
Abstract
Introduction
The use of CT head scanning for traumatic brain injury (TBI) is a vital diagnostic tool, guided by risk stratification tools. This study aims to review the use of CT head scans and adherence to guidelines for TBI in two New Zealand emergency departments (EDs).
Methods
Retrospective observational study of patients referred for head CT from EDs to exclude a significant intracranial injury between 1st September 2018 and 31st August 2019. Clinical data were collected regarding presenting patterns, identification of injuries on CT scan and adherence to National Institute of Clinical Excellence (NICE) CT head guidelines.
Results
Out of 425 included cases, 41 (10%) patients had an intracranial injury seen on their CT head scan. Patients who reported loss (32% vs 20%, p < 0.05) or possible loss of consciousness (34% vs 22%, p < 0.05) and had a Glasgow Coma Score (GCS) <13 (17% vs 8%, p < 0.05) or focal neurology (10% vs 3%, p < 0.05) were more likely to have an intracranial injury on CT. Interestingly, 17 (41%) patients with CT diagnosed injuries had a GCS 15 and no focal neurology. NICE guidelines were adhered to in 364 (86%) of CT requests. In the 14% of cases that did not meet guideline criteria, all CT head scans were negative.
Conclusion
CT head scans are a valuable tool in TBI, and guidelines successfully identify those with significant intracranial injuries. However, the rate of significant injury for the total population requiring head CT remains low, with over 90% of head CTs in the population normal, despite high guideline compliance, perhaps identifying a role for novel objective tests in ED guidelines internationally.
Keywords
Introduction
Traumatic brain injury (TBI) is a common emergency department (ED) presentation.1,2,3 Early recognition of TBI in EDs is essential to provide timely treatment. Diagnosis and management can be challenging; the injury location and premorbid condition of a patient can lead to marked variation in the symptoms and clinical signs identifiable at presentation.
Traumatic brain injury diagnosis is determined following clinical history, neurological examination and use of CT head imaging. Rates of CT head scans have increased exponentially over the last few decades. 4 They have become a vital diagnostic tool for clinicians and have resulted in quicker diagnoses and better patient outcomes. However, the majority of TBIs that present to EDs are mild. 3 It is hard in this group in particular to determine if a CT scan will be beneficial. Only 5% of head CT scans in patients with mild TBI are positive 5 ; however, the significance of missing an injury on CT scan has so far justified this ongoing liberal use.6,7,8
The concern with the low rate of positive findings on CT scans is that the scans are not risk-free due to the radiation exposure.9,10 In addition, they confer a significant cost to the health care system not only from the radiology costs but from those related to ED waiting times and LOS. 11 This variability and escalating CT use has led to the development of clinical guidelines and pathways to aid decision-making. These tools include the Canadian CT head rule or the New Orleans Criteria 12 that combine Glasgow Coma Scores (GCS) with other clinical risk factors to determine which patients should undergo imaging. International consensus agrees on certain definitions of injury severity according to GCS scores (mild 13–15, moderate 9–12 and severe 3–8). 1 In the UK, the National Institute of Clinical Excellence (NICE) have produced guidelines for head CT use based on the Canadian CT head rules. 13
In New Zealand, the Accident Compensation Corporation (ACC) have produced evidence based guidelines for CT head scanning based on the NICE guidelines 13 advising only to request CT head scans in trauma patients when indicated by a validated clinical decision rule. This is in keeping with the Choosing Wisely campaign statements published by the Australasian College of Emergency Medicine (ACEM) and supported by the Royal Australasian and New Zealand College of Radiologists (RANZCR). 14
This study aims to characterize the use of CT head scans in two New Zealand emergency departments, a major referral centre and a regional/rural centre. In particular, it will aim to review presenting patterns, injury identification with CT scans and adherence to clinical guidelines. The secondary aim is to review if there are any differences in presenting patterns, CT results and guideline compliance between the two EDs included and according to age.
Methods
Study design and setting
Nice guidelines for CT head in adults.
