
Abstract
Introduction
Child participation in sport is important for physical, cognitive and psychosocial wellbeing. Australian rules football has high participation, but also carries a high risk of injury due to the contact nature of the sport. This study aimed to evaluate changes in the presentation and hospital admission of paediatric Australian rules football-related injuries, and to compare the severity of these injuries with those from other team ball sports.
Materials and methods
At an Australian paediatric major trauma service, ED and hospital trauma registry data relating to Australian rules football injury between 2009 and 2015 were obtained. Data from other common team ball sports with a shared field of play were also identified.
Results
During the study period, there were 10,003 ED presentations, and 1110 admissions resulting from team ball sports. With 4751 ED presentations and 616 admissions, Australian rules football accounted for almost one-third of all sports-related presentations and admissions, and around half of the team ball sports cohort. Compared to other team ball sports patients, Australian rules football-related patients were 40% more likely to be admitted, and nearly twice as likely to be classified as severe injury. Australian rules football players presented with different injury patterns were compared to other team ball sports players; admitted players were significantly more likely to have sustained head or neck injuries, and were more than twice as likely to sustain truncal injury.
Conclusions
Australian rules football is a common cause of ED presentations and results in substantial morbidity, both overall and when compared with other team ball sports. Australian rules football should remain a focus for ongoing and active research into strategies which reduce injury risk.
Introduction
Participation in sport is important for children to improve fitness, acquire skills in teamwork and coordination and maintain physical, cognitive and psychosocial wellbeing. Over 70% of all children in the state of Victoria, Australia participate in some form of organised sport outside of school. 1 Within this population, Australian football (known eponymously as ‘AFL’ after the professional Australian Football League) is the most played team ball sport (TBS), estimated to involve 15% of children aged under 15. 2 As such, AFL may be seen as an integral component of the Australian culture in childhood.
AFL is a fast-paced contact sport involving kicking, handballing and running with an oval-shaped ball on a large oval field. Collisions with opposing players are common, providing a variety of injury mechanisms (Figure 1). In most Australian states, AFL outranks all other organised sports as a cause of emergency department (ED) presentations and hospital admissions.3,4 Common features of AFL which carry the potential for injury. These include high catching (‘marking’) (a) and contesting possession or ‘shepherding’ players with the ball (b). Tackling high (c) or with the head unprotected (d) and pushing in the back (e) are illegal but not uncommon. A common mechanism of abdominal injury in AFL involves a player being tackled (f-i) and brought to the ground (f-ii) with both players landing on the ball (f-iii).
In order to encourage the maximum participation in sports, the risks of injury must be mitigated. Severe injury is known to occur in children playing AFL. However, the overall profile of severe injury remains unknown, and the last published paediatric data regarding broader epidemiology and injury patterns are more than a decade old.5,6 This retrospective study was undertaken to evaluate changes in ED presentation and hospital admission of paediatric AFL-related injuries, and to compare the severity of injuries sustained playing AFL with those from similar sports.
Methods
Setting
The Royal Children's Hospital Melbourne (RCH) is a large Australian tertiary paediatric referral hospital. The RCH is the designated paediatric major trauma service for the state of Victoria, and also provides primary health care for children within metropolitan Melbourne. The ED census is approximately 85,000 presentations per year. Victoria contains approximately six million people, including around one million children.
Patient data sources
ED presentation data were obtained for the period January 2009 through October 2015. Demographics, epidemiology and injury diagnoses were included in the data reviewed; injury information was based on a truncated list of ICD-9 codes used in the ED. Formal or informal participation in AFL at the time of injury was primarily based on the injury activity field (which is compulsorily collected in state EDs), augmented by review of free-text descriptions of injury events entered by ED staff. Following the methodology of earlier studies,7,8 a small number of ED presentations following injury playing an unspecified football code were classified as AFL, due to the predominance of this code within the state.
For patients subsequently admitted to hospital, the ED dataset was supplemented by more detailed data on injuries sustained, treatment received and other hospital-based measures from the trauma registry. Datasets extracted from ED records and the registry were merged to ensure that all patients were identified in each source, and to provide a single study cohort for analysis.
Patients aged 18 years and over at the time of injury were excluded. The RCH treats patients aged less than 18 years, although patients aged 16 or 17 years with suspected major trauma are triaged by the Victorian ambulance service to adult centres. 9
Comparison and sub-groups
For comparative purposes, data from other popular TBS (‘soccer’ football, basketball, netball and rugby) were also identified from both ED and Trauma Registry sources, using the same methods as the AFL injuries. Cricket and tennis were excluded as players do not generally compete within the same areas of the sporting field. Other TBS such as hockey were excluded due to small patient numbers. The cohort of non-AFL TBS patients was evaluated against AFL patients as a group, although breakdowns are provided for each sport as supplementary data.
