
Abstract
Background
Vertical deceleration injury is a unique urban phenomenon of blunt injury resulting in significant morbidity and mortality. Since evaluations began in the 1940s and more extensively in the 1980s through 2005, the fall height at which 50% of patients are expected to die (LD50) has been consistently estimated to be 40 ft (12.1 m) and historical reports suggest no patients were able to survive a fall greater than 50 ft (15.2 m). The aim of this study was to determine the current LD50 or survivable free fall height in comparison to historical reports.
Study design
The trauma database at an urban level one trauma center was reviewed for all falls from a significant height from January 2010 to December 2015. The data were stratified based upon the height of the fall. The height at which 50% of patients were expected to die was determined by logistic non-linear regression line plot.
Results
In total, 110 patients were identified, with 97 meeting criteria for inclusion into the study. Twelve patients fell from 60 ft (18.2 m) with six survivors. The calculated LD50 was 48 ft (14.8 m) when the heights of a story and floor were standardized to 10 ft (3 m); if the height was increased to 12 ft (3.7 m) per story, the LD50 would be 68 ft (20.1 m).
Conclusions
The survivable height, as well as the LD50 of vertical free falls, has increased as compared to previous studies. We assume that this is attributable to the advances in diagnostic imaging, interventional radiology therapies, critical care, and field management of these patients. A fall from 80 ft (24 m) exceeds the maximum threshold of force that the human body can withstand.
Introduction
Free falls from significant height represent a distinct mechanism of blunt injury resulting from significant acceleration–deceleration injury and undeterred force from the impact. The first description of “Jumper Syndrome” as a clinical entity was reported by Lewis et al. 1 Since then, multiple case studies and retrospective reports have been published describing the pathophysiologic events. Risser et al. 2 demonstrated that there were no survivors from falls greater than 60 ft (18.3 m). Since these publications, the accepted height where statistically 50% of the patients would die (LD50) was approximated at 40 ft (12.1 m). The last time that the constellation of symptoms, prognosis, and LD50 of this class of patients was evaluated was a decade ago. 3 The aim of this paper is to evaluate the survivable height and LD50 of free fall compared to prior studies.
There are several unique distributions of injuries in this population related to axial loading and shearing forces exerted upon the junction of fixed and mobile structures. Injuries sustained are the result of the kinetic energy (KE) directed into the body (KE = 0.5ċmċv2) determined by mass of the individual (m), impact velocity (v) based on the height (h) of the fall and the force of gravity (g), such that v = √(2ċgċh).1,4,5 A person falling from 40 ft (12.1 m) will have an approximate impact velocity of 56 kph and those from 60 ft (18.3 m) will have an approximate impact velocity of 80 kph.1,4,5 A 70-kg person falling from 40 ft (12.1 m) will strike the ground with 8.232 kgċm/s2 or 1850 pounds of force (Flb), while the same person falling from 60 ft (18.3 m) will sustain 12.545 kgċm/s2 (2820 Flb) of force.
There are five variables that determine the injuries produced from a free fall: kinetic energy acting on the body, the impact surface, the physical condition of the person, the area of energy dispersed, the orientation of the victim at the time of impact, and the occurrence of a decelerating force during the fall, also known as midfall impact.3,6 Case reports exist in which individuals have fallen from extremely great heights to survive; those who survive suffer severe polytrauma, morbidity and disability. Their survival is due to the nature of the impact material, such as sand, water, and snow, or their impact velocity being decreased by an object in midfall.3,7,8 Patients who do collide with an object during their descent are often impaled causing a significant amount of injury, but it is universally agreed that this impact saves the person’s life if they do not expire upon impalement. 7 Those patients whose falls result from an accident are most likely to be intoxicated, as high as 92% in some series. 9 Despite this fact, accidental falls often occur on the job, most commonly in construction workers. 8
The patterns of injury that are found in adults compared to children are markedly different. Children tend to have a higher rate of intracranial injury and decreased amount of axial skeleton fractures and intra-abdominal injury. Children are also more likely to survive a fall from higher elevations than adults. It is believed that children are able to survive the increased energy from a fall due to their cartilaginous skeletons, the decreased tone of their muscles and increased body fat content. 10 In the adult population, the height of free fall is often associated with the degree of injury, but the same cannot be said of these types of injuries in children.