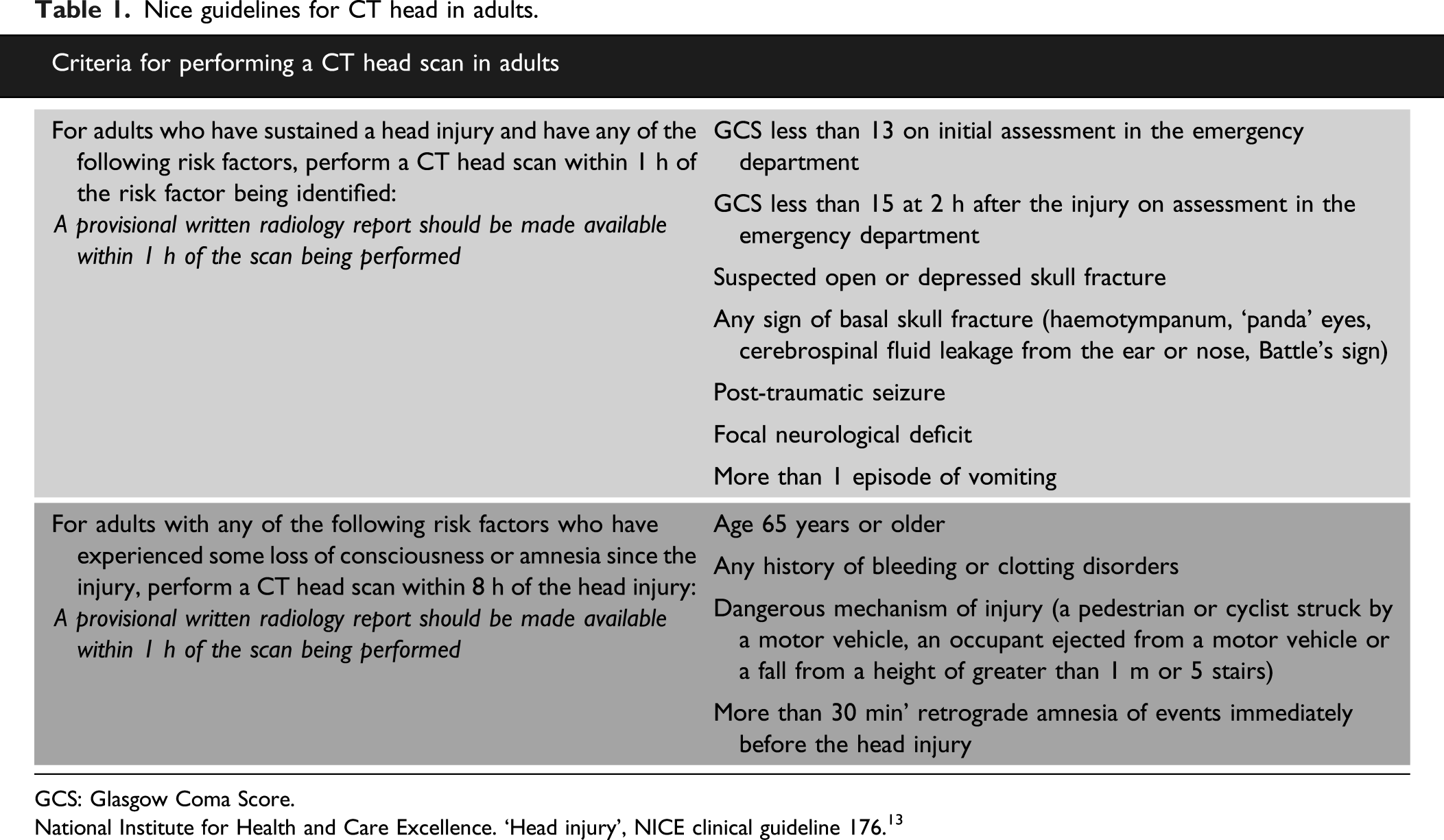
GCS: Glasgow Coma Score.
National Institute for Health and Care Excellence. ‘Head injury’, NICE clinical guideline 176. 13
Patient selection
Patients with TBI were screened using the radiology database. CT head indication is a free text field in the database, therefore to generate a sample inclusive of TBI patients, the words ‘injury’ and ‘trauma’ were flagged from the CT head indication field. Cases were included in the analysis if patients were over 18 years of age with a clear history of trauma presenting within 48 h of the suspected injury. Patients were excluded if they had a pre-existing acute brain injury, if the CT scan was cancelled after the initial request or if an emergency department doctor did not see the patient.
Data collection
Patient records were reviewed and data collected included demographics, presenting features, CT head indication, CT head result and CT wait times. A data collection form was developed using a REDCap database hosted by the University of Otago (Version 10.1.2). Data were de-identified at time of data entry and a unique study ID was created for each case. All questions were coded into yes/no fields or single radio button options to limit variation in responses. Adherence to the NICE guideline was reviewed based on documentation of CT indication. A clinically important positive head CT finding was defined as the presence of any of the following criteria: skull fracture, pneumocephalus, intracranial haemorrhage or contusion, traumatic infarction, diffuse axonal injury or signs of herniation. Patients with CT scans meeting these criteria will be recorded as CT positive, and those not meeting these criteria will be recorded as CT negative. The data dictionary is available as online Supplementary Material.
Statistical methods
Data analysis was completed using SPSS software (SPSS Inc. IBM Corp. Released 2019. SPSS Statistics for Windows, Version 26.0). To describe the data, frequency and proportions are displayed in the included tables. Medians with interquartile ranges were calculated for skewed continuous data. The null hypotheses were that there would be no difference between the age comparator groups and the two ED departments regarding presenting patterns, CT findings and guideline compliance. Chi squared tests or Fisher Exact tests were used to compare proportions where appropriate and Mann Whitney U testing was performed to compare continuous skewed data. Missing data were not included in statistical testing.
