
Abstract
Background
To evaluate visual outcomes and quality of life in soldiers after ocular trauma, with a focus on how vision impairment affects their daily overall well-being.
Methods
This cross-sectional observational study was conducted among soldiers who sustained ocular trauma in either or both eyes, resulting in best-corrected visual acuity (BCVA) of ≤6/36 in at least one eye and had been clinically stable for a minimum of six months. After ocular examination, the National Eye Institute 25-Item Visual-Function Questionnaire was introduced to measure vision-related quality of life. Data was analyzed using SPSS-version-23.0. T-test and one-way ANOVA tests were used to see the difference between groups. P < 0.05 was considered significant.
Results
Thirty-eight male participants, all with monocular vision loss, were included. Mean age at presentation was 37.3 ± 8.4years (range: 23–55years). The most common cause of injury was road-traffic accidents (42.1%). Low visual quality of life was reported in VFQ25 composite score (56.47 ± 15.97) and across all 11 subscales. Specifically, participants with BCVA ≤6/36 reported substantial difficulty in terms of ‘ocular pain’ and ‘near activities’ (p < 0.05). Also, a significant difference in ‘ocular pain’ was found between those with ‘no perception of light’ and those who had undergone removal of one eye (p = 0.00). The majority reported significant challenges in ‘role difficulties’ (p = 0.01) and ‘dependency’ (p = 0.04).
Conclusion
Ocular trauma significantly lowers visual quality of life, with substantial deficits not only in visual acuity but also in daily functioning, emotional well-being and independence. Beyond visual acuity, factors such as role difficulties, dependency, driving and mental health should be prioritized, when assessing recovery and rehabilitation needs for those recovering from trauma.
Introduction
Vision is one of the utmost powerful senses and has tangible effects on individuals’ development. Although the eyes occupy only 0.1% of the total and 0.27% of the anterior body surface area, ocular trauma is seen far more frequently than these tiny percentages would suggest. 1 Ocular trauma constitutes nearly 75% of all ocular emergencies and is one cause responsible for monocular visual loss.2–4 It remains a significant contributor to ocular morbidity among military personnel. 5
Historically, ocular trauma among soldiers was reported in approximately 3% of injuries during the Indo–Pakistani War of 1965, 4.8% during the Indo–Pakistani War of 1971, and increased to 10.5% during the Indian Peace Keeping Force deployment in Sri Lanka between 1987 and 1990.6,7 Previously, this upsurge in ocular trauma was due to increased use of fragmentation weapons, however, currently the causes of ocular trauma have shifted from combat-related incidents to more common occurrences such as workplace injuries, domestic injuries, road-traffic accidents (RTA), sports injuries, field exercises and mishandling of weapons. In addition, improvements in medical care to combat casualties will have also resulted in survival with ocular injuries when previously they would have died.
Ocular trauma causes visual disability (VD) and has a negative impact on overall quality of life (QoL).8,9 However, the literature lacks comprehensive data on how VD impacts vision-related QoL (VrQoL), which is a measure that includes not only vision but also generic health domains such as emotional well-being, mental health and social functioning, and task-oriented domains related to day-to-day visual functioning. Current assessments of VD focus on Best-Corrected Visual Acuity (BCVA) as the only single factor, but they fail to account for factors such ocular pain, inability to participate in sports, social well-being and emotional impacts of losing career prospects.
To address this gap, several tools have been developed, including the SF-36 measure and the National Eye Institute 25-Item Visual-Function Questionnaire (NEI-VFQ25). The NEI-VFQ25 is specifically designed to measure VrQoL in patients with ocular conditions, considering both functional and psychosocial aspects of vision loss.10,11
This study aims to evaluate VrQoL in soldiers who have suffered vision loss following ocular trauma using NEI-VFQ25, in order to provide a more accurate and holistic understanding of the challenges faced and to guide appropriate counselling.
Methods
A cross-sectional study was conducted at a tertiary eye care center from March 2020 to March 2021. The study was approved by the Institutional Ethics Committee, Command Hospital (Western Command), under approval number 05/04/AUG/CHWC/2020, dated 04 August 2020. This study included soldiers who sustained ocular trauma in one or both eyes with BCVA decreased to 6/36 or below in at least one eye and had been clinically stable for the last six months. Participants with any associated significant head or limb trauma that may have caused restriction on independent mobility leading to an adverse impact on QoL and participants who were unwilling or unable to undergo vision testing due to mental or physical conditions were excluded from the study. As the assessments were performed at a single time point, no prospective follow-up was undertaken, and causal inferences regarding change in QoL over time are beyond the scope of this study.
