
Abstract
Introduction
Major trauma centres are effective in reducing morbidity and mortality rates following serious injury. Many patients attending major trauma centres present with traumatic brain injuries, requiring specialist assessment in screening for potential cognitive deficits. Numerous cognitive screens exist but it is currently unclear which are used most frequently within major trauma centres. This study aimed to identify which screening tools are used most frequently in major trauma centres in England to enable discussion around their suitability for this clinical population.
Method
Electronic surveys were distributed via a mailing list to Clinical Psychologists and Clinical Neuropsychologists in major trauma centres across England to gather data on the use of cognitive screens.
Results
Fourteen Clinical Psychologists in Neuropsychology participated. Results suggest major trauma centres in England are currently using the ACE-III (50%) or MoCA (42%) as the most frequently used screens for cognitive difficulties following traumatic brain injury. Cognitive screening pathways are multi-disciplinary involving OTs (86%), psychologists (qualified 79%; assistant 57%) psychiatrists (36%), mental health nurses (7%) and therapy assistants (7%).
Conclusions
Major trauma centres are using evidence-based cognitive screens at present, but further work is needed to develop more effective, better validated cognitive screens for traumatic brain injury populations. Increased inter-professional discussion on the practice of cognitive screening would be beneficial for patients seen within major trauma centres.
Introduction
Major trauma
Major trauma describes serious injuries that are life changing and could result in death or serious disability, including traumatic brain injuries (TBIs), severe wounds and multiple fractures.1–3 There are currently 27 major trauma centres (MTCs) providing specialised trauma care and rehabilitation to adults and children in England, with one planned for Wales. 4 Major trauma is the most common cause of death in people aged under 45 and as a result, the NHS has identified major trauma as a problem for public health. 5 The major trauma network was implemented in 2012 in England and has resulted in a 19% improvement in the chance of surviving a major trauma. 6 The process of care for a major trauma requires excellence during each part of the pathway: from initial contact with the patient and pre-hospital assessment, through to acute trauma care and both acute and general rehabilitation.1–3,7
TBI
Annually, 1.4 million people present to emergency departments in England and Wales with a recent head injury and 200,000 of these are admitted to hospital, with one-fifth potentially having skull fracture or evidence of a TBI. 8 The majority of people presenting with a TBI present with a normal or minimally impaired consciousness level (Glasgow Coma Scale [GCS] greater than 12)8,9; however, even mild TBI can result in cognitive and behavioural deficits. Patients with TBI can present with impairment in a variety of cognitive domains including executive functioning, memory, attention, and perception. 10 Identifying patients experiencing cognitive impairment assists in clinical management, determines the need for therapeutic interventions, and refines resource allocation. 8
Awareness of cognitive impairment is the responsibility of all members of the multi-disciplinary team (MDT) in a MTC. Assessment of cognitive impairment ranges from short, structured measures such as the GCS, 9 through to monitoring post-traumatic amnesia (PTA), administering cognitive screens, or engaging patients in in-depth neuropsychological testing. A holistic, person-centred approach to assessment incorporates clinical histories, clinical interviews with patients and/or family members, behavioural assessments, and functional assessments alongside cognitive screens. 11 This range of assessments serves to inform MDT opinions regarding recovery, mental capacity assessments, rehabilitation, patient flow, onward referrals and discharge destination, and a return to meaningful life following TBI.
A high proportion of patients seen within an MTC will have the potential for cognitive impairment by the nature of their illness or injury. Caseloads can be high, turnover on acute wards can be high, and services may experience pressures such as funding cuts or low staffing levels. To meet the cognitive needs of large populations within this challenging context, there is a need for quick to administer measures which can identify people in need of more in-depth assessment and intervention such as neuropsychological assessment and cognitive rehabilitation.
The nature of cognitive impairment caused by TBI causes difficulties in developing screening tools, as individuals may experience highly specific deficits in one area (e.g. anomia), with other cognitive functions intact, through to widespread damage across multiple cognitive domains. 10 As a result, it is important to consider how to screen for cognitive changes in MTCs following a TBI, the place of cognitive screens within a MTC pathway and the importance of using tools within MTCs which are evidence-based, freely available, and can meet the needs of a MT population.