Fractures are the most common injuries sustained based upon the positioning of the patient at the time of impact.1,3,4,8,11 Those patients who land in a vertical orientation have the force of the injury traveling through their axial skeleton and subsequently transferred to the pelvis and spine causing fractures at these points.4,8 Falls from four floors or greater have a predictable pattern of fractures involving the impact extremity, the pelvis, and the spine. It is important to note that the discussion of appropriate measurement comes into question when defining the height from which patients fall. Some authors refer to the height of a floor as 10 ft (3.1 m), while others refer to the height of a floor to be between 12 and 15 ft (3.7–4.6 m)1,8,11; 66% will sustain a pelvic fracture after falling from six floors, while 10% of patients who fall one floor will sustain a pelvic fracture. 4 Skull fractures, intracranial hemorrhage, spinal fractures, and calcaneal fractures are common and significant injuries that occur in this population.4,6,9,11,12
Methods
A single-institution retrospective review was conducted from the records of St. Barnabas Hospital, a level one trauma center in Bronx borough of New York City. The trauma database was reviewed for all patients presenting with a significant fall from 1 January 2010 through 31 December 2015. Electronic medical records were reviewed for patient demographics at the time of injury, the recorded height of the fall, the injuries sustained, and the disposition of the patient. The height of 20 ft (6.1 m), or two floors, was chosen as the minimal significant height for a fall as this represented three times the height of an average sized person. A 10 ft height (3 m) per floor or story was chosen to avoid possible bias and falsely elevated survivable height or LD50. The hypothesis of this study was that there would be no difference in the survivable height from a fall nor in the LD50 from vertical deceleration injury when compared to historical data.
Number of patients sustaining skull, intracranial, and maxillofacial fractures.
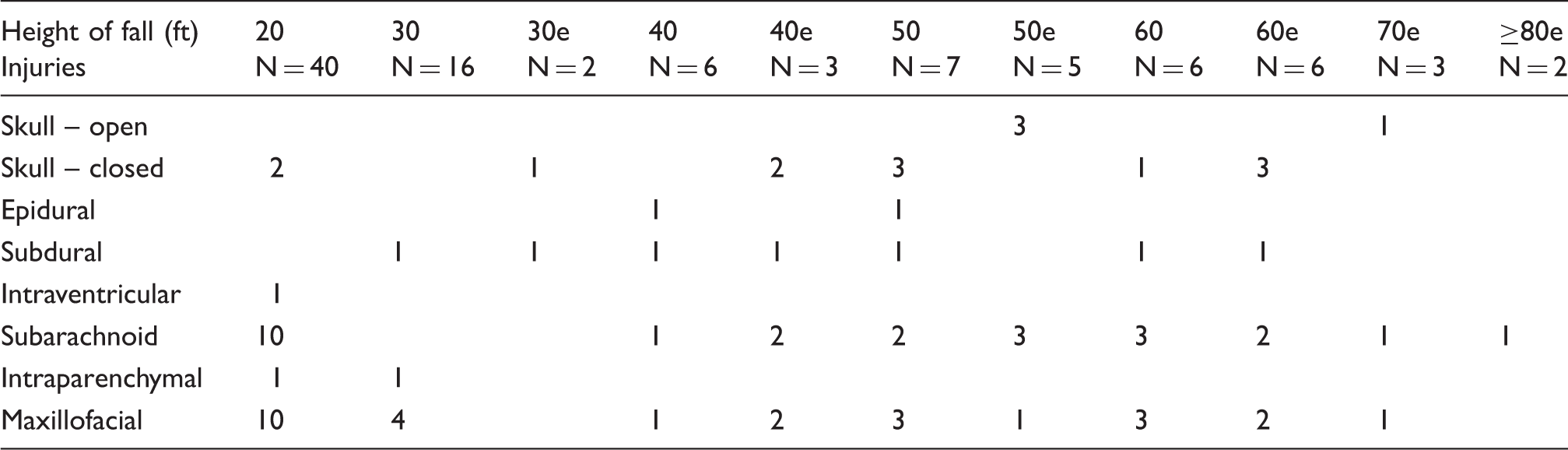
Note: The suffix ‘e’ denotes expired patients.
Patients who died in the field or en route to the hospital were included if they arrived at the hospital to be pronounced, whereas those not brought to hospital were not included in these figures. Death most often occurred on arrival to the trauma center or within 24 h. Those patients dying within 24 h of presentation were included as mortalities.
Following the collection of data, the information was stratified into patient groups based upon the height from which each patient fell. The injuries sustained were recorded to search for common injuries that correlated with fall height. The information was plotted into a stacked column chart to demonstrate how the collective of patients fared based upon the height of their fall. A four-parameter logistic nonlinear regression line plot was constructed to determine the point at which 50% of patients were expected to survive the fall (LD50).