Visual disability percentage (VD%) was calculated according to the Rights of Persons with Disabilities Act 2016 guidelines for certification in India, based on the visual acuity and visual field parameters of the worse eye. ‘Stable for six months’ indicated no progression of visual loss, no active inflammation, and no further surgical intervention required during the preceding 6-month period.
Questionnaire
All the participants underwent baseline ocular examination and then were administered the standardized NEI-VFQ25 questionnaire for data collection.11,12 It is a well-established interviewer administered survey tool that was developed to assess the effect of eye disorders on a patient's visual QoL. This questionnaire measures the influence of VD and visual symptoms on emotional well-being and social functioning, in addition to, difficulties related to daily visual tasks. It contains a base set of 25 vision-targeted questions representing 11 vision-related subscales, along with an additional single-item general health related question. The 12 dimensions of VrQoL are general health, general vision, ocular pain, near activities, distance activities, vision-specific social functioning, vision-specific mental health, vision-specific role difficulties, vision-specific dependency, driving, color vision and peripheral vision. The questionnaire was scored on a scale of 0–100 in accordance with the VFQ25 scoring algorithm, with a score of 100 indicating the best VrQoL.
Scoring VFQ25 is a two-step process. Firstly, numeric values from the survey are recoded following the scoring rules with a higher score representing better functioning. Each item is then converted to a 0–100 scale so that the lowest and highest possible scores are set at 0 and 100 points, respectively. Here, the scores represent the achieved percentage of the total possible score, for instance, a score of 80 represents 80% of the highest possible score. After this, items within each sub-scale are averaged together to create the 12 sub-scale scores, with scores representing the average for all items in the sub-scale that the participant answered. Lastly, it needs to calculate an overall composite score for the VFQ25 by a simple average of the vision-targeted sub-scale scores, excluding the general health-related question. By averaging the sub-scale scores rather than the individual items, it gives equal weight to each sub-scale. The composite VFQ25 score, which combines all of the pre-weighted categories, reflects the overall effect of the level of visual function on the participant's life.
Data collection
The data collection was done by a single interviewer who administered the questionnaire. The interviewer-administered Hindi-translated and culturally adapted version of the NEI-VFQ25 was used, based on previously validated psychometric testing in the Indian population. The questionnaire was administered by a trained ophthalmic professional to ensure uniformity of data collection. Internal consistency in our cohort was assessed using Cronbach's alpha, which demonstrated acceptable reliability across key subscales (α values ranging from 0.72 to 0.89). As this was a single-time cross-sectional assessment in participants with stable vision loss, test–retest reliability could not be evaluated.
After obtaining written informed consent, participants were asked to provide the best-suited response for each question as per the survey format. Responses obtained were converted into a raw score as per the scoring key provided. An overall composite score was calculated as an average of all subscales, excluding the general health subscale. Scores of each VFQ subscale were analyzed after stratification was done based on BCVA (grouped into three as 6/36→3/60; 3/60-Perception of light, PL negative; others with enucleated or exenterated eye) and VD% (grouped into four groups as 20–30; 31–50; 51–75; and 76–100).
Statistical analysis
Data were entered in an Excel sheet. Double entry and accuracy of entered data were rechecked. SPSS version-23.0 was used for data analyses. Categorical variables have been presented as percentage and continuous variables as mean ± standard deviation (mean ± SD). The QoL scores of participants were expressed as the means ± SD. T-test and one-way ANOVA test were used to see the difference between the groups. Normality of continuous variables was assessed using the Shapiro–Wilk test to determine suitability for parametric testing. Independent samples t-test and one-way ANOVA were used only for variables demonstrating normal distribution. For variables not meeting normality assumptions, non-parametric tests (Mann–Whitney U test) were applied accordingly. A p-value of <0.05 was considered statistically significant.
Results
A total of 38 male participants with monocular loss of vision following ocular trauma completed the NEI-VFQ25 questionnaire. The descriptive analysis of ocular injuries is described in Table 1.
Descriptive analysis of ocular injuries.