Cognitive screens
There are many tests designed to provide a brief screening assessment of cognitive functioning. 12 There is no definitive or agreed definition of a ‘screen’, although Cullen et al. 13 defined a cognitive screen as one that was designed to, or had been used to, screen for cognitive impairment and took < 20 min to administer. Screens are commonly expected to sample multiple cognitive domains.
Cullen et al. 13 identified and reviewed 39 brief cognitive screens, many of which were designed for the assessment of older adults, 14 not TBI populations. A criticism of all screening tests is that due to their broad remit and time-limited nature, they may fail to identify all patients experiencing subtle cognitive impairment and may incorrectly classify patients without cognitive impairment as impaired, due to a range of confounding factors. Test selection and interpretation of results therefore need careful consideration.
Within MTCs, the priority for cognitive screening is to identify strengths and weaknesses across multiple cognitive domains, to guide further assessment and treatment including: (1) Supplementing other functional assessments and behavioural observations; (2) Monitoring recovery and treatment effects; (3) Informing neuropsychological assessments; (4) Identifying patients who would benefit from further inpatient or community neurorehabilitation; (5) Informing discharge planning.
In order to do this, there are a number of important factors to consider
10
:
Psychometric properties of tests including reliability, validity, sensitivity and specificity; The demographic characteristics of the populations in which they were developed and validated; Ability of the test to account for additional considerations (e.g. pre-morbid difficulties, pre-morbid personality, comorbidities, aphasia, atypical schooling); Cost; Administration format and time (including the relevance of the setting they were developed in, e.g. inpatient bedside vs. outpatient clinic); The qualifications and or experience required for test administration.
To date, there is no guidance on the use of cognitive screens within MTCs or an international ‘gold standard’.1,2,7,8 This study aimed to identify which screening tools are used most frequently in MTCs in England to enable discussion around their suitability for this clinical population. We hypothesised that MTCs in England would be using widely available cognitive screens which may not have been originally intended for use with a TBI population.
Method
Survey
Survey questions.
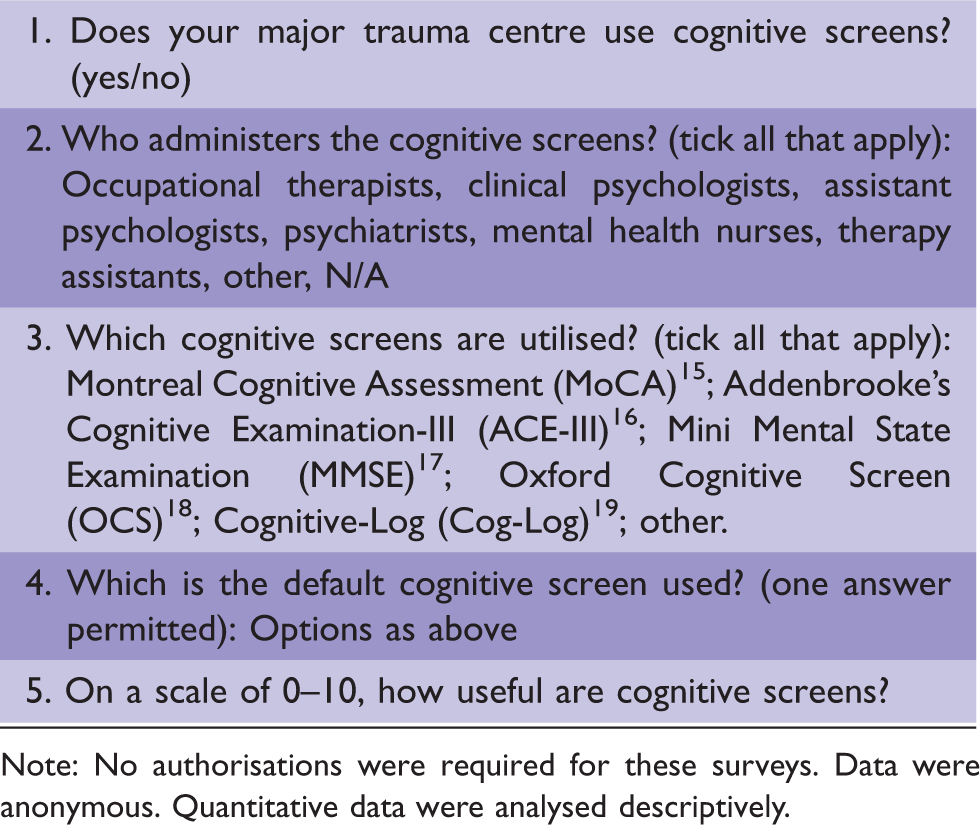
Note: No authorisations were required for these surveys. Data were anonymous. Quantitative data were analysed descriptively.