A hybrid definition was used for severe injury. Patients were classified as ‘severe’ if they met any of the following criteria: (1) Patients not discharged to home including patients requiring inpatient rehabilitation or dying after injury. (2) Patients identified as potentially seriously injured prior to, or on arrival to hospital including patients transferred via a retrieval service, or receiving Trauma Team Activation on arrival. (3) Patients who required substantial resuscitation or urgent surgery. This included patients receiving CPR, intubation, ICU admission or blood transfusion, any urgent operating theatre transfer within 90 min of hospital arrival, or vital surgery to intracranial, intrathoracic, intraabdominal, pelvic or spinal areas within 48 h.10–12 (4) Patients with significant anatomical injury. This included anyone sustaining an injury of Abbreviated Injury Scale (AIS – 2008 update) 13 severity of 3 or greater, and also included all patients meeting the state major trauma criterion of an Injury Severity Score (ISS) 14 greater than 12. 15
Analysis
For statistical analysis, continuous variables were expressed as median and IQR, due to non-normal distributions. Categorical variables were reported as percentages and compared using odds ratios, or Chi square or (where necessary) Fisher's exact tests with assessment of standardised residuals and the Cochran–Armitage test for trend. 16 All statistical analysis was performed using Microsoft Excel 2010 (Microsoft Corporation, Redmond, USA) and Stata IC 14.0 (StataCorp, College Station, USA). A two-sided 5% level of significance was employed throughout.
Results
Population and patient groups
The ED records for 521,790 presentations between 2009 and 2015 were retrieved and reviewed. Of 100,075 injury-related ED presentations, 16,166 related to (non-motorised) sporting injury, of which 10,003 presentations related to TBS, with 4751 (47%) of these related to AFL. AFL consequently accounted for 29% of all sports-related ED presentations.
Over the same period, 14,381 patients aged under 18 years were included on the trauma registry following admission for blunt, penetrating or burn injury. There were 101 patients (0.7%) who bypassed ED and were admitted directly to the hospital, of which two (both from AFL) were injured as a result of TBS. Of 1986 sport-related admissions, TBS patients accounted for 1110 admissions – 616 (55%) from AFL, which consequently accounted for 31% of sports-related RCH admissions. Children presenting to the ED after AFL injury were 40% more likely to be admitted than those injured playing other TBS (OR 1.43; 95% CI 1.26, 1.62).
Epidemiology of TBS presentations
Patients presenting to the study hospital after injury playing team ball sports (TBS).

Note: Numbers in brackets refer to column percentages. Boldface used for total figures in the relevant columns.
All but two admitted patients are also included in ED presentations data.
Percentages split across all TBS patients for this breakdown.
Chi square value (with P value) reported for this breakdown.
Standardised residuals demonstrated significant departure from expected values and contribution to overall significance.
Some injury types combined for ED presentations data. Percentages for injury type for admitted patients do not add to 100% as these patients could be coded with multiple injury types. Consequently, odds ratios (with 95% confidence intervals) for incidence of each injury type are reported for this breakdown.
Data complete to October of 2015 only.
