
Abstract
Introduction
Increasingly complex distal radius plate designs are available for treating distal radius fractures. As a result, many fractures are being ‘over-treated’ with more complex volar plate designs than necessary. We hypothesise that significant cost savings could be made by rationalising the use of complex locking plate designs.
Methods
Over a two-year period, radiographs of 250 consecutive distal radius fractures fixed with volar locking plates were reviewed and the type of plate, and type and number of screws used for fixation were noted. Preoperative radiographs were independently reviewed to ascertain if it would have been possible to stabilise the fracture with a simpler, extra-articular plate design. Potential cost savings were then calculated.
Results
It was deemed that 89 (36.5%) of the 250 cases originally treated with a more complex 2 column variable angle plate could have been treated with an extra-articular construct, leading to potential savings of £19,224.
Conclusion
It is clear from our data that many distal radius fracture patterns are being ‘over-treated’ with complex locking plate designs with multiple rows of screws and that substantial cost savings could be made by selecting an appropriate construct to suit the fracture pattern.
Introduction
In the current economic climate, huge financial savings are required throughout the NHS whilst maintaining standards in patient care as the NHS is facing its largest efficiency challenge in history. To achieve the predicted £20 billion savings required throughout the NHS, individual trusts and departments are required to achieve savings of approximately 5% per year. 1 Distal radius fractures account for up to 17% of all fractures and are becoming increasingly common in the aging population. 2 As a result, management of these fractures accounts for a large proportion of trauma budgets.
There has been a recent huge increase in the number of distal radius fractures being treated with locking plates in the belief that these enable a superior fixation, increased stability and allow earlier mobilisation and therefore produce a better clinical outcome compared with plaster cast or percutaneous wire treatment. In response to this market demand, many manufacturers have developed increasingly complex and specific locking plates to address particular problems that each fracture pattern poses. Although this has in theory increased stability of fixations, it restricts the direction and placement of screws which are ‘locked’ in a fixed direction in the plate. In order to combat this, many companies now offer ‘variable angle’ locking screws, which in conjunction with specific plates, allow the surgeon greater flexibility in screw placement whilst still locking the screw into the plate. This theoretically is beneficial in more complex fracture patterns with smaller fracture fragments, but also has the potential disadvantage of screws being placed inappropriately such as into the radio-carpal or distal radial-ulnar joints.
The recently published pragmatic randomised controlled UK Distal Radius Acute Fracture Fixation Trial (DRAFFT) reported no difference in patient-reported outcomes between locking plates and Kirschner wire fixation in a specific and large group of fractures which could be reduced closed to a satisfactory position. 3 The authors highlighted that Kirschner wiring is a technique which is both quicker and cheaper to perform.
Whilst it is apparent that great cost savings could be made by treating more distal radius fractures using Kirschner wiring, volar plating has become a favoured technique amongst many surgeons over the last decade.
Given the rise in popularity of locking plates over this period, many current trainees and newly appointed consultants will have had limited training in wiring techniques in comparison to locking plates and prefer to use a technique they are more familiar with – certainly for more complex fractures. With the burgeoning number of plate designs available on the market, it has also become apparent that many of those fractures that are being treated with volar locking plates are potentially being ‘over-treated’ with more complex plate designs than are required for particular fracture configurations. This may be due to a poor understanding of the principles of different plate designs by surgeons, an over-engineering of plates for simple fractures and the constraints in plate selection imposed by various trusts. We hypothesised that significant cost savings could be made by rationalising the use of complex locking plates and using cheaper, less specific extra-articular locking plates constructs in the surgical management of distal radius fractures.
Method
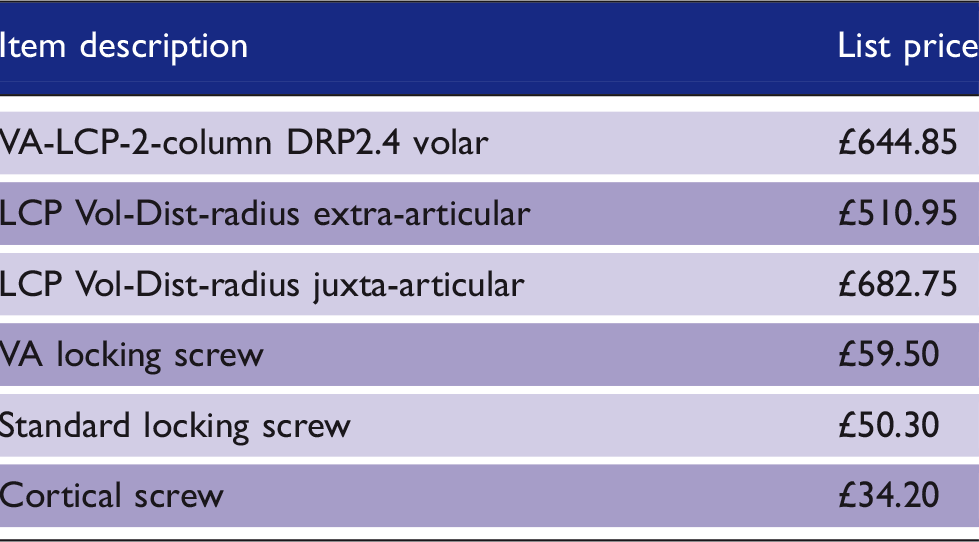
List prices and contract prices for each plate and screw type used across the 250 patient cases.
