
Abstract
Objectives
Falls are common in older people, causing significant mortality and morbidity, but little is known about this phenomenon in developing countries. This study aimed to investigate falls in older people in the developing world, comparing fallers with other trauma patients.
Methods
We conducted a prospective observational study of older trauma patients in Trinidad over a four-month period, comparing falls victims with other trauma patients, in relation to their demographic, pre-morbid and injury characteristics.
Results
A total of 439 older trauma patients (aged ≥65 years) were included. Fallers were older (median age 75 years (interquartile range 65–89 years) vs. 70 years (interquartile range 65–79 years) in non-fallers). Overall, 65.2% of fallers were female, compared to 43.7% of non-fallers. Fallers were more likely to suffer from multiple pre-existing diseases, with 29.8% having ≥3 comordibities, compared to 9.7% of non-fallers. Fallers were also more likely to be on multiple medications: 7.1% were on five medications, compared to no non-fallers. Fallers also sustained more severe injuries and presented with higher acuity than non-fallers. Admission and referral rates were higher among fallers compared to other trauma patients (59.9% vs. 30.4%).
Conclusions
Older patients who fall are a distinct group from other older trauma patients, with unique demographic, clinical and injury-related characteristics. This information is useful in planning preventive and management strategies for these patients.
Introduction
Falls are the commonest mechanism of injury in older people, but there is limited research comparing falls with other types of trauma in this age group. Among these older patients low falls are the most lethal injury mechanism they sustain. 1 Several authors have investigated falls in older people, but did not compare older fallers with other trauma patients.1–3
The developing world’s population is ageing, and by 2050 three-quarters of the world’s older people will live in developing countries. 4 Understanding the health and social problems that older people face is particularly relevant in these countries.5,6
Falls are an important cause of morbidity and mortality in older people.1,3 Sampalis et al. compared older falls victims in Canada with those involved in road traffic collisions (RTCs), and found a higher risk-adjusted mortality in those with falls, 7 but that study’s findings may not be transferable to developing countries. We therefore designed this study to compare older patients with falls to other older trauma patients, in a developing country.
Materials and methods
A prospective observational study of trauma patients ≥65 years presenting to the Emergency Department (ED) of San Fernando General Hospital, a tertiary hospital serving the South of the island of Trinidad, was conducted over a four-month period (April to June 2010), comparing fallers with other trauma patients. Previous research has shown that trauma accounts for approximately one in five ED admissions in Trinidad, with falls accounting for one-third of all injuries. The commonest mechanisms of injury are accidents, followed by assaults (including gunshot wounds and stabbings) and RTCs. 5 Falls were defined according to the World Health Organisation’s definition as ‘an event which results in a person coming to rest inadvertently on the ground or floor or other lower level’. 8 A ‘slip or trip’ was defined as an accidental mechanical interruption of gait which may or may not have resulted in a fall.
Trauma patients were defined as any patients sustaining injuries due to mechanical force. All trauma patients aged ≥65 years who were admitted to the ED during the period of the study were included. Patients who sustained thermal and chemical injuries as well as those with drowning or near-drowning were excluded. Trauma patients were identified through an injury surveillance database maintained in the ED and cross-checked with the admissions register to identify any potential trauma patients who may have been missed by the injury surveillance system. A data collection form was completed by the staff in the ED for each patient. Missing data were then extracted from patients’ clinical notes by the lead researcher.
Demographic characteristics (age and gender), pre-existing medical status (type and number of chronic illnesses, number of medications), injury characteristics (injury severity and number of injuries) and outcomes (hospital admission, discharge home or referral to a specialist) were compared. Abbreviated Injury Scores (AIS) were calculated for each injury from ICD-10 codes. If an ICD-10 code was mapped in more than one AIS, and the lowest AIS was used. Statistical analysis was performed using SPSS version 21.0. Categorical data were compared using Chi squared analysis. Multiple logistic regression analysis was used to identify any associations between the risk of falls and age, gender, or comorbidities.
Anticipating the prevalence of significant characteristics (demographic, injury-related and pre-morbid conditions) to be approximately 20–50%, we estimated that a sample size of 92 patients per arm of the study would identify significant differences in the two patient groups with a margin of error of 10%.
