
Abstract
Aims
The aims of this study were to describe the profile and longer-term outcomes of major trauma patients with unstable open pelvic fractures.
Patients and methods
An observational study was performed using data from the population-based Victorian State Trauma Registry. Adult (≥16 years) major trauma patients who had sustained an unstable open pelvic fracture between 1 July 2010 and 30 June 2017 in Victoria (Australia) were included. Patient demographics, injury event, severity and management data were extracted. Patients were followed up at 6, 12 and 24 months post-injury to collect information about health status, function and return to work.
Results
There were 67 patients. The mean (SD) age was 41.4 (18.3) years, and 66% were male. Seventy-six per cent were road traffic injuries, 96% were managed at Level 1 trauma centres and all were multi-trauma patients. A third were Tile C fractures and 80% underwent surgical stabilisation of the pelvic injury. Eighty per cent were admitted to intensive care. The in-hospital mortality rate was 9%. Most (89%) survivors were discharged to an inpatient rehabilitation facility. The proportion classified as ‘severe disability’ on the Glasgow Outcome-Scale Extended declined from 38% at 6 months to 19% at 24 months. The overall three-level EuroQoL five-dimensional instrument score increased with time indicating better health status, and 50% of patients returned to work by 24 months.
Conclusions
Major trauma with unstable, open pelvic fracture is rare. Low in-hospital mortality was observed. Most survived to hospital discharge and outcomes improved with time post-injury, but 75% of patients experienced persistent pain and ongoing mobility and activity restrictions.
Introduction
Open pelvic fractures, where the fracture directly communicates with a wound of the skin, rectum or vagina, are uncommon, rarely occur in isolation, are often life threatening, and are complex to manage due to the risk of haemorrhage and sepsis resulting from injury to major blood vessels and retroperitoneal organs.1,2 These injuries are diverse in presentation and are predominantly sustained in high-energy incidents such as road traffic crashes and falls from height.
In-hospital mortality following open pelvic fracture has declined markedly over recent decades. Most patients now survive these severe injuries, often with the risk of life-long morbidity including loss of function, persistent pain and reduced quality of life. Kassam et al. described the morbidity associated with open pelvic fracture as ‘undoubtedly high’, 2 but few studies have investigated the longer-term patient-reported outcomes of survivors of open pelvic fracture.3–8 Recent data are notably lacking.
Previous studies have been single-centre studies with retrospective follow-up of patients at inconsistent timeframes after injury. Brenneman et al. studied the health-related quality of life, pain and return to work outcomes of 33 survivors from a single Canadian trauma centre at an average of four years post-injury. 3 The retrospective cohort study by Vallier et al. of women with severe pelvic ring fracture included just four cases of open pelvic fracture and follow-up ranged from 12 to 46 months post-injury.5,6 The outcomes of 15 survivors of open pelvic fracture were abstracted from the patient medical record at an undefined timeframe post-injury by Ferrera and Hill, 4 whilst Hermans et al. described the clinical outcomes only, at a mean of six months after injury, in a cohort of 24 cases from The Netherlands. 9 Giordano et al. reported the health status outcomes of 11 of 18 survivors as ‘satisfactory’ at a mean of 16 months post-injury. Therefore, the aims of this study were to describe the profile and longer-term outcomes of major trauma patients with unstable open pelvic fractures using prospectively collected data from a population-based trauma registry.
Patients and methods
Setting and design
Victoria is Australia's second most populous state with a population of 6.3 million and has a regionalised trauma system. Pre-hospital triage and inter-hospital transfer guidelines dictate the transport of injured patients to the most appropriate centre. The system includes a single ambulance service and three Level 1 trauma centres (two adult and one paediatric), and is monitored using the population-based Victorian State Trauma Registry which collects data about all major trauma patients in the State.10,11 Major trauma is defined if any of the following are present; death following injury, an Injury Severity Score (ISS) >12, admission to an intensive care unit (ICU) for >24 h, and urgent surgery (intracranial, intrathoracic, intraabdominal, and fixation of pelvic or spinal fractures). The registry collects data from all patients arriving at any of the 138 trauma-receiving hospitals in the State, including deaths on arrival and deaths in the emergency department. Pre-hospital and acute care setting data are collected. All survivors to discharge are followed-up by telephone at 6, 12 and 24 months post-injury.12–14 The registry has ethics approval from the ethics committees of the Department of Health and Human Services, Monash University, and trauma-receiving health services.
