
Abstract
Introduction
Hypothermia at admission in trauma patients has been significantly associated with worse outcomes and increased blood usage. Previous studies have found variably significant associations between ambient temperatures and incidence of hypothermia in trauma patients.
Methods
The trauma quality improvement registry was queried for data on trauma patients admitted direct from the scene over a 5-year period. This database was matched to daily weather data taken from the nearest National Oceanic and Atmospheric Administration land-based climate monitoring center, and further combined with blood usage data from the laboratory information system.
Results
Multivariate logistic regression models predicted significant associations between ambient temperature and patient admission temperature for severely injured patients. No significant direct associations were predicted between ambient temperature and in-hospital mortality or blood usage. Models predicted a significant association between decreased admission temperature and increased likelihood of both blood transfusion and mortality for a severely injured subgroup.
Conclusions
Ambient temperature is a significant contributor to the rate of admission hypothermia in trauma patients. Most of the variability in admission temperatures for severely injured trauma patients remains unaccounted for by models using standard markers of anatomic and physiologic severity. Decreasing admission temperature is significantly associated with increased mortality and likelihood of blood transfusion for severely injured patients.
Introduction
The “bloody vicious cycle”, named by Kashuk et al in 1981, 1 identifies hypothermia, acidosis, and consumptive coagulopathy as principal and self-perpetuating etiologies of life-threatening hemorrhage after traumatic injury. Most proteins in the coagulation cascade are enzymes and accordingly have diminished activity outside of their optimal temperature range2,3 and pH.4–6
Accordingly, hypothermia in trauma patients at time of presentation to a trauma center has been extensively associated with worse outcomes and increased blood product usage.7–9 As an independent predictor of mortality,10,11 hypothermia is a potential therapeutic target for interventions such as active warming.12,13
Severe injury can directly cause hypothermia via inhibition of thermoregulation and the shivering response as well as through mechanisms associated with shock. 14 These mechanisms are consistent with the significant associations between increasing injury severity and penetrating injuries with the incidence of hypothermia. 11 , 15 However, a primary mechanism associated with injury severity does not rule out a contributory effect of exposure. Accordingly, understanding whether trauma-associated hypothermia is associated with seasonal variation in weather can inform decisions to deploy active warming therapies in pre-hospital and hospital-based settings. 16
Despite what may seem like an obvious association between colder weather and increased prevalence of hypothermia in trauma patients, various studies have produced conflicting results. A prospective observational report from Seattle published in 1987 showed no seasonal differences in the incidence of hypothermia, with similar scene and transport times between patients. 9 A 1990 report from San Diego showed no association of hypothermia with time from injury to admission as a proxy for exposure. 17 Similarly, a 1998 report from Rutherford et al in Nashville compared month by month incidence in hypothermia in patients admitted to the Surgical Intensive Care Unit (SICU) and found no significant differences. 18 In contrast, two studies from New South Wales and Melbourne in Australia found significant increases in hypothermia on presentation during winter months versus summer months. 10 , 19
One hypothesis for the lack of significance seen in the Seattle study was the limited seasonal variation in temperature of the pacific northwest. During the time period studied in Seattle, winter was on average 10-15°C colder than summer. 9 The study performed in Melbourne reported a mean minimum winter temperature of 5.1-8.0 °C or 41-46°F, 10 and review of Australian governmental weather data from 2008 shows a 5 °C difference between mean minimum winter and summer temperatures. 20 Based on this, seasonal variation in temperatures is insufficient to explain why both Australian studies generated significant associations between season and hypothermia prevalence while American studies did not.
In addition to ambient temperature, precipitation is associated with increased odds of accidental hypothermia in non-trauma exposed populations. 21 Given the discrepancies in the literature and potential clinical impact, we evaluated the associations between ambient temperature, precipitation, and snowfall with presenting hypothermia, mortality, and blood product usage in a severely injured trauma population. We hypothesized that colder ambient temperatures and the presence of precipitation and snow would be associated with increased hypothermia and worse outcomes.
Methods
Study setting, population, and inclusion and exclusion criteria
This single center retrospective study was conducted at a level one primary adult trauma referral center that averages 8500 trauma admissions per year, with the majority of these admitted directly from the scene of injury. The study was approved by expedited review of the Institutional Review Boards (IRB).
The trauma quality improvement registry was queried for data on trauma patients admitted direct from the scene to the trauma resuscitation unit (TRU) over a 5-year period (midnight 1 January 2014 through midnight 31 December 2018). Data fields taken from this database included sex, height, weight, location and description of injuries, admission date and time, travel time, initial vital signs, and outcomes including in-hospital mortality and ventilator days. Patients were excluded if they had missing information for variables of interest or if their transit times were over six hours.
Weather and blood data sources
Climate data was taken from the nearest National Oceanic and Atmospheric Administration (NOAA) land-based climate monitoring center. 22 Patient identifiers taken from the trauma database were used to identify associated blood product transfusions in a comprehensive database of all transfused blood products. This transfusion data was taken directly from the transfusion laboratory information system (Cerner Laboratory, Cerner Corporation, North Kansas City, MO).