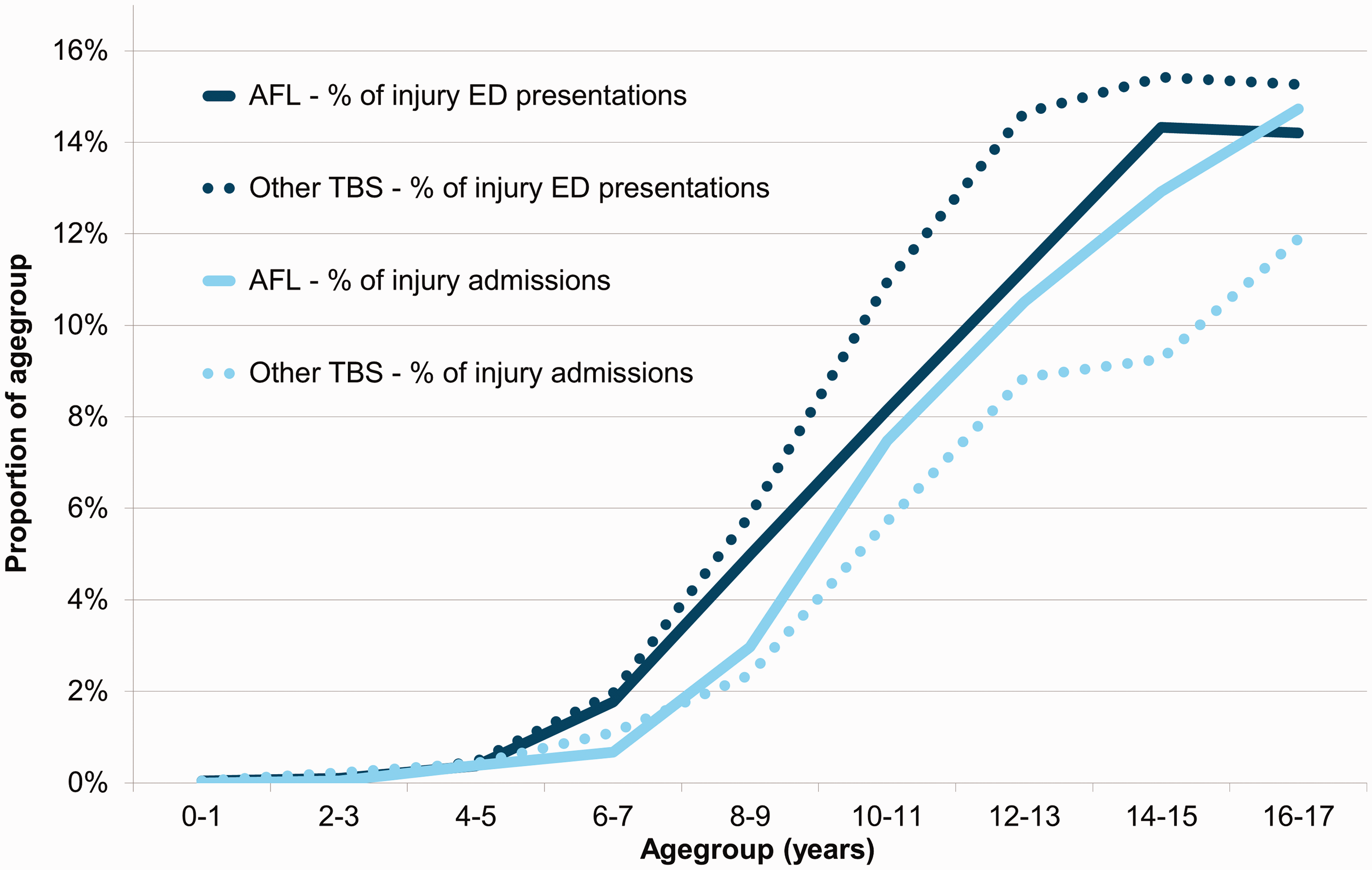
Number of patients injured playing AFL and other TBS, broken down by age group and expressed as proportions of ED presentations and admissions.
Collision-related injuries were common in AFL (Table 1). In both the ED and registry datasets, injured AFL players were twice as likely as other TBS participants to present or be admitted as a result of collision with other players (OR in registry dataset 2.19; 95% CI 1.99, 2.41). Fall-related injuries were frequent amongst all TBS players, particularly in admitted patients.
Additional epidemiological data and hospital outcomes for patients admitted to the study hospital after playing team ball sports (TBS).
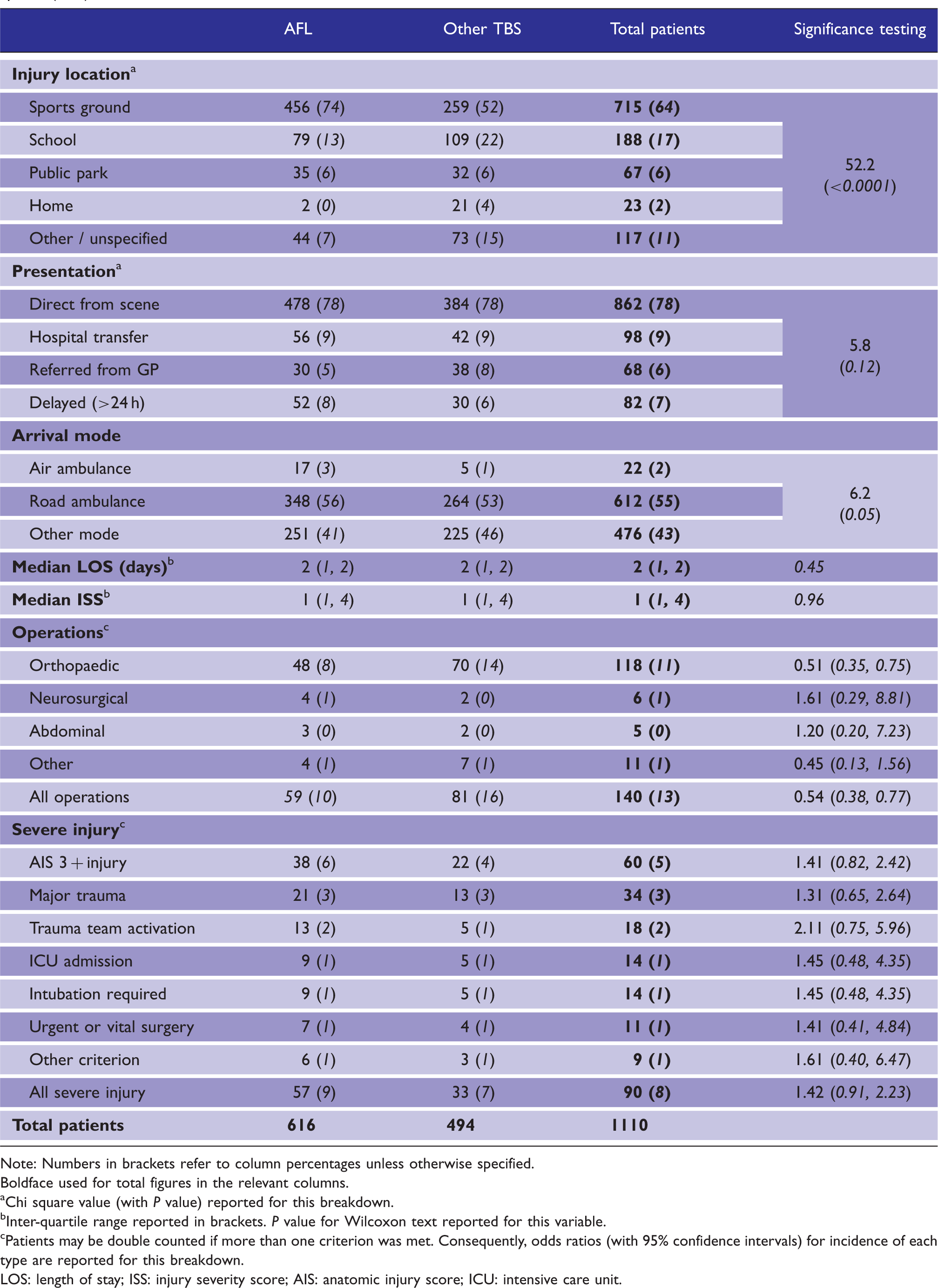
Note: Numbers in brackets refer to column percentages unless otherwise specified. Boldface used for total figures in the relevant columns.
Chi square value (with P value) reported for this breakdown.
Inter-quartile range reported in brackets. P value for Wilcoxon text reported for this variable.
Patients may be double counted if more than one criterion was met. Consequently, odds ratios (with 95% confidence intervals) for incidence of each type are reported for this breakdown.