Patients and procedures
Adult (≥16 years) major trauma patients with an unstable open pelvic fracture and a date of injury from 1 July 2010 to 30 June 2017 were included in this study. Demographic and injury event details, relevant clinical observations, diagnoses, injury severity, procedures and operations, in-hospital outcomes, and data collected at the 6-, 12- and 24-month follow-up time points, were extracted. Unstable open pelvic fractures were identified from the Abbreviated Injury Scale coding (AIS) and checked against the text injury descriptors. The registry uses trained and accredited AIS coders who undertake a detailed examination of the medical record documentation, radiology and surgical reports to assign codes to all injuries sustained. The unstable pelvic fracture codes were:
i. Open pelvic ring fracture, incomplete disruption of posterior arch, partially or vertically stable (856162.4) ii. Open pelvic ring fracture, complete disruption of posterior arch, fracture is totally unstable (vertical shear; 856174.5).
The AIS codes were used to allocate the ISS, and identify the presence of associated injuries, grouped according to AIS body region, with a severity score of 3 or greater considered serious. Rectal, vaginal, vulval and bladder injuries were also identified using AIS codes. Pre-existing conditions were mapped from the International Classification of Diseases 10th revision Australian Modification (ICD-10-AM) diagnosis codes to the Charlson Comorbidity Index (CCI), 15 whilst the patient's residential postcode was used to assign a level of socioeconomic disadvantage and geographic remoteness. The Australian Classification of Health Interventions (ACHI) codes were used to determine the pelvic fracture surgical management and associated procedures, including diverting colostomies.
Telephone interviews were conducted at 6, 12 and 24 months after injury to collect function, health status and return to work outcomes. Highest level of education, self-reported pre-injury level of disability and pre-injury work status were also obtained at the first follow-up interview. The 3-level EuroQoL five-dimensional instrument (EQ-5D-3L) was used to measure health status. 16 Each EQ-5D-3L item has three options: no problems, some problems and severe problems. Age and gender population weights (tariffs) are applied to the item responses to generate preference weights, resulting in a utility score ranging from −0.594 to 1, where 0 represents a health state equivalent to death, 1 represents perfect health and a score <0 is considered worse than death. The Glasgow Outcome-Scale Extended (GOS-E) measures overall function on a scale from 1 (death) to 8 (upper good recovery). 17 Whilst originally developed to measure head injury outcome, the GOS-E has been validated for use in multi-trauma populations.18,19 Return to work status (yes/no) was collected from patients who were working or studying prior to injury. A pelvic fracture outcome score was not used as these are not validated in multi-trauma patients20–22 and injury-specific measures are known to discriminate poorly between functional loss related to other injuries in multi-trauma. 23
Data analysis
Descriptive statistics were used to summarise the cohort. Mean and standard deviation (SD), or median and interquartile range (IQR), were used for continuous variables depending on the distribution of the variable. Frequencies and percentages were used for categorical variables. Categories were collapsed for some variables to avoid small cell counts and the potential for statistical disclosure. All analyses were performed using Stata Version 15.
Results
From July 2010 to June 2017, 67 major trauma patients with unstable open pelvic ring fractures were hospitalised in Victoria, Australia, averaging 9.6 per year. Figure 1 shows the flow of participants through the study. Table 1 shows the demographic and injury event profile of the cohort. The mean age of patients was 41 years and two-thirds were male. More than half had no CCI conditions, 79% were working prior to injury and 88% reported no pre-injury disability.