Results
Figure 1 shows the case selection process and Table 2 shows the baseline characteristics of all patients and two comparator groups (age and department). The age group cut-off at 65 years matches the NICE guideline risk stratification criteria. Case selection process. Baseline characteristics. GCS: Glasgow Coma Score; NOAC: novel oral anticoagulant; MVA: motor vehicle accident. *p <0.05 comparison between age groups, **p <0.05 comparison between EDs. aAny report of alcohol or drug ingestion or use recorded in notes was deemed as intoxication.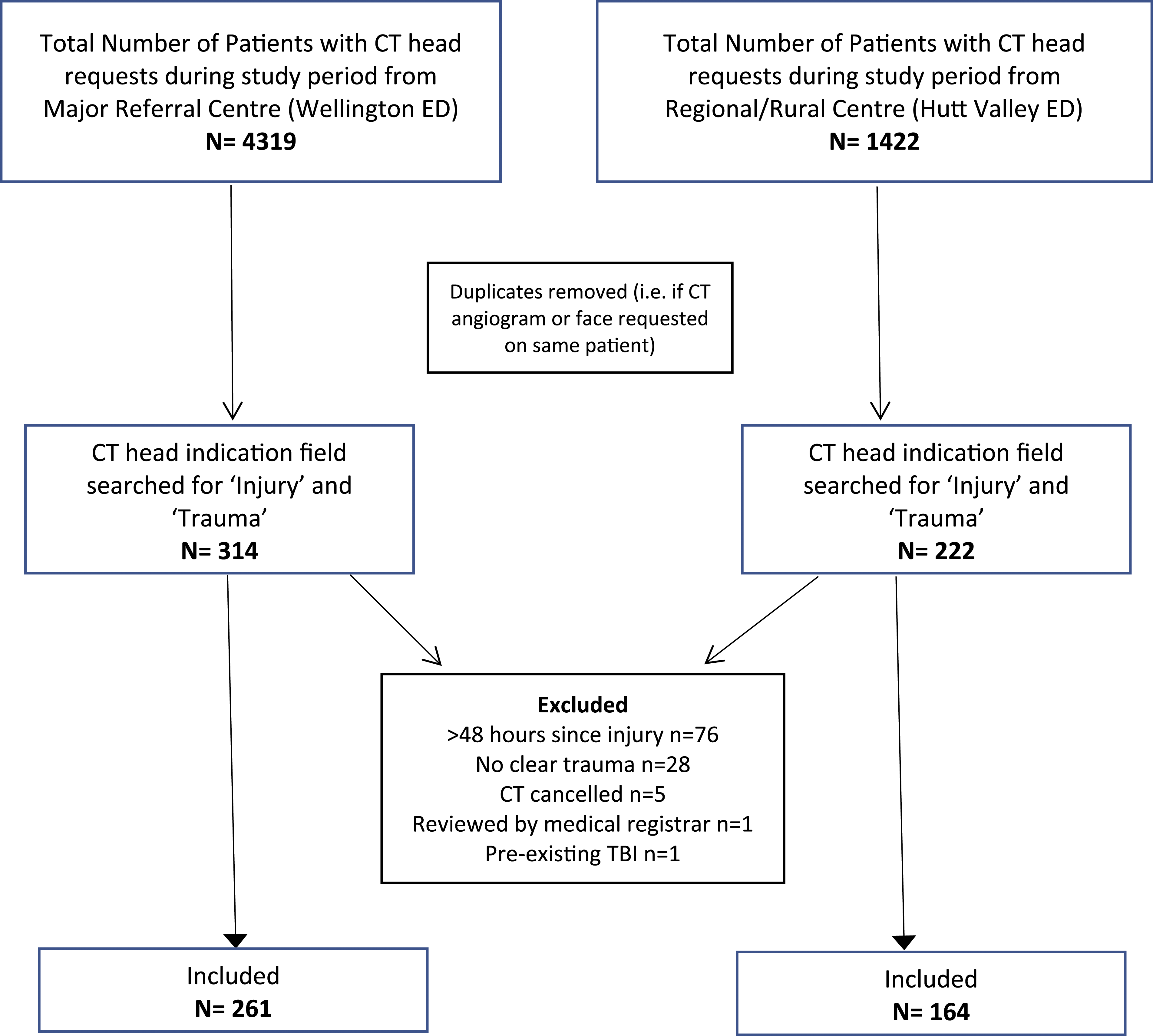
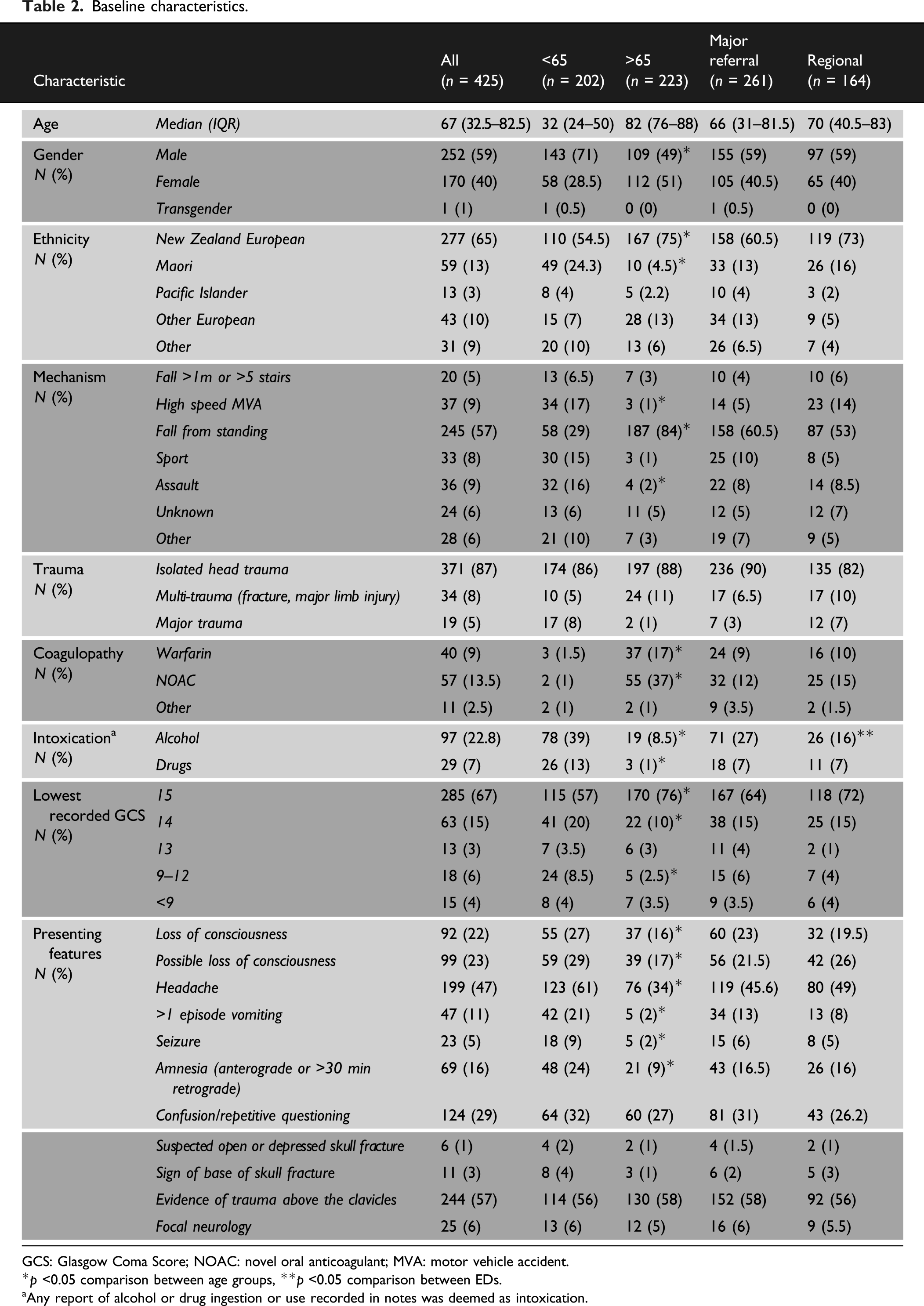
The median patient age was 67 (IQR 32.5–82.5). Most patients presented with isolated head trauma (87%) and the majority were injured following a fall from standing height (57%). Based on GCS scores, 85% of patients had a mild injury, 6% had moderate head injuries and 4% had severe head injuries. Patients <65 were more likely to have a headache and a GCS <15 and have risk factors such as loss or possible loss of consciousness (LOC) and amnesia. Patients >65 were more likely to be on anticoagulation therapy.
There were no significant difference in demographics between the two EDs. Patients presenting to the major referral centre were more likely to be intoxicated (27% vs 16%, p < 0.05); otherwise, there were no differences between presenting features, severity or type of trauma between the departments.
Indications for CT scanning and compliance with NICE guidelines
CT Indication according to risk factors identified in NICE guidelines.
