
Abstract
Background
Acute colonic pseudo-obstruction (ACPO) is a common and potentially serious complication of surgical and trauma care. A possible contributor to ACPO development is impaired mobility. Major trauma patients, particularly those with spinal trauma, are at risk of prolonged mobility restrictions. The aim of this study was to assess the association between impaired mobility and the development of ACPO in major trauma patients undergoing acute thoraco-lumbar spinal fixation.
Methods
A retrospective cohort study involving major trauma patients admitted to a tertiary trauma facility was performed. The Hospital Trauma Registry was utilised to identify consecutive major trauma patients having urgent thoraco-lumbar spinal fixation. ACPO was defined as dilation of the transverse colon >6 cm or caecum >9 cm without mechanical cause. Immobility was defined by proxy as surgeon-prescribed mobility restrictions. Analysis was performed using multivariable logistic regression.
Results
ACPO occurred in 34 of 454 patients studied (7.5%). Colonoscopic decompression was required twice. Neostigmine or surgical resection were not required. There was no ACPO-related mortality. On multivariable regression, adjusted for confounding variables, post-operative mobility restrictions were associated with a three-fold increase in odds of ACPO (odds ratio 3.1; 95% confidence interval 1.1–8.9, P = 0.04).
Conclusion
ACPO was a common, although low-morbidity complication in this cohort. Surgically prescribed mobility restrictions were associated with higher odds of ACPO in major trauma patients having thoraco-lumbar spinal fixation. Attention should be given to early mobilisation, where possible, in these patients.
Keywords
Background
Acute colonic pseudo-obstruction (ACPO) is a poorly understood phenomenon that may complicate surgical and trauma care. The underlying pathophysiology is generally considered to be a relative excess of sympathetic over parasympathetic drive to the left colon, with subsequent non-function and progressive colonic distension.1,2 Untreated, the colon may continue to distend until ischaemic perforation occurs, with potentially grave results.
Trauma is associated with higher rates of ACPO development. The incidence of ACPO following elective surgery has been reported at 0.04% to 0.22% following spinal fixation and joint replacement in large-scale registry studies.3–5 In contrast, ACPO occurrence of 1.6%, 6 2.7% 7 and 7.5% 8 were reported following emergent hip, pelvic and spinal fixation, respectively.
The reasons for the higher incidence of ACPO following spinal trauma are not currently clear. Multi-trauma patients are exposed to a range of potential risk factors including opiate exposure, prolonged fasting and potential electrolyte derangement.1,4,5,9 Spinal trauma itself has been implicated in a causative role via disruption of the autonomic pathways supplying the colon. 10 Finally, multi-trauma patients with spinal fracture may be poorly mobile, despite spinal fixation, for prolonged periods. Reduced mobility is frequently described as a risk factor for ACPO, although the evidence supporting this appears limited to retrospective series with variable definitions of reduced mobility, that did not control for confounding variables.11–13
We hypothesised that relative immobility was one of the key drivers to the development of ACPO in the setting of thoraco-lumbar spinal trauma requiring fixation. The aim of this study was to assess the association between post-operative immobility and ACPO in a cohort of major trauma patients undergoing acute thoraco-lumbar spinal fixation after thoracic or lumbar trauma, adjusting for the potential confounding effects of other variables.
Methods
Ethics approval was granted by the Royal Melbourne Hospital Ethics Review Board, including for waiver of consent given the retrospective nature of the study according to Australian National Health and Medical Research Council guidelines. The Hospital Trauma Registry (H-TR) was utilised to identify all cases of major trauma with unstable thoracic or lumbar spinal fracture requiring fixation between November 2015 and December 2021. The hospital is a tertiary trauma facility that treats approximately half of the major trauma of the state of Victoria, Australia. The H-TR is a comprehensive database that includes all major trauma presenting to the hospital. It is maintained prospectively by trained health information officers. The H-TR includes details on the mechanism, injuries, timing and nature of interventions, comorbidity status and outcomes, including mortality and length of stay. Additional data were extracted from patient charts and cross-referenced to the registry data. Surgical intervention details, symptomology, radiological findings, interventions and progress were extracted from patient medical records; 10% of the data was recollected for quality control.
Definitions
The principal exposure of interest was mobility restrictions prescribed peri-operatively. This was defined as any weight-bearing limitation through the lower limbs prescribed by surgeons in operative notes at the time of the spinal fixation. For example, touch weight-bearing or non-weight-bearing would both be recorded as mobility restriction.