Research ethics approval was obtained from the Southwestern Regional Health Authority and the University of the West Indies. All study participants were required to provide written signed consent.
Results
Demographic and clinical characteristics of study participants.

Table 1 summarises the demographic and clinical characteristics of older fallers and non-fallers. Fallers were more likely to be female (219 (65.2%) vs. 45 (43.7%), p < .001). The median ages of fallers and non-fallers were 75 years (interquartile range (IQR) 65–89 years) and 70 years (interquartile range (IQR) 65–69 years), respectively. Falls occurred more often in the home than did other injuries (89% vs. 49.5%, p < .001). While 28(8.3%) fallers lived alone, none of the non-fallers lived alone (p < .001).
Older fallers had more pre-existing medical conditions and were on more medications (Table 1). Overall, 100 (29.8%) fallers had three or more medical conditions, compared to 10 (9.7%) non-fallers (p < .001). These included ischaemic heart disease (95 (28.3%) vs. 18(17.5%), p = 0.029), hypertension (185 (55.1%) vs. 42 (40.8%), p = .013) and stroke (25 (7.4%) vs. 1(1%), p = .015). Ten (3.0%) falls were associated with seizures and seven (2.1%) with syncope.
While 24 fallers were on five or more medications, no non-fallers were on ≥ 5 medications (p < .001). The use of anti-hypertensives (177 (52.7%) vs. 40 (38.8%), p = .018), cardiac medication (123 (36.6%) vs. 20 (19.4%), p = .001) and nonsteroidal anti-inflammatory drugs (NSAIDs) (123 (36.6%) vs. 13 (12.6%), p < .001) was more prevalent in fallers.
Adjusted odds of falls with age, gender and comorbidities. a
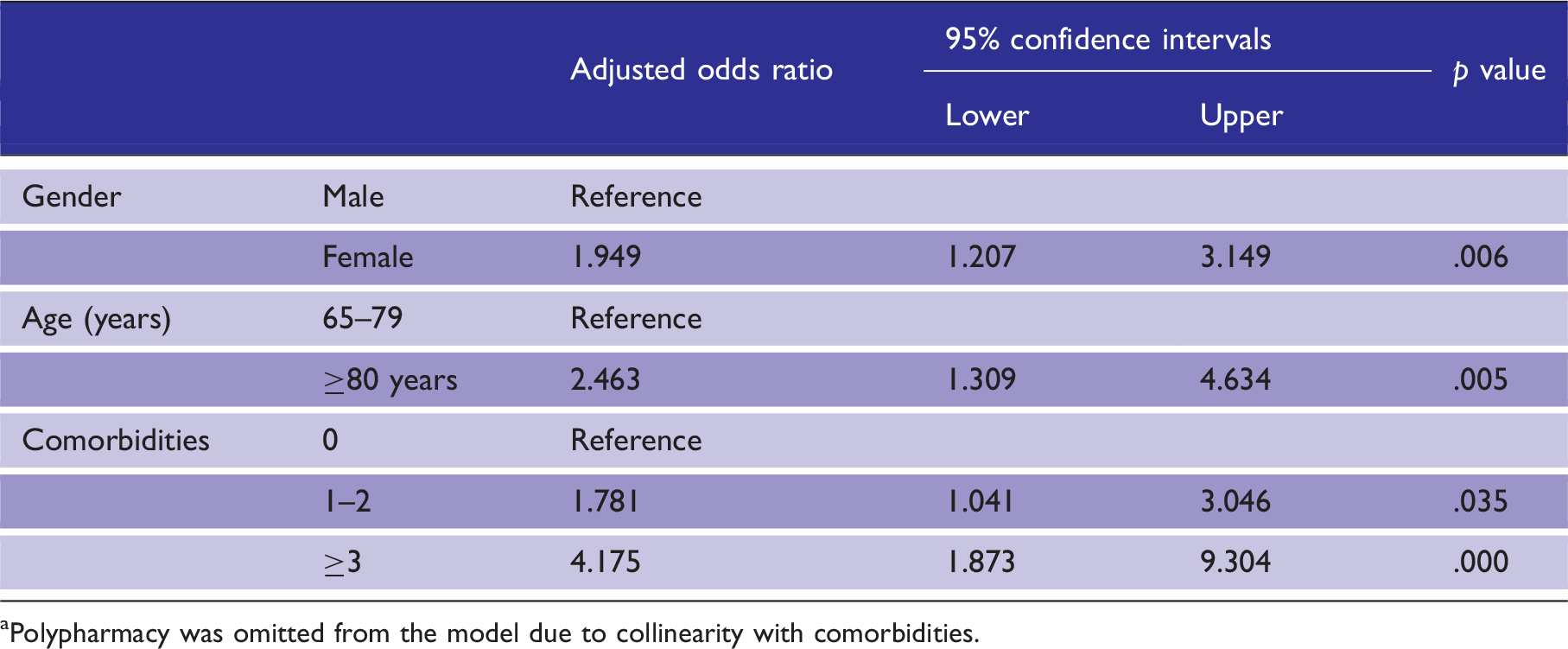
Polypharmacy was omitted from the model due to collinearity with comorbidities.
