
Abstract
Background
Interprosthetic femoral fractures between ipsilateral total hip arthroplasty and total knee arthroplasty (TKA) represent an increasingly significant clinical challenge, reflecting the growing prevalence of periprosthetic fractures, rising arthroplasty rates, and an ageing population. Biomechanical studies have identified reduced interprosthetic distance and compromised cortical bone quality as key risk factors; however, clinical data guiding prophylactic management strategies—such as femoral bridge plating—remain limited.
Methods
A survey of 137 orthopaedic surgeons (118 consultants) was conducted to assess current practice and attitudes towards prophylactic femoral bridge plating. Respondents were asked about factors influencing their decision-making—such as interprosthetic distance, bone quality, and implant constraint—as well as their definitions and methods of measuring interprosthetic distance.
Results
75% of surgeons would consider prophylactic plating when the interprosthetic distance was less than two cortical diameters. 62% would prophylactically plate if there was less than 60 mm between implants. 12% stated they would never bridge. Poor bone quality (60%), traumatic indications (52%), and higher TKA constraint (31%) increased the likelihood of bridging. Surgeons varied in how they measured implant distance and whether they considered intramedullary cementing an acceptable alternative. 88% of respondents agreed this is an important clinical question, with the majority supporting future research.
Conclusion
This survey reveals significant variation in current practice regarding prophylactic femoral bridge plating. While many surgeons favour plating in cases of short interprosthetic distances or compromised bone, decision-making is multifactorial. Further clinical research is essential to develop evidence-based guidelines in this challenging area.
Keywords
Introduction
Interprosthetic fractures (IPF) between ipsilateral hip and knee arthroplasties present a complex and increasingly relevant challenge for orthopaedic surgeons, both in terms of prevention and management. Although the true incidence of IPFs remains uncertain, they are estimated to account for up to 5–7% of all periprosthetic femoral fractures (PFFs). 1 With rising arthroplasty volumes, an ageing population, and the increasing prevalence of periprosthetic fractures,2,3 the burden of IPFs is expected to grow substantially.
Prophylactic strategies to reduce the risk of IPFs have been proposed, including the use of a spanning femoral plate to bridge adjacent implants—particularly when interprosthetic distance is short, such as in the presence of a stemmed total knee arthroplasty (TKA). However, clinical evidence supporting prophylactic bridge plating remains limited. In a series of proximal femoral fractures with stemmed TKAs, Peiró et al. advocated lateral plating to overlap the constructs, reporting no major complications. 4 Similarly, Sato et al. described “whole-span plating” in 10 patients with PFFs, observing no refractures but a 90% transfusion rate, highlighting the potential physiological burden of such interventions. 5
Biomechanical investigations have sought to clarify the mechanisms underlying IPFs and the factors that increase fracture risk. Soenen et al. demonstrated, using 3D femoral models, that interprosthetic distances below 110 mm markedly increase the risk of shaft fractures, particularly in osteoporotic bone. 6 Mühling et al. found that maintaining a minimum 10 mm interprosthetic gap mitigated strain peaks in synthetic bone models. 7 Conversely, Weiser et al. reported that cortical thickness, rather than implant spacing, was the dominant factor influencing fracture risk. 8 This finding was supported by Lipoff et al., who identified thin cortices, wide medullary canals, and an increased canal-to-cortex ratio as key risk factors. 9 Similarly, Mühling et al. and Iesaka et al. observed that reduced cortical thickness and the presence of a loose stem tip both act as stress risers, increasing peak strain between implants.7,10
Unfortunately, there is a paucity of real-world clinical data on risk factors for IPFs. As such, our aim was to conduct a survey to assess current practice among lower limb arthroplasty surgeons to determine how surgeons manage cases of ipsilateral total hip arthroplasty (THA) and TKA, and whether surgeons feel there is merit to prophylactically bridging the implants to reduce the risk of IPF. We also wanted to investigate the factors which may influence a surgeon's decision to prophylactically bridge.
