
Abstract
Introduction
First responders are routinely exposed to traumatic workplace incidents that can result in post-traumatic stress disorder (PTSD). First responder organizations utilize different types of peer led programs to support first responders following a critical incident including the Critical Incident Stress Management Program (CISM) and stand-alone peer support programs. Little research has been done to determine the benefits or limitations of stand-alone peer support programs on the mental health of first responders. The aim of this project was to understand what characteristics of peer support facilitate post-traumatic growth (PTG) in first responders.
Methods
A literature search was completed using the City University of Seattle library database, ResearchGate and Google Scholar. The studies used in this review were found on EBCSOhost, ProQuest, PubMed and Wiley Online. This review includes literature published since 2006 that references post-traumatic growth in first responders, and/or their preferences for support, their coping styles and organizational impacts on growth. Thematic analysis was conducted to identify the themes and patterns in the final 10 research papers.
Results
This literature review identified five themes of formal and informal peer interactions that support PTG in first responders. (1) Peer support assists first responders with the processing of traumatic events and (2) managing organizational stressors. (3) Peer support alone may not lead to PTG and requires the use of adaptive coping behaviours. (4) First responders who actively engage with peer support experience increased well-being and (5) relational safety with peers encourages disclosure that leads to post-traumatic growth.
Conclusion
Formal and informal peer support contribute to post-traumatic growth (PTG) in first responders. Further research needs to be done to differentiate between the effects of trained peer support and support from colleagues.
Keywords
Introduction
The type of peer support first responders receive in the days following a traumatic or critical incident can impact their trauma response. A critical incident is an event experienced or witnessed by a first responder that is significant enough to cause them acute stress which may ‘overcome their normal ability to cope’. 1 Not all first responders suffer from post-traumatic stress disorder (PTSD) due to critical incidents and some first responders may even experience increased wellness or post-traumatic growth (PTG - a positive psychological transformation) following a critical incident.2,3
PTG can be viewed as a ‘coping process of positive reinterpretation, positive reframing, interpretive control, or reconstrual of events’. 4 It is not considered to be a direct outcome of a traumatic experience but rather an integration of the traumatic experience ‘into a previous view of the world’. 3 PTG is a process that involves the experiencing of a traumatic event, enduring a psychological struggle and then experiencing growth because of the challenge to their belief system. 5 PTG is a response to stress that allows a person to develop new schemas resulting in better relationships with others, a greater appreciation for life, a changed set of life priorities, a change in their self-perception and even changes in religious or spiritual beliefs.1,2,6 Research shows that early interventions by first responder peer support teams can assist first responders with developing PTG. 7
The post-traumatic growth inventory (PTGI) is the most common measure of growth after a crisis. 8 The PTGI uses a self-report inventory of 21 items, grouped into five domains: ‘relating to others, new possibilities, personal strength, spiritual change and appreciation of life’. 9 There are other versions of the PTGI including a short version known as PTGI-SF, forms for children and a version that measures PTSD and PTG following a critical incident. The newest version of the PTGI, the PTGI-X, includes a component that includes spiritual-existential change items. The PTGI-X has the same five factor structure as the original model but includes other items to measure changes in spiritual and existential domain among individuals with less traditional religious beliefs. 8
First responder peer support programs vary greatly in their implementation. The Critical Incident Stress Management (CISM) model is the most commonly used crisis intervention program among Canadian first responder organizations. A study of Canadian first responder organizations found that peer support programs vary and may offer either a critical incident stress management (CISM) program, a crisis intervention program based on debriefings (Critical Incident Stress Debriefings - CISD), a stand-alone peer support program, or no peer support program. 10 There is confusion in emergency service organizations about which crisis intervention model is most appropriate. 11 Beshai and Carleton 10 found that 23% of agencies use the broader CISM model while 22% of agencies used only ‘part of a specific crisis-focused psychological intervention programs’ like CISD. Stand-alone peer support programs were only used by 20% of the Canadian first responder organizations.
Stand-alone peer support is an umbrella term that refers to peer teams that offer a wide range of support, while crisis intervention refers to specific interventions following a critical incident. Peer support differs from friends providing support because peer support members have mental health training and supervision in how to provide appropriate mental health assistance. Peer support, unlike crisis intervention, takes place at any time. Peer support also varies from professional mental health care because of a lack of power differential. 10 Stand-alone peer support is both an inherent part of crisis intervention and extends beyond crisis intervention debriefings 10 to include ongoing support for workplace and personal problems. 12
The aim of this paper is to gain a broader understanding of the characteristics of peer support that facilitate PTG in first responders. The research question for this paper is, how does peer support facilitate post-traumatic growth in first responders? This review discusses the effect of peer support, and other factors, such as coping strategies and active engagement with peers, and organizational support that may impact PTG in first responders.