LOS: length of stay; ISS: injury severity score; AIS: anatomic injury score; ICU: intensive care unit.
The proportion of patients who had been playing TBS rose with increasing age (Figure 2). Above the age of 12, AFL accounted for more than 10% of trauma admissions, and 11% of ED presentations. The incidence of AFL injury was higher during the April–August AFL season, peaking in May (Figure 3). Overall, other TBS injuries were more evenly distributed throughout the year, with low points only during the main school holiday season in December and January. Overall, 19% of AFL ED presentations, and 28% of admissions (170 patients) occurred outside of the usual AFL season. Average monthly ED presentations for AFL and other TBS. Darker colour represents AFL season.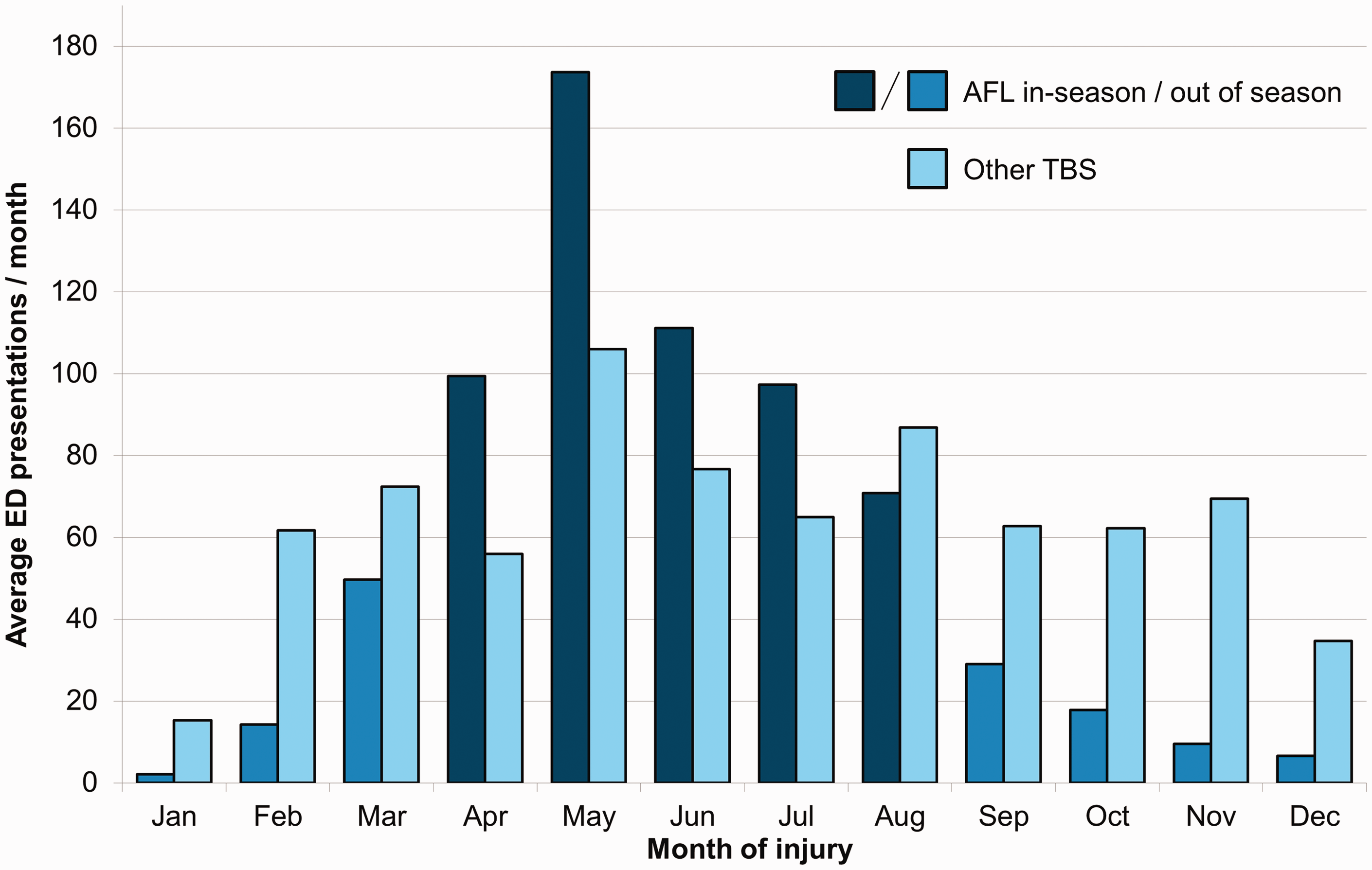
Compared to other TBS, the proportion of injuries and presentations which were AFL-related did not trend significantly over the seven years evaluated (Table 1). Although the total number of TBS patients increased numerically each year, there was no significant increase in the proportion of total ED presentations or total injuries which resulted from AFL or TBS.
Injuries sustained – Type and location