Methods
The senior authors (tertiary centre revision lower limb arthroplasty surgeons) met to discuss the pertinent factors associated with decision-making on interprosthetic fractures in patients with stemmed THA and TKAs. A questionnaire was created and distributed within multiple departments across England and also publicised on social media. Responses were collated in a data collection spreadsheet and analysed quantitively and qualitatively.
Results
Demographics of survey respondents
One hundred thirty-seven orthopaedic surgeons responded, of which 118 were consultants and 19 were fellows, associate specialists, or registrars. Of the 118 consultants, 67 (57%) practice both elective and trauma surgery, 41 (35%) elective only and 10 (8%) trauma only. Of the 109 consultants practicing electively, 67 (61%) work in a tertiary centre, 41 (38%) in secondary care/district general hospitals and 1 (1%) privately only. Of the 77 consultants practicing trauma, 40 (52%) work in a major trauma centre and 37 (48%) in a trauma unit.
Of the respondents, there were high numbers of primary and revision hip surgeons, and surgeons performing open reduction internal fixations for femoral periprosthetic fractures. There were lower, but still commendable, numbers of surgeons performing revision knees and endoprosthetic replacements (Figure 1).
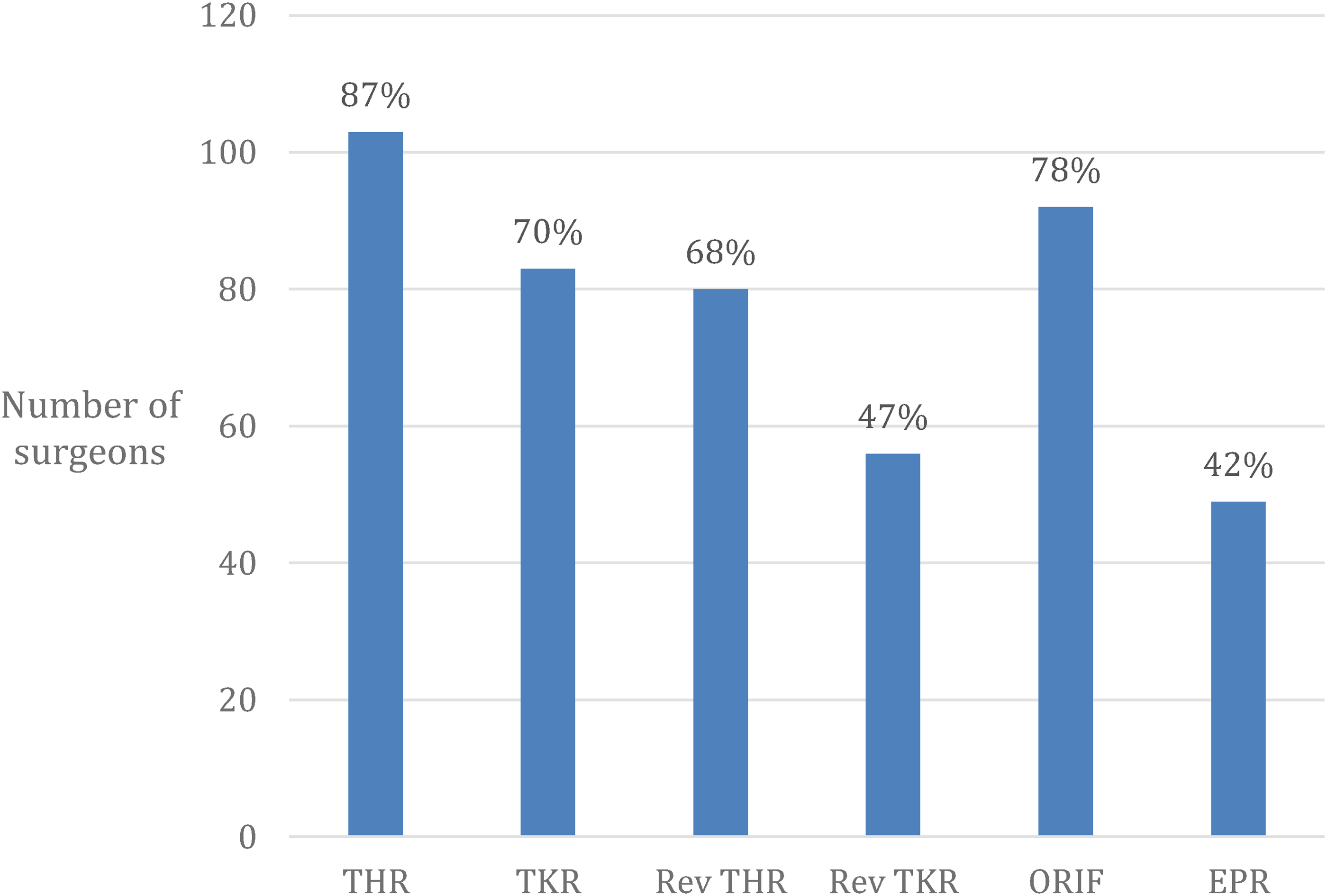
Operative practice of consultant surgeons. THR, performs over 50 primary total hip replacements per year; TKR, performs over 50 primary total knee replacements per year; Rev THR, performs over 10 revision hip replacements per year; Rev TKR, performs over 10 revision total knee replacements per year; ORIF, performs over 10 femur periprosthetic fracture open reduction internal fixations per year; EPR, performs over 5 endoprosthetic replacements per year.
When would you prophylactically bridge the femoral implants?
With respect to millimetre (mm) of unprotected diaphyseal bone; 12% of surgeons would never bridge, 40% would prefer to use number of cortical diameters to make this decision. Of those that would use mm to decide, 41/55 (75%) would bridge if less than 60 mm (Figure 2).
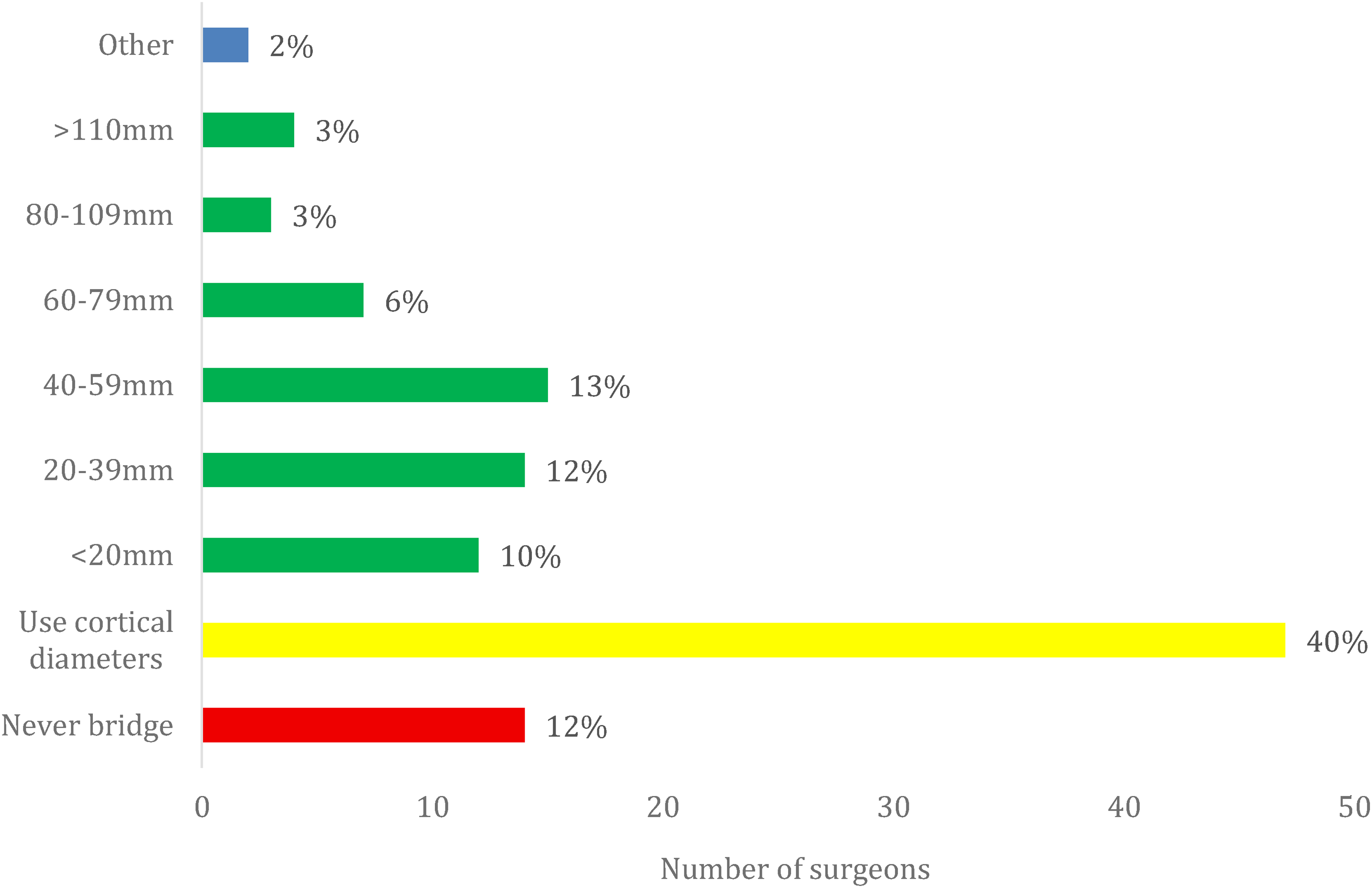