Results
Overall, 318 distal radius fractures fixed with locking plates were identified in the two-year data period – 68 were excluded (27 dorsal plates, 22 volar rim plates, 16 combined and 3 with other associated injuries) leaving 250 cases for analysis. A majority, 172 (68.8%), were female, and the overall mean age was 57.74 years (range: 18–93) – 141 fractures (56.4%) were on the left and there were no bilateral fractures. Twelve (4.8%) patients had treatment for an ulna styloid injury, and one (0.4%) had a triangular fibrocartilage complex (TFCC) repair. Out of the 250 cases, 67 (26.8%) were operated by hand surgeons with a specialist interest in distal radius fractures and 183 (73.2%) were performed by general trauma and orthopaedic surgeons; 192 (76.8%) of the cases had fixation using the most expensive style ‘VA-LCP 2-column DRP 2.4’ plate, 32 (12.8%) using an ‘LCP Vol-Dist-Radius Extra-articular’ plate and 26 (10.4%) using an ‘LCP Volar DRP 2.4 Juxta-articular’ plate.
The number and percentage of theoretical versus actual plate used in each of the 250 patient cases.
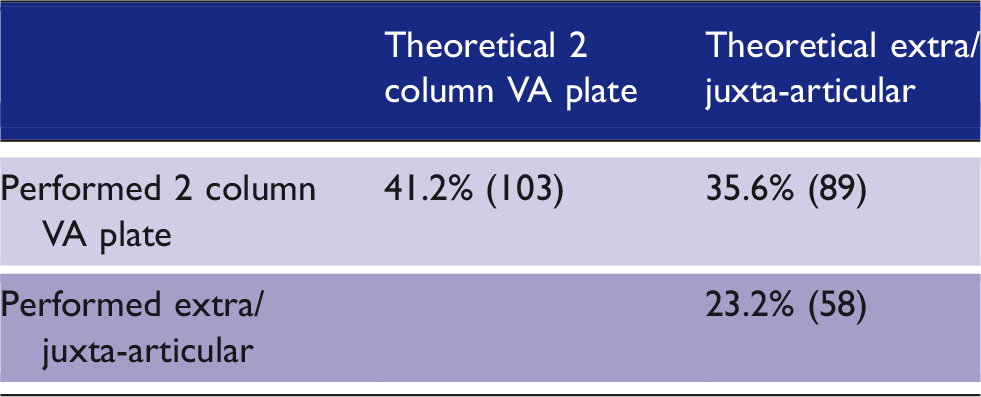
Out of the cases that theoretically could have, or actually did have, an extra-articular-type plate used, 17/147 (6.8%) were performed by hand surgeons, and the remaining 130/147 (93.2%) were performed by general orthopaedic surgeons. The 32 cases where the extra-articular plate was used were all performed by non-hand surgeons, and where an extra-articular or juxta-articular plate could have been used but was not, 17/89 (19.1%) were performed by hand surgeons, with the remaining 72 (80.9%) performed by general orthopaedic surgeons. The 58 cases where an extra-articular or a juxta articular plate was actually used were all performed by general orthopaedic surgeons. There were 90 variable angle screws used in total for the 250 cases, 85 (94.4%) by hand surgeons and five (5.6%) by general orthopaedic surgeons.