Flow of participants through the study. Demographic profile of patients with open pelvic ring fracture in Victoria (July 2010 to June 2017). n = 5 missing. n = 4 missing. n = 11 missing. n = 14 missing. n = 1 occurred in Victoria but location unknown.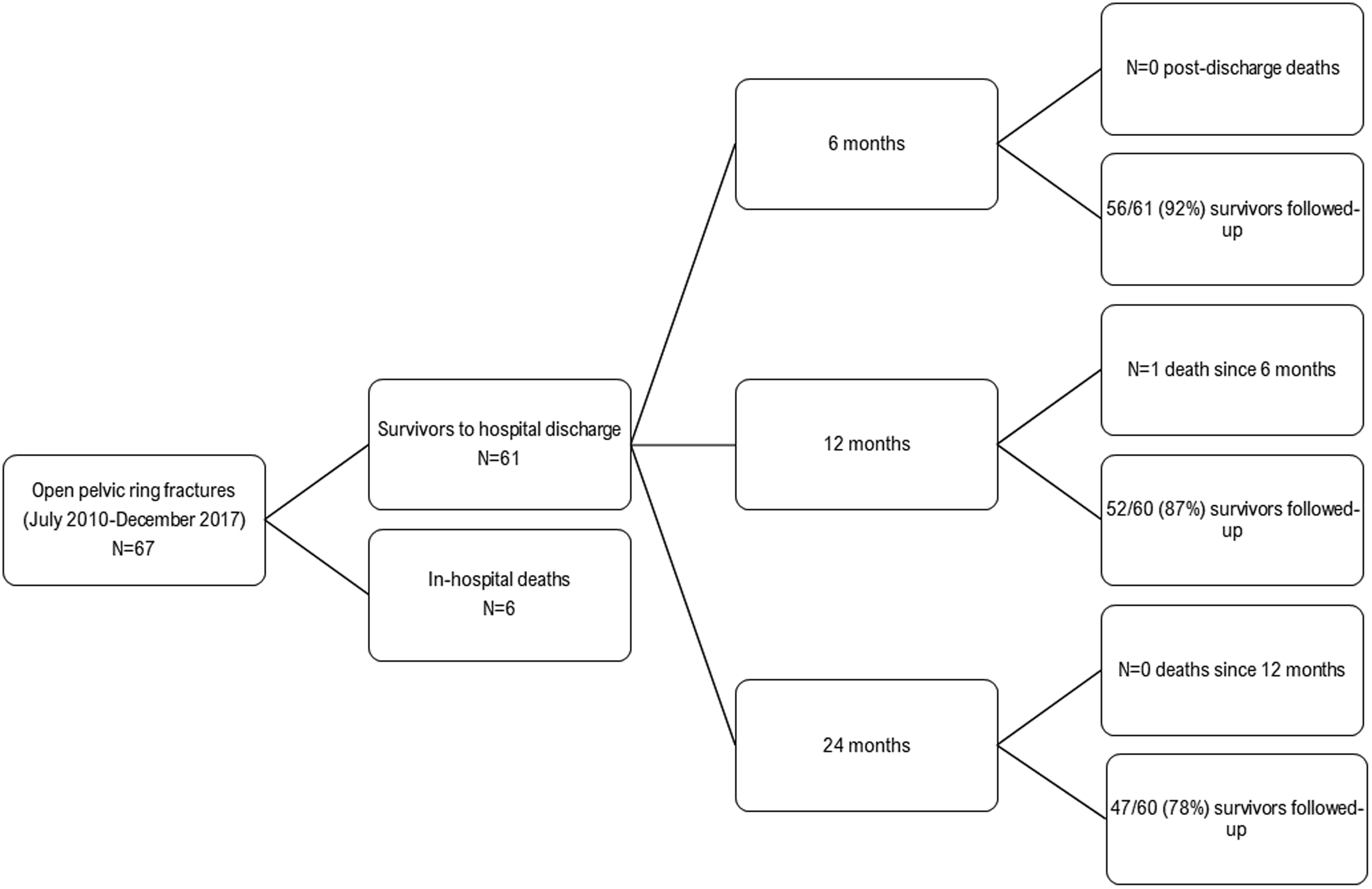

Most cases were due to unintentional (accidental) events. Eleven were intentional events of which 10 were self-harm (Table 1). Seventy-six per cent of cases were road traffic injuries – most commonly pedestrians, motor vehicle occupants and motorcyclists. ‘Other’ causes’ cases included firearm discharge, horse-related incidents, machinery and being struck by an object. The blood alcohol concentration (BAC) was known for 45 (67.2%) cases and was zero in 34 cases, detected but less than 0.05 g/100 mL in 3 cases and greater than 0.05 g/100 mL in 8 cases. Where the BAC exceeded 0.05 g/100 mL, seven were road traffic injuries.