When would you bridge the femur with respect to mm of unprotected diaphyseal bone?.
With respect to number of cortical diameters between implants; 12% of surgeons would never bridge, 17% would prefer to use mm between implants to make this decision. Of those that would use cortical diameters, 51/82 (62%) would bridge if less than 2 cortical diameters (Figure 3).
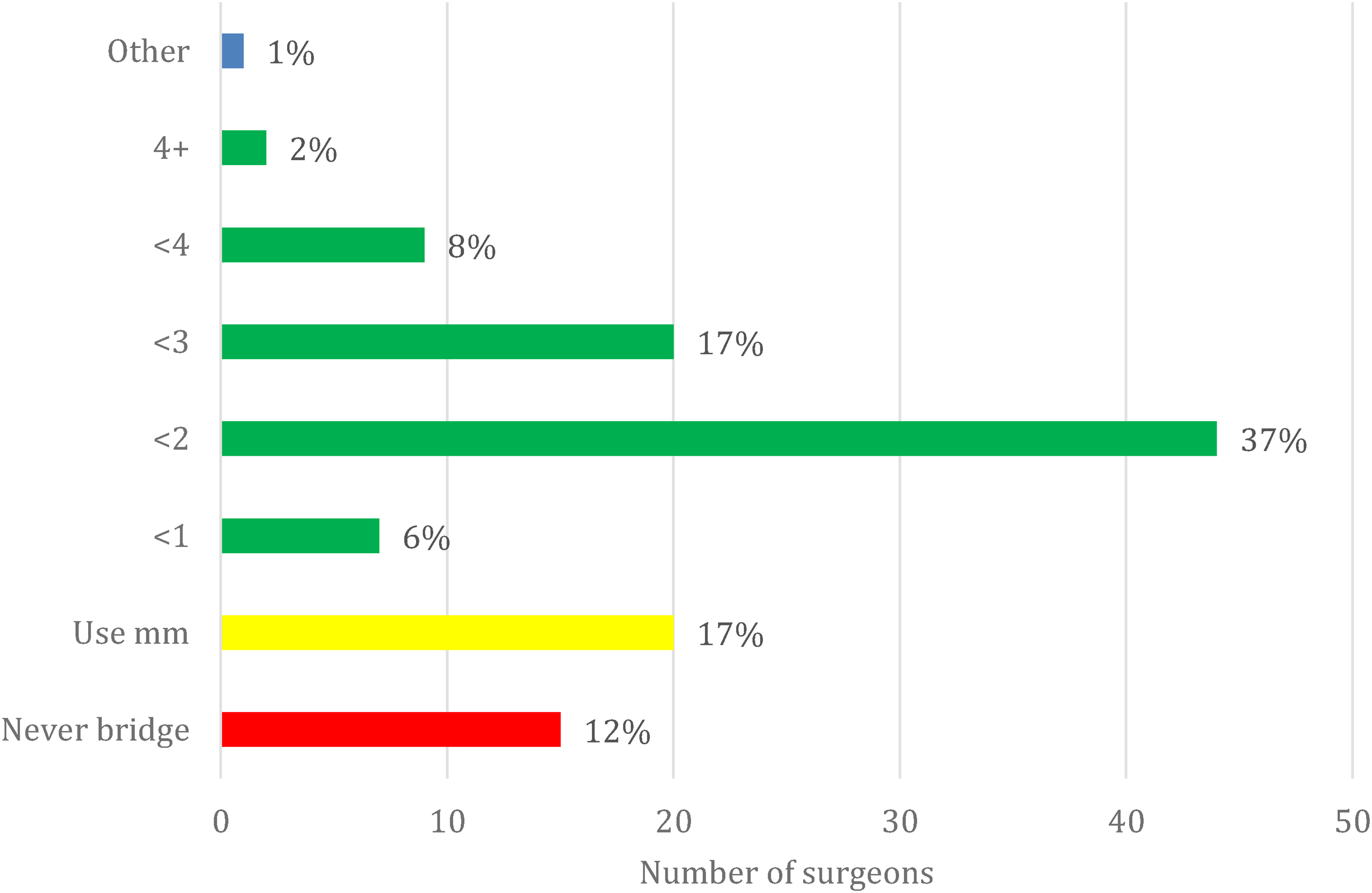
When would you bridge the femur with respect to number of cortical diameters between implants?.
Other factors that influence the decision to prophylactically bridge the femur
Seventy-one (60%) of surgeons were more likely to bridge if there was poor bone quality (e.g. known history of osteoporosis); 61 (52%) of surgeons said they were more likely to bridge if the indication for surgery was trauma and 37 (31%) of surgeons said they were more likely to bridge if the stemmed knee replacement had more constraint (e.g. hinge or distal femur replacement).
Other factors mentioned in the free text response section were the age of the patient, life expectancy, previous fragility fracture, physiological capacity of the patient to tolerate the additional surgical insult, patient's activity level, falls risk, availability of kit or company representative, and technical challenges involved in getting fixation around a stem.
Other questions
Where do you measure interprosthetic distance from?
57/118 (48%) measure from the tips of the implants, 47/118 (40%) measure from the last part of the constructs (including cement tails and cement restrictors), and 14/118 (12%) measure from the area of most meaningful cortical fixation.
Would you deem filling the canal with cement as an acceptable bridging technique?
Thirty-four (29%) of surgeons felt that cement alone could be used to prophylactically bridge the femur.
Is this an important clinical question to answer?
One hundred four (88%) felt this was an important question.
What would help with future decision-making?
78/118 (66%) felt a clinical trial would help, 63/118 (53%) said National Joint Registry data would be of worthwhile, 46/118 (39%) valued expert opinion, and 39/118 (33%) were happy with their own personal experience.