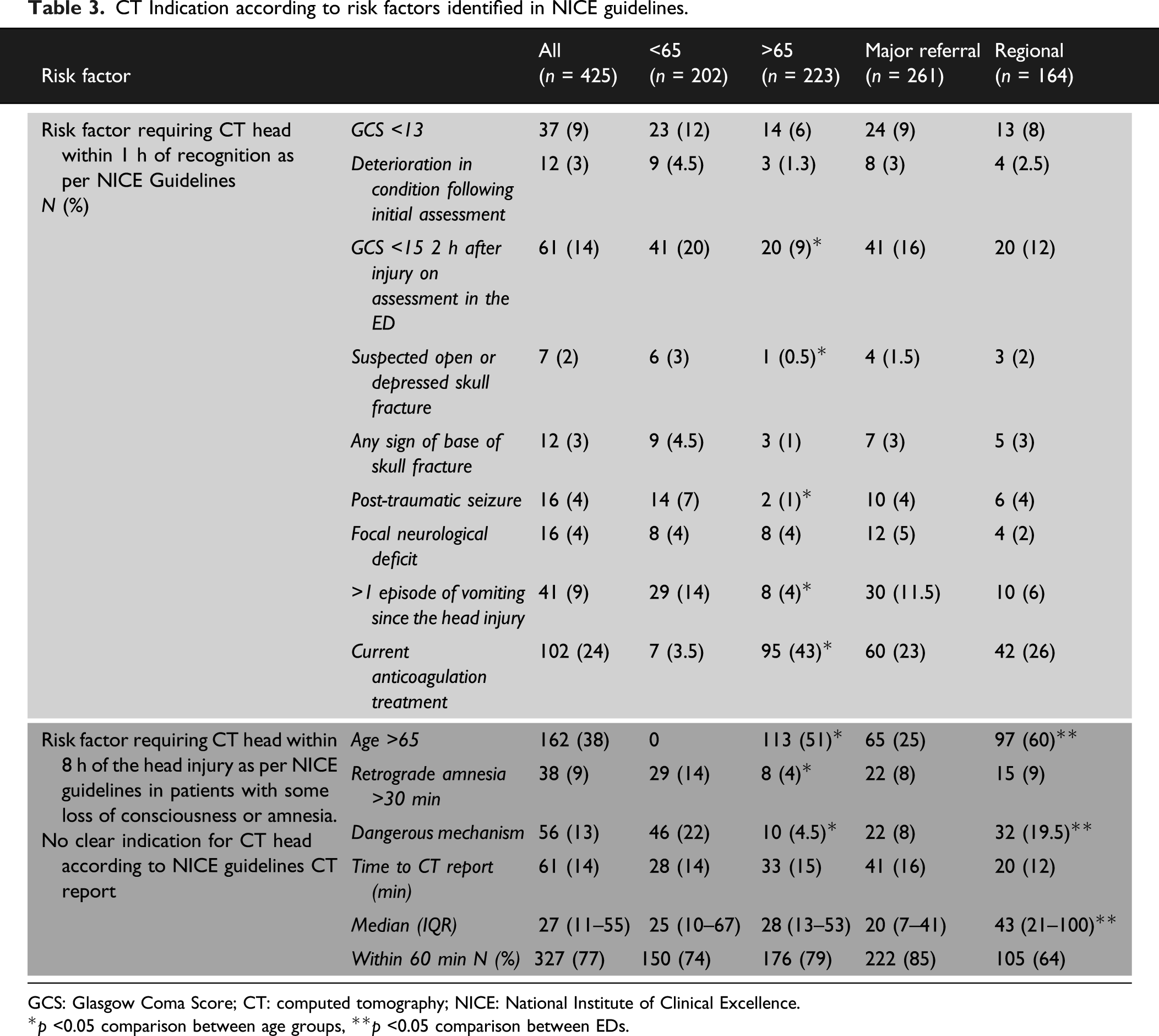
GCS: Glasgow Coma Score; CT: computed tomography; NICE: National Institute of Clinical Excellence.
*p <0.05 comparison between age groups, **p <0.05 comparison between EDs.
The most common indication for CT scanning at both sites was age >65 with some LOC or amnesia (38%). In those <65, 22% underwent CT scanning because of a dangerous mechanism with some LOC or amnesia (vs 4.5%, p < 0.05) and 14% underwent CT scanning because of >30 min of retrograde amnesia (vs 4%, p < 0.05).
The results showed that 61/425 (14%) of CT head scans performed did not clearly meet NICE criteria. Twenty-four of these cases had CTs requested because of their age, but they did not have any LOC or amnesia and no other risk factors were present. In 14 cases, patients were intoxicated with alcohol and it was noted that this was limiting assessment. In those <65, 43% of those not meeting criteria were intoxicated with alcohol affecting assessment. CT head reports were reported within 1 h in 77% of cases as recommended by NICE guidelines. Median time to CT report was longer at the regional centre (median time 28 (IQR 13–53) minutes vs 43 (IQR 21–100) minutes, p < 0.05).
CT results and characteristics of significant injuries
CT results and injuries identified.
