
Abstract
Traumatic shoulder dislocation with proximal humerus fracture is a rare entity among children and treatment is always challenging. We present the case of a child with anterior dislocation of the shoulder associated with complete displaced proximal humerus metaphysis fracture. The fracture was treated by closed reduction using an innovative joystick technique and then fixation by two intramedullary K-wires. The dislocation was easily reduced after the fixation of the fracture. This method of treatment enables us to achieve excellent radiological and clinical results in a short time.
Introduction
Traumatic shoulder dislocation is rarely seen in children. 1 Fractures around the shoulder joint in young children tend to occur through the growth plate because of its relative weakness, and Salter-Harris type 1 and 2 injuries are commonly seen around the shoulder. 2 A combination of a fracture with dislocation is extremely rare and treatment is always challenging. In most cases, open reduction is chosen in order to fix the fracture and to get a stable reduction of the joint.2,3 We present the case of a six-year-old girl with a shoulder dislocation and proximal humerus metaphysis fracture, treated by closed reduction using a joystick method and fixation by two intramedullary K-wires achieving a good anatomical reduction of the fracture and shoulder joint with excellent clinical results. There are no previous reports of treatment of fracture-dislocations of the shoulder in children by a closed method using the joystick technique.
Case report
A six-year-old girl was a back-seat passenger (not wearing a seat belt) involved in a car accident when the car collided with a barrier on the road. She presented with severe pain and gross swelling of the right shoulder and physical examination revealed a palpable humeral head anteriorly. She was able to feel and move all her fingers; there was no external wound and injury to any other part of the body. A radiograph confirmed anterior shoulder dislocation with a severely displaced fracture of the neck of the humerus (Figure 1(a) and (b)). After preoperative preparations, the patient was taken to the operating room where a trial of a closed reduction under fluoroscopy was not successful.
A plain radiograph revealed dislocation of the shoulder (a), completely displaced fracture proximal metaphysis humerus (b).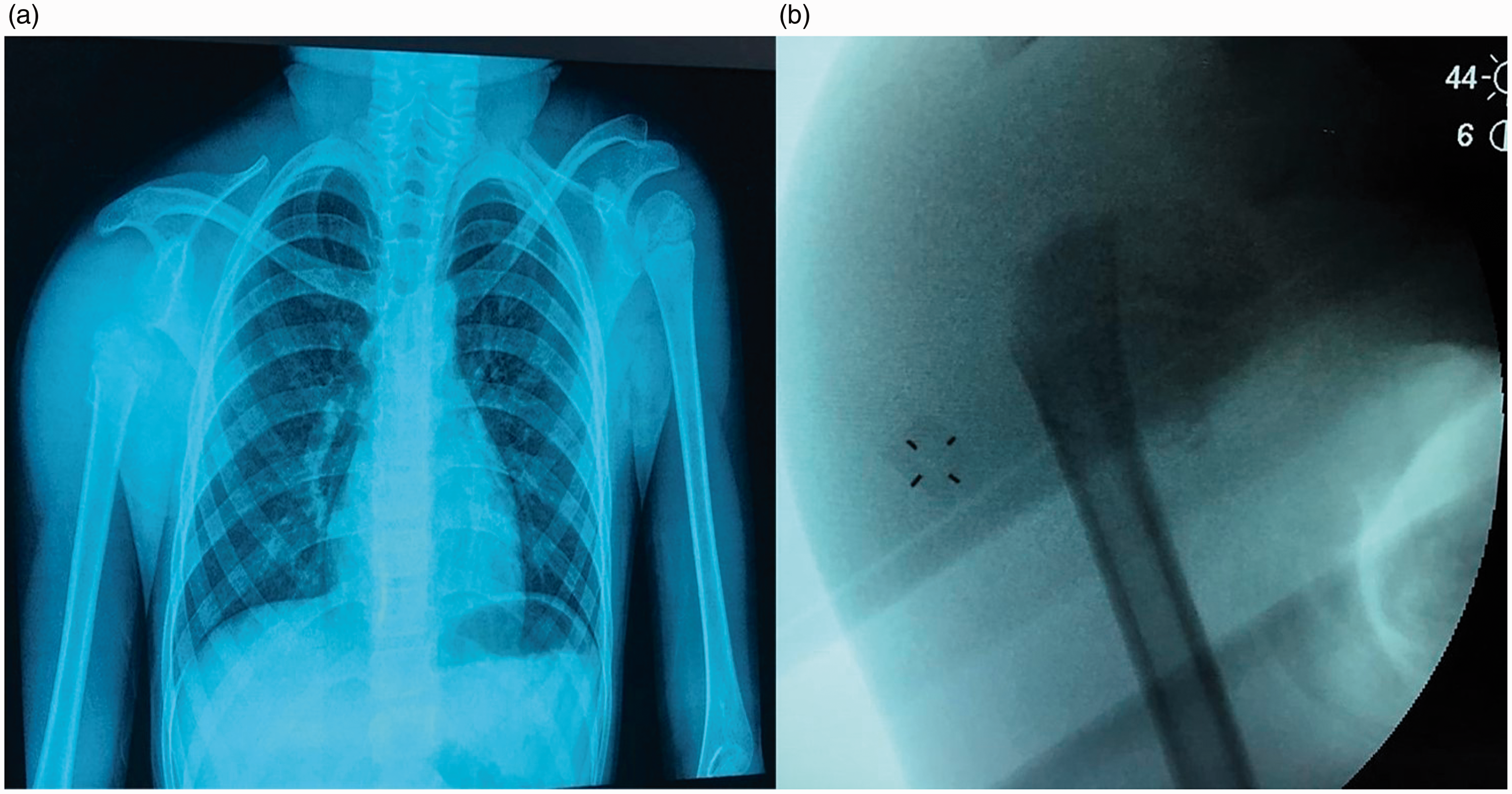
After making a 4-cm incision on the posterolateral aspect of the distal arm, a 3.5 mm drill hole was expanded with an awl, so that a 2 mm K-wire could be inserted into the medullary cavity of the humerus with the help of T handle under the guidance of intra-operative fluoroscopy (Figure 2(a) and (b)). The sharp tip of the wire was excised and bent 15 degrees. Under fluoroscopy, an attempt to reduce the fracture by a technique like the Metaizeau method
4
was tried but was unsuccessful.
(a) 2-mm K-wire was inserted in the medullary cavity of the humerus with the help of T Handle, (b) under fluoroscopy, K-wire is pushed up into the humerus, (c) second K-wire put into the humeral head percutaneously and used as a joystick, (d) intraoperative radiograph showing second K-wire put into the humeral head percutaneously and used as a Joystick, (e) anatomical reduction of the fracture, (f) insertion of second intramedullary K-wire and (g) one-year postoperative radiograph showing healed fracture.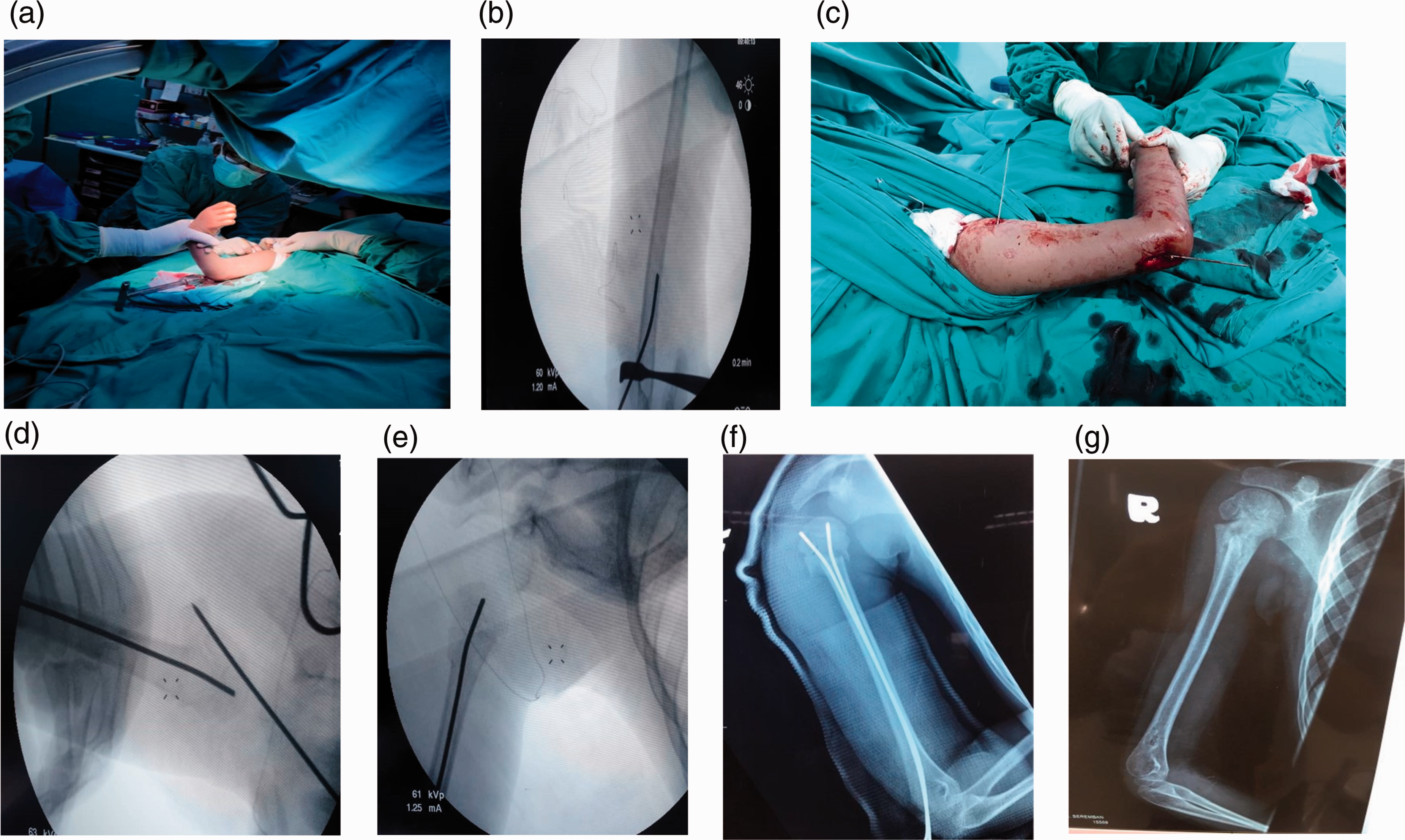