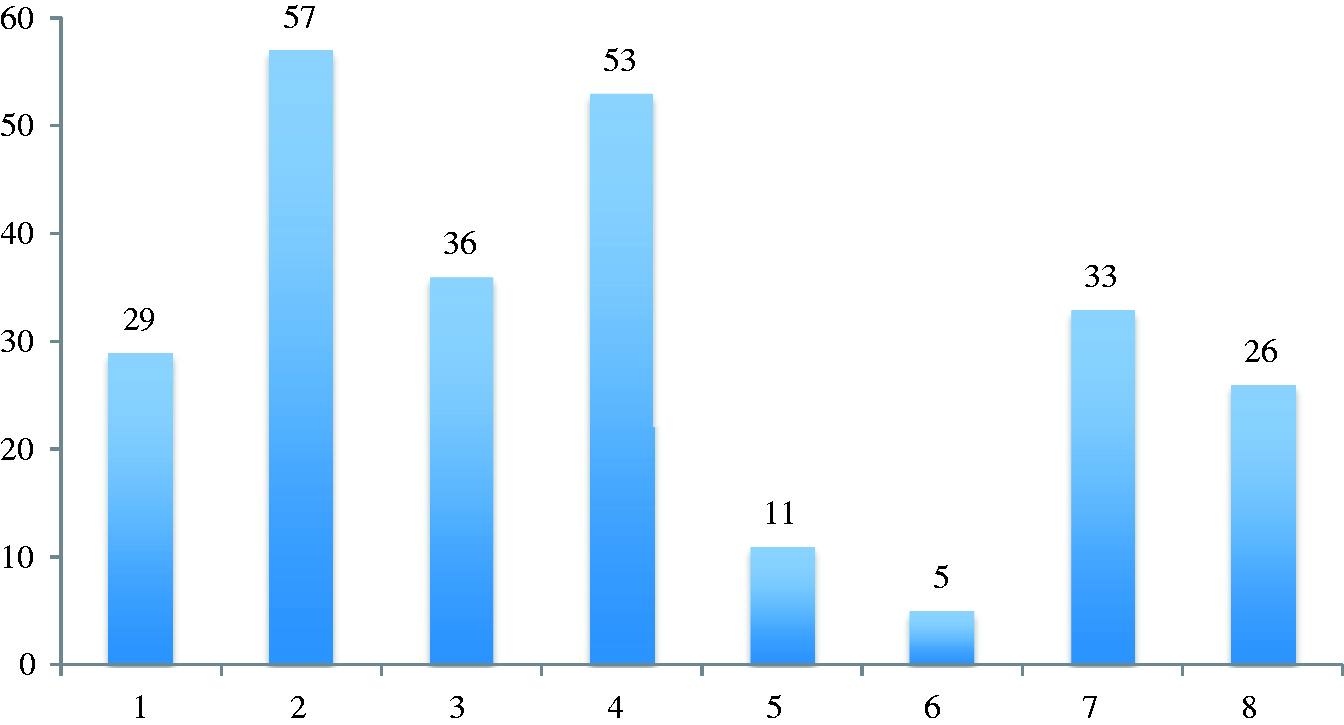
In the 58 cases where the extra-articular and juxta-articular plates were used, a mean number of 4.17 distal screws were used, with the mode number of screws being 4. Figure 1 shows the number of distal screws used in the 58 cases where an extra-articular or juxta-articular plate was used. In the 192 cases where a VA-LCP 2-column plate was used, a mean number of 5.9 distal screws were used.
Number of distal screws used in each extra-articular and juxta-articular case.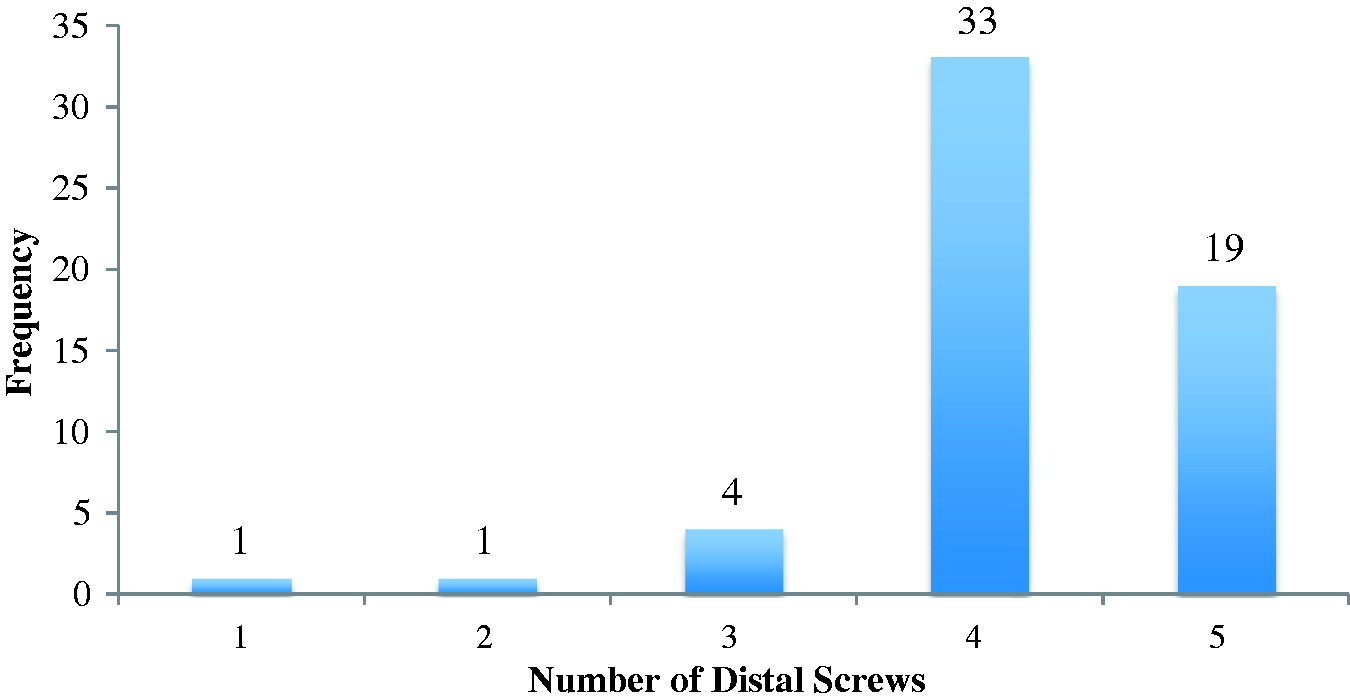
Figure 2 shows the range of AO classifications assigned to the 250 pre-operative X-rays and Figure 3 shows the Frykmann Grade assigned to the X-rays.
