
Abstract

Abdominal trauma in children is uncommon, with potentially serious consequences and difficult diagnosis. Focused Assessment with Sonography for Trauma (FAST) has good sensitivity and specificity for hemoperitoneum and intra-abdominal injuries. 1 The Blunt Abdominal Trauma in Children (BATiC) score uses Doppler ultrasound, abdominal signs, hemodynamic stability and blood analysis to define the risk of intra-abdominal injury. A cut off point of 6 on this scale provides a high negative predictive value (100%) and 100% sensitivity for injury detection, 2 meaning that a stable patient with low BATiC and normal ultrasound would not need hospital admission or CT.1,2
In our urban pediatric hospital serving a local population of approximately 278,000 children there were 98,402 attendances to our emergency department in the last year, of whom only 40 presented with abdominal trauma (0.04%). Twenty-four (60%) were boys, the median age was 6.5 years (IQR 5–11) and 40% (16) required admission: 7/16 into the intensive care unit, 5/16 onto an observation ward (less than 48 h stay), and 4/16 were hospitalized to a ward, with a median overall stay in hospital of 192 h (IQR 30–321.8 h). The mechanisms of injury were traffic accidents in 32.5% (13/40), fall from a height 17.5% (7/40), fall from standing 15% (6/40), swing 15% (6/40), or bicycle 12.5% (5/40), bullying 5% (2/40), and maltreatment 2.5% (1/40).
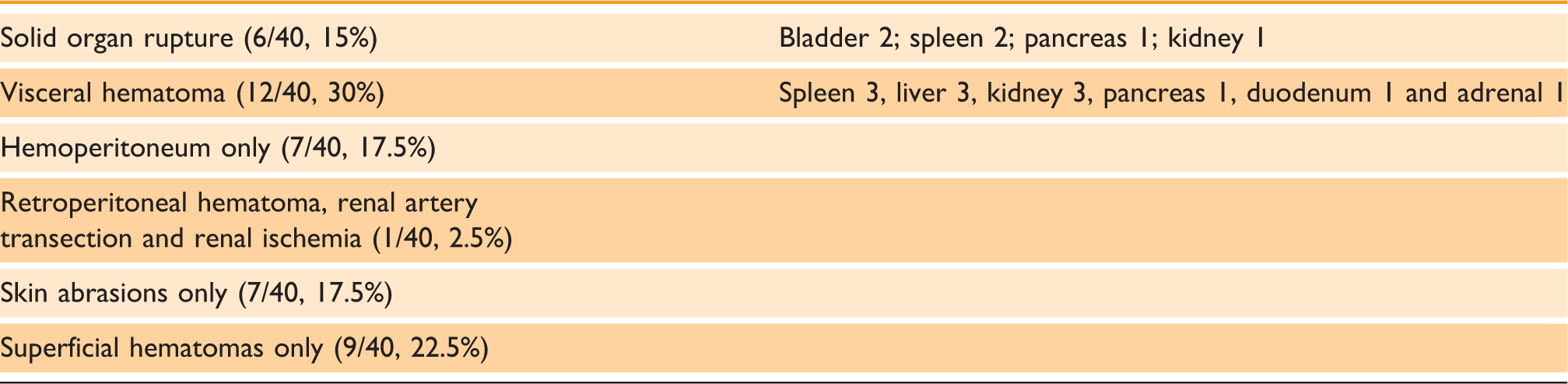
List of injuries identified.
There was only one case of delayed diagnosis (of a kidney hematoma) at 24 h after an initial normal ultrasound scan. The treatment was surgical on one occasion with nephrectomy for renal pedicle rupture and conservative treatment with analgesics and rest in 28/40 cases (70%). Three patients required a transfusion, and in one of these cases required mechanical ventilation. In 9/40 cases (22.5%) no treatment was required. The outcome in all cases was excellent with no mortality or significant morbidity.
These data, in common with other published articles, 3 do not show a correlation between severity and the mechanism of injury. Although CT is the gold standard in adult trauma, sonography can be a good alternative in children. The BATiC score should be used routinely for deciding when a CT is needed; so in our experience with BATic score: 5/6 CT were pathologic. Blood analytics such as transaminases or amylase seem to be useful tests for visceral injury, but more studies are necessary. In our sample most children with abdominal trauma were managed conservatively with excellent outcomes.