Results
Fourteen psychologists from 27 invited MTCs in England completed the survey (52% response rate) and all respondents reported that cognitive screens were used in their MTCs. Participants were asked to rate the usefulness of cognitive screens on a scale of 0 (not at all useful) to 10 (essential) and the mean perceived usefulness was 8.29 out of 10 (SD 1.07).
The most frequently used cognitive screens in MTCs in England (using the definition of cognitive screen provided by Cullen et al. 13 ) were the Addenbrooke’s Cognitive Examination-III (ACE-III) 16 (50%) and the Montreal Cognitive Assessment (MoCA) 15 (42%), followed by ‘Other’ tests of cognition (8%) provided in a free text answer. On analysis, the cognitive screens referenced under ‘Other’ related to screens used in paediatric settings (Children’s Cognitive Screening Instrument (CCOSI) 20 and Children’s Orientation and Amnesia Test (COAT) 21 ).
These results supported the hypothesis that MTCs would be using widely available cognitive screens (ACE-III and MoCA), but which were not originally intended for use with a TBI population (dementia and stroke, respectively).
Cognitive screen demographics.
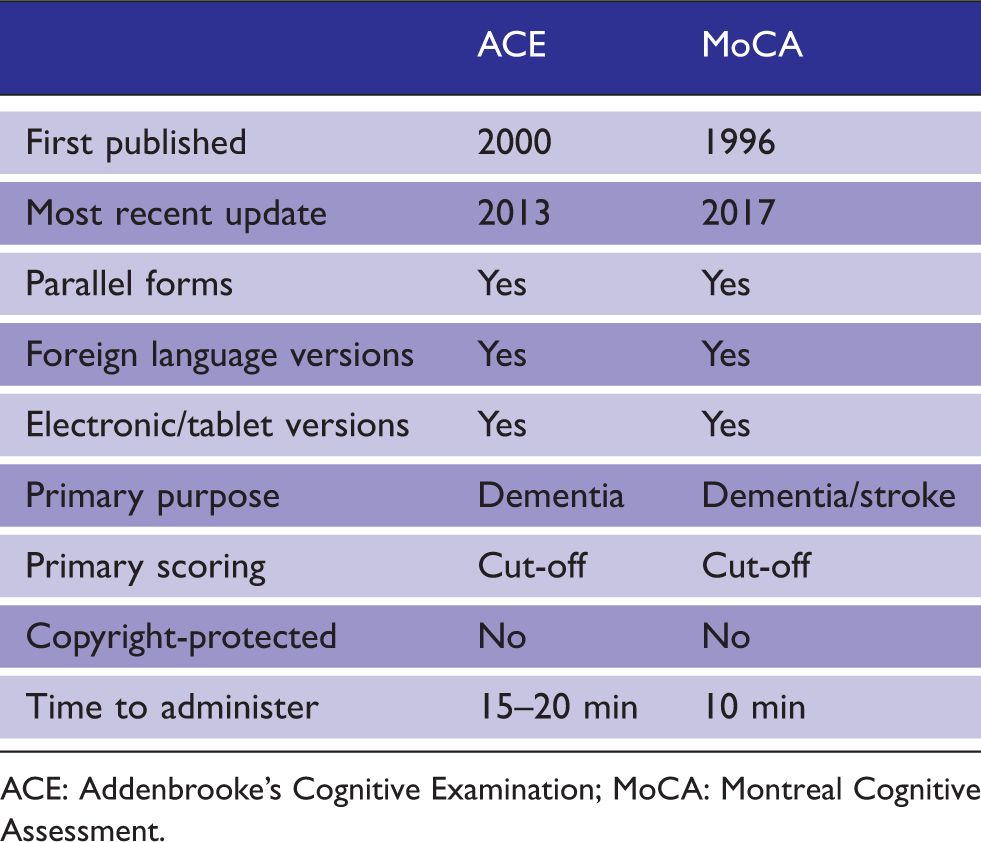
ACE: Addenbrooke’s Cognitive Examination; MoCA: Montreal Cognitive Assessment.