Fifty-one patients were transported directly from the scene of injury to the hospital providing definitive care; 36 by road ambulance; and 15 by air ambulance (helicopter). Sixteen patients experienced an inter-hospital transfer. Six were transferred using the state's retrieval services and eight were transferred by the ambulance service (5 by road ambulance and 3 by air ambulance). Ninety-six per cent of cases received their definitive care at a Level 1 trauma centre.
Injury severity characteristics of patients with open pelvic ring fracture in Victoria (July 2010 to June 2017).
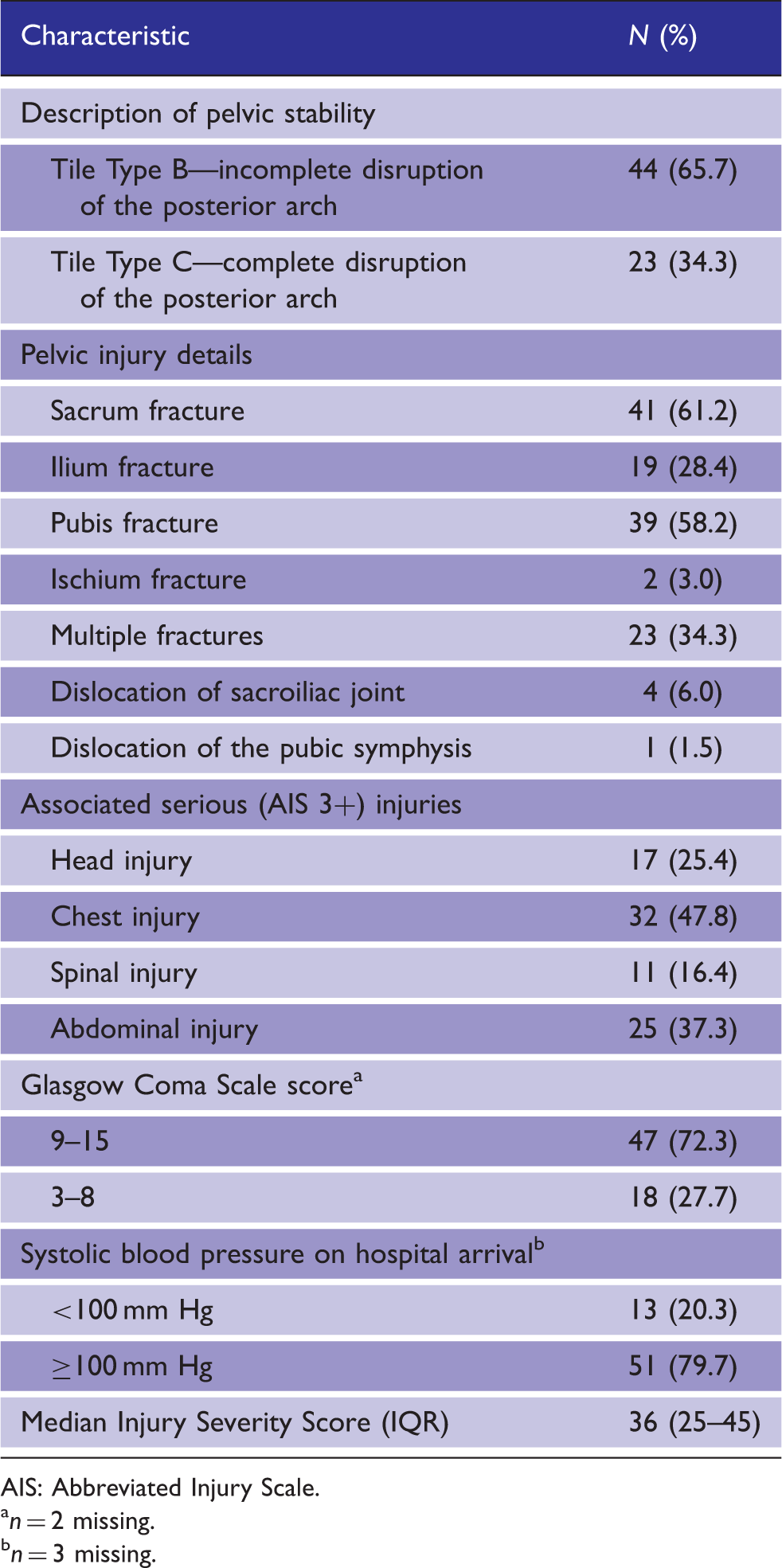
AIS: Abbreviated Injury Scale.