Statistical analysis
Data cleaning, combination, and analysis were performed in the R statistical computing language version 3.5.3 (“Great Truth”) utilizing the tidyr, ggplot2, survival and survminer packages.23–25 Linear and logistic regression were performed using generalized linear modeling via the base R stats package. Area under the curve calculations (AUC) for receiver operating characteristic (ROC) curves were performed using the pROC package. 26
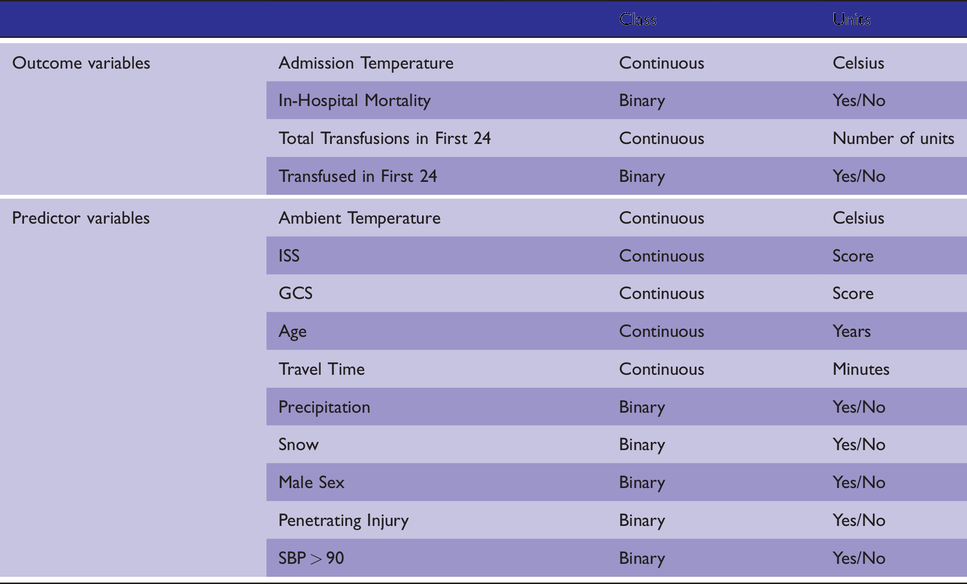
In multivariate logistic regression models of mortality, co-variates were selected based on previously established associations with survival in trauma. 27 Variables treated as continuous included patient age, injury severity score (ISS) for anatomic severity, Glasgow coma score (GCS) for neurologic severity, and admission temperature. Categorical variables included sex, whether systolic blood pressure was greater than 90 mmHg, and type of injury as penetrating or not. Multivariate linear regression models of admission temperature utilized the same co-variates in addition to mean ambient temperature as a continuous variable and the presence of precipitation or snowfall as categorical variables (Table 1).
Names, classes, and units of variables used in linear and logistic regression modeling.
Planned subgroup analyses included severely injured patients (ISS > 15) and patients transfused any blood products within 24 hours of admission. Hypothermia was defined as an admission temperature less than 36 °C, and hyperthermia was defined as a temperature greater than 38 °C, with normothermia inclusive of 36-38°C. 28
In univariate comparisons, P values are reported for continuous variables as the result of two-sided t tests and for categorical variables as the results of Fisher’s exact test, both with a significance threshold of 0.05. Averages of patient data are reported as medians and interquartile ranges, and averages of weather data are reported as means unless specified otherwise.
Results
From 1/1/2014 to 12/31/2018, the trauma database recorded a total of 20,742 direct from scene trauma admissions (Figure 1). Removing records with missing data or a transport time over six hours left 17,390 patients for analysis (Table 2). Three thousand and ninety-four patients had an ISS greater than 15, and 1,185 received a blood product in the first 24 hours.
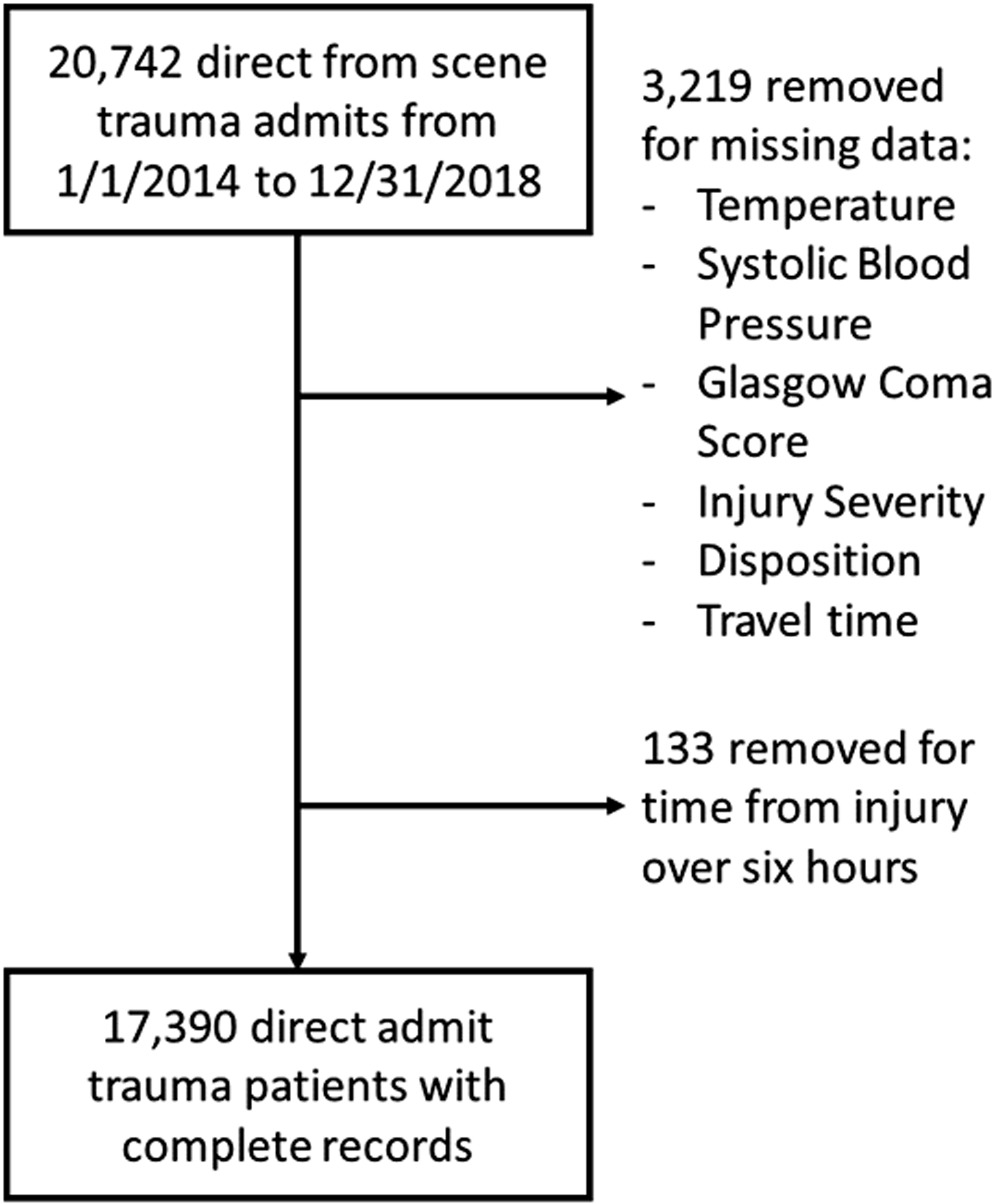
Flowchart showing patient selection process.