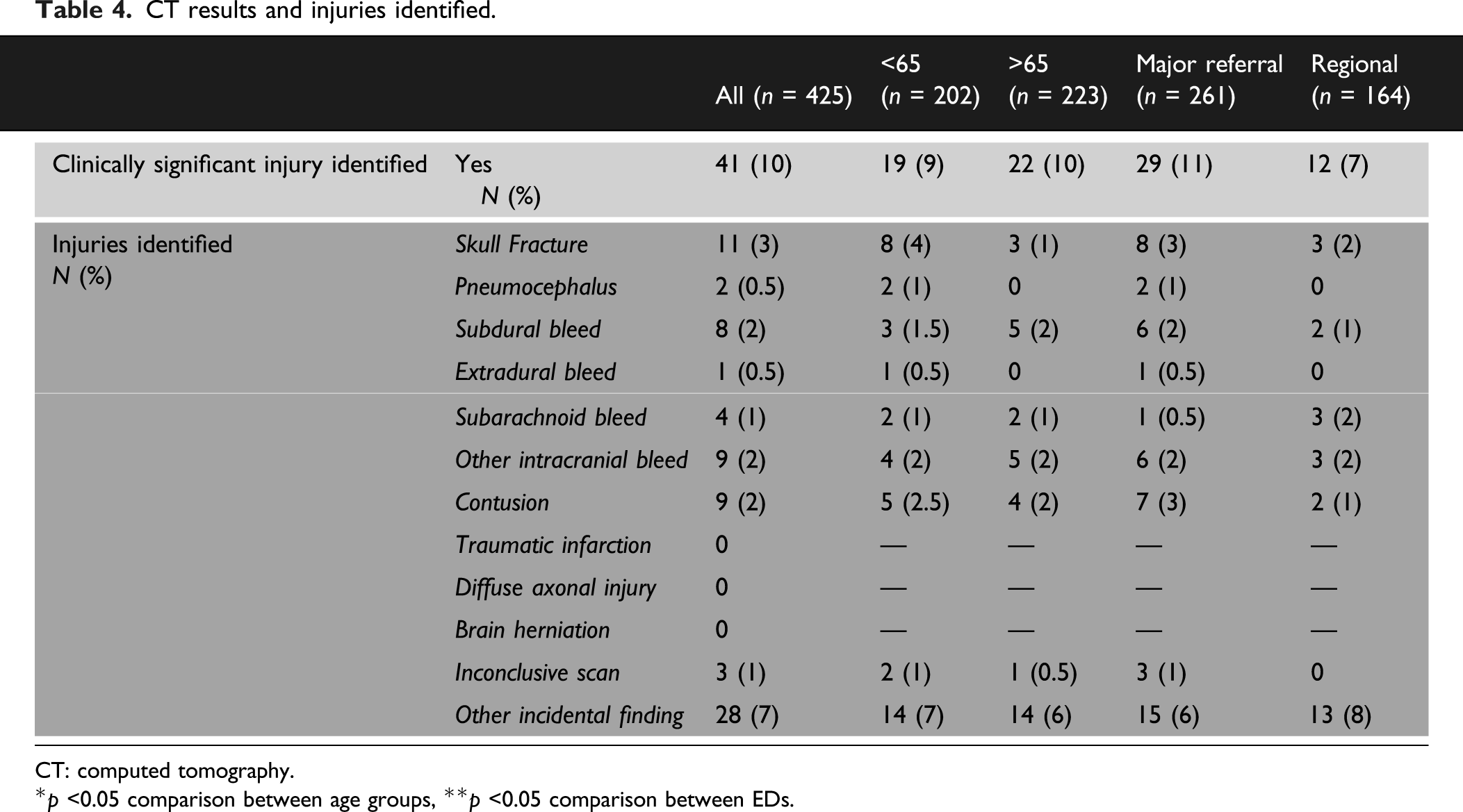
CT: computed tomography.
*p <0.05 comparison between age groups, **p <0.05 comparison between EDs.
Characteristics of patients identified with clinically significant injury on head CT scan.
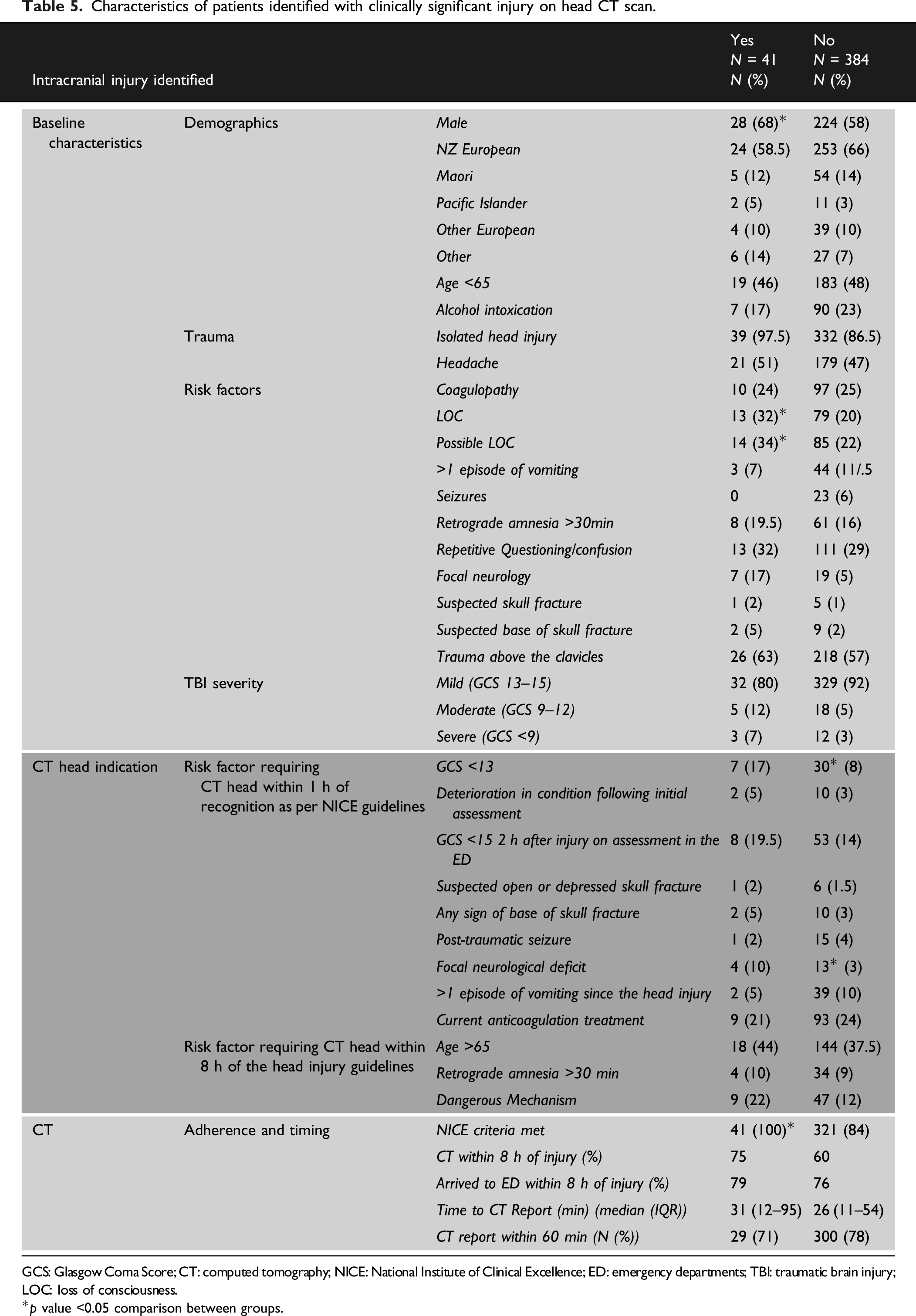
GCS: Glasgow Coma Score; CT: computed tomography; NICE: National Institute of Clinical Excellence; ED: emergency departments; TBI: traumatic brain injury; LOC: loss of consciousness.
*p value <0.05 comparison between groups.
Patients with a positive CT scan were significantly more likely to report loss or possible LOC and on examination were more likely to have a GCS <13 and focal neurology. Interestingly, 17/41 (41%) of patients with a significant injury identified had a GCS of 15 and no focal neurology. Nine of these 17 patients were on anticoagulation, 8 were >65 with possible LOC or confusion, 4 had a dangerous mechanism with possible LOC 2 had >1 vomit, 1 had >30 min of retrograde amnesia, 1 had a suspected base of skull fracture fracture and 1 had a suspected skull fracture. Regarding patient outcomes, 1% (4/425) of patients required neurosurgical intervention and 3% (14/425) required ICU. 40% (171/425) were discharged from the ED and 24% (101/425) were admitted to an EDOU.
Discussion
Our results show that 10% of patients who present to EDs with TBI had a clinically significant injury identified on CT scan, and 1% required neurosurgical intervention. The majority of head injuries occurred in males were mild and due to isolated head trauma. Those with a reduced GCS and focal neurology at presentation were more likely to have a positive CT scan. Interestingly, one in four patients with a positive CT had a GCS 15, no focal neurology and were not on anticoagulation therapy.