Table 1 shows the types of injury sustained by TBS patients, while Figure 4 illustrates the regions of the body injured. Differences between AFL and other TBS patients were seen in both the ED and registry datasets. Although fractures, sprains and head injuries were common in both (Table 1), the registry dataset recorded more superficial injuries alongside other injuries. Heat maps showing the relative incidence of injury for TBS patients. AFL and other TBS breakdowns are provided for both ED presentations and admissions. Percentage values are rounded.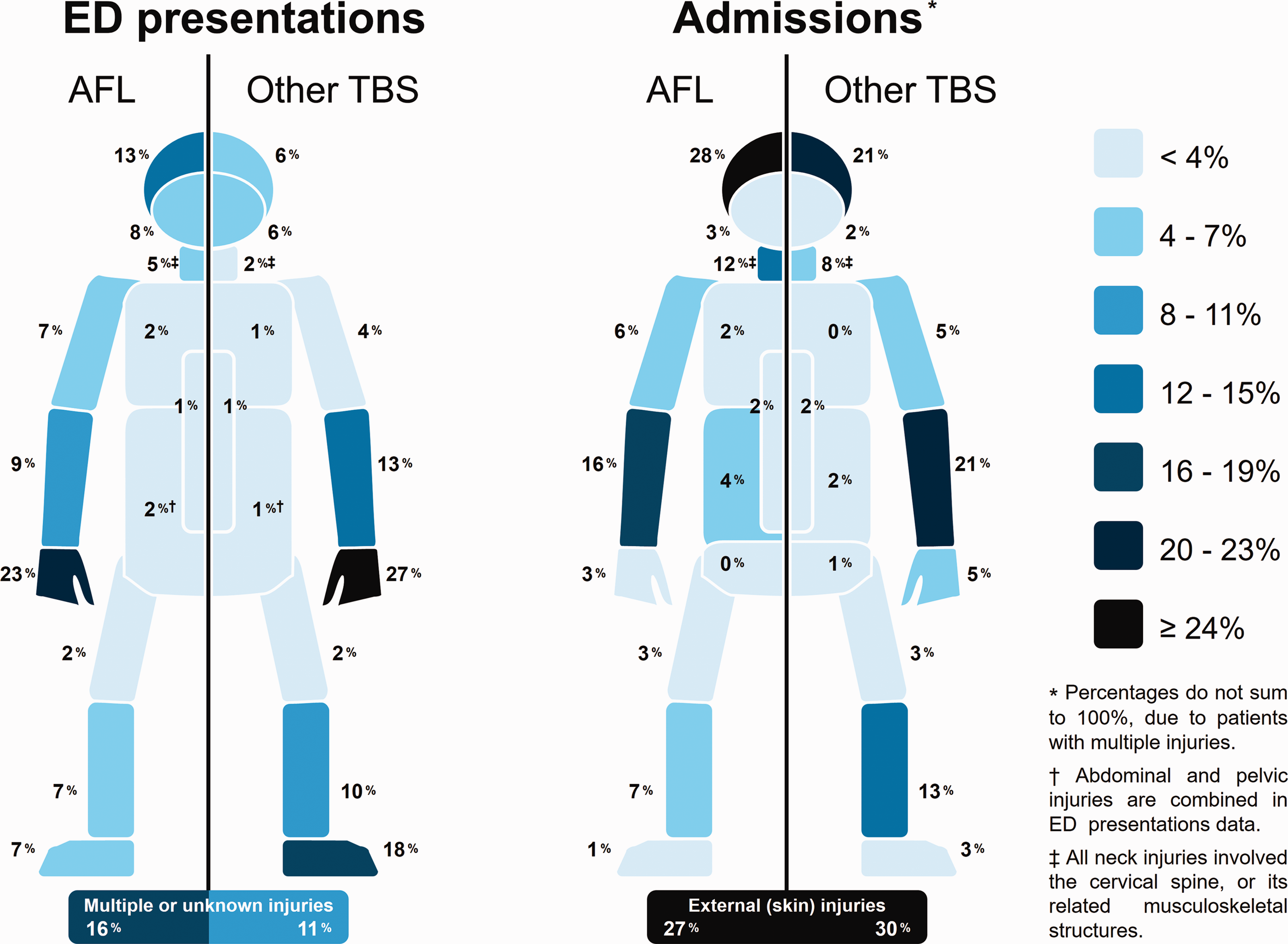
ED presentations for all TBS patients demonstrated a high frequency of injuries to the upper limb (particularly the hand or wrist), lower limb and head (Figure 4); however, few injuries to the wrist or hand required admission. Compared with other TBS patients, admitted AFL patients were significantly more likely to sustain injuries to the head (overall OR 1.46, 95% CI 1.11, 1.94), the neck (OR 1.52, 95% CI 1.01, 2.29) or to the chest or abdominal regions (overall OR 2.23, 95% CI 1.17, 4.26; Figure 4). However, they were less likely to sustain injuries at or below the elbow (OR 0.68; 95% CI 0.51, 0.91), or at or below the knee (OR 0.42; 95% CI 0.29, 0.63; Figure 4). Patients admitted after AFL injury were less likely to sustain fractures than other admitted TBS patients (OR 0.63; 95% CI 0.49, 0.80) (Table 1). A total of 289 admitted AFL patients sustained non-superficial injuries to multiple body regions, compared with 170 patients playing other TBS; AFL players presenting to RCH ED were consequently almost twice as likely to have sustained multitrauma as other TBS patients (OR 1.94; 95% CI 1.60, 2.35). No changes in injury patterns were seen over the period evaluated.
Severity of injury and healthcare burden
Of the 1110 admitted TBS patients, 140 (13%) received at least one operation, with most (118) receiving orthopaedic surgery (Table 2). In keeping with the higher incidence of limb injuries in this group, admitted patients playing AFL were only half as likely to receive surgery compared with other TBS patients (OR 0.54; 95% CI 0.38, 0.77). Of the patients receiving urgent or vital surgery, AFL-related patients required neurosurgical or abdominal surgical intervention, while patients injured from other TBS (all basketball) required neurosurgical intervention or pelvic fixation. No TBS patients required operative intervention by more than one surgical specialty.