Epidemiologic characteristics of the post-selection dataset and subgroups.
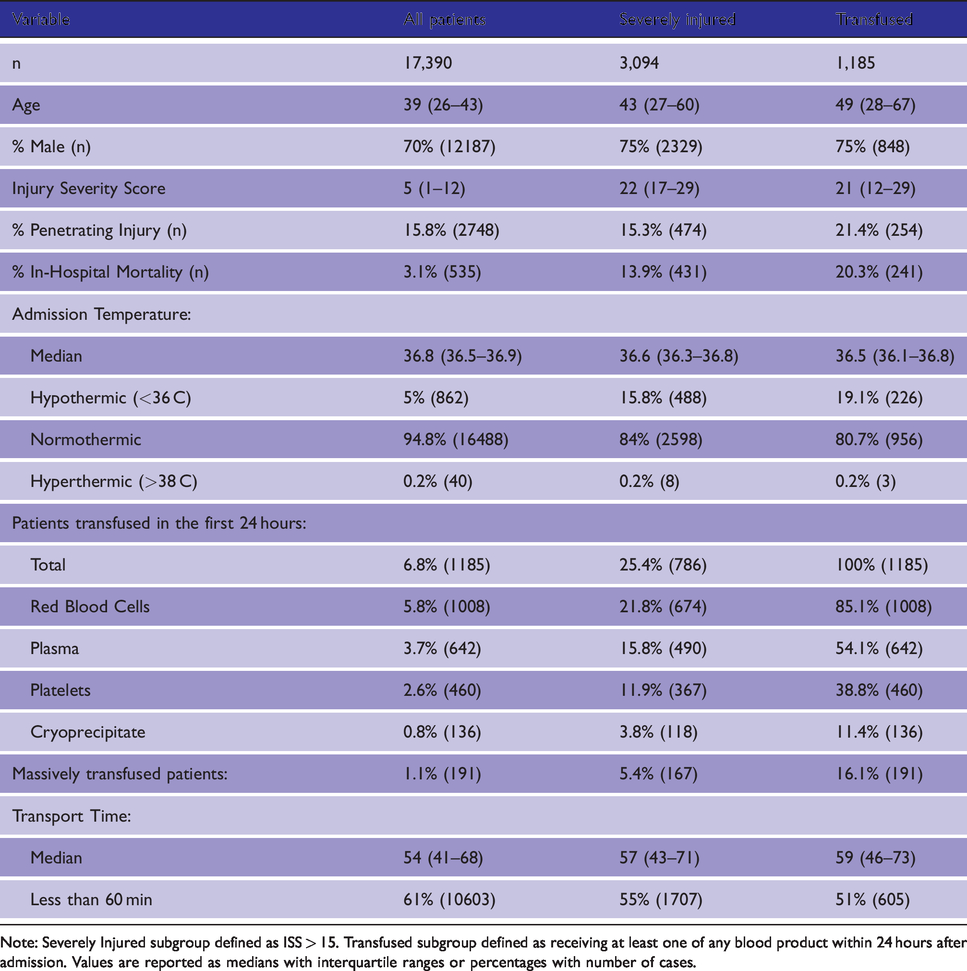
Note: Severely Injured subgroup defined as ISS > 15. Transfused subgroup defined as receiving at least one of any blood product within 24 hours after admission. Values are reported as medians with interquartile ranges or percentages with number of cases.
Ambient temperature, patient admission temperature, and outcomes
Ambient temperatures varied seasonally across the 5 years of the study period (Figure 2), with a recorded minimum daily mean ambient temperature of -12.8 °C on 2/20/2015 and a daily mean maximum of 31.7 °C on 8/14/2016. Out of 1825 days in the study period, 634 (34%) had precipitation recorded, and 55 (3%) had snowfall.