Methods
This literature review provides an overview of research related to post-traumatic growth in first responders as a result of interactions with peer support. This review compared the findings of the selected research papers to provide an interpretive analysis of the literature. This review is expected to provide information that will inform future research and policy/program development to increase PTG in first responders.
Search Strategy
A literature search was conducted using the City University of Seattle library database, ResearchGate, PubMed and Google Scholar. The original search criteria for the studies were that they had to be peer reviewed, include at least one first responder type (i.e. police officers, firefighters, emergency medical services, emergency medical technicians and/or dispatchers), use post-traumatic growth as a measure of well-being and identify peer support or crisis intervention support models. There were limited results with this search criteria. A secondary search was done with the combined terms using ‘AND’: first responder and CISM, first responder and peer support, first responder and post-traumatic growth, and post-traumatic growth and peer support. A third search was done using a combination of three search words: peer support, PTG and first responder; PTG, first responder and coping; and CISM, PTG and first responders. A final search was done using the terms organizational support, first responders and PTG. The studies used in this review were found on EBCSOhost, ProQuest, PubMed and Wiley Online.
Eligibility Criteria
The final 10 studies selected for the review were chosen based on whether they included at least two of the following criteria: first responder, peer support, PTG, organizational support and social support. Studies that were excluded from the search included studies that referred to a specific model of peer support other than CISM or stand-alone peer support, and those with suicide intervention programs. Four studies were selected because of their focus on the organizational impacts of traumatic stress on first responders, which impacts growth, 13 and the preferences for support that influence the support seeking behaviour of first responders.14–16 Two studies were chosen due to their focus on first responder coping styles that influence well-being.17–18
Data Collection
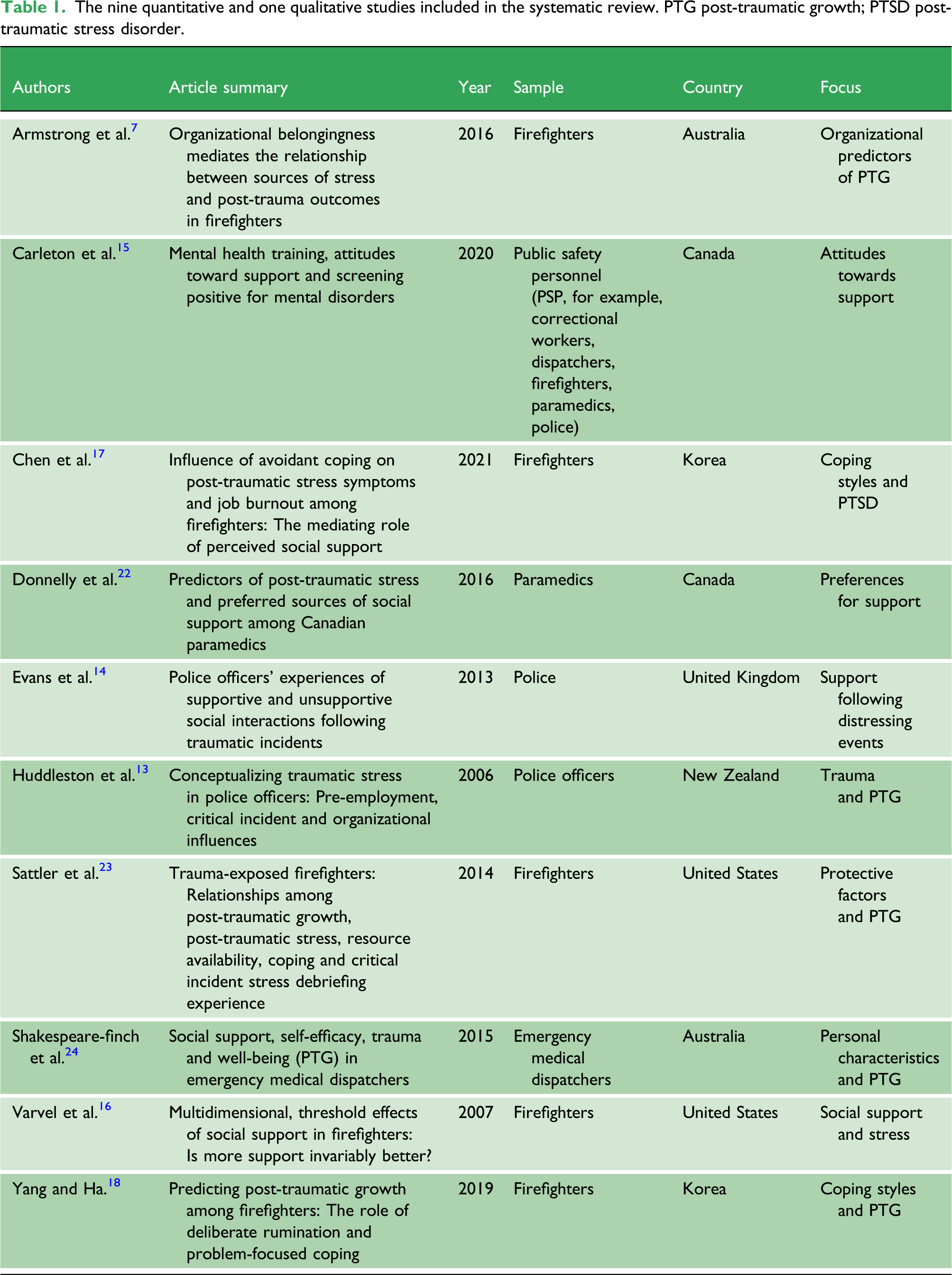
The nine quantitative and one qualitative studies included in the systematic review. PTG post-traumatic growth; PTSD post-traumatic stress disorder.
Results
Five main themes emerged from the studies that relate to the interactions between peer support and first responders that support growth: • Peer support assists with processing of traumatic events • Peers provide support with organizational stressors • Social support increases the use of coping strategies • Active engagement with peers encourages growth • Relational safety encourages disclosure
Peer support assists with processing of traumatic events