Overall, 90 patients injured playing TBS were categorised as severe injury; 57 from AFL and 33 from other TBS (Table 2). AFL-related patients presenting to ED were almost twice as likely as other TBS patients to be subsequently classified as severe injury (OR 1.92; 95% CI 1.25, 2.95), or to have sustained an injury of AIS 3 or greater (OR 1.92; 95% CI 1.13, 3.25). There were no significant differences in incidence between AFL and other TBS amongst admitted patients.
The median lengths of stay and ISS of admitted AFL and other TBS patients were identical. However, the total number of RCH bed days required to treat AFL patients (1228, followed by soccer with 481 days and basketball with 368) was numerically much higher than for any other TBS. No patients died after playing TBS. Four patients required inpatient rehabilitation – three after playing AFL and one who had been playing soccer.
Discussion
Burden of AFL on EDs
This study provides a new appreciation for the scale of the burden of injury attributable to AFL within a paediatric population. TBS are a common cause of injury in children presenting to the study hospital, and accounted for a third of all sports-related presentations. Amongst older children, TBS – and AFL in particular – account for a significant proportion of overall ED burden during the AFL season from May to September. For males aged 12–17 years, AFL presentations to ED in the peak month of May accounted for 18% of all ED presentations (740 of 3986). The seasonality of AFL injury can also place additional stress on overall ED resources as the AFL season coincides with winter, when ED presentation rates are more than a third higher than the summer holiday period.
In our cohort, AFL contributed a disproportionately high number of TBS-related presentations and admissions to hospital when compared with Victorian state data on participation rates in sport – 48% of ED TBS presentations and 55% of TBS admissions, compared with an estimated 20–25% of TBS participation. 2 In addition, AFL contributed to 63% of all TBS-related severe injury, likely due to the contact nature of AFL. Rugby is the other major contact TBS in Australia, and despite low participation in Victoria contributed to 3% of ED TBS presentations and 7% of TBS admissions in our cohort. Previous studies have shown that AFL has similar injury rates to rugby.17,18 However, the high local participation in AFL combined with the risk of injury created a much higher AFL-related healthcare burden in our cohort.
A trend towards increasing injury incidence with increasing age was consistent with the results of several previous prospective cohort studies.5,19,20 This may reflect the age-tiered progression from a reduced contact to a full-contact version of the game after the age of 13, 21 although participation rates and playing styles may also vary. However, there is conflicting literature regarding the change in injury rates after the paediatric age range: elite level players have decreased injury rates, while community level players have increased injury rates that peak over the age of 25.22,23 The peak ED presentation age after 12 years of age is consistent with other hospital-based studies, but contrasts with community-based studies which found that injury rates peaked in the 17–18 year age range.5,19 This may reflect older participants choosing to seek healthcare in other settings, coupled with state triage guidelines which divert trauma patients over the age of 16 to adult hospitals. 9
Injuries sustained during AFL and other TBS
AFL has been recognised as a leading cause of sports-related head injuries;24,25 in one recent study, AFL accounted for 47% of concussions presenting to a paediatric ED, 26 while earlier data from the RCH found that AFL contributed to 60% of TBS-related closed head injuries.24,25 Similar proportions were observed in our cohort, as AFL contributed to 67% of all TBS-related head injury presentations, and 62% of head injury admissions (Table 1). Despite rule modifications to discourage contact to the head, the proportion of head injuries related to AFL remains high and should remain a target for injury prevention. The AFL Commission (the national governing body for AFL) has produced guidelines for the management of concussion, 27 although adherence to on-field head injury management rules may still be suboptimal. 26 Crucially, though, concussion guidelines are primarily focused on injury mitigation and not prevention.
More broadly, admitted AFL participants had higher incidences of head, neck, chest and abdominal injury compared with other TBS. The overall incidence of these injuries was fairly low, with four patients requiring operative management over the seven-year period. However, the relative potential for such injuries to result in life-changing consequences should not be understated. It is possible that specific modifications to rules or coaching strategies may be able to mitigate the risks of injury, but any assessment of these was outside the scope of the current study.