n = 2 missing.
n = 3 missing.
Eleven (16.4%) patients had sustained injuries to the urethra or ureter, and 12 (17.9%) had bladder injuries. No penile, vulva or vaginal lacerations were recorded, but eight had sustained lacerations to the perineum, four patients had anal lacerations and two had lacerations of the scrotum or testes. Seven (10.5%) patients sustained a rectal laceration, whilst six patients had colon lacerations, and one had sustained a laceration of the small intestine. Seven patients underwent a faecal diverting procedure. Liver and gall bladder (n = 11), spleen (n = 9) and kidney (n = 3) lacerations were also recorded in this cohort.
Pelvic injury management and in-hospital outcomes of patients with open pelvic ring fracture in Victoria (July 2010 to June 2017).
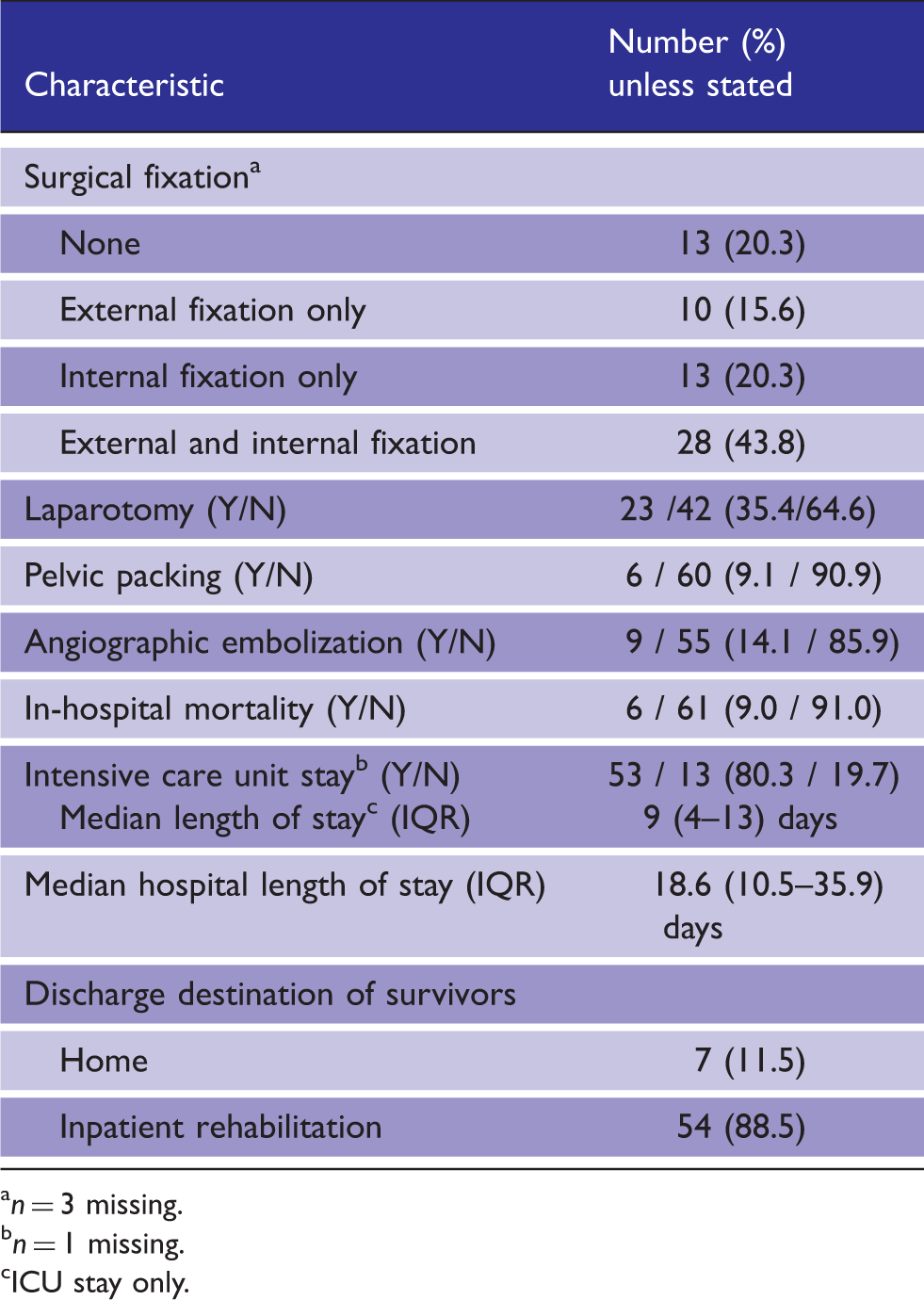
n = 3 missing.