Critical incident stress debriefings were found to mitigate PTSD symptoms 22 and to support PTG in first responders.7,23 Social support also ‘provides the individual with an opportunity to re-construct their life narrative, in a manner that allows the integration of the traumatic experience’. 1 Opportunities to talk with peers assist first responders with processing difficult critical incidents that first responders are exposed to on a regular basis. CISD are often facilitated by trained peer members within first responder organizations so social support and peer support are dominant features of CISD. Sattler al 23 found that attendance at debriefings showed a positive but weak association with PTG and that a positive attitude about debriefings was positively associated with PTG.
Debriefings have been described as the ‘sharing observations and facts about the event and discussing emotional reactions and thoughts about the incident with peers and facilitators immediately following the event’. 16 Debriefings provide an opportunity to discuss the difficult characteristics of a critical incident with peers and are thought to lessen the shame and self-criticism that first responders might experience following these events. 14 Evans et al. found that social support during debriefings reminds first responders that they are ‘not alone’ and talking is ‘a vital means of processing “traumatic” events’. 14 Yang and Ha 18 found that rumination had the strongest influence on PTG in firefighters when compared to coping strategies. Rumination provides an opportunity for ‘perceiving benefits in traumatic situations and discovering meanings’. 18 First responders who expect debriefings to be helpful will benefit from the experience.
Debriefings consist of an overlap of components such as peer involvement and social support or camaraderie. 23 According to Shakespeare-finch et al., 24 social support during debriefings encourages PTG through the processing of traumatic events. Though researchers were unable to determine which of the factors of debriefings, such as social support and peer support, lead to PTG they suspect that social support from peers plays a significant role. 23 Sattler al. 23 determined that firefighters appreciate social support and camaraderie during debriefings. Camaraderie is related to social support and provides many benefits to first responders that encourage positive relationships, access to resources and ‘advice that can help individuals process the trauma and facilitate adaptive coping…’. 23 Armstrong et al. 7 found that peers provide social support during debriefings which encourages feelings of belongingness and trust.
Peers provide support with organizational stressors
A lack of organizational support can negatively impact post-trauma outcomes for first responders.13,23 Organizational stressors contribute to increased stress symptoms in first responders which negatively impact the development of PTG. 23 In fact, organizational stressors create more trauma symptoms for first responders than the traumatic experiences they witness during operational duty. 13 Varvel et al. 16 determined that for firefighters with low levels of peer support and very high levels of stress, social support has a strong positive effect on levels of occupational stress. In a study of police recruits in New Zealand, organizational stressors were the most common reason for seeking peer support within the first 12 months of employment. 13 Peer support assists first responders with managing organizational stress by providing social support to deal with stressors.