Older fallers were more likely to have dysmobility, visual impairment and pre-existing cognitive impairment (Table 1) and 95 (28.3%) fallers had a history of a previous falls, compared to three (2.9%) non-fallers (p < .001).
Injury characteristics of the study participants.
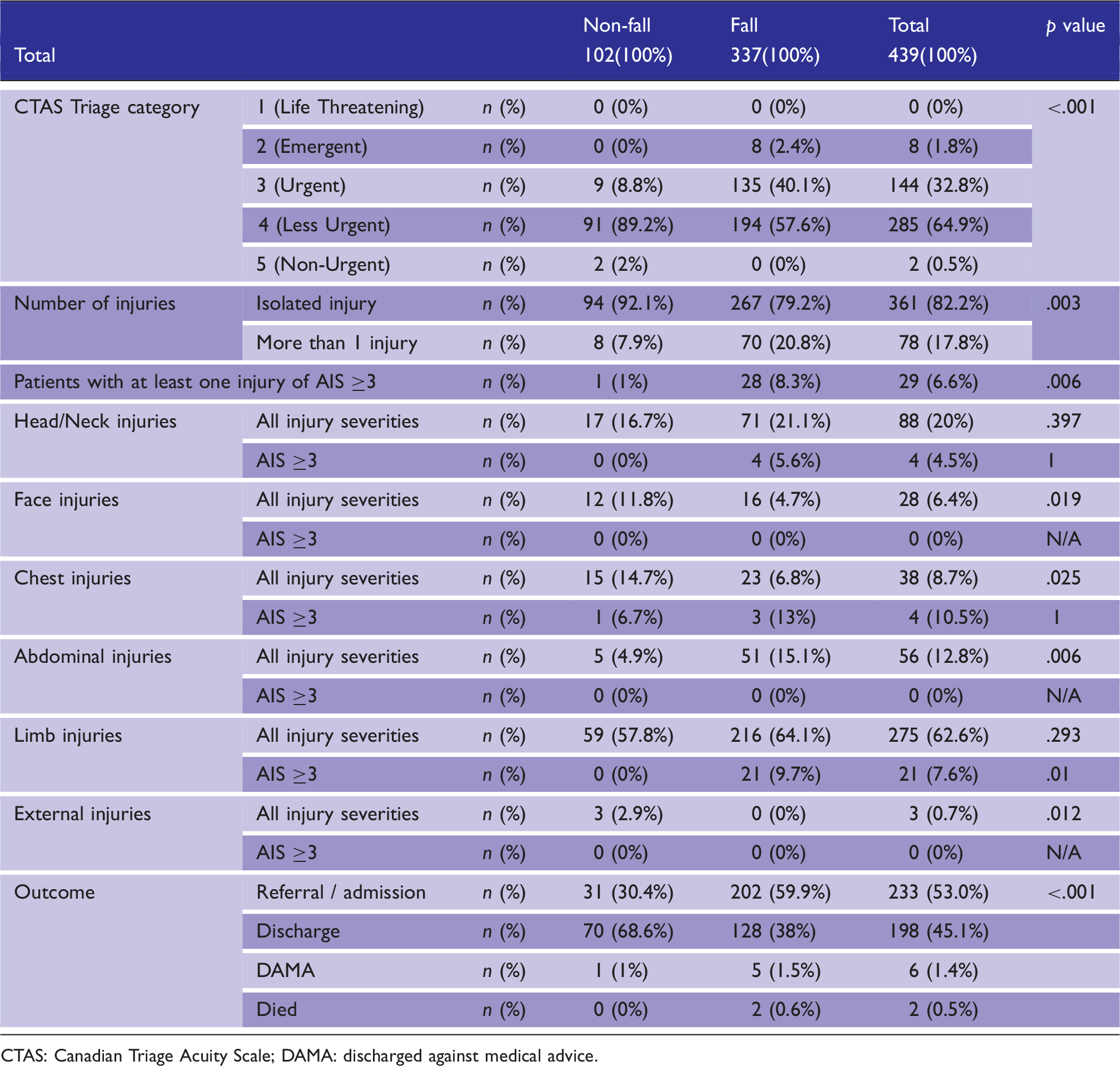
CTAS: Canadian Triage Acuity Scale; DAMA: discharged against medical advice.