Major trauma was defined using the Victorian major trauma criteria. 14 This included: cases with mortal injury; an injury severity score (ISS) >12; intensive care unit admission for more than 24 hours; or urgent surgery to the head, chest, abdomen, spine or pelvis within 48 hours.
The primary outcome, ACPO, was defined as symptomatic colon dilatation (transverse colon >6 cm or caecum >9 cm) in the absence of distal mechanical obstruction or identifiable cause of functional obstruction as previously described.15,16 Imaging included both abdominal X-ray and computed tomography. Maximal diameter was measured using imaging software if not reported.
Post-operative analgesia type was categorised as patient-controlled intravenous opiate use (PCA), epidural anaesthesia and enteral analgesia. For analysis, this was dichotomised as PCA use versus non-use. Level of thoraco-lumbar fracture was categorised as thoracic or lumbar depending on predominant distribution and spinal surgical approach was defined as posterior or other (comprising anterior or circumferential). Injury pattern was considered as an important potential confounder. This was categorised into two summary variables: Major non-orthopaedic injury – including traumatic brain injury; major chest injury (organ injury severity score (ISS) >2) and abdominal solid organ injury or laparotomy; and major non-spinal orthopaedic injury, including pelvic and limb fracture. Soft tissue injuries were not recorded. Electrolyte deficiency was defined as any replacement of magnesium (oral or intravenous) or potassium excluding maintenance fluid prescriptions.
The primary outcome was development of ACPO according to the above definition. Additional outcomes included length of hospital stay, interventions required and mortality rates.
Statistical analysis
All statistical analyses was performed using STATA (Stata 17, Statacorp, TX USA).
Baseline data were presented as counts, percentages, median values and interquartile ranges. Regression analysis results were presented as odds ratio, 95% confidence intervals (CI) and P-values. Univariable logistic regression analysis was performed of main variables with odds of development of ACPO as the main outcome of interest.
A Directed Acyclic Graph (DAG) was used to assess which variables could be considered as potentially confounding variables in the association between mobility status and development of ACPO. The primary variables identified as potential confounders including age and gender, American Society of Anesthesiologists (ASA) score, ISS, injury patterns (as reflected in the combined variables of major non-orthopaedic injury and non-spinal orthopaedic injury) as well as opiate exposure, reflected in PCA use, electrolyte replacement and spinal cord injury.
Multivariable logistic regression was performed with mobility restrictions as the exposure of interest and APCO as the outcome of interest, adjusted for the potentially confounding effects of the co-variables selected from the DAG. Cases with missing values from these variables were not included in the multivariable regression.
Results
The H-TR identified 460 patients with major trauma undergoing thoraco-lumbar spinal arthrodesis. Six cases were excluded as three did not undergo thoraco-lumbar spinal arthrodesis, one underwent delayed repair in a subsequent admission and two patients were missing clinical notes. Of the remaining 454, a total of 34 cases of ACPO were identified (7.5%). Dilated colon was seen on imaging in two patients but not considered as ACPO, due to diagnoses of Clostridium difficile colitis and mechanical obstruction respectively. Post-operative mobility status was not documented in three patients.
No mortality from ACPO was seen. No patients required surgery or neostigmine, two patients underwent colonoscopic decompression and the remainder were successfully treated medically, including enema and rectal tube utilisation. Full details on treatment have been reported elsewhere. 8
Demographics and baseline comparisons are reported in Table 1. Age, gender, ASA score and comorbidity status were similar across the two groups. However, patients with mobility restrictions prescribed tended to have higher ISS and higher rates of associated injuries, including chest wall, abdominal and other fractures. Spinal fracture distribution and surgical management were broadly similar. In addition, length of stay was substantially longer in patients with prescribed mobility restrictions (median 19 days vs. 9 days).
Demographics.