Domains covered by cognitive screens.
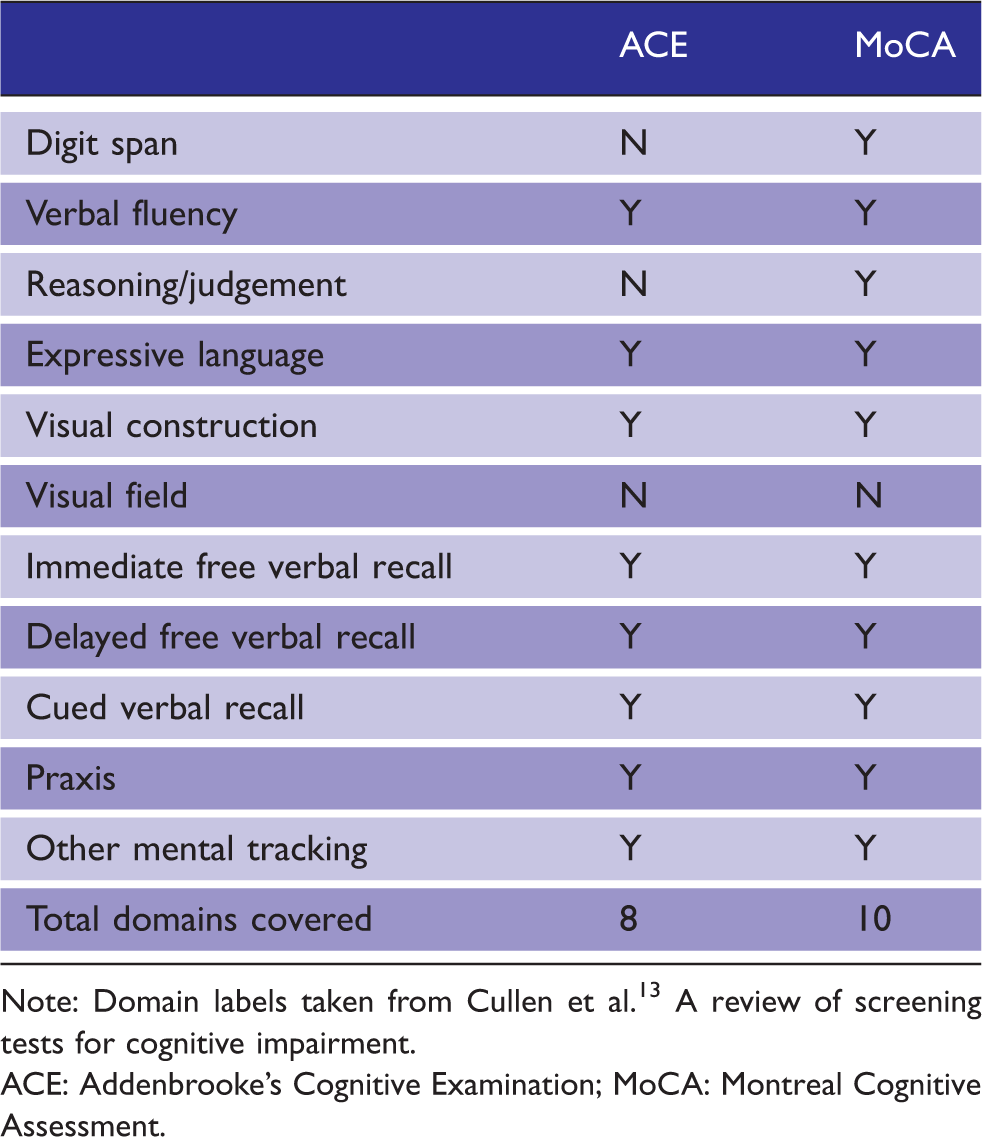
Note: Domain labels taken from Cullen et al. 13 A review of screening tests for cognitive impairment.