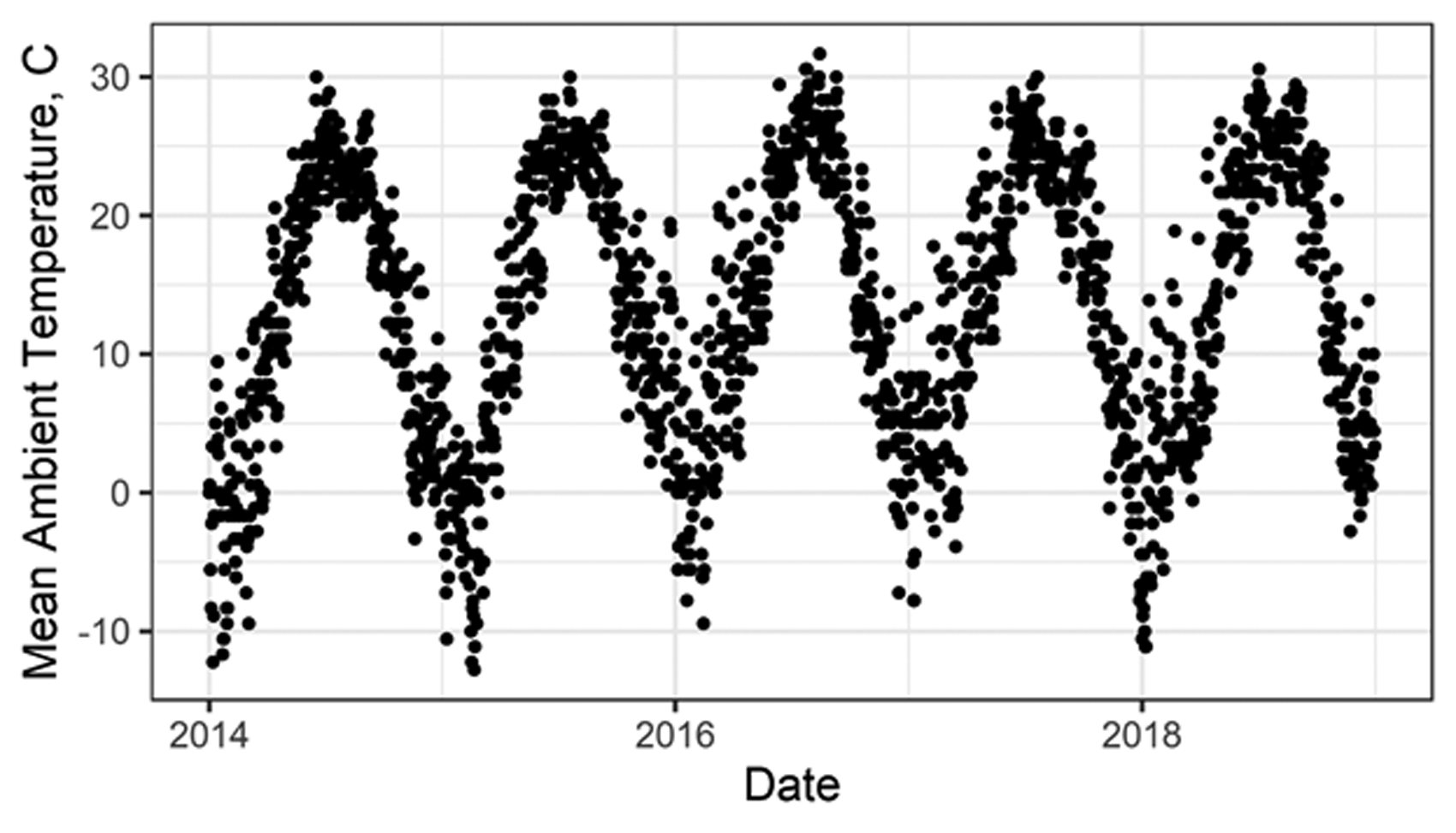
Ambient temperature variation over the study period.
Linear regression models of admission temperature predicted significant associations with ambient temperature in univariate and multivariate models (Tables 3, 4 and Figure 3). Multivariate binary logistic regression models of in-hospital mortality predicted significant associations between admission temperature and mortality in the severely injured cohort but not in transfused patients (Table 5). Hypothermic patients had an in-hospital mortality of 22%, which was significantly higher than the 2% and 2.5% mortality rates of normo- and hyperthermic patients (P < 0.001 and P = 0.007 respectively) (Figure 4). Univariate logistic regression analyses did not show a direct significant association between ambient temperature and mortality in both the previously defined severely injured and transfused subgroups.
Univariate linear regression model for admission temperature.
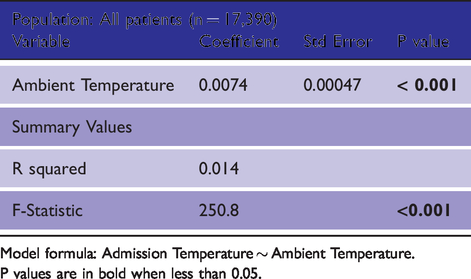
Model formula: Admission Temperature ∼ Ambient Temperature. P values are in bold when less than 0.05.
Multivariate linear regression model for admission temperature.