The LD50 was calculated using the method developed by Miller and Tainter in 1944.14,15 The raw data were converted into mortalities per total participants in each treatment group which was determined by height. The percentage of mortalities per treatment group was then calculated as mortalities/total subjects × 100. The corrected percentage was then calculated for 100%: 100((n−.25)/n) = 99.75, where n equals the total number of subjects included in study. Probits, or probability units, were then determined from the corrected mortality percentage using Finney’s table,
16
and the Log (base 10) of height calculated. A scatter plot of the Log of height versus probit of mortality was then generated using spreadsheet software. A trendline with equation for the trendline and its R2 coefficient was then generated based upon this analysis (Figure 1). The equation was then solved for x using the probit, for 50% (y = 5.00, determined from Finney’s table).14–16
Formula and graphical representation for determining the LD50 for vertical deceleration injuries.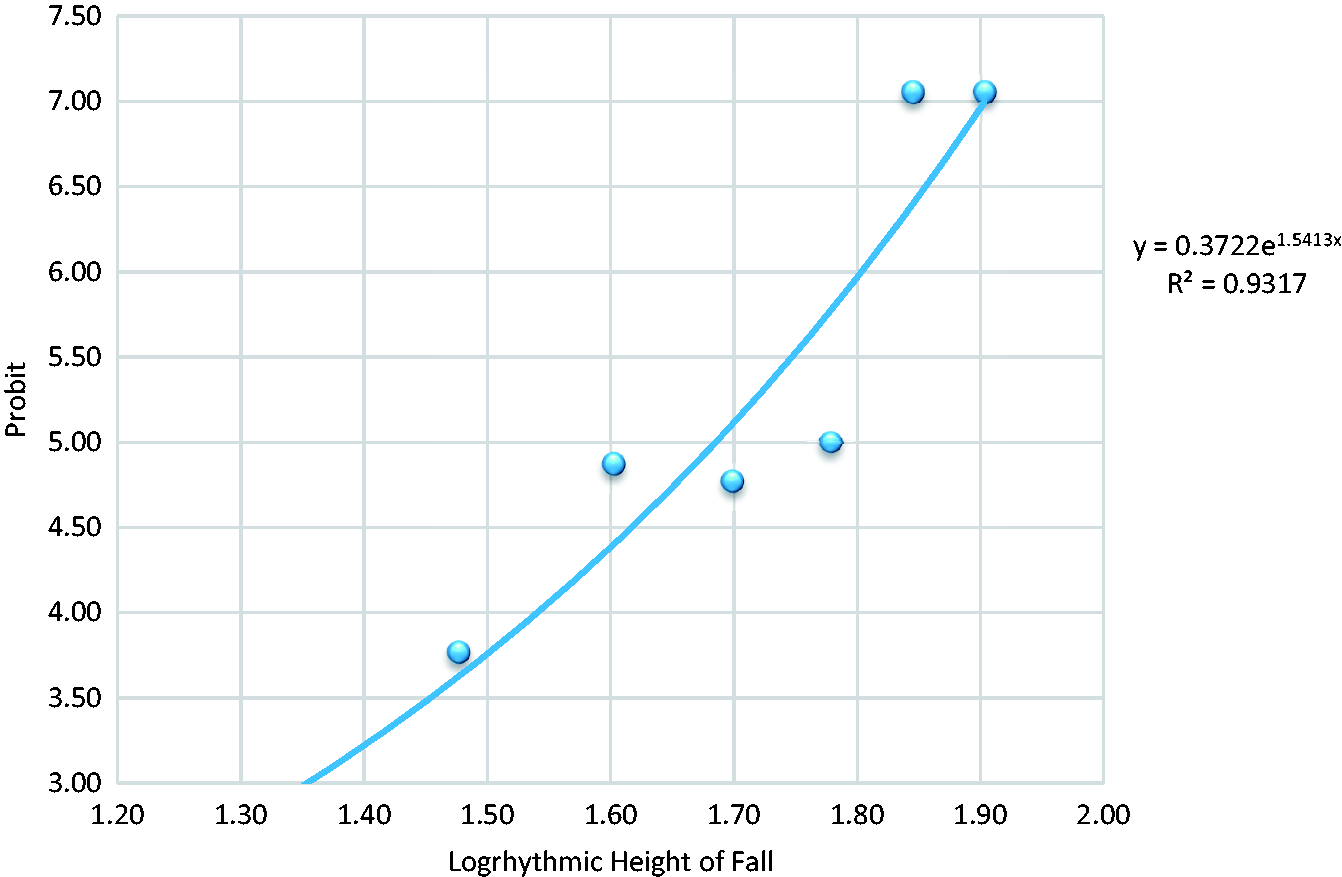
Results
In total, 110 potentially relevant patients were identified in our registry: four were excluded due to concomitant injuries, two due to falling into a body of water, three because of the age criteria and five due to midfall impact; hence, 97 patients met criteria for inclusion in this study and their injury burden and ISS are shown in Tables 1–6. Twenty-one of these patients died (Table 6 and Figure 2). There were seven unobtainable autopsy reports (two from the 50 ft (15.2 m) group, three from the 60 ft (18.2 m) group and one from each of the 70 ft (21.2 m) and 80 (24.2 m) groups). All 40 patients who fell from 20 ft (6.1 m) survived including one who suffered only minor lacerations and abrasions; 16/18 patients survived a fall from 30 ft (9.1 m) – those who died from a 30 ft fall suffered closed head injury, aortic laceration, and traumatic arrest.