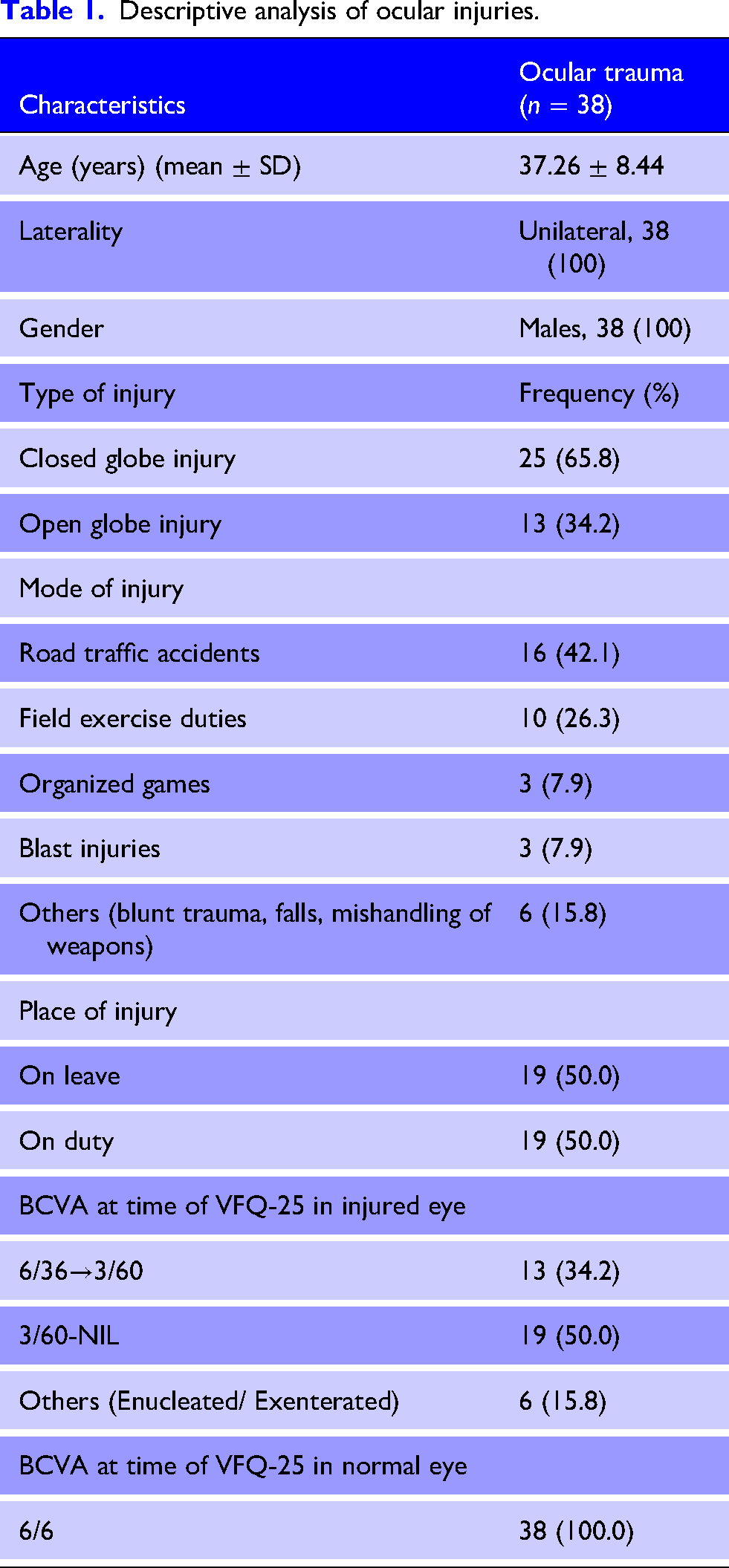
The mean age of presentation was 37.3 ± 8.4 years (range: 23–55years). The most common cause was RTA (42.1%), followed by workplace injuries (26.3%). The remaining cases were attributed to various other causes, such as blast injuries or mishandling of weapons.
Injury characteristics
Overall, 65.8% had closed globe injury and 34.2% had open globe injuries. All the participants had monocular loss of vision with better eye having BCVA of 6/6 and ≤6/36 in the injured eye. Half of the participants had BCVA <3/60 (50%), indicating severe vision impairment, while 34.2% had vision better than 3/60 in the injured eye. Six participants (15.8%) had undergone enucleation or exenteration of the globe due to severe ocular trauma.