Under screening, a further 2 mm K-wire was centered in the dislocated humeral head through the middle of the deltoid muscle and used as a joystick (Figure 2(c) and (d)). By manoeuvring both wires, successful reduction of the fracture was achieved (Figure 2(e)). Once the fracture was reduced, the humeral head spontaneously slipped easily into the socket, and a second intramedullary K-wire of similar size was inserted to achieve steadiness (Figure 2(f)). The stability of the fracture and joint was assessed by continuous screening. Postoperatively, the shoulder was immobilized by U slab and a sling. At six weeks, K wires and U-slab were removed, and the patient was allowed mobilisation in a sling for two weeks. Follow-up at 12 weeks showed excellent clinical and radiological results (Figure 3(a) to (d)).
Clinical photographs 12 weeks after injury showing the pain-free full range of motion at the right shoulder.
There was no sign of avascular necrosis at one-year follow-up and the child had a full range of pain-free movement (Figure 2(g)).
Discussion
Combination of shoulder dislocation with fracture proximal humerus in children: Literature review.
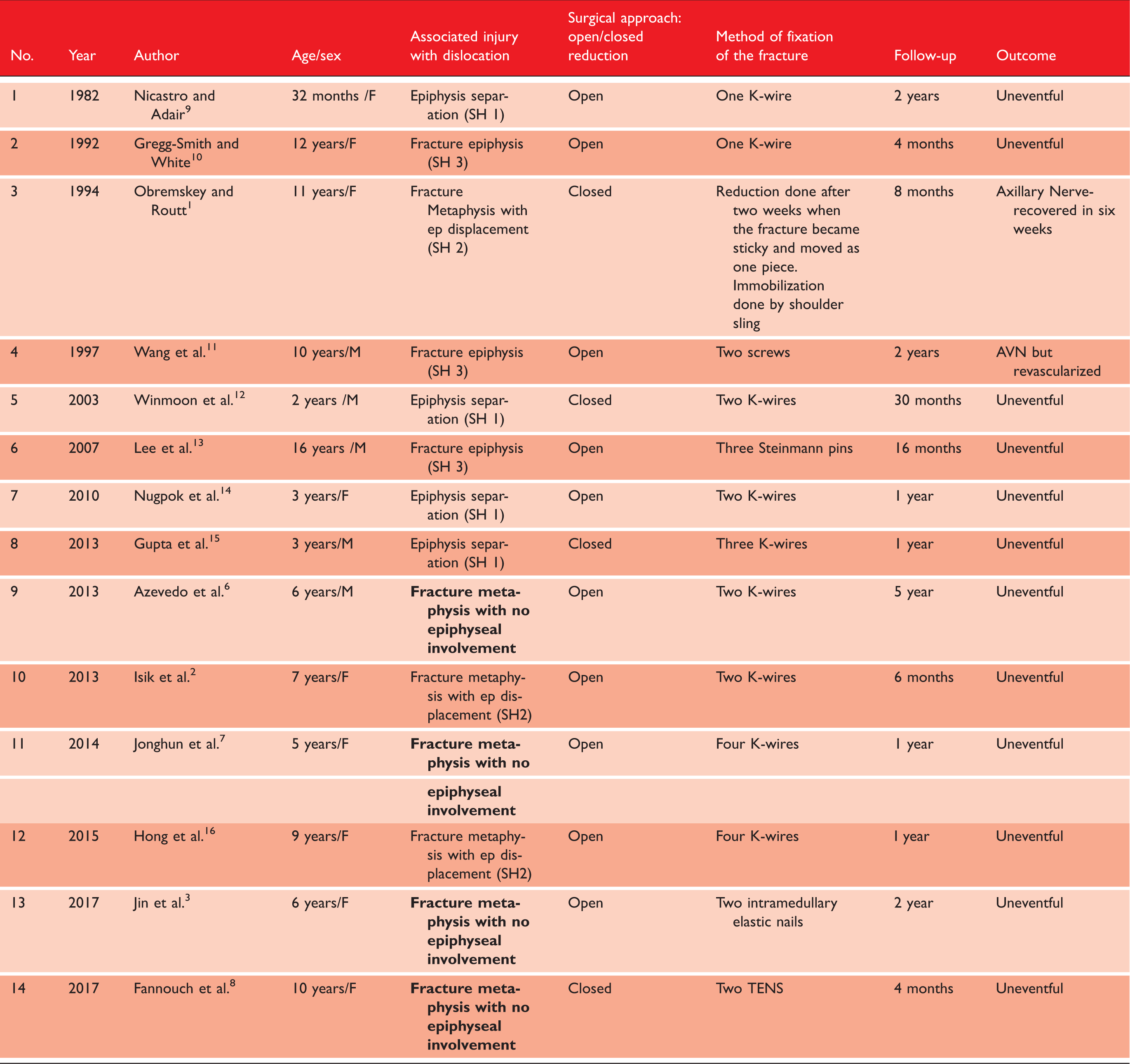
Fractures on the proximal humerus not involving the physis are even rarer.
In four cases of fracture-dislocation shoulder where the physeal plate was not involved,3,6–8 only one was treated by closed reduction of the dislocation with intramedullary fixation of the fracture.
Closed reduction of fracture and dislocation is always difficult. Jin et al. 3 attempted closed reduction with an elastic stable intramedullary nail (ESIN) but failed and had to perform the open reduction. Isik et al. 2 reported dislocation with a fracture in a similar age group and claimed excellent results only after