n = 1 missing.
ICU stay only.
Longer-term outcomes of patients with open pelvic ring fracture in Victoria (July 2010 to June 2017).
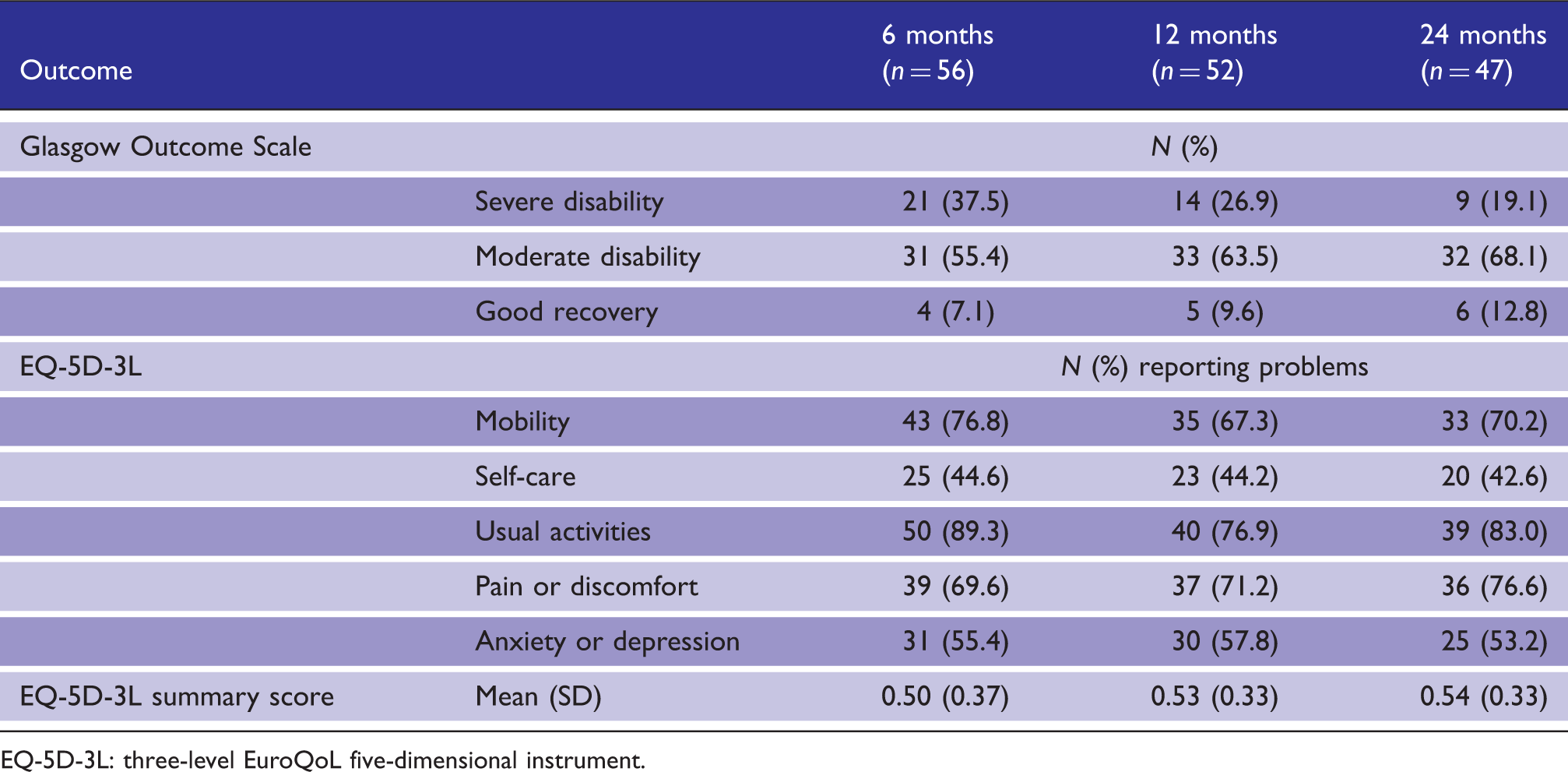
EQ-5D-3L: three-level EuroQoL five-dimensional instrument.
