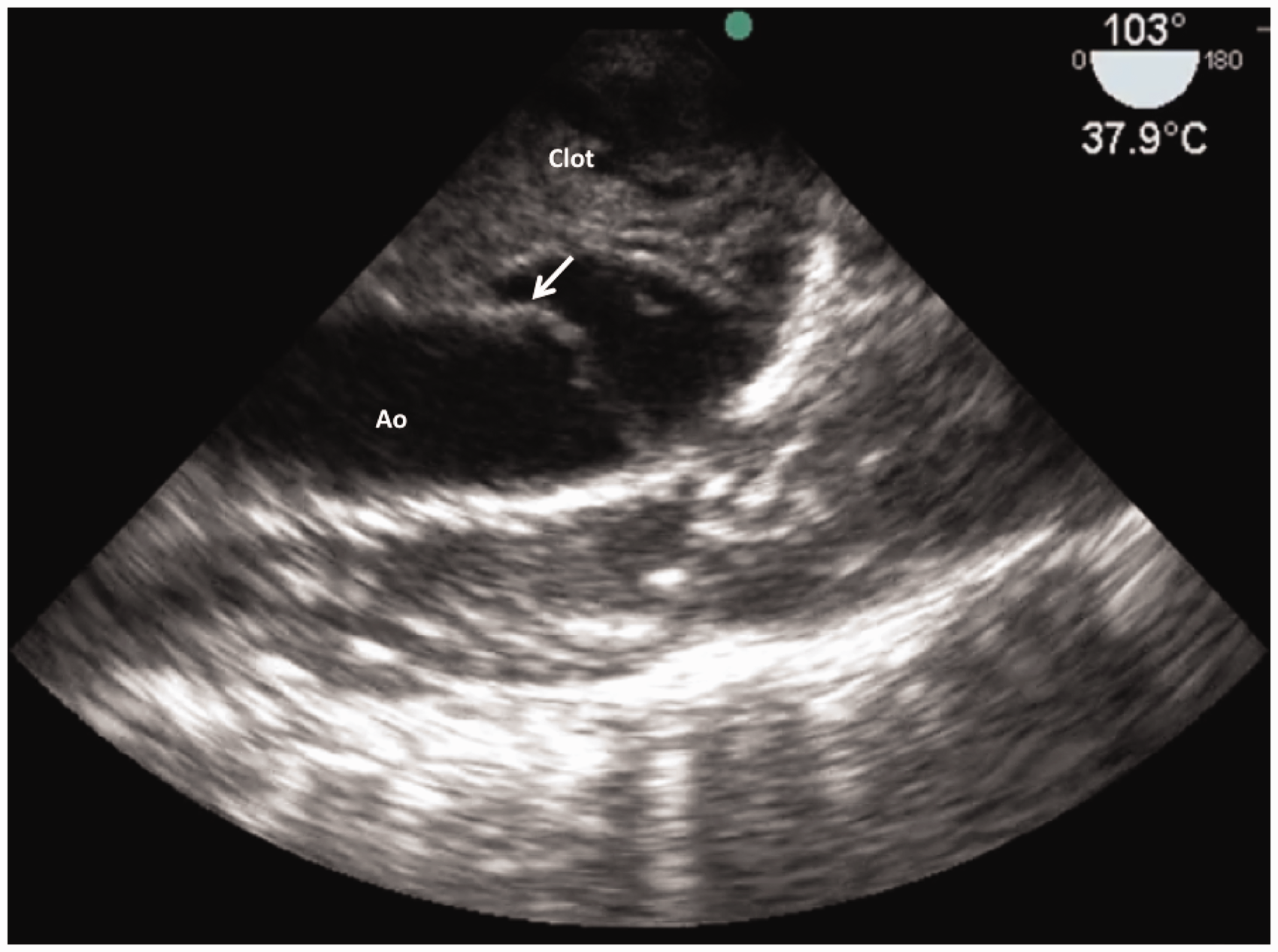
A Sonosite Edge® Ultrasound machine equipped with a transesophageal probe was deployed by the trauma team leader. A goal-directed transesophageal echocardiogram (TEE) was rapidly performed (duration of exam was less than 5 min), simultaneously with other resuscitative efforts. The initial view, a mid-esophageal four-chamber view, of the heart was immediately noted to be abnormal with compression of the left atrium (LA) and left ventricle (LV) from a neighboring, yet unidentified, soft tissue appearing mass (Figure 1). Upon further evaluation, the mass was identified to be hematoma and its compressive effects of the LA and LV were consistent with left-sided, regional tamponade. Importantly, the absence of hemopericardium was noted. Shifting attention to transverse views of the descending thoracic aorta demonstrated a focal disruption at the descending thoracic aorta just distal to the left subclavian artery in keeping with an aortic tear and pseudoaneurysm consistent with BTAI (Figure 2). Reorientation to a longitudinal view confirmed both the location and the extent of this injury in a second plane (Figure 3).