National Institute of Clinical Excellence guidelines were adhered to in 86% of cases. Importantly, all positive CT scans were identified with the use of NICE criteria in our study and those who did not meet criteria had negative head CT scans. This implies the guideline is relevant, valid and ED doctors support its clinical application. A systematic review 16 investigating the adherence to guidelines in TBI showed that international compliance was quite variable between 18% and 100%. Adherence was highest in centres using guidelines based on strong evidence. Adherence to the NICE CT scan guidance was highest, reaching 70–100% in the five studies referenced. 16
Despite high compliance, this study does not prove that the NICE guideline is always clinically safe. In a larger study, 17 2.4% of patients with a positive CT scan did not meet NICE criteria. It is reasonable for clinicians to sometimes deviate from guidelines if their clinical judgement compels them to. However, one could argue that patients with negative CTs who did not meet NICE criteria had unnecessary exposure to radiation. This could be true for 14% of patients in this study, which also has an impact on radiology use and ED length of stay.
Ninety percent of CT head scans performed in this study were negative. It is unlikely improving guideline compliance to 100% will significantly reduce the proportion of scans that are negative. Looking only at those patients meeting guideline indications, 11.2% were positive compared to 9.6% in the total cohort, so there would be a very small difference. Additional tools beyond guidelines would therefore be needed to significantly reduce the need for CT scans to exclude a clinically significant injury.