Discussion
Open pelvic fracture is a rare but potentially devastating injury, yet information about the longer-term outcomes of these patients is sparse. In this population-based, multi-centre study, undertaken in a mature, regionalised trauma system, we found low rates of in-hospital mortality, but significant sustained morbidity; 13% had achieved a good functional recovery, 17% reported no problems with usual activities, and 50% had returned to work, at 24 months post-injury. The findings reflect the long and challenging recovery for people who survive major trauma with an unstable, open pelvic fracture.
The estimated incidence of hospitalised, unstable open pelvic fracture was 0.02 per 100,000 population per year, highlighting the rarity of this injury type. The profile of the patient population was consistent with other studies; most patients were young, male and sustained their injuries in high-energy mechanisms including road traffic collisions and falls from height.3,4,8,9,24–30 However, there were differences. Most studies reported a mean ISS of 21 to 31,3,8,9,24,26–30 whilst the mean ISS in our patient population was 38. In our cohort, 14% underwent angiographic embolisation and 9% went to theatre for pelvic packing procedures. Eighty per cent underwent surgical fixation of the pelvic fracture, with 64% undergoing open reduction and internal fixation of the fracture. Brenneman et al. in their study of 44 open pelvic fractures found that 16% did not undergo surgical stabilisation, 3 whilst this rate was higher in the study by Hermans et al. where a third of patients' fractures were not operatively managed, 9 potentially reflecting the higher proportion of intrinsically stable Tile Type A fractures in the latter study. Others have not provided equivalent surgical management data for comparison.8,30 Consistent with recommendations, 1 all of our patients with rectal lacerations underwent a temporary colostomy.
Despite the higher overall severity of our cases, we observed an in-hospital mortality rate of 9%. Consistent with our findings, Hermans et al. and Siada et al., reported mortality rates of 4% and 16% in their single centre studies of 24 and 25 open pelvic fractures, respectively. 9 Others have reported mortality rates ranging from 16% to 45% for studies of open pelvic fractures.3,8,25,26,28,30–32 The lower rates of in-hospital mortality observed in ours, and other recent studies, potentially reflect improvements in the management of severe pelvic ring fractures specifically, and improvements in trauma care overall including improved uptake of inclusive trauma systems. Notably, 96% of open pelvic fractures in our study were definitively managed in the State's Level 1 trauma centres.
Previous studies have reported rates of discharge to inpatient rehabilitation ranging from 33% to 50%,3,9,30 compared to 89% of our cohort. The mean hospital LOS in our cohort was 27 days, which is consistent with previous studies which have reported mean LOS ranging from 19 to 44 days.3,8,9,30 The differences observed could reflect the higher overall severity of our cohort and potentially greater availability of inpatient rehabilitation allowing more rapid access to this specialist service.