The range of AO classifications assigned to the 250 pre-operative X-rays. Frykmann Grade assigned to the 250 pre-operative X-rays.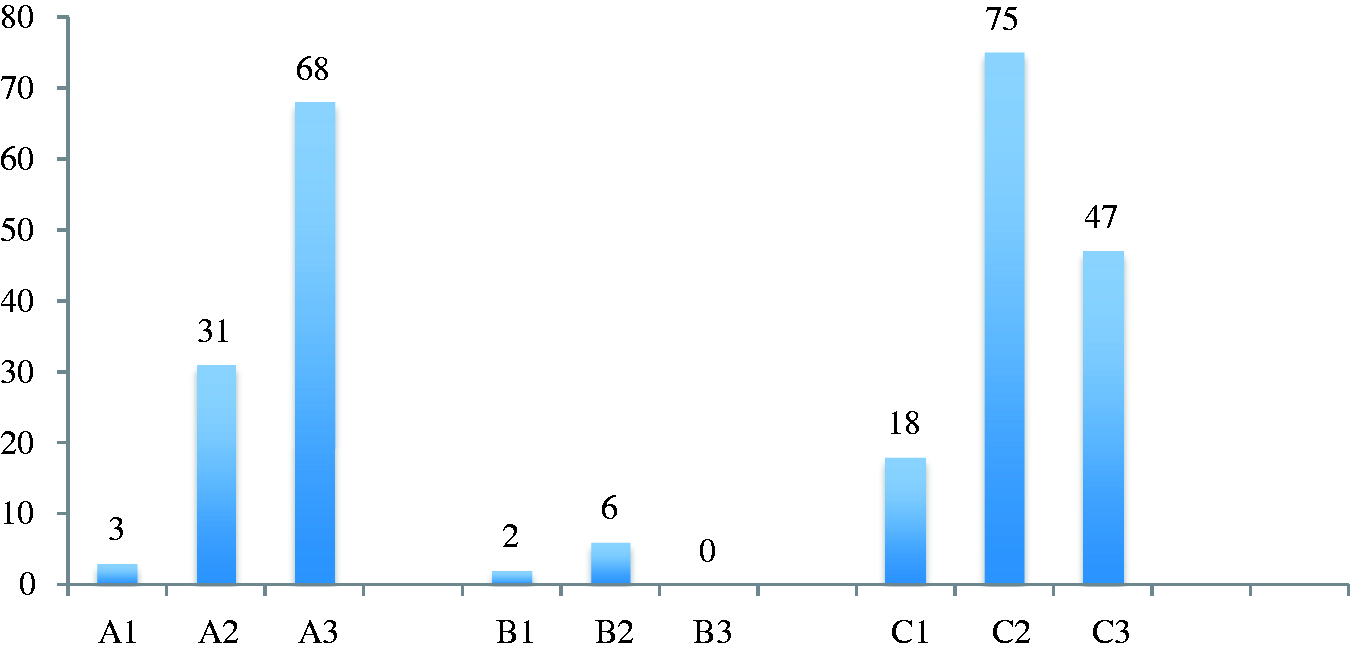
Using a set combination of an extra-articular plate with one cortical and two standard locking screws in the shaft and five distal locking screws theoretical savings of £11,830.50 were possible in those 89 cases where the extra-articular plate could have been used instead of using the VA-LCP 2-Column plate; if a similar combination with only four distal standard locking screws was used (which was the commonest configuration), then the potential saving was £19,224.60 (7.5%) over the two-year period.