In terms of minor injury, there is little agreement regarding leading injury types sustained by children playing AFL.3,5,28 In our population, fractures and soft tissue injuries such as sprains and haematomas appeared in equal proportions, compared with a higher incidence of soft tissue injuries in community cohorts. 19 Injuries to the head, face, neck, legs and arms have also previously been reported.29,30
Strengths and limitations
A strength of the present study was the size and completeness of the datasets used, particularly for registry data which had complete data for all fields used. A further strength of the ED dataset evaluated was the use of narrative free-text fields of the exact injury event as collected by ED staff, which was often able to identify mis-coded patients or clarify less specific codes. Of 10,003 patients identified with TBS, 1293 patients (13%) – including 773 of the 4751 AFL patients (16%) – were originally coded to a sport or activity other than the sport to which their injury event was definitively allocated after free-text review. For admitted patients, final classifications were confirmed by cross-referencing with more detailed registry data. However, the retrospective nature of this study means that data may still have been mis-coded. These findings underscore the importance of narrative fields in routine ED injury surveillance datasets. 31
A further strength is the multi-level design which enabled patients which may have been missed in one data source to be identified by another. However, as a tertiary paediatric hospital, presentation and referral biases may exist. The RCH is the sole paediatric major trauma centre within an inclusive state trauma system, receiving 85% of the hospitalised paediatric major trauma in the state. 32 State guidelines mandate that ambulance services triage potentially severely injured children under 16 years to the RCH, while patients aged 16 years and over are triaged to adult major trauma centres. 9 This may have resulted in an underestimation of the incidence of AFL injury in patients aged 16 or 17, and an overestimation of AFL's contribution to morbidity (Figure 2). Severe paediatric trauma from AFL-related injury is known to have been treated at adult centres in the state. 33 However, in our study, there was little evidence to suggest that a referral bias affected the AFL group to a greater or lesser extent than the other TBS group (Table 2). Use of air ambulance transport was numerically higher in the AFL group and showed a moderate effect size, but numbers were comparatively small and these patients were evenly split between inter-hospital transfers and direct transfers from the injury scene.
There was a substantial gender disparity in our study population, with boys over-represented in all TBS but particularly AFL. However, it is not known how this compares with actual participation. Girls' participation in AFL has increased since alongside the commencement of a professional women's AFL competition in 2017, although this was outside the study period. Further study is needed to reassess whether the observed disparity in presentation reflects actual exposure bias, or true differences in the experience of playing TBS across genders which may increase or decrease injury risk.
Finally, although the present study compared the incidence of patient presentations and admissions to a large tertiary paediatric hospital with the most current population participation data, there may be biases in this data, or the assumptions made in using it. Participation rates are based on population samples only; they may change over time and also do not provide any information on exposure (i.e. the length of time that each participant is engaged in sport over a given time period).
Conclusions
In an Australian state where AFL is popular, AFL is a common cause of ED presentations. Due to the contact nature of the sport and high participation rates, AFL resulted in substantial hospital-based morbidity. Children playing AFL are at an increased risk of head, chest and abdominal injury compared to other team ball sports.
Injury prevention should be enshrined within the governance structures of both peak and community sporting bodies. Specific to AFL, greater innovation is required. Simple checklists such as concussion guidelines which focus on the post-injury environment are insufficient. AFL should remain a focus for ongoing and active research and social commentary regarding potential risk factors.
Supplemental Material
sj-pdf-1-tra-10.1177_1460408620941335 - Supplemental material for An evaluation of the presentation and severity of Australian football injury in children
Supplemental material, sj-pdf-1-tra-10.1177_1460408620941335 for An evaluation of the presentation and severity of Australian football injury in children by Leopold Simma, Cameron S Palmer, Alan Ngo, Helen E Jowett and Warwick J Teague in Trauma
Footnotes
Declaration of conflicting interests
The author(s) declared no conflict of interest with regards to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained from the Royal Children's Hospital Human Research Ethics Committee (Reference # DA041-2015-12).
Informed consent
Informed consent was not sought as the research was done without patient involvement. Patient data were collected using a registry for quality assurance purposes, and the use of this anonymised data was approved by a Human Research Ethics Committee. Consequently, data are not available to external researchers. A summary of results will be made available to the public through our institution's website.
Guarantor
CSP.
Contributorship
LS and CSP conceived the study. LS, CSP and WJT gained ethical approval. HEJ took the images used in Figure 1. CSP extracted and analysed data, LS and CSP interpreted the data. LS drafted the manuscript, and CSP and AN undertook redrafts of the manuscript. All authors (LS, CSP, AN, HEJ, WJT) contributed to and approved the final manuscript.
Acknowledgements
Associate Professor Teague's position as an Academic Paediatric Surgeon and Director of The Royal Children's Hospital Trauma Service is generously supported by The Royal Children's Hospital Foundation.
Provenance and peer review
Not commissioned, externally peer reviewed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.