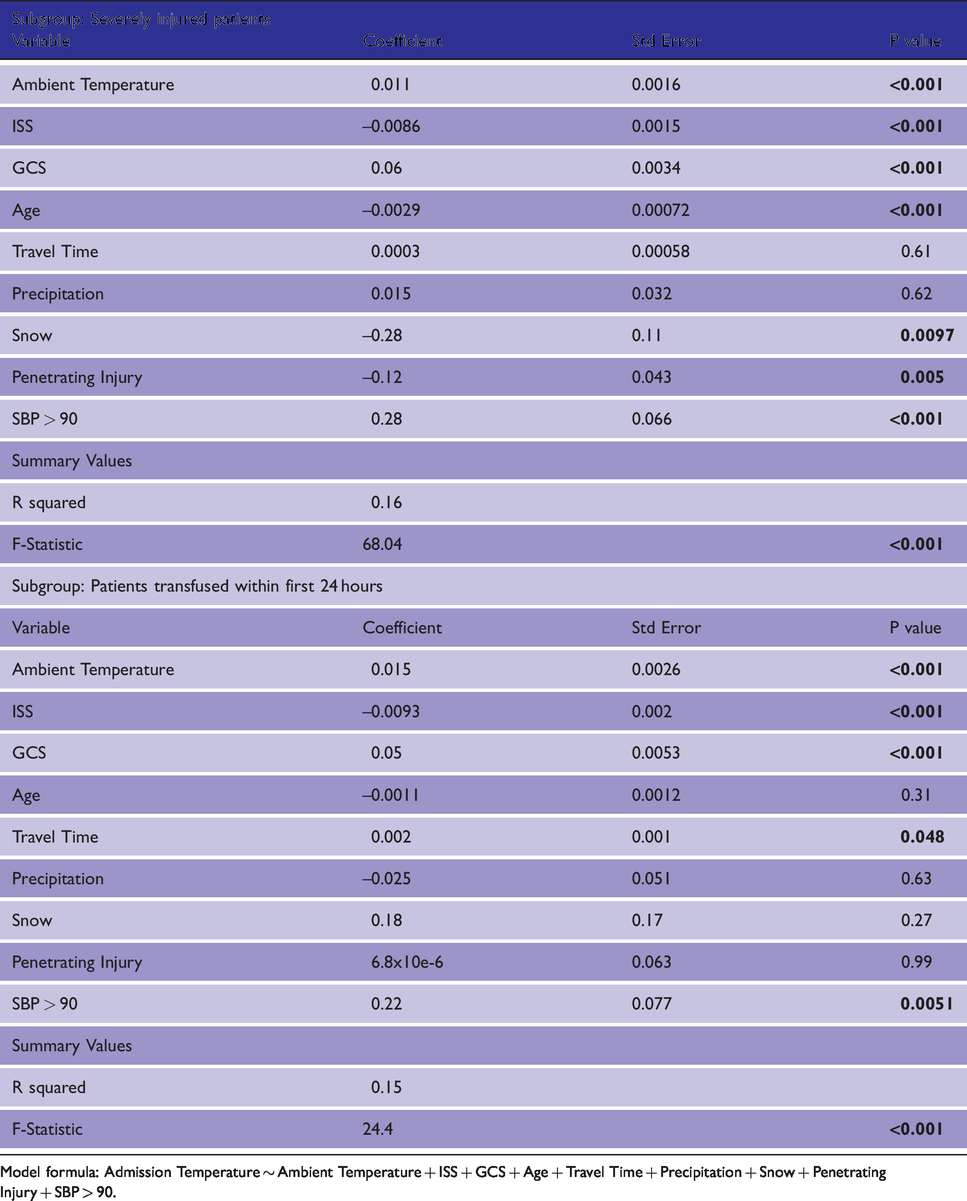
Model formula: Admission Temperature ∼ Ambient Temperature + ISS + GCS + Age + Travel Time + Precipitation + Snow + Penetrating Injury + SBP > 90.
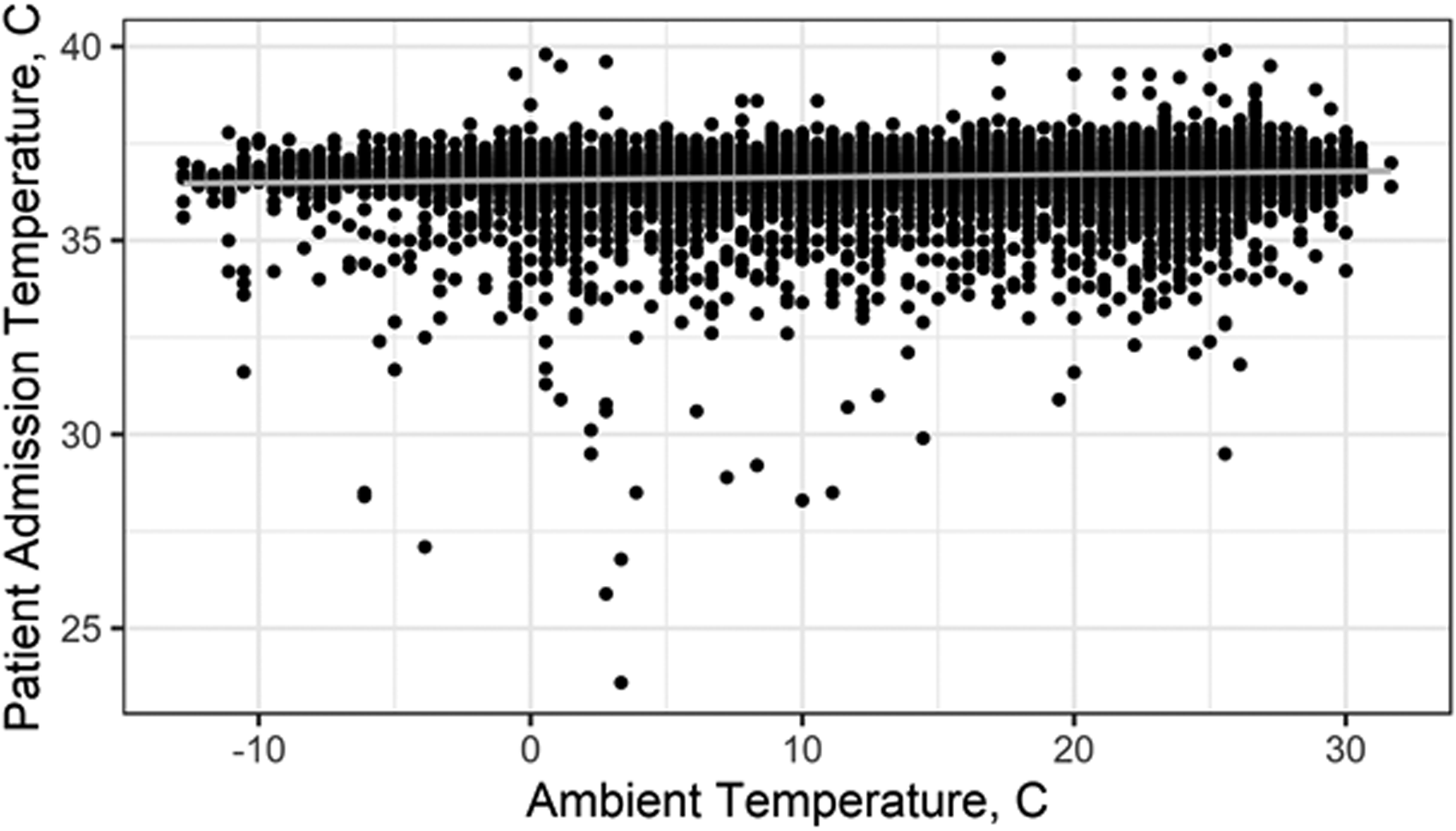
Ambient temperature and patient admission temperature, all trauma patients.