ACE: Addenbrooke’s Cognitive Examination; MoCA: Montreal Cognitive Assessment.
OTs (86%) and psychologists (qualified 86%; assistant 57%) were the MDT members most commonly completing cognitive screens in MTCs, followed by psychiatrists (36%), mental health nurses (7%) and therapy assistants (7% (Figure 1).
Occupations administering cognitive screens in major trauma centres (MTCs).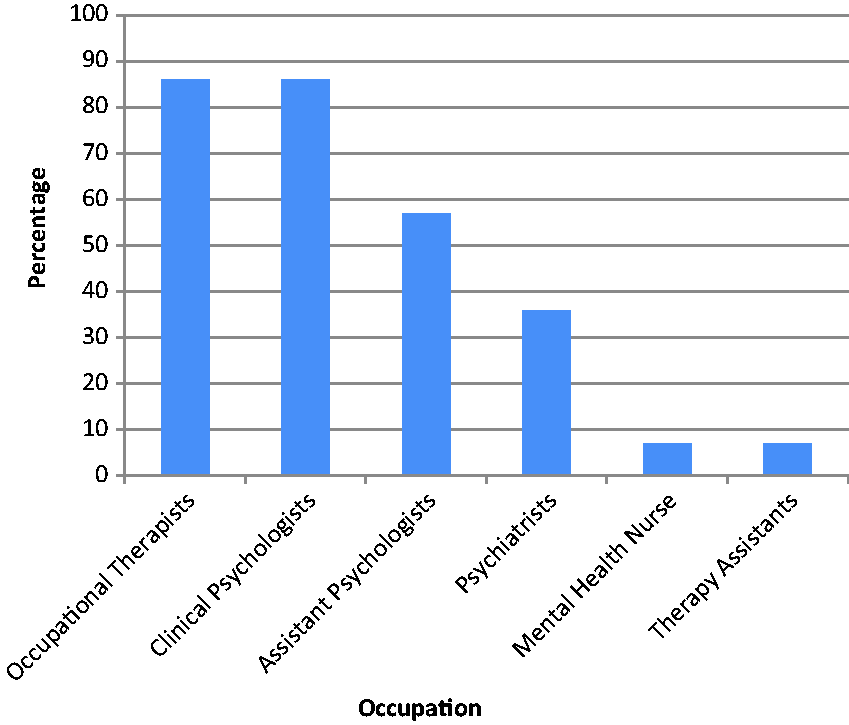
Discussion
Cognitive screens provide a method to screen large numbers of patients for potential sequelae of TBI and are perceived as valuable for assessment and care planning by psychologists within MTCs in England. Both of the most frequently used screening tools identified in this survey (ACE-III and MoCA) are free, simple and quick to administer (<20 min) and address multiple areas of cognition. They have additional utility in that they are flexible, multi-purpose, and have parallel forms and foreign language versions. One difficulty with both these screens is that they are not currently able to account for premorbid factors or comorbidities such as expressive communication difficulties. They should be used in combination with communication, functional and behavioural assessments with the option for consultation with neuropsychology where appropriate.
Evidence from the literature supports the use of the screening tools identified in this survey. Studies suggest that both the MoCA and the ACE-R (previous version of the ACE-III) are more sensitive than the MMSE in brain injury populations22,23 and that the MoCA can be used serially to detect statistically reliable change over time. 24
However, the screening tools commonly used within MTCs in England (MoCA and ACE-III) were both originally designed to screen for dementia. The discrepancy between the target use and current use of this measures means that these screening tools may not be equally effective with all types of cognitive impairment, e.g. patients with damage to their frontal lobe(s) may do well on this type of test while showing clear difficulties in everyday life. 25
Currently, we are exploring the use of the Brain Injury Cognitive Screen (BICS) 26 with people with TBI, and the Oxford Cognitive Screen (OCS) 18 for people with TBI and aphasia. 27 The BICS was developed for use in MDT assessment of patients with TBI early in rehabilitation 28 and is sensitive to changes in areas commonly affected in brain injury, including memory, attention, processing speed, and executive function. It has emerging psychometric evidence 29 and is free for clinical use, although it takes longer to administer than most screens. It would be beneficial to compare the performance of the BICS against the ACE-III and MoCA for people with TBI. Zhang and Feinstein also propose a more sensitive combination of subtests for assessing cognitive impairment in TBI than the MoCA, namely the Stroop Test, the Symbol Digit Modalities Test, and a visual version of the Paced Auditory Serial Addition Test 2-second trials. 30
The OCS was designed for people with stroke. It is freely available, takes approximately 10–15 min to administer, and accounts for aphasia and visuospatial neglect by using short, high frequency words, forced-choice response formats, vertical layouts, and multimodal presentations. It is not currently copyright protected and is has parallel forms, foreign language versions and electronic/tablet versions. It explores the domains of attention, memory, language, praxis and use of number. Demeyere et al. 31 compared the OCS and MoCA and found that the OCS had higher sensitivity than the MoCA, detected impairments in multiple domains which were undetected by the MoCA; and could be used with a larger number of patients than the MoCA, due to aphasia adaptations.