Clinical outcomes at both 6 and 12 months post-operative were conducted for all 250 patients. A total of 28/250 patients (11.2%) required some form of further surgical intervention following the insertion of the volar plate; 24 required either removal of screws, or complete removal of metalwork. Indications included pain and stiffness, irritation of soft tissues and tenosynovitis confirmed on ultrasound scan caused by protrusion of screws. Two of these 24 patients had removal of metalwork due to complications associated with a secondary wrist trauma and not the insertion of the volar plate. The other four who required surgical intervention, did not have removal of any metalwork, but underwent median nerve neurolysis, carpal tunnel decompression, flexor pollicis longus tenolysis and median nerve block for complex regional pain syndrome.
With regard to plate type, 5/28 patients requiring secondary surgical intervention had either an extra- or juxta-articular plate inserted, comprising 8.62% of the 58 patients who had a simpler design plate inserted. Furthermore, 23/28 (82.1%) patients requiring secondary surgical intervention had the more complex variable angle plate inserted, equating to 12.0% of all the 192 patients who originally had a more complex volar plate inserted; 11/23 (47.8%) of those who had further surgical intervention following insertion of the more complex plate were patients who were deemed suitable for a simpler plate.
Discussion
It is reassuring that the vast majority of the variable angle screws (94.4%) were inserted by specialist hand surgeons. This would imply that the referral process in place appears to be adequate and the more complex fractures are being dealt with by specialist hand surgeons. We would therefore advocate that variable angle plates and screws should only really be used in complex fracture pattern types, ideally by specialist upper limb surgeons familiar with these types of fractures, ideally where it is anticipated the variable angle option will be required. We accept that there may be limitations placed on surgeons by trusts in only stocking certain plates for convenience of stocking, but whilst this is beyond the surgeon’s control, costs could still be controlled by only using the necessary number of screws to stabilise the fracture rather than filling all the distal locking holes. By simply reducing the number of distal locking screws used from seven down to five in a locking plate, over £100 per case could be saved without necessarily affecting patient outcomes. The supplier used by our trust (Synthes) has updated their stock and pricing, since this study data were collected and if the new pricing structure were applied to the data, then annual savings of £19,667 would be possible, which equates to a 15.4% cost reduction, which is well above the 5% expected by the Department of Health.
Over three quarters of those need further interventions had the more complex variable angle plate inserted. It may be that those receiving a more complex 2 column/variable angle plate did so as they had a higher energy, more complex injury, and were therefore always more likely to develop complications; however, 11/23 (47.8%) were patients who were deemed suitable for a simpler plate, which suggests that complications may be related to construct design, for example, inappropriate placement of variable angle screws, rather than due to the injury pattern alone.
Conclusion
It is clear from our data that many distal radius fracture patterns are being ‘over-treated’ with complex locking plate designs with multiple rows of screws and that substantial cost savings could be made by selecting an appropriate plate and screw number to suit the fracture pattern.
We have shown that if a rational approach is taken to plate and screw selection in the fixation of distal radius fractures then significant cost savings are possible – in this example, savings of up to £19,224.60, with potential savings in the future of up to £39,334.20. Whilst we are not advocating any change in clinical practice or the type of fixation technique when treating distal radius fractures, where a decision has been made to fix a fracture with a volar plate and screw fixation, we would certainly strongly recommend more consideration to the type of plate used to stabilise these fractures and a greater understanding of the number and placement of screws required in each case to achieve a stable construct. If this approach were to be used, then the cost savings within orthopaedic departments across the country and for the NHS as a whole may be significant.
Footnotes
Acknowledgements
The authors attribute this work to The Birmingham Hand Centre.
Ethical Approval
Ethical approval was not sought for the present study because the study was a retrospective review of intra-operative imaging studies and was performed following institution audit registration and oversight. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was not sought for the present study because it involved anonymised review of radiographic imaging and case notes as part of a registered routine clinical audit.
Provenance and peer review
Not commissioned, externally peer reviewed.