Outcomes by free fall height.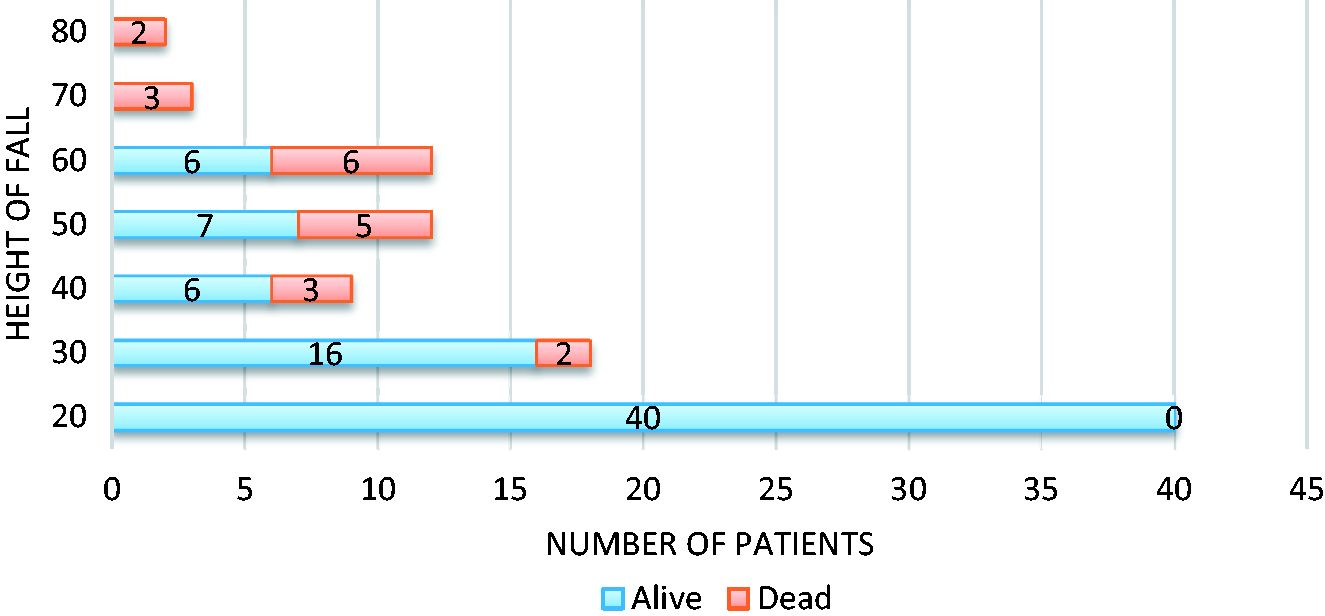
Most of the patients (7/12) who fell from 50 ft (15.2 m) survived the fall and were brought to the hospital and required admission; one patient died approximately 24 h after admission, from an open skull fracture, multiple rib fractures, and closed lumbar fractures. Half of the 12 patients who fell from 60 ft (18.2 m) survived, whereas all those who fell from higher, i.e. 70 ft (21.2 m) or above, died on scene or en route and were pronounced dead on arrival.
Of the 97 patients, there were 80 head and facial injuries, 56 spinal fractures, 136 thoracic injuries, 91 abdominal injuries, 120 extremity fractures (Tables 1 to 5). By using the method described by Miller and Tainter, the logistic analysis identified that our LD50 was 48 ft (14.6 m) within this data set (Figure 1).
Discussion
The height of vertical deceleration fatalities as well as the LD50 has remained constant for the last half of a century at 40 ft (12.1 m); our data for the last five years have calculated an LD50 of 48 ft (14. 6m). There are several issues that arise from this. The first is that our data attempted to eliminate the possibility of false elevation of the LD50 height by decreasing the height of fall to the lowest 10 ft (3 m) as well as converting stories and floor definitions to a standard 10 ft (3 m) measure; as 40 ft (12.1 m) and four stories vary by definition and report which may imply that the LD50 of free falls is unchanged as 48 ft (14.6 m) and four stories may be synonymous. Although it has been demonstrated by previous authors that there were no survivors falling from six stories, 2 we have demonstrated that falls from this height are survivable and half of the patients within this subset of data survived beyond the initial 24 h of admission. Although not conclusive, we believe that this supports the argument that the mean survivable height of free fall has increased.