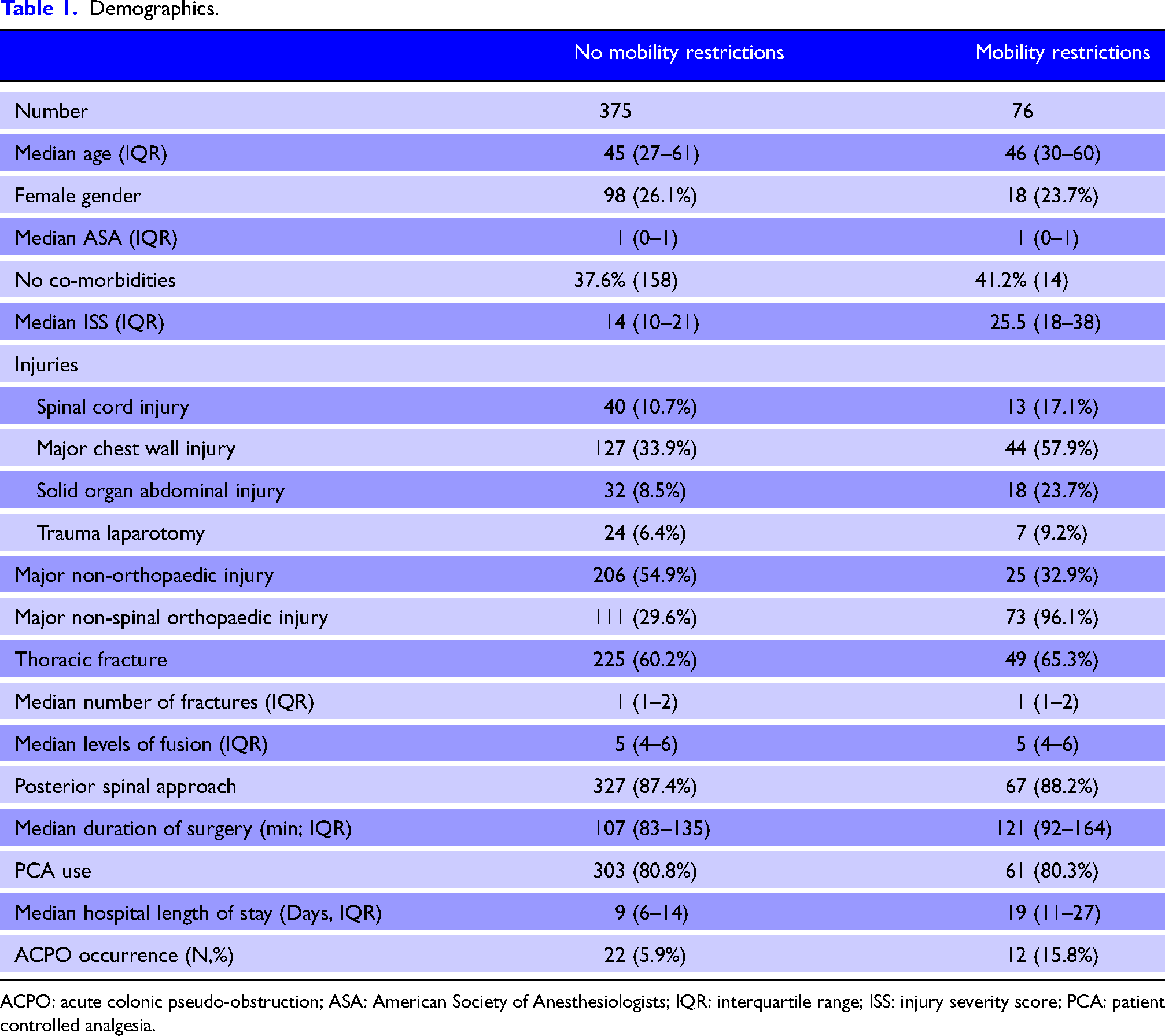
ACPO: acute colonic pseudo-obstruction; ASA: American Society of Anesthesiologists; IQR: interquartile range; ISS: injury severity score; PCA: patient controlled analgesia.
Univariable regression
The findings of univariable regression are reported in Table 2. Post-operative mobility restrictions were associated with an OR of 3.0 (95% CI: 1.4–6.0, P < 0.01) for the development of ACPO.
Univariable logistic regression for development of ACPO.