Midesophageal short axis view of the descending thoracic aorta (Ao) immediately distal to the left subclavian. This image demonstrates an intra-luminal flap (arrow) and generous peri-aortic, mediastinal clot consistent with an aortic transection. Mid esophageal four-chamber view of the heart obtained shortly after patient presentation. The usual 4 chamber view is quite distorted by the significant compression from mediastinal clot compressing on the left atrium (LA) and, to a lesser extent, the left ventricle (LV). Midesophageal long axis view of the descending thoracic aorta (Ao) immediately distal to the left subclavian. This image demonstrates an intra-luminal flap (arrow) and generous peri-aortic, mediastinal clot consistent with an aortic transection.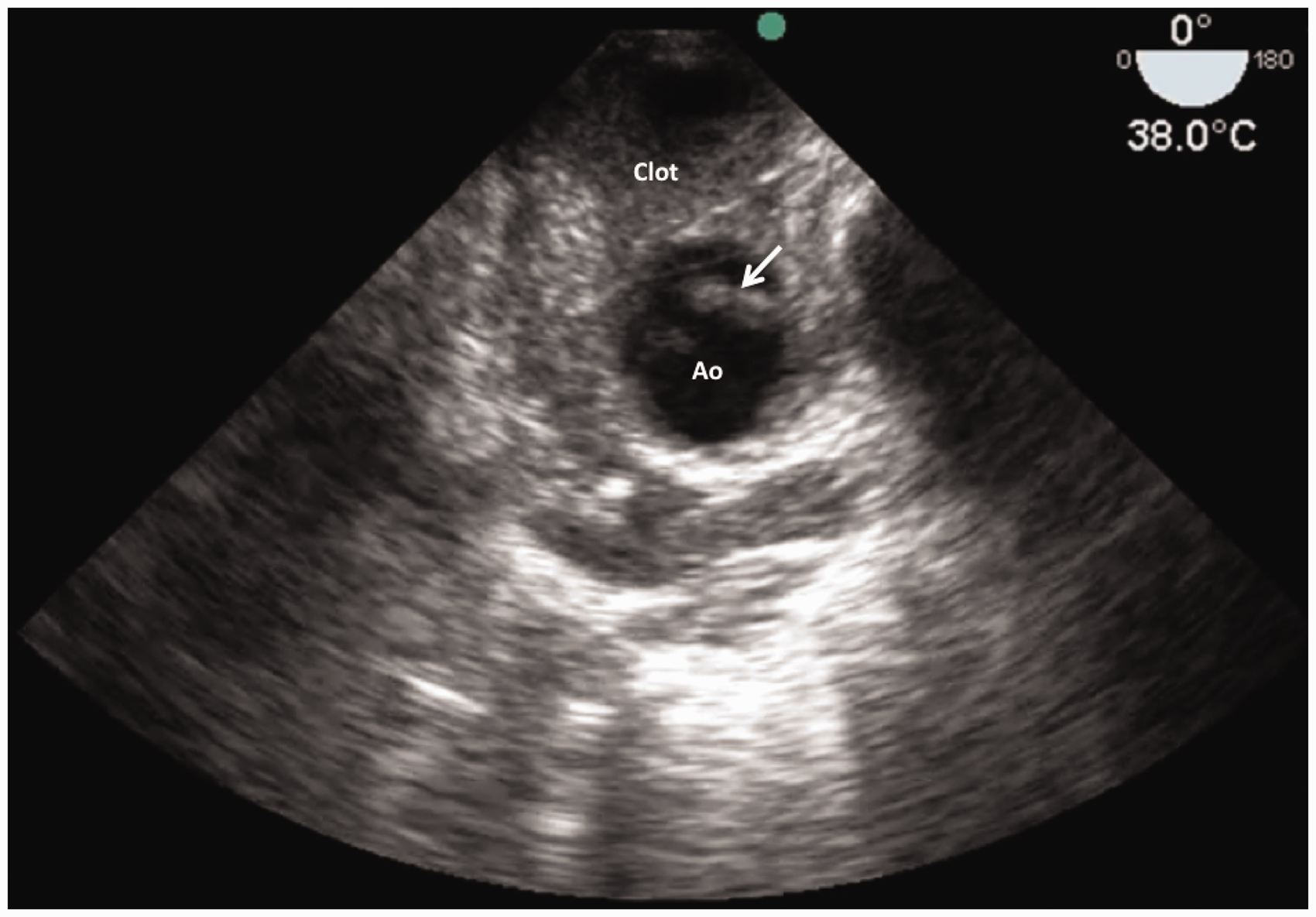
Given the identification of BTAI and associated mediastinal hematoma causing tamponade physiology, urgent surgical management was arranged. The patient was transferred to the operating room, but unfortunately vital signs were lost on the operating table and the patient expired. An autopsy was performed and did ultimately confirm the cause of death to be a transection of the descending thoracic aorta.