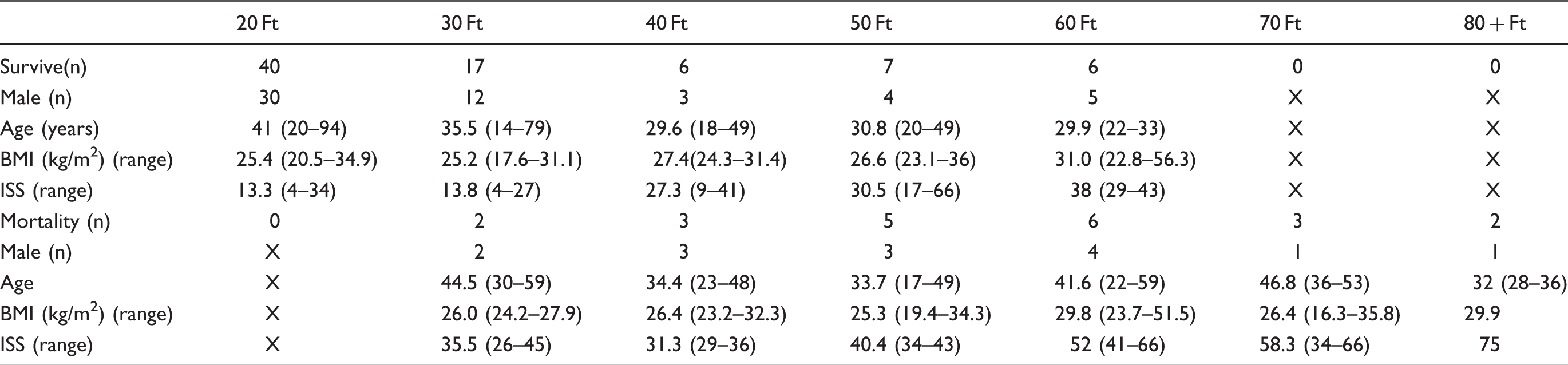
As expected, the mean and individual ISS increased as the height of the fall increased in both the surviving and mortality groups (Table 6) and ISS was higher at all heights in the mortality groups than the survivors; however, the mean ISS was lower in the 40 ft (12.1 m) mortality group than the 30 ft (9.1 m) group, which we attribute to statistical error due to the small groupings. Mean BMI was not significantly different between different fall heights of survivors, different fall heights of those that expired, or when comparing survivors to the deceased. Males were more commonly found to have sustained vertical deceleration injuries.
Number of patients suffering spinal fractures.

Note: The suffix ‘e’ denotes expired patients.
Number of thoracic injuries sustained.
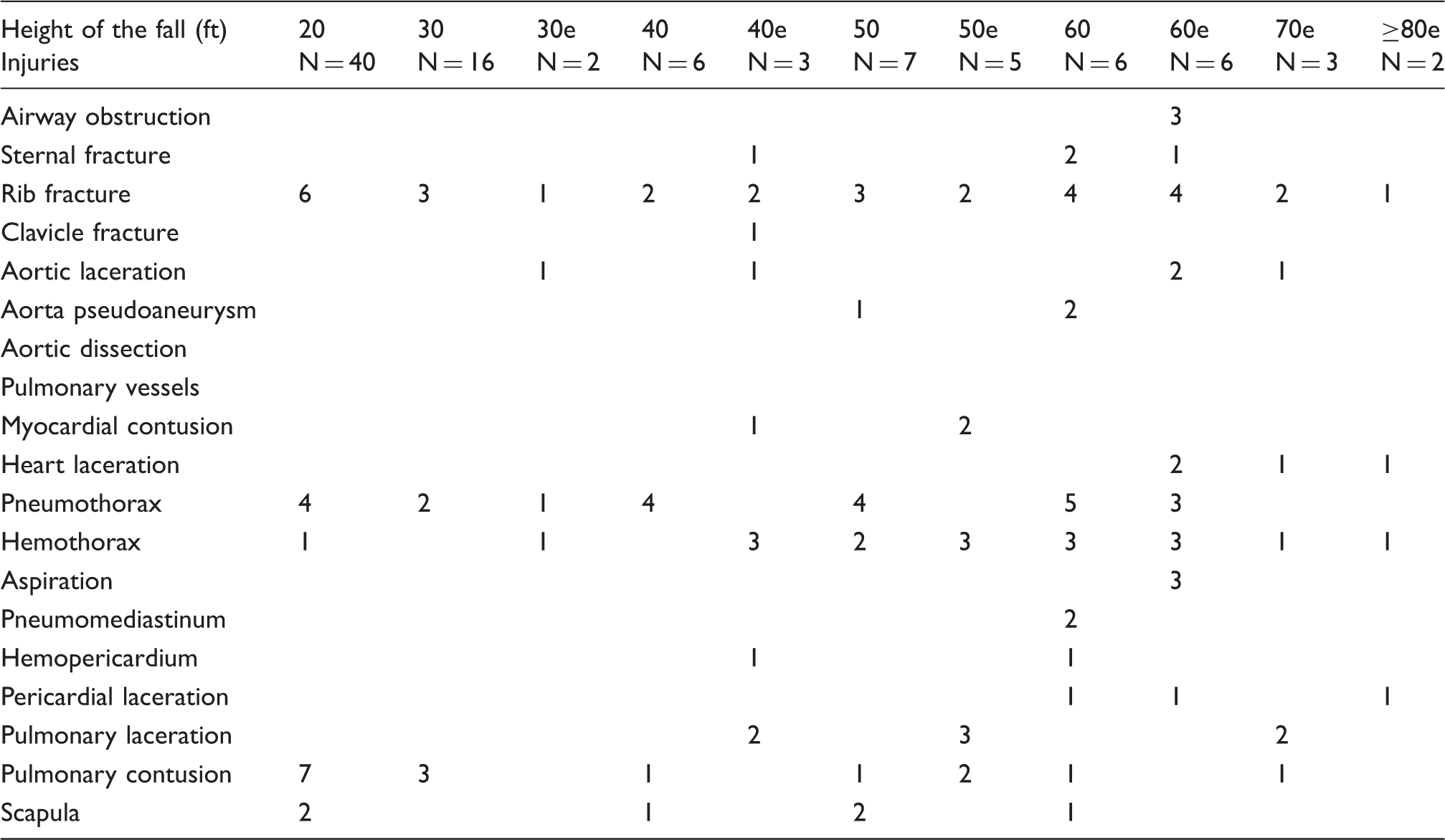
Note: The suffix ‘e’ denotes expired patients.
Open skull fractures were always associated with mortality. There were multiple intracranial hemorrhages, and patients who expired often had more than one type of intracranial hemorrhage. There were 80 head and facial injuries amongst the 97 patients (Table 1). Historically, intracranial and skull injuries are common within this population of patients. Patients who land on their feet from free fall are subject to basilar skull fractures, craniofacial disassociations, and intracranial hemorrhage.8,9,11 As many as 80% of patients who die from vertical deceleration injuries are found to have intracerebral hemorrhage. 12