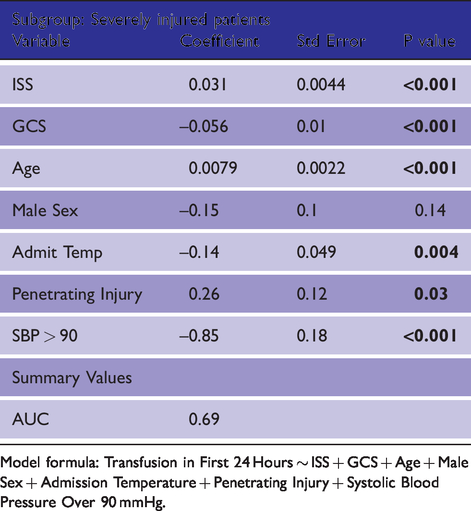
Multivariate binary logistic regression model of in-hospital mortality.
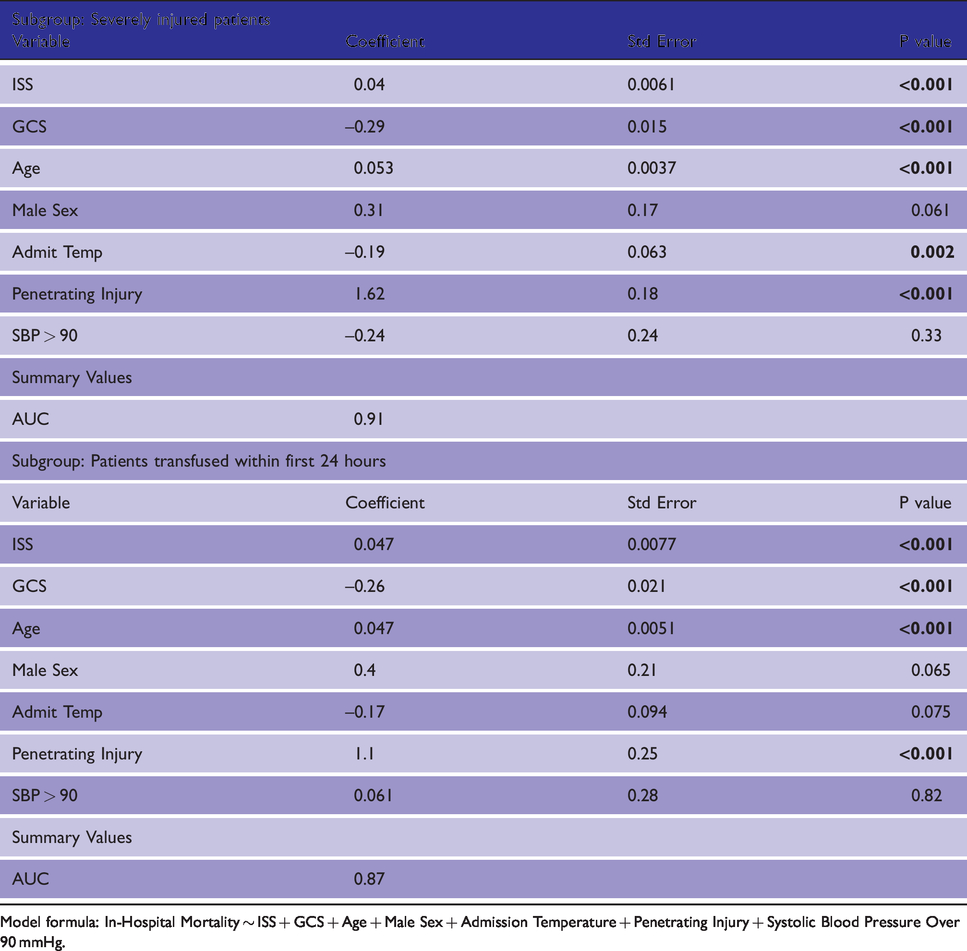
Model formula: In-Hospital Mortality ∼ ISS + GCS + Age + Male Sex + Admission Temperature + Penetrating Injury + Systolic Blood Pressure Over 90 mmHg.