Support from supervisors was found to be more effective than support from peers in assisting first responders with managing organizational stress symptoms. In fact, Varvel et al. 16 found that support from supervisors created a greater reduction in stress symptoms in firefighters, over support from peers. Support from supervisors included tangible help, social integration support, being given more responsibility at work and the reassurance of skills. According to Varvel et al., 16 the only factor of peer support found to impact stress levels in firefighters was the opportunity for nurturance, and this finding was not statistically significant. The availability of support from supervisors provides first responders with the feeling that they are a part of a group with ‘shared interests, attitudes and activities’. 16 The reassurance of worth from supervisors contributes to the reduction in stress symptoms in firefighters. 16 While this information does not relate to peer support specifically, the findings are significant in that they show the need for comprehensive organizational support for first responders that includes peer support and support from supervisors. The findings suggest that there are limitations to the type of support that peer support can provide to first responders. First responder organizations need to be aware of the limitations when developing policy and procedures around the role of peer support.
Social support increases the use of coping strategies
The results of the studies suggest that receiving social support increases the use of personal coping strategies in managing the trauma and occupational stress associated with working as a first responder. Social support alone may not explain the variance in levels of PTG in first responders and growth may be mediated by personal coping.7,24 The researchers in the studies found that support and recommendations from peers facilitate the use of adaptive coping strategies such as meaning making, emotional management, positive thinking and problem solving. Armstrong et al. found that the effect of social support ‘on post-trauma outcomes may be mediated by other variables such as self-disclosure or moderated by the shattering of core beliefs’. 7 According to Sattler et al., peers provide advice that can help ‘individuals process the trauma and facilitate adaptive coping; and can enhance well-being’. 23 Chen et al. 17 found that social support increases positive thinking and cognitive restructuring, which alleviates depressive thinking in firefighters. Recommendations from peers may assist firefighters in ‘taking action to resolve feelings of distress, manage emotions, clarify values and life priorities’ 23 which contributes to their well-being and growth.
The use of adaptive coping behaviours also increases the confidence of first responders in managing their post-trauma outcomes. The theoretical model of PTG states that two of the psychological constructs of PTG are the finding of inner strength and looking for new possibilities8,25 which relates to the construct of self-efficacy. Self-efficacy is a ‘belief in one’s capacity to handle situations and accomplish tasks’. 24 Shakespeare-finch et al. 24 found that the combination of receiving social support and self-efficacy positively predicted PTG in dispatchers and negatively predicted PTSD. Dispatchers with greater self-efficacy ‘believed they were capable of handling tasks effectively, were better able to deal with the stressful nature of the job, and therefore experienced greater well-being’. 24 Yang and Ha 18 found that problem-focused coping significantly contributed to PTG in firefighters. Problem-focused coping strategies may include ‘active coping, focusing on the issue, positive reinterpretation, and establishing plans…’ after a traumatic event. 18
Certain personality traits in first responders are associated with the use of coping strategies that results in PTG. The use of coping strategies predicts the ability of first responders to manage stress and increase well-being while avoidant behaviours decrease well-being. Yang and Ha 18 found that firefighters who exhibit extroversion and optimism are more inclined to use problem-focused coping and adaptive coping strategies. Both extraversion and optimism were related to problem-focused coping while extraversion contributed to adaptive coping such as support seeking. 18 Chen et al. 17 found that avoidant coping increases PTSD and job burnout in firefighters. First responders with extraversion and optimism are more likely to seek support 18 from peers leading to increased growth while those with avoidant coping styles may experience increased PTSD symptoms. 17
Active Engagement with Peer Support Encourages Growth
Receiving social support and seeking social support both contribute to PTG in first responders, and there may be an interaction between these two functions. Receiving social support positively and significantly leads to PTG, and reduced levels of PTSD in first responders. 24 Mutual disclosure with trusted peers increases PTG by receiving support through formal interactions such as debriefings and informal interactions with peers. Informal interactions with peers provide opportunities to give and receive support through talking, humour and subtle indications of support. 14 Shakespeare et al. 24 found that social and peer support increases the social support systems of first responders and that active engagement with these social support systems promotes PTG in first responders. Engagement with peer support increases the social support systems of first responders and may increase the self-efficacy of first responders in managing their own mental health. 23
First responders’ need for social support consists of both giving and receiving support but that giving social support may negatively predict PTG in first responders. 24 Shakespeare-finch et al. 24 found that giving support does not lead to well-being, PTSD or PTG in dispatchers. Due to the nature of their jobs and having to listen to the distress of others throughout the workday, dispatchers do not have the emotional resources to support others and may even require additional support after hours. 24 While these findings were specific to dispatchers, it may apply to other first responder types. The need for peer support outside of working hours may increase for first responders. Of concern is that peer support members who work and provide support during the day are also expected to support their peers outside of working hours which could increase their risk of burnout. Organizations need to ensure that the well-being of peer support members is monitored and that the peer support members themselves have adequate social support and mental health resources to support them. Future research could investigate the needs of first responders outside of working hours.