Fifty-six spinal fractures were identified among our patients (58%) (Table 2), which is comparable to the historic data that 60% of patients sustaining vertical deceleration will have a spinal fracture. The most common spinal fractures occur at the thoracolumbar junction causing neurologic deficits; approximately one-third (37%) of spinal fractures are unstable after a fourth floor fall. 11 These fractures can be clinically silent because pain or tenderness is an uncommon finding on physical exam.4,8,11
Number of patients with abdominal injuries and their American Association for the Surgery of Trauma grade (G) and number with each grade.
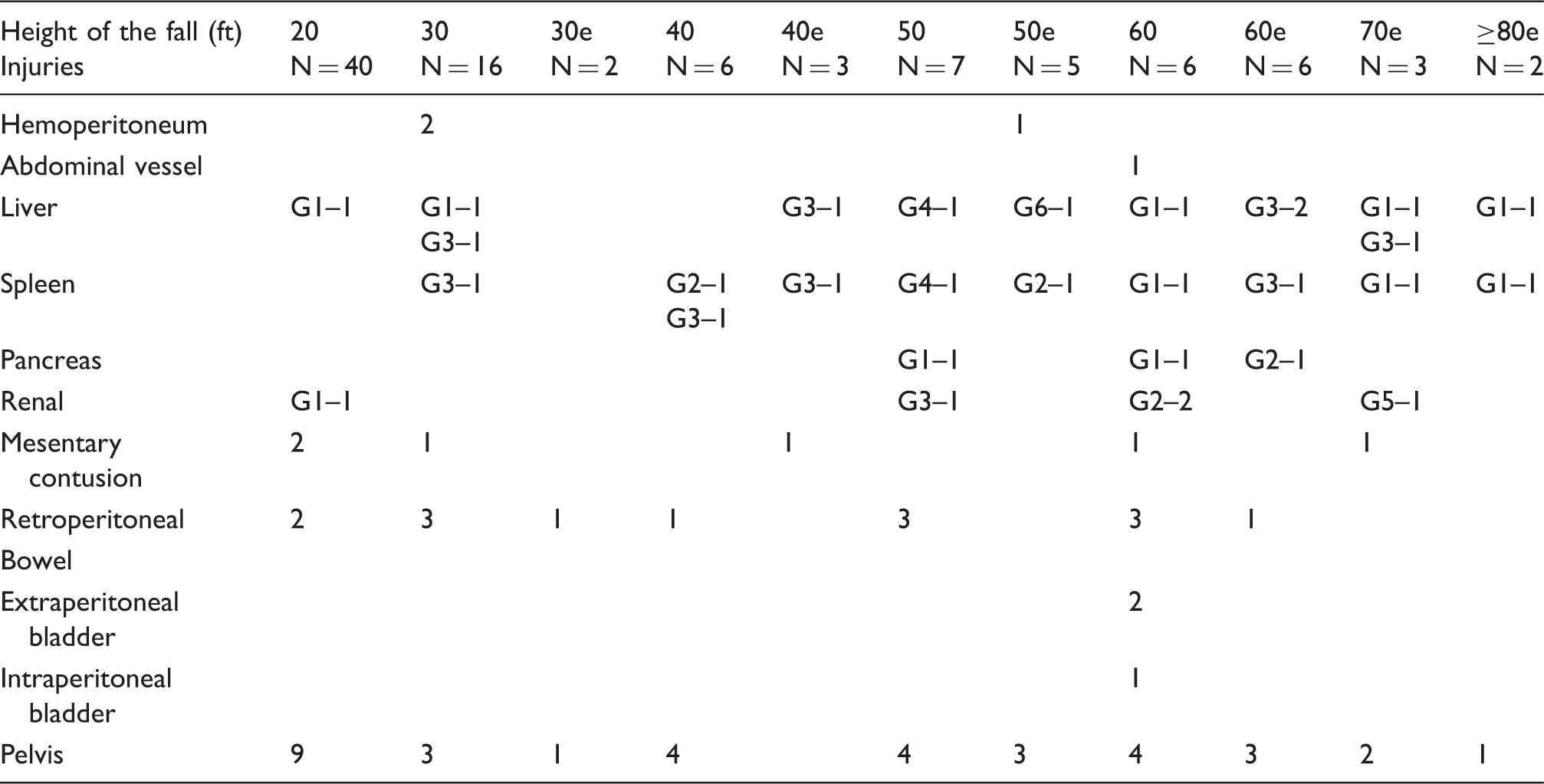
Note: The suffix ‘e’ denotes expired patients.
Number of patients with extremity injuries.
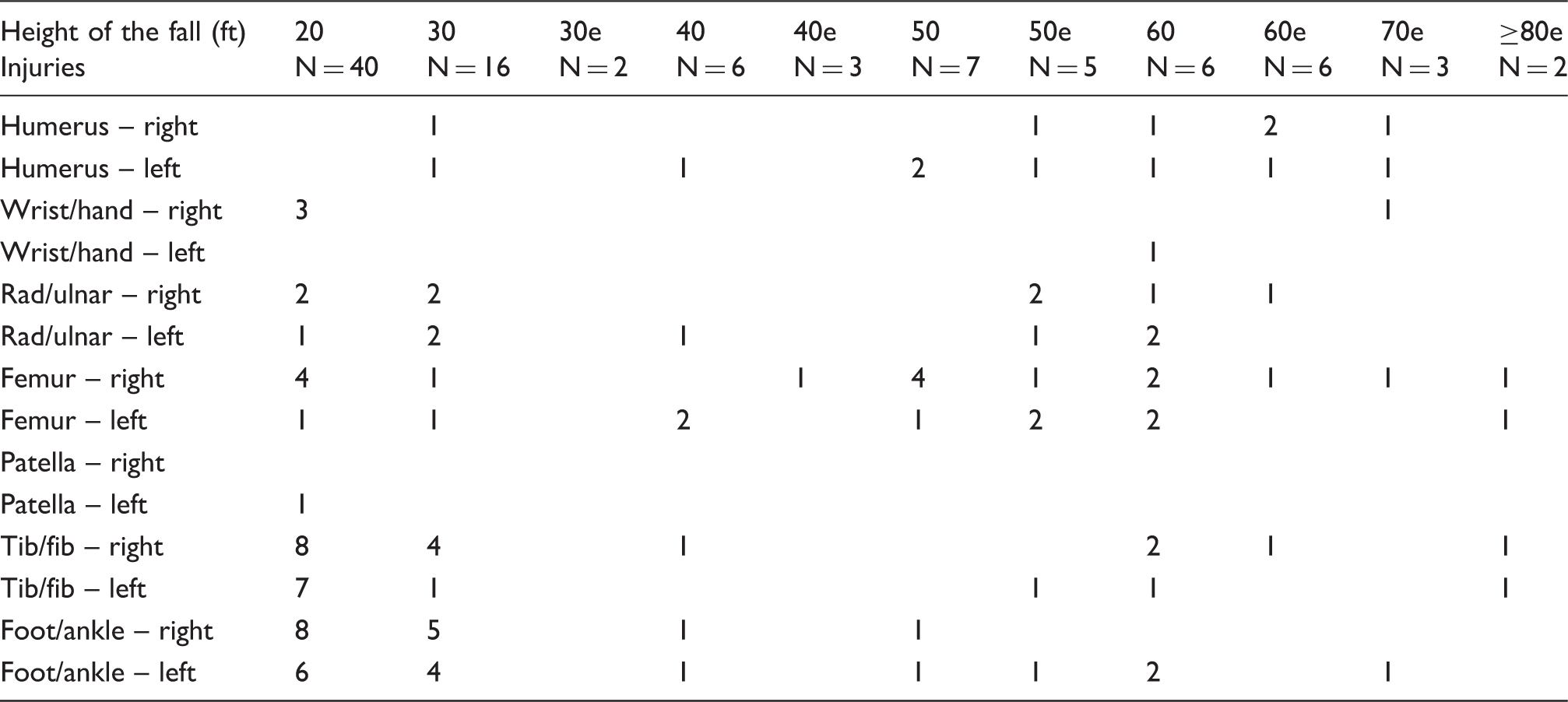
Note: The suffix ‘e’ denotes expired patients.
Patient data based on fall height.
As demonstrated by Brandes and McAninch, 17 the height of a fall did not correlate with the degree of renal injury. In their study, no renal devascularisation (Grade 5 renal injury) was identified, whereas in our data set, one patient who fell from 70 ft (21.3 m) was found to have a kidney stripped of its vascular supply from the impact. The inability to correlate height of fall to abdominal solid organ injury was demonstrated in this data set as well. One patient suffered complete devascularisation of the liver after falling from 50 ft (15.2 m) while less significant hepatic injuries were found on patients who plummeted from increased heights. Internal hemorrhage is another commonly encountered cause of significant morbidity and mortality in vertical deceleration injuries. The most common source of bleeding in these cases is due to retroperitoneal hemorrhage and bleeding from fracture sites. 11