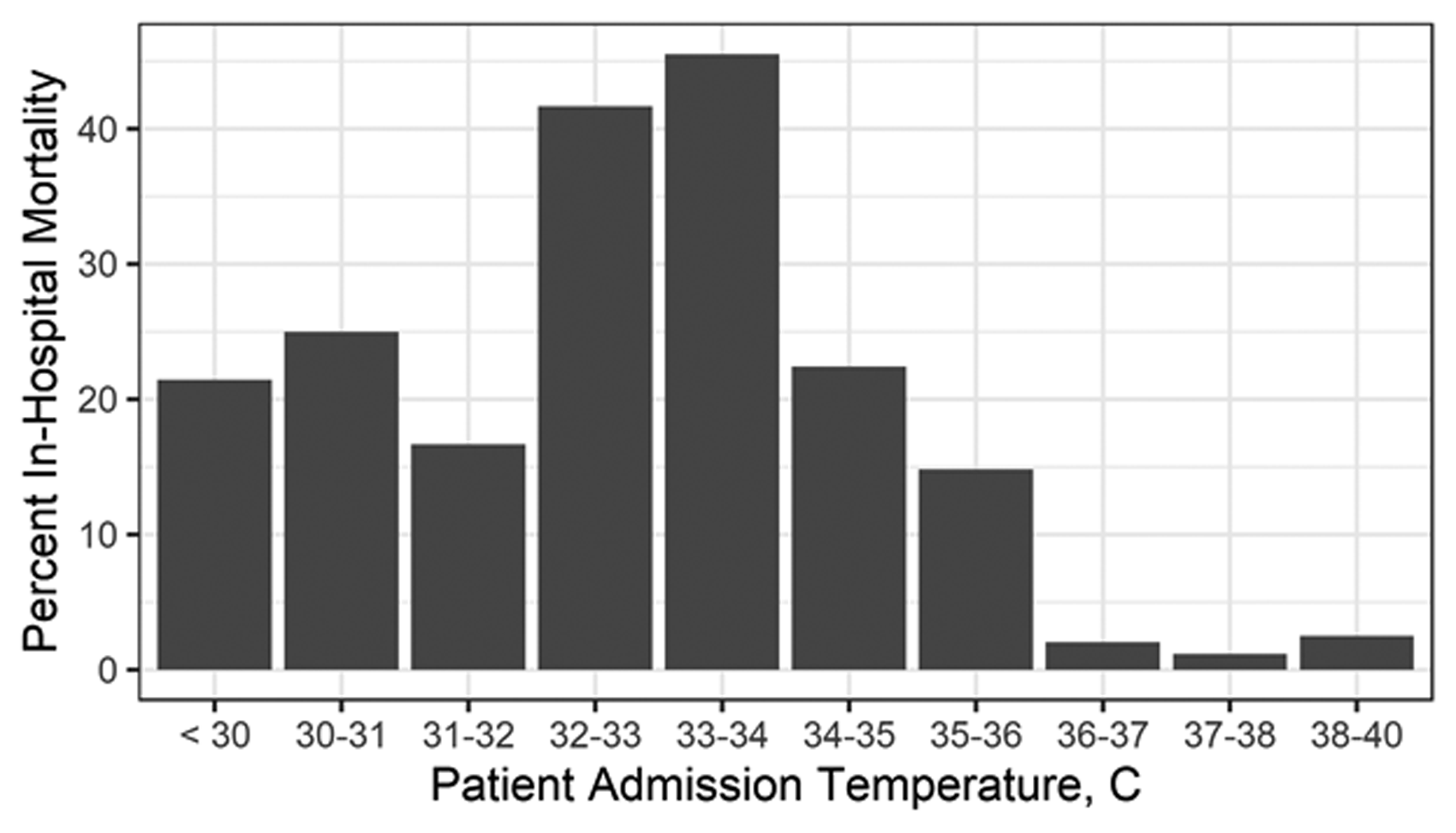
In-hospital mortality for all trauma patients expressed as percent of patients with admission temperatures between ranges, right inclusive.
Blood transfusion, patient admission temperature, and ambient temperature
In a multivariate regression model of the association between blood transfusion and admission temperature using the same covariates as the mortality model, decreasing admission temperature was significantly associated with increased likelihood of any blood product administered in the severely injured subgroup in the first 24 hours (Table 6). Decreasing admission temperature was also significantly associated with an increased total number of blood products administered in the first 24 hours among transfused patients (Table 7).
Multivariate binary logistic regression model of any transfusion occurring in the first 24 hours after admission.
Model formula: Transfusion in First 24 Hours ∼ ISS + GCS + Age + Male Sex + Admission Temperature + Penetrating Injury + Systolic Blood Pressure Over 90 mmHg.
Multivariate linear regression model for blood products transfused in first 24 hours after admission for all transfused patients.
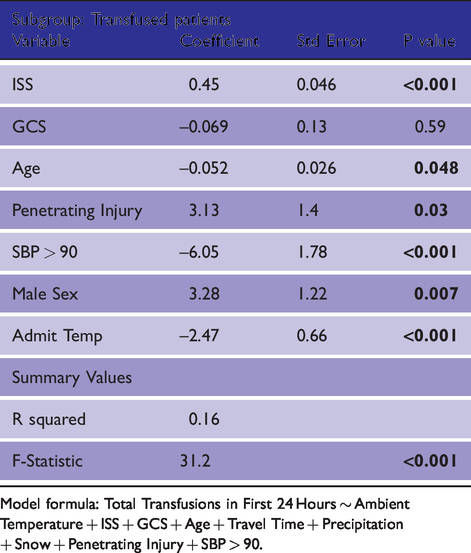
Model formula: Total Transfusions in First 24 Hours ∼ Ambient Temperature + ISS + GCS + Age + Travel Time + Precipitation + Snow + Penetrating Injury + SBP > 90.