Relational Safety Encourages Disclosure
Relational safety amongst peers encourages personal disclosure about the impact of the distressing events experienced by first responders. 14 While relational safety itself does not directly contribute to PTG, it is a necessary component in the development of social relationships that lead to PTG. First responders who feel safe amongst peers are more likely to disclose the difficulties they are experiencing as a result of traumatic workplace exposure. First responders who are willing to engage in peer support are selective in choosing which peers to talk to. 14 Safety in relationships is paramount to effective peer interactions that lead to PTG.
While formal interventions such as debriefings were found to contribute to PTG in first responders,7,23 first responders showed a preference for informal social support from peers and family members.14,22 Informal dialogue with peers encourages communication and camaraderie based on a mutually supportive relationship. The qualities of peer relationships that are appreciated by first responders include a close relationship, selfless listening, indirect banter, acceptance, trust and humour. 14 The informal interactions with peers provide safe interactions that may lead to increased PTG through encouraging the processing of events and receiving of social support. Without relational safety with peers, first responders may be less likely to seek support resulting in increased PTSD and lower rates of PTG.
Humour significantly predicts PTG in first responders. 14 Humour provides an opportunity to re-appraise potentially traumatic events in a way that is non-threatening. 14 Excessive emotional expression with peers was found to be risky and might interfere with a first responders' reputation. Humour among colleagues in general was viewed as positive because it ‘diverts attention away from negative emotional processing and can evoke positive emotions’. 14 Humour may be used in both formal and informal interactions with peers. While there may be some risk in disclosing to peers there are many benefits such as group cohesion, safety and emotional processing which encourage positive emotions among peers.
The studies in this review found that first responders are less likely to access support from peers 15 but that support from peers is more beneficial in providing support for operational stressors and mental health issues. 24 Carleton et al. 15 found that first responders are more likely to access support from spouses and friends than from employee and family assistance programs or from leaders within their organizations. Yet Shakespeare-finch et al. 24 suggest that the support received by coworkers or peers may be more beneficial to first responders because coworkers understand the stressors associated with the job 24 while family members and friends may not. 22 Family members and friends of first responders may be reluctant to hear about the traumatic events they witness at work because it makes them feel uncomfortable and they worry about the safety of their first responder. 14 The lack of understanding from family and friends as well as concerns about disclosure make peer support a more accessible and beneficial option for first responders dealing with organizational stress and mental health issues.
Discussion
Relationship of Findings to Theoretical Models
The findings of this review support the systemic approach to peer support outlined by Mead and MacNeil. 20 This framework suggests that first responders make meaning through interactions with each other. 20 According to the studies, a dialogue with peers encourages first responders to build an alternative perspective about their traumatic experiences, roles and relationships 20 by engaging in conversation with peers. This framework emphasizes the cognitive processing of events that may lead to PTG rather than the behavioural aspects required to assist with growth. To effectively evaluate growth in first responders, a combination of cognitive processing and behavioural changes should be measured.
The findings do not fully support the narrative approach to trauma informed peer support. The MacNeil and Mead 21 framework for peer support includes several constructs but only four of them were supported by this review. The renaming of experiences, a sense of community, mutual responsibility across peer relationships and flexibility in the kinds of supports offered, were found by the studies to contribute to PTG in first responders. Flexibility in the types of support offered was not directly referenced in the studies but may relate to formal and informal types of support as well as the preferences for informal interactions between peers. The studies do not reference the constructs of critical learning, instructive interactions (activities, meetings and conversations) with peers and boundary setting within relationships as set out in the narrative framework for peer support. 21 The focus of this review was on the supportive interactions that first responders have with peers rather than instructive interactions which may explain why the findings did not support the construct of instructive interactions. There was also no mention in any of the studies of mutual boundary setting. Boundaries are a challenge for first responder peer teams, 10 because peer team members are both coworkers and support personnel. Occasionally there are ‘mismatches between peers support personnel and those needing support’ 10 which can create ethical issues. The lack of support for this theoretical framework is likely due to the limitations of available research on PTG in first responders rather than on the framework itself.