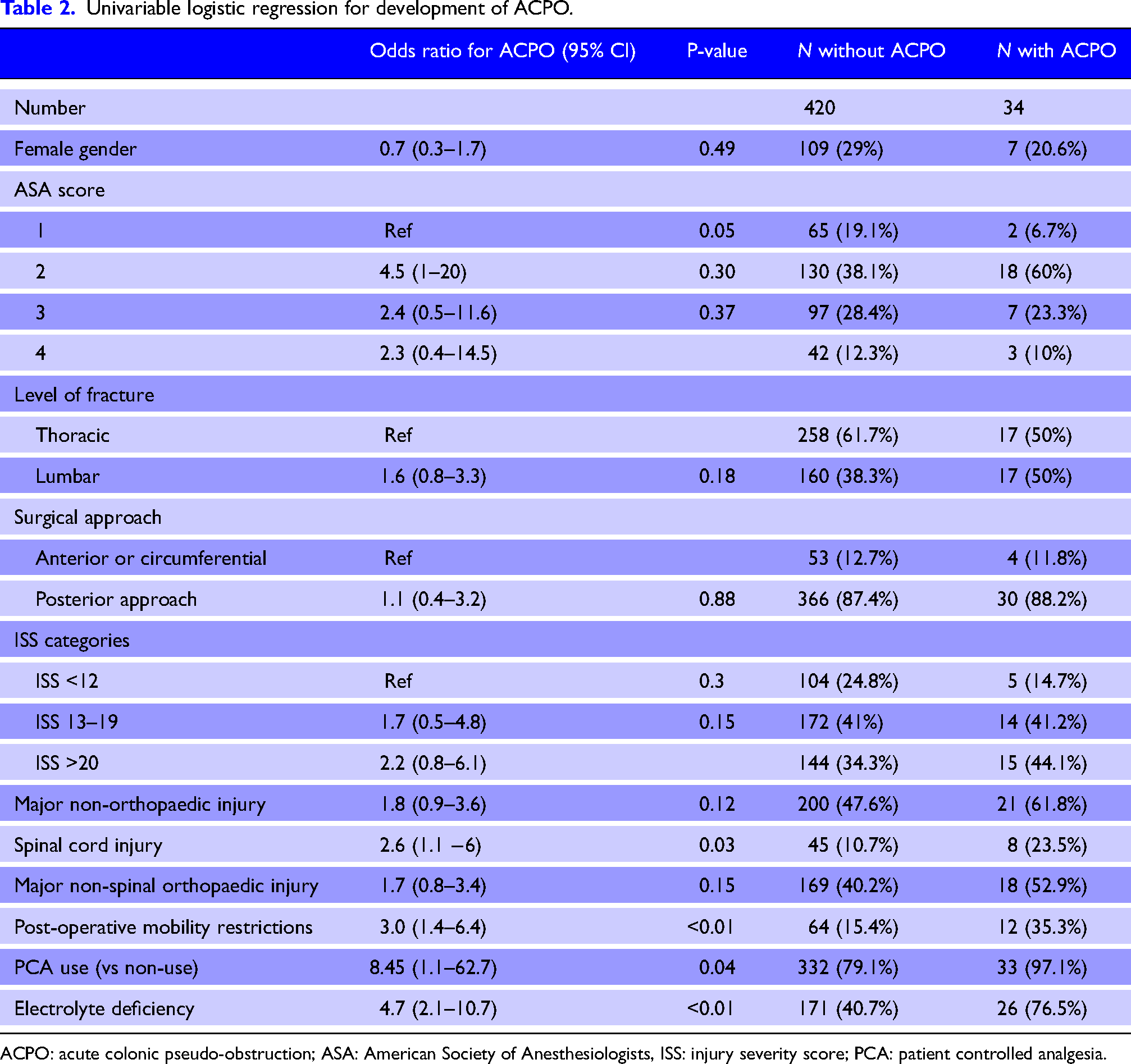
ACPO: acute colonic pseudo-obstruction; ASA: American Society of Anesthesiologists, ISS: injury severity score; PCA: patient controlled analgesia.
There was no evidence of an association between ACPO development and age, ISS score, fracture level, surgical approach or gender. Electrolyte deficiency had a strong relationship with ACPO development (OR: 4.7; 95% CI: 2.1–10.7, P < 0.01). PCA use had a strong correlation with ACPO development, however this was limited by very low numbers. A single patient developed ACPO in the absence of PCA use, making this data difficult to interpret.
Multivariable regression
Multivariable analysis was performed using logistic regression, controlling for potential confounders as identified in the DAG (Table 3). ASA score was initially planned for inclusion in the model, though was poorly recorded, such that 80 missing values were identified; to avoid excessive reduction in sample size, this was excluded from the model. After adjusting for the effects of age, gender, ISS and injury patterns, electrolyte deficiency and spinal cord injury, post-operative mobility restrictions retained evidence of an association with ACPO (OR: 3.1, 95% CI: 1.1–8.9, P = 0.04). Electrolyte deficiency remained a strong association with ACPO development in this model (OR: 5.1, 95% CI: 2.1–12.1).