Triage categories were higher in fallers; eight (2.4%) were triaged as emergent and 135 (40.1%) as urgent, compared to zero (0%) and nine (8.8%) of the non-fallers, respectively (p < .001). Patients with falls were more likely to be referred or admitted than non-fallers (p < .001).
Discussion
Compared to non-fallers, older people with falls were more likely to be female and had a higher chance of being admitted to hospital. These finding concur with previous research on falls in developed countries.9,10 Naraynsingh et al. reported higher rates of hospitalisation and increased injury severity among older trauma patients in Trinidad. 5 Our study has further demonstrated that falls produce more serious consequences than other types of trauma in older people.
In our study, older fallers and non-fallers represented two distinct groups. Fallers were older, more socially isolated, had more medical conditions and were on more medication than other trauma patients. The poorer levels of health and social support in fallers may explain why more falls occurred in the home, as these patients would be less likely to go out. This increasing risk of social isolation among fallers poses significant public health challenges in developing countries with rapidly aging populations. Several authors have noted the association between pre-existing medical conditions, polypharmacy and falls.1,3,11 This study confirms this association in older people in the developing world, and reinforces the importance of addressing these underlying conditions when managing older patients who present with apparently simple falls.
Older fallers in our study had more severe injuries than other patients. These findings are similar with the previous research: Sampalis et al. demonstrated a higher mortality rate among older fallers, while both Spaniolas’ and Sterling’s groups showed that ground level falls in older people were associated with more severe injuries and higher mortality.1,3,7 The generally low incidence of severe injuries in our study may be because we mapped ICD-10 codes to the lowest possible relevant AIS scores, thus underestimating injury severity. 12
The injury patterns in our study did not conform to those found in other studies of older trauma patients. While head and limb injuries were more prevalent in fallers, these differences were not statistically significant, possibly due to the small sample size. However, the increased prevalence of chest, abdominal, facial and external injuries in older non-fallers has been reported by others. 7 The higher incidence of severe limb injuries in fallers reflects the increased risk of fractures in this group.3,5
This is the only study to date to compare falls with other mechanisms of injury in older people in the world. However, there are few limitations. The study sample was relatively small, and this may account for the lack of significant differences in injury patterns between the two study groups. This was also a single centre study. However, the San Fernando General Hospital serves approximately half of the population of Trinidad and Tobago, and patients attending the ED are representatives of the population as a whole. Ideally, a prospective multi-centre trauma registry involving all major hospitals on the island would provide much better data on trauma in general and trauma in elders in particular.
Conclusion
We therefore intend to establish a trauma database across all hospitals in Trinidad and Tobago, which will allow us to monitor all trauma patients, including those with falls, and develop a better understanding of the role of injuries in the morbidity and mortality of older patients.
The results of this study will provide useful information to those creating strategies for managing elderly trauma patients in developing countries. We intend to use the demographic and clinical data from this study to develop and test interventions for falls prevention in older people in our setting, including home-based falls prevention programmes as well as medication reviews and routine vision and hearing tests for older persons who present to the ED with falls.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Provenance and peer review
Not commissioned, externally peer reviewed.