Discussion
We have presented the first description of BTAI identification by trauma physicians, in the trauma bay, as part of the primary survey, using goal-directed TEE.
In a meta-analysis comparing the diagnostic accuracy of TEE to CT and MRI, TEE was shown to have clinically equal reliability to axial imaging modalities in confirming or ruling out non-traumatic thoracic aortic dissection.6,7 Furthermore, TEE has shown its utility as a point-of-care diagnostic tool for a wide variety of mediastinal pathology and has demonstrated value as an adjunct in resuscitation in both the emergency department and critical care settings. 8 With this information in mind, there is the potential for the use of goal-directed, point-of-care TEE toward the diagnosis of a suspected BTAI in the unstable trauma patient.
Estimates suggest that less than 25% of patients with a BTAI will survive to be evaluated in a hospital, and as many as 50% will die in the first 24 h after their injury. 9 The Society for Vascular Surgery guidelines suggest that those patients presenting with a BTAI in the form of an intramural hematoma, pseudoaneurym, or rupture should have endovascular repair within 24 h of the identification of their injury. 10 Although many of these patients are stable enough for delayed repair, a percentage of this population does present in extremis, as was the situation in this case. When BTAI is suspected in an unstable patient, point-of-care TEE may be a feasible method of bedside diagnosis that offers several distinct advantages over traditional modalities. First, point-of-care TEE obviates the need for potentially hazardous transfer for advanced diagnostic imaging. Second, point-of-care TEE can separate those patients who are unstable as a result of their BTAI (due to compression and tamponade) from those who have BTAI but are unstable from other causes (pelvic hemorrhage, abdominal hemorrhage, etc.). Third, point-of-care TEE allows providers to choose appropriately between endovascular versus open approaches to unstable BTAI patients. This differentiation will become ever more important as vascular surgical training moves towards endovascular versus open operative techniques and as trauma providers become more adept with the resuscitative endovascular balloon occlusion of the aorta (REBOA) and less dependent upon resuscitative thoracotomy. 11
The adoption of FAST and its development into e-FAST has added significant bedside diagnostic power to the resuscitation and management of trauma patients. However, their limitation in interrogating the mediastinum leaves a diagnostic gap in certain common life-threatening pathology such as BTAI. We propose that the addition of focused, goal-directed TEE should be considered for appropriate patients being cared for by providers who are competent in limited-scope TEE. Though it does not serve to replace a full diagnostic TEE examination, goal-directed TEE may have a role in further extending the comprehensive bedside diagnostic abilities of the trauma physician to include rapid, definitive identification of traumatic mediastinal pathology. We encourage further adoption of TEE in this role as a standard part of clinical practice in resuscitation-oriented clinical programs, such as critical care, trauma, and emergency medicine. As point-of-care ultrasound training programs continue to be adopted in academic institutions, further clarity and consensus surrounding the scope and training of goal-directed TEE will be needed.
Supplementary material for this paper can be found at: http://tra.sagepub.com/supplemental.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Arntfield has served as an educational consultant for Fujifilm, Sonosite Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.