Extremity fractures were common (Table 5) with 121 identified, 31 of which were in the ankle and foot. Historically, calcaneal fractures are another common finding of a particular significance as they indicate a marked loading force from vertical orientation; between 10 and 25% of patients with these injuries will have sustained thoracic or lumbar spine injuries.4,8
Much like there are lethal doses to all therapeutic drugs, there is inevitably a purely lethal dose of a free fall, as the human body is only capable of sustaining a certain amount of force exerted upon it and we believe that a fall from 80 ft (24.3 m) or greater exceeds the maximal load that the human body can withstand. The reason for the suggested increase in survivable height was not determined by this study, but we suspect that this is due to a combination of improvements in field management by emergency medical teams, increasingly rapid imaging, improvements in minimally invasive and endovascular procedures as well as better quality intensive care. Without the intersection of these four advancements, an increase in the survivable height of a free fall would have been impossible.
There are limitations to this study: we did not evaluate the patient’s reasons for falling, i.e. accident or intentional, nor did we evaluate if the individual was intoxicated at the time. This was intentional as we believed it may have influenced the evaluation of the data. A further drawback is that this study was performed at a single institution and with a limited number of patients. Although there was an increase in the height of survivable falls, there was no great change in the LD50. To comment further on this, we decreased the heights of stories and floors to a standard 10 ft (3 m) which undoubtedly influenced the outcomes of the mean survivable height. It is important to note that the LD50 is an underestimate due to our standardization requirements. Had we calculated the height of floors and stories to be 12 ft (3.7 m), the LD50 would be 68 ft (20.7 m). A final limitation is the absence of seven autopsy reports which limited the knowledge of the complete spectrum of injuries.
Conclusions
We assume that improvements in field triage and management, expedited and accurate diagnosis made by imaging, advances in interventional radiology as well as critical care have led to the improved survival of patients falling from increased heights. With this analysis, we have shown that there has been an increase in the survivable height of free falls, although there may not have been an increase in the survivable mean height, or LD50. To our knowledge, this is the first article produced within the past decade to study this condition. We hope that our observations will encourage others to re-evaluate the survivable height and LD50 of vertical deceleration injuries at other institutions and encourage traumatologists to continue their efforts to improve the survival rate in this complicated but potentially salvageable class of patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.