One in ten scans (10%) performed identified a clinically significant intracranial injury. Prevalence of significant injury in Europe and Australasia has been reported at 8–9%.17,18 The slightly higher incidence in this study may represent better selection of patients for CT in our study, or conversely it could mean that the doctors were being over cautious and under ordering scans. It is not possible to determine this from our study and further prospective analysis would be required. Both departments included in this study have a high level of Emergency Medicine Specialist supervision which could result in better risk stratification. To the authors’ knowledge, no significant injuries were missed during the study period. The most common injury identified on CT scan was skull fractures followed by intracranial bleeding, similar to findings in other studies.1,17,19
Unsurprisingly, it was significantly more likely for those who had lost or may have lost consciousness and had a GCS <13 and those with focal neurology to have a significant injury on CT scan. Of note, 40% of patients with a significant CT finding had a GCS of 15 with no focal neurology. Furthermore, half had no headache and 80% were classed according to GCS scores as having a mild head injury. This is not an anomalous outcome as other research supports these findings; for example, studies from Europe and the UK show that between 58% and 64% of patients with significant intracranial injuries seen on CT scan had a GCS 15.17,19 Clinically this makes risk stratification without the aid of clinical tools and guidelines difficult and means that clinicians cannot be reassured when a patient appears clinically unharmed. Significant intracranial pathology cannot be excluded based solely on clinical history, examination and GCS determination, again exposing the limitations of this approach and justifying the ongoing use of the NICE guidelines despite the low yield of injuries seen following CT head scanning.
CT head scans remain a vital diagnostic tool for ED clinicians. They are widely available, easily interpreted and able to detect life-threatening injuries rapidly. 20 However, in mild TBI particularly, finding the balance that minimizes unnecessary radiation exposure and economic costs whilst ensuring that patients with potentially dangerous intracranial hemorrhages are identified remains challenging. 20 Because of the current limitations excluding TBI clinically in EDs, research into the detection and use of objectively measured clinical biomarkers has increased exponentially over the last decade. Evidence supports the use of biomarkers as negative predictors of acute TBI detected on CT scans.5,21 In Scandinavia and other areas of Europe, guidelines are in use that include biomarkers as objective tests to aid decisions regarding which patients require CT scans as part of their management.21,22 It has decreased CT rates by 32% and is estimated to save €71 per patient. 22
The limitations of this study relate to the data collection process and retrospective design. The method used to identify patients for this study is likely to have missed patients who did not have the words ‘injury’ or ‘trauma’ in the CT head indication field which could have led to some selection bias. Given our baseline demographics and presenting features are similar to international literature, it is likely that our sample can still draw valuable conclusions. Furthermore, compliance with guidelines was measured based on documentation rather than knowing specifically what the clinician asked and identified, this method of chart review is prone to bias. 23 However, it is largely accepted that clinical documentation including key decisions should be recorded as standard. Future prospective studies reviewing all TBI presentations including those who do not undergo CT scan would be useful to further review guideline adherence.
Conclusion
CT head scans are a valuable tool in TBI and guidelines successfully identify those with significant intracranial injuries. This study supports the ongoing use of clinical guidelines given the rate of significant injuries seen in patients with an absence of other clinical symptoms. However, the rate of significant injury for the total population requiring head CT remains low, with over 90% of head CTs in the population normal. This finding persists despite high guideline compliance, potentially highlighting a need to explore the use of novel objective biomarkers in ED TBI guidelines internationally.
Supplemental Material
sj-pdf-1-tra-10.1177_14604086211023646 – Supplemental Material for Acute traumatic brain injury and the use of head computed tomography scans in the emergency department
Supplemental Material, sj-pdf-1-tra-10.1177_14604086211023646 for Acute traumatic brain injury and the use of head computed tomography scans in the emergency department by Alice Rogan, Vimal Patel, Jane Birdling, Jessica Lockett, Harnah Simmonds, David McQuade and Peter Larsen in Trauma
Footnotes
Acknowledgements
The authors would like to thank Hutt and Wellington Emergency Departments for their data contributions; the research offices at CCDHB and HVDHB for their local approval and support; the RAG-M and University of Otago Health Committees for their approval and the University of Otago (Wellington) Department of Surgery and Anaesthesia for their expertise and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Research was conducted in accordance with ethical approval obtained from the University of Otago Human Ethics committee (Reference HD20/001).
Informed consent
Informed consent was not sought for the present study because this was a retrospective chart review of de-identified routinely collected data. Local authority approval was sought from the District Health Board in order to access this information in accordance with ethical approval.
Guarantor
AR.
Contributorship
Project design: AR, DM, and PL; data collection: AR, VP, JL, HS, and JB; analysis: AR and PL; write-up: AR, PL, DM, VP, JB, HS, and JL; final article review and agreement by all authors.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.