This survey identified that a variety of professionals administer cognitive screens within MT. Neither the ACE-III nor the MoCA require specialist education or training to administer. However, considerations regarding the administration and interpretation of scores may benefit from discussion and consultation with staff with specialist knowledge (e.g. Clinical Neuropsychologists). Further online training should be considered32,33 as without training there may be a large margin of error. Cognitive screens should be administered in combination with more ecologically valid functional assessments such as the Multiple Errands Test 34 adapted for hospital settings 35 and kitchen assessments. Cognitive screening within MTCs is dependent on MDT working and may vary within centres. Consequently, there is need for increased discussions across professional groups regarding cognitive screening tools and pathways. There is potential for greater inter-disciplinary teaching/training on cognitive assessment.
Future research should investigate the assessment of cognition across MT pathways, especially as confidence and knowledge may vary outside MTCs, and it has been established that patients with mild head injuries with other MT comorbidities may be admitted to wards with different specialities which may not have clear pathways for cognitive assessment. 36 The development of consistent pathways based on evidence would improve patient care, and could then be integrated into future National Institute for Health and Care Excellence (NICE) or international guidelines regarding cognitive screens in MTCs.
There is a need to develop pathways for recommended PTA, mood and cognition assessments in an MTC, mirroring the UK pathway for mood and cognitive assessment used in stroke. 37 Within the Trauma Audit and Research Network (TARN) database in England and Wales, cognitive data are collected subjectively via Functional Independence and Functional Assessment measures 38 and Northwick Park Therapy Dependency measure of therapy input 39 evaluations, but no direct measurement of cognitive screening is audited (as in national stroke pathways). This information may need to be captured as part of a rehabilitation prescription.
Strengths and limitations
The use of an open-ended question within the survey was designed to capture maximum information on this under-researched topic. However, this resulted in some answers which were not possible to review within the scope of this article (e.g. best practice for the five paediatric MTCs in England) or answers with multiple components (e.g. a combined measure of PTA and ACE-III). The use of the Cullen criteria resulted in the omission of some potentially valuable cognitive screens (e.g. the BICS) which should be incorporated in further research. Although this study obtained a response rate equal to or greater than many survey-based studies, overall the sample size is small and may not be representative of all MTCs. Further research should aim to ensure representation and increase knowledge through increased sample sizes, more in-depth research methods (e.g. qualitative interviews) and a greater breadth of multi-disciplinary participants including other therapy, nursing and medical professionals. This will enable the possibility to explore any differences in practice and the perceived usefulness of specific cognitive screens. Given the key role played by Occupational Therapists in administering cognitive assessments during the acute phase of admission, this survey should be replicated with this professional group to capture their experience and expertise.
Footnotes
Acknowledgements
None.
Contributorship
AT and HW designed the study and AT led on data collection. AM and AT wrote the first draft of the manuscript, all authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study as the Health Research Authority decision tool (recommended by the employing hospital’s R & D department) identified that this study did not require NHS REC approval. Participants were NHS staff and data were collected anonymously.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AT.
Informed consent
Written informed consent was not sought for the present study because participants implied consent for their anonymous data to be used through completion of the online survey.
Provenance and peer review
Not commissioned, externally peer reviewed.
Trial registration
Not applicable.