Despite the low prevalence of self-reported pre-injury disability and pre-existing conditions, disability was prevalent after open pelvic fracture. Post-discharge mortality was rare but 87% of patients experienced either moderate or severe disability at 24 months post-injury. More than 70% of patients continued to report problems with usual activities, pain and discomfort and mobility at 24 months post-injury. Seventy-nine per cent of our cohort were working or studying prior to injury and the return to work rate was 50% at 24 months after injury. There was clear evidence of improvement in outcomes with time post-injury. Comparison with other studies is difficult as most studies did not assess longer-term outcomes at all. Where follow-up was undertaken, inconsistent time points post-injury were used ranging from an average of six months 9 to four years. 3 Ferrera and Hill reported that 7 of the 15 survivors of open pelvic fracture study experienced a ‘fair’ outcome and 8 were ambulating without assistance or were independent. 4 When and how these outcomes were measured was not described. Hermans et al. followed their cohort at an average of six months but measures of function and health status were not collected, with only clinical outcomes recorded. 9 Brenneman et al. reported a return to work rate of 64% at a mean of four years after injury. 3 Consistent with our study, they also observed marked reductions in general health, bodily pain and physical function using the 36-item Short Form Health Survey. Function was measured using the Functional Independence Measure (FIM) and the mean score at follow-up was 123 out of 126, suggesting little to no problems with activities of daily living. 3 Notably, the FIM has been shown to have low responsiveness and high ceiling effects in major trauma patients, limiting its usefulness as a follow-up tool. 33 Whilst comparison with other published studies of open pelvic fracture patients is limited, the prevalence of problems on the EQ-5D, functional loss and return to work rates observed show profoundly poorer outcomes than the wider major trauma patient population.13,14
To our knowledge, this is the only population-based study of the longer-term outcomes of major trauma patients with open pelvic ring fracture, and represents one of the largest cohorts of this uncommon injury. Missing data was low, and follow-up rates were high at each time point post-injury, especially for this type of cohort. However, limitations must be acknowledged. We used data from a population-based major trauma registry and identified unstable open pelvic fracture cases, their management and associated injuries using AIS, ICD-10-AM and ACHI codes. Stable open pelvic fractures were excluded, and individual record review was not undertaken, precluding additional classifications such as the Young–Burgess and Gustilo–Anderson, though inter-rater reliability of these classifications has been shown to be poor in severe pelvic ring fracture. 34 Nevertheless, using multiple data sources enabled cross-checking and confirmation, and the profile of patients was inherently similar to studies undertaken using both registries and individual record review. Follow-up was undertaken using outcome instruments validated for major trauma patient populations, but a specific pelvic outcome instrument was not used. Finally, despite the high number of patients studied relative to the literature, there were insufficient numbers to establish predictors of better or poorer outcomes of these patients.
Conclusion
Low in-hospital mortality following major trauma with unstable, open pelvic fracture in Victoria, Australia was found, reflecting coordinated early management. Most patients survived to hospital discharge and, despite the severity of this injury and the very high prevalence of multi-trauma, outcomes improved with time post-injury, with up to 50% returning to work by 24 months. However, major trauma with unstable open pelvic ring fracture remains a devastating injury with 75% of patients experiencing persistent pain and ongoing mobility and activity restrictions.
Footnotes
Declaration of conflicting interests
The author(s) declared no conflict of interest with regards to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BB was supported by an Australian Research Council Discovery Early Career Researcher Award Fellowship (DE180100825). PAC was supported by a National Health and Medical Research Council Practitioner Fellowship (545926). BJG was supported by an Australian Research Council Future Fellowship (FT170100048). The VSTR is funded by the Department of Health and Human Services, Victoria and the Transport Accident Commission.
Ethical approval
Ethical approval for this study was obtained from the Monash University Human Research Ethics Committee (Project ID 14882).
Informed consent
Informed consent was not sought for the present study as it used existing data from the Victorian State Trauma Registry, which collects data using an opt-out process.
Guarantor
BJG.
Contributorship
BJG, ME, IS and WV researched literature and conceived the study. All authors were involved in protocol development, and WV was involved in gaining ethical approval. BJG wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgements
We thank the Victorian State Trauma Outcome Registry and Monitoring (VSTORM) group for providing Victorian State Trauma Registry data.
Provenance and peer review
Not commissioned, externally peer reviewed.