Discussion
This survey of lower limb arthroplasty consultants demonstrates that most surgeons would consider prophylactic bridge plating of the femur to reduce the risk of IPFs when the distance between hip and knee implants is less than 60 mm or two cortical diameters. However, there remains substantial variation in practice, with 12% of respondents indicating they would never bridge the femur. The decision to prophylactically plate is clearly multifactorial and influenced by both patient- and implant-related factors.
The incidence of IPF is expected to rise as a result of an ageing population and the increasing number of total hip and knee arthroplasties, including revision procedures, being performed in the UK. 2 IPF represent a devastating complication, often associated with prolonged morbidity and significant technical challenges. Management options depend on fracture configuration and implant stability, ranging from internal fixation to complex revision or endoprosthetic reconstruction. 11 These interventions are associated with high complication rates, including prosthetic joint infection, re-fracture, non-union and hardware failure, with 2-year survivorship from reoperation reported as only 71%. 12 Furthermore, the physiological impact of both the initial injury and subsequent reconstruction must be carefully considered in this typically elderly, frail patient group.
Prophylactic bridge plating to span the diaphysis between hip and knee implants has been proposed as a means of reducing the risk of IPF. Despite its theoretical benefit, the evidence base supporting this approach is limited, which is reflected in the considerable variability in clinical practice demonstrated by this survey. Prophylactic plating is not without potential drawbacks: additional surgical time, soft-tissue dissection, and the risk of further complications must be weighed against the anticipated benefit. Indeed, Taniguchi et al. reported a femoral fracture occurring despite prophylactic plating between a hip hemiarthroplasty and hinged knee prosthesis. 13 An alternative strategy to bridge the interprosthetic gap is to fill the femoral canal with cement; 29% of respondents in our study considered this an acceptable technique.
Identifying patients at highest risk of IPF remains challenging. Although biomechanical studies have demonstrated that reduced interprosthetic distance and narrow cortical width increase fracture risk,6–10 clinical decision-making is influenced by many additional factors. In our cohort, 60% of surgeons reported they were more likely to prophylactically plate in the presence of poor bone quality, defined variably as osteoporosis, osteopenia, prior fragility fracture, or radiographic cortical thinning. Half of respondents were more likely to plate when the indication for arthroplasty was trauma—patients who typically have compromised bone stock. Additionally, 31% indicated they would consider bridging when a constrained knee prosthesis was used, likely reflecting concern regarding increased force transmission at the bone–implant interface. Other factors influencing decision-making included patient frailty, activity level, falls risk, equipment availability, and the technical feasibility of fixation around an existing femoral stem.
Despite the variation in individual practice, the majority of surgeons in this survey would bridge implants with a prophylactic plate when the interprosthetic gap was less than 60 mm or two cortical diameters. This highlights a general concern among surgeons regarding the risk of IPFs, despite the lack of robust clinical evidence to guide practice. Notably, 88% of respondents agreed that this remains an important and under-researched area. The multifactorial nature of the decision-making process and the heterogeneity of patient and implant variables make the design of a definitive clinical trial particularly challenging. Even seemingly simple parameters—such as how interprosthetic distance should be measured—lack consensus among surgeons.
Further biomechanical and clinical research is therefore warranted to better define thresholds for intervention, identify patients at greatest risk, and evaluate the true efficacy and cost–benefit of prophylactic bridging in the prevention of interprosthetic femoral fractures.
Conclusion
This national survey of 118 consultant lower limb arthroplasty surgeons highlights substantial variability in the use of prophylactic bridge plating to mitigate the risk of IPFs between ipsilateral total hip and knee arthroplasties. While most respondents favoured bridging when the interprosthetic distance was less than two cortical diameters or 60 mm, a notable minority (12%) reported they would never employ this technique. Decision-making was influenced by multiple factors, underscoring the multifactorial and complex nature of this clinical problem. Further clinical studies are warranted to establish evidence-based guidelines for the prevention of IPFs in this challenging cohort.
Footnotes
Acknowledgement
The authors would like to thank the John Charnley Trust for supporting this research (no funding necessary).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.