25-Item Visual-Function Questionnaire scores
25-Item Visual-Function Questionnaire composite and subscale scores are presented in Table 2. The overall composite score was 56.47 ± 15.97, indicating a low visual QoL across all the subscales. The subscale with the lowest score was ‘driving’, with a mean of 21.05 ± 23.29, reflecting significant difficulty in this area.
VFQ25 composite and subscale scores of the participants when stratified based on best-corrected visual acuity.
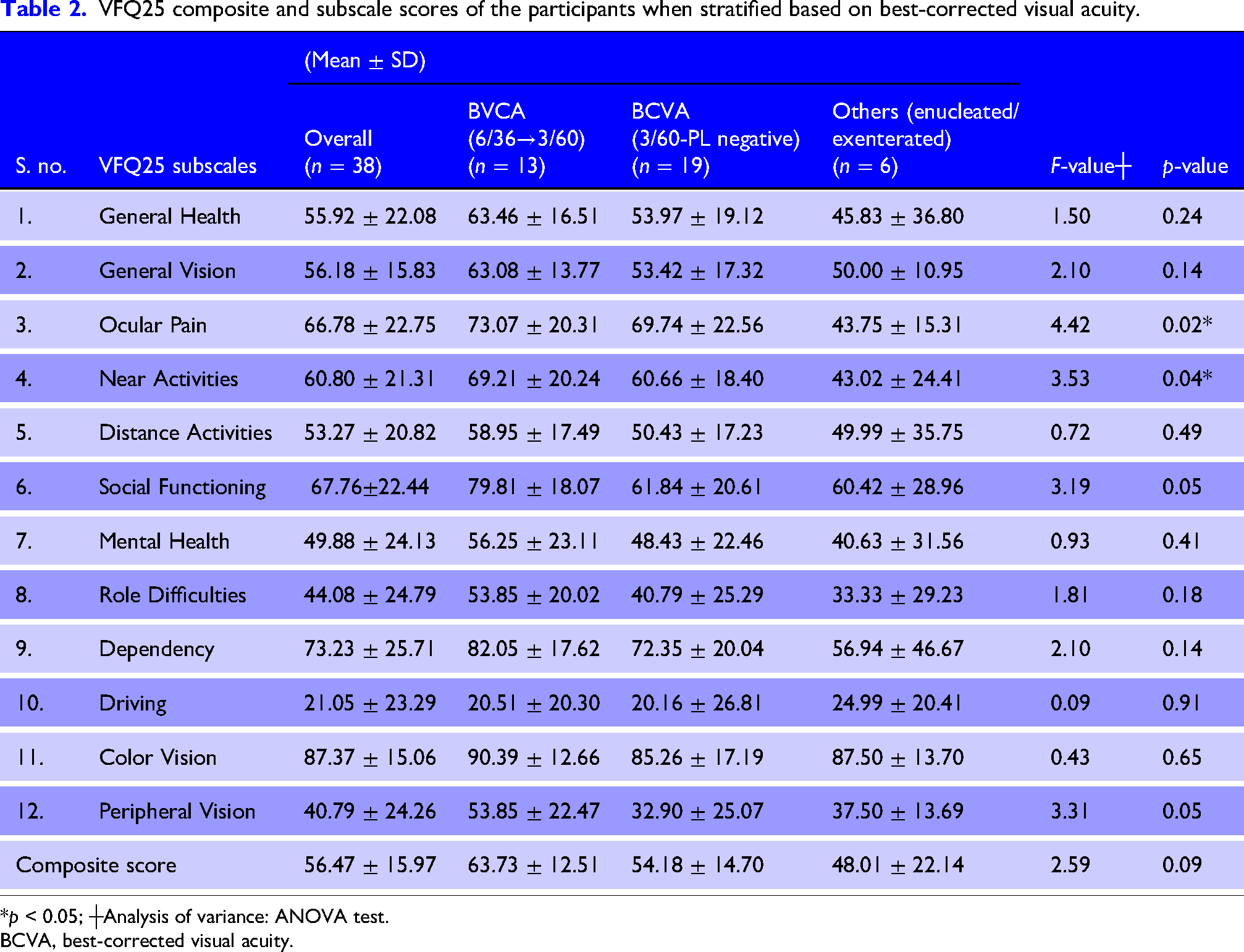
*p < 0