open reduction, but the patient took a longer time to achieve full function. Fannouch et al. 8 reported the satisfactory radiological union and full function after closed reduction and intramedullary pinning. We failed to get a reduction of the fracture by this method, so inserted another K-wire in the center of the humeral head and used it as a joystick to reduce the fracture. The fracture was easily reduced anatomically by manoeuvring both wires under fluoroscopy. Once the fracture reduced, the humeral head went easily into the socket. The key to managing dislocation with a fracture is the reduction of the fracture. We found this method to be relatively easier to reduce the fracture, allowing the head to move into the socket without any resistance. To our knowledge, this method has not been previously reported in the literature.
Conclusion
We recommend using this joystick technique when a closed reduction of the fracture-dislocation of the shoulder fails. It is effective and quick and provides excellent long-term outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Hospital Tuanku Jaafar Hospital, Seremban, Malaysia (Approval No. HTJS/101/070 Jilid 5 (44)).
Informed consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Guarantor
MAI.
Contributorship
MAI wrote the first draft of the article. All other authors reviewed, edited the article and approved the final version. VBP and MS edited clinical photographs and organized them for the article.
Acknowledgements
We would like to thank the patient and her parents for their kind permission.
We also would like to thank the Director-General of Health, Malaysia for permitting us to publish this case report.
Provenance and peer review
Not commissioned, externally peer reviewed.