A sensitivity analysis was performed including ASA score, with only minimal change to the effect of mobility restrictions (OR: 3.1, 95% CI: 1.0–9.6, P = 0.05, N = 361). PCA use was also excluded from the model due to the low numbers (single event without PCA) and statistical unreliability. A second sensitivity analysis was performed including PCA use, with some slight attenuation of the effect of mobility restrictions (OR: 2.8, 95% CI: 0.9–8.8, P = 0.08).
Spinal cord injury had some evidence of association with ACPO development on univariable logistic regression (OR: 2.5, 95% CI: 1.1–6.0, P = 0.03), which remained borderline significant on multivariable logistic regression analysis (OR: 2.6, 95% CI: 1.0–6.8, P = 0.05).
Multivariable logistic regression for effect of mobility restrictions on ACPO development, after adjusting for gender, age, ISS, other injuries and electrolyte deficiency.
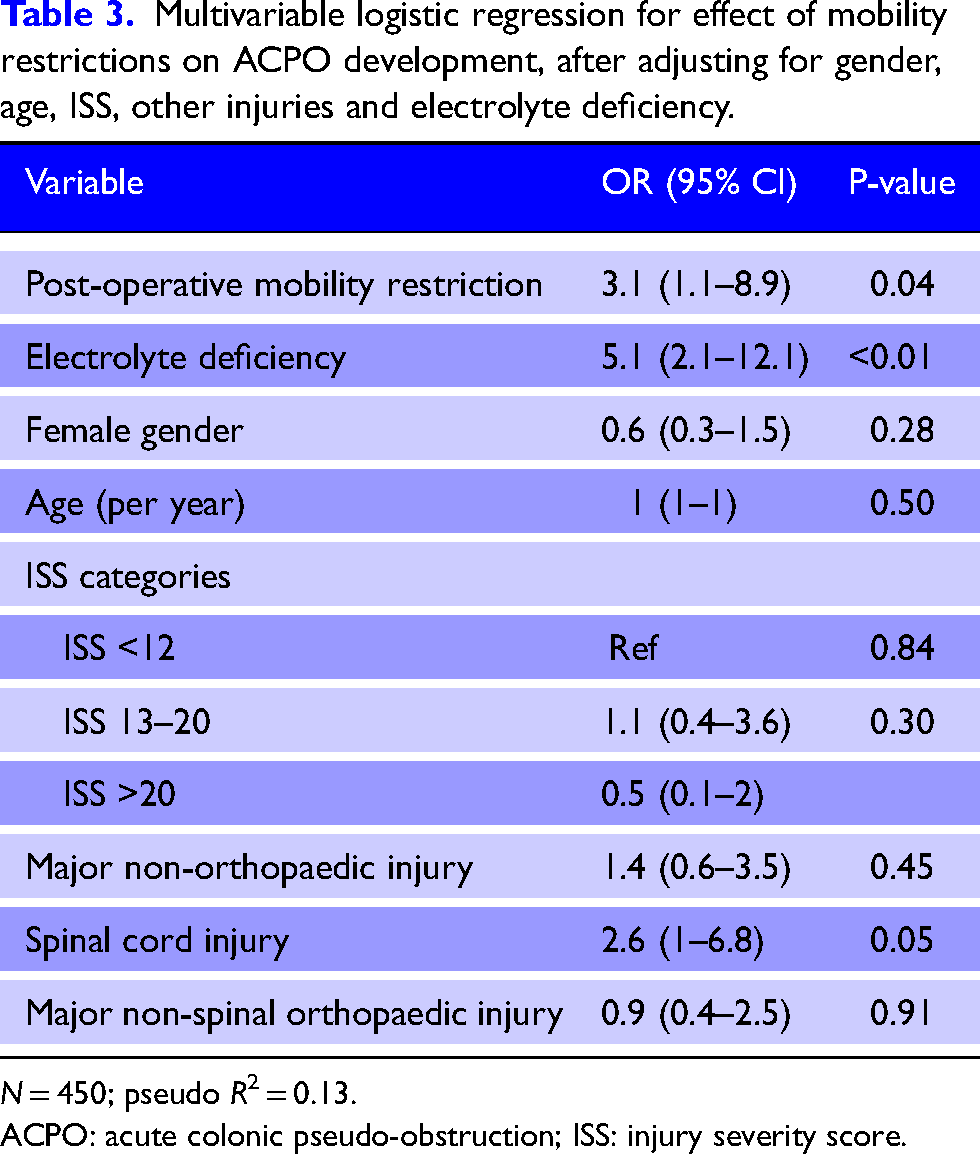
N = 450; pseudo R2 = 0.13.