The findings of the studies generally support the theoretical framework of PTG as outlined by Tedeschi and Calhoun. 8 They defined PTG as a positive psychological change caused by the struggle with challenging circumstances. 8 The constructs of PTG supported by the studies include the reevaluation of priorities, finding inner strength, looking for new possibilities and seeking support. 25 Peer support was found to assist with the development of the constructs of PTG as outlined in the model, apart from the discovery of spiritual meaning. 25 None of the studies measured the development of changes in spiritual beliefs that lead to growth. This lack of emphasis on spiritual development may be related to the focus of the research studies on the cognitive processes associated with growth rather than on spiritual dimensions of growth.
Limitations
There is extensive research on the outcomes of CISM but limited research on the effects of peer support for first responders, despite the widespread use of peer support in first responder agencies. The initial literature search only identified five papers with the criteria: PTG, first responders and peer support, and two of those papers contained quantitative data. The lack of research on this topic limits the findings of this review and identifies a significant gap in the research. Future research should include quantitative studies that measure PTG in first responders who use peer support and compare that with first responders who use only formal support and/or a combination of peer support and formal support.
The papers in this review do not readily distinguish between talking to trained peer support members versus talking to colleagues. Peer support members are colleagues; however, the results of this review cannot be attributed specifically to trained peer support. The lack of a clear definition of the functions of peer support across organizations and within the studies impact the findings of this review. Future research should study the differences between the specific functions of trained peer support versus informal interactions with peers/colleagues.
One of the weaknesses of the studies is that the demographics were varied. While all of the studies sampled first responders, the type of first responder, age, gender and marital status of the samples varied considerably between studies. First responders are often referred to as a distinct group, despite the fact that each first responder group (police, firefighters and dispatchers) experience trauma symptoms differently and have different needs for interventions. 26 Future research should study the impact of multiple trauma exposure, both workplace and personal trauma, on the concurrent development of PTSD and PTG in each first responder type.
All the selected studies for this review used non-probability sampling to obtain their samples, which can result in a lack of generalizability to a larger population. 27 Non-probability sampling is the non-random selection of participants based on convenience or specific criteria to collect data. The advantage to non-probability sampling in these studies is that first responders are a distinct population so the use of non-probability sampling can allow the development of theories relevant to the practical application of peer support in first responders experiencing traumatic incidents. A longitudinal study of PTSD and PTG comparing all first responder types would be beneficial to understanding the long-term effects of chronic trauma exposure on first responders and how peer support contributes to PTG across first responder types.
The sociocultural differences between the samples in the selected studies may reflect a difference in the presentation of PTG, management styles and organizational procedures across cultures. 28 The differences in culture between samples may impact the generalizability of the research to other cultures with different value systems and beliefs about how first responders should behave.
Conclusion
This systematic review revealed that the interactions of peer support that lead to the development of PTG in first responders include receiving social support during debriefings, and informal support from peers that assists with managing stressors. Peer support promotes PTG in first responders during formal and informal interactions by encouraging discussion, modelling positive coping behaviours and encouraging first responders to receive and seek support. Peers provide a buffer to ongoing stressors, encourage self-efficacy and provide first responders with alternative perspectives or advice. The formal social support provided by peer support members during debriefings encourages first responders to process traumatic workplace events.
The willingness of first responders to engage with peer support members also contributes to PTG in first responders. Personality traits such as extraversion and optimism may lead to support seeking which increases PTG, while avoidant behaviours reduce support seeking and may lead to increased PTSD. Social support from peers provides first responders opportunities to talk, use humour to evoke positive emotional processing and access subtle opportunities for support outside of the formal work environment. Peer support focused on increasing social support systems and encouraging first responders to actively engage with social support systems will increase post-trauma outcomes in first responders.
Of significance is the finding that social support alone may not lead to PTG in first responders but requires the mediation of self-coping variables and organizational support. Social support by peers may initiate the cognitive processing of events that encourages first responders to take action that leads to increased well-being and continued growth. This review indicates that there is significant value in using peer support to assist first responders with the processing of difficult events and that having access to peer support encourages PTG in first responders.
Footnotes
Author Contributions
Dr Christine Mhina provided writing assistance, technical editing, language editing, and proofreading.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
ND
Contributorship
ND researched literature and conceived the study. ND did the thematic analysis. ND wrote the first draft of the manuscript. ND reviewed and edited the manuscript and approved the final version of the manuscript.