In univariate analyses, there were no significant associations predicted between ambient temperature and likelihood of any transfusion in all patients and the severely injured subgroup. Linear regression models did not predict significant associations between ambient temperature and quantity of blood products transfused in the first 24 hours or during the admission period for the transfused subgroup.
Discussion
Decreasing ambient temperature, or cold weather, was significantly associated with decreased admission temperatures in univariate and multivariate comparisons, including for severely injured and transfused trauma patients. Using the model for transfused patients, all other variables held constant, a 20 °C decrease in the ambient temperature would predict a 0.3 °C decrease in admission temperature with a 95% confidence interval (95% CI) of plus or minus 0.1 °C.
This effect size may seem clinically small yet is still larger in potential impact than other covariates measuring the severity of a patient’s injury and risk for poor outcomes. Using the same transfused patient model for admission temperature, a 0.3 °C (0.24 – 0.36 95% CI) drop in admission temperature was associated with a change in GCS of 6 or a more than 30-point change in ISS.
Penetrating injury was significantly associated with decreased admission temperature in the severely injured subgroup but not the transfused subgroup (Table 4). This may be partly due to covariance of penetrating injury with the risk of transfusion in the first 24 hours, as the transfused subgroup had a higher percentage of penetrating injuries. Similarly, age was significantly associated with decreased admission temperature in the severely injured subgroup, with a small effect size suggesting some weak correlation between diminished physiologic reserve and increased incidence of admission hypothermia. Hypotension, a marker of physiologic distress, was predicted to be significantly associated with decreased admission temperature in both the severely injured and transfused subgroups.
Other weather factors were not consistently associated with admission temperature across subgroups. The presence of precipitation was not significant for either subgroup, and snowfall was only significant associated with decreased temperature in the significantly injured subgroup.
Travel time was significantly associated with decreased admission temperature in the transfused subgroup, but with a small effect size. This could be attributable to residual confounding by patients who were transferred or transported over long distances not filtered out by the selection steps.
Multivariate logistic regression models for in-hospital mortality showed a significant association between admission temperature and mortality for severely injured patients but not for transfused patients. Admission temperature was also significantly associated with likelihood of any transfusion as well as total number of transfusions during the first 24 hours.
The discrepancy in significant associations between admission temperature and overall mortality for highly injured versus transfused patients suggests that selecting transfused patients reduces the impact of admission temperature by removing its association with transfusion. Significant associations were predicted between risk and amount of transfusions and admission temperature in severely injured patients. This link between hypothermia and transfusion is likely related to the well-established association between hypothermia and coagulopathy in trauma.3,29
Other differences between the severely injured and transfused subgroups in our models for admission temperature include significant effects of snow, age, and penetrating injury on the severely injured subgroup model and travel time on the transfused patient model. Given the relatively few days that had snow in our study period, that difference may be due to outliers in the severely injured subgroup. The difference in significance of age and penetrating injury suggest that the differences in type of insult and tolerance of physiologic insults might be included in the likelihood of transfusion in the first 24 hours.
Previous studies on the associations between ambient temperature and patient admission temperatures analyzed differences across months 18 or seasons 9 , 10 , 19 in areas with historically temperate weather. 17 Tracking of daily temperature provides increased accuracy as well as giving clearer descriptive power in a linear regression model. The greater variation in temperatures seen in daily weather data in addition to the much larger sample size likely explains the difference in significance between the current results and previous negative studies.
These findings suggest a possible benefit of additional pre-hospital interventions for hypothermia in severely injured patients when ambient temperatures are decreased. Previous studies have shown benefits to temperature control with active prehospital warming. 13 , 30 At our institution, blood warmers are routinely employed in both the pre-hospital and hospital settings for severely injured patients. Future prospective evaluations of pre-hospital active warming should consider the impact of ambient temperature when determining their impact on clinical outcomes.
Limitations of this study include its retrospective, observational design, as well as the low R2 values observed in all linear regression models. The method used to obtain arrival temperature was not recorded. Significant variability in admission temperature remains unaccounted for by weather and the measures of physiologic and anatomic severity included in our models. Additional measures, including evidence of coagulopathy or base excess, could potentially provide a better fit at the cost of excluding additional patients lacking laboratory data. The low R2 value for the model for total blood products used in the first 24 hours admission also suggests that additional data points are necessary to predict total blood usage. Travel time in the trauma database utilized for this study consisted of a single time measurement from confirmed or estimated time of injury to arrival at the trauma center. Additional information on the amount of scene time and travel time for each patient could provide insights into whether either is significantly independently associated with hypothermia as well. Although usage of blood warmers is common at our institution, more detailed data on their use could inform analysis of whether cold blood was transfused to certain trauma patients.
Conclusion
Over a five-year period, colder weather was associated with lower admission temperatures among severely injured trauma patients at our institution. Colder admission temperatures are significantly associated with increased odds of transfusion and of in-hospital mortality in severely injured patients. These findings can inform decisions regarding the evaluation and implementation of prehospital warming interventions for severely injured trauma patients.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the University of Maryland Baltimore Institutional Review Board (HP-00040726).
Informed consent
Informed consent was not sought as this is not a case study or series. This study solely uses data obtained for non-research purposes.
Trial registration
Not applicable.
Guarantor
CM.
Contributorship
CM conceived the study, obtained trauma and blood transfusion data, analyzed data, and wrote the first draft of the manuscript. NS obtained weather data and co-wrote the first draft of the manuscript. MF and BJ reviewed and expanded the manuscript. All authors edited and approved the final version of the manuscript.
Provenance and peer review
Not commissioned, externally peer reviewed.