ACPO: acute colonic pseudo-obstruction; ISS: injury severity score.
Discussion
ACPO in this population of major trauma patients undergoing urgent spinal fixation was a relatively common but low-morbidity complication. No mortality was seen from ACPO, and no patient required surgery. This was less severe than expected, but not dissimilar to other contemporaneous studies. 17
In this study, reduced mobility, represented by mobility restrictions prescribed by surgeons at the time of spinal surgery, was associated with an approximately three-fold increased risk of ACPO. To our knowledge, this is the first report of a relationship between reduced mobility and ACPO after adjusting for potentially confounding variables. This provides further support to the hypothesis that impaired mobility contributes to ACPO development. However, the pathophysiological mechanisms behind this are unknown. Immobility has certainly been linked to constipation, 18 though even there the mechanism is not yet understood. There remains considerable room for research to understand the pathophysiology underlying ACPO.
The chief limitation to this study relates to defining and recording reduced mobility. We used a proxy measurement of prescribed, post-operative mobility restrictions to provide a standardised measure. However, this does not consider gradations in degree of mobility, and nor does it necessarily reflect actual mobility observed. Non-compliance with mobility recommendations (whether encouraging or limiting activity) reduces the clinical accuracy of this proxy measure. Other studies that have reported on post-operative mobility have also described poor mobility in vague terms, such as slow progression relative to a standard physiotherapy reference, 11 or ‘delay to mobilisation’. 12 Improved precision in the measurement of mobility would likely require a prospective study with dedicated assessment of mobility each day.
In addition, whilst all attempts were made to identify and reduce confounding via DAG and multivariable logistic regression, residual bias remains a potential weakness in this retrospective cohort. One potential residual confounder is opiate exposure. Numerous studies have linked opiate exposure, including PCA use, with ACPO development.6,9,19–21 In this study, opiate exposure could only be recorded via the mode of delivery, such as PCA use. Here, the single event that occurred without a PCA makes interpreting data difficult and resulted in very broad confidence intervals. Direct measurement of opiate intake via a prospective study design would enable more accurate comparison. Nonetheless, minimising opiate exposure has extensive advantages and should be promoted.
Spinal cord injury is a second potential variable confounding the relationship between ACPO and mobility restrictions. The literature has not previously reported a direct link between spinal cord injury and ACPO development, though changes to colonic function (including constipation and incontinence) are documented. 22 Mechanistically, spinal cord injury could plausibly contribute to ACPO development either via disruption of autonomic reflex pathways or via the associated immobility that may occur as a result. 10 There was some evidence of effect on multivariable regression analysis. However, this study lacked power for this factor, and a larger sample size may be required for precision.
The strong association with electrolyte deficiency is consistent with reported literature, though a causative association has yet to be established.1,5,23
Finally, there are a host of additional factors – including pre-injury gut motility, comorbidities, additional medications including dopaminergics and antipsychotics, and other complications – that all interplay to influence colonic motility and risk of ACPO, and that are not measurable through a retrospective cohort design. Ideally, a prospective study would be performed to evaluate all of these risk factors, with attention to accurate recording of actual mobility, forms and dosages of opiates and other analgesia used. This would generate a more accurate assessment of contributing aetiology. In the meantime, strategies to reduce these risk factors are in line with best practice and should be pursued.
Conclusion
ACPO was a relatively common but low-morbidity complication of emergent surgical fixation of the thoracic or lumbar spine following trauma, occurring in 7.5%.
Surgeon-prescribed mobility restrictions were associated with a three-fold increase in ACPO development in multivariable analysis, controlling for age, gender, ISS, electrolyte deficiency, injury pattern and spinal cord injury.
Consideration to minimisation of mobility restrictions and earlier post-operative mobilisation, where feasible, may help reduce rates of ACPO development. Minimisation of intravenous opiate use may also be beneficial. Further research should focus on these areas, ideally through prospective methods, to further evaluate individual risk contribution with the goal of preventing ACPO.
Footnotes
Acknowledgements
Kellie Gumm, Laura Bennett, Cheng Feng, Dilshan Udayasiri.
Author contribution
JC was involved in literature review, study design, data collection, data analysis, and writing; IH in study design, data analysis, interpretation, writing, and critical revisions and DR in study concept and design, data analysis, interpretation, writing, and revisions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Correction (July 2025):
This article has been updated to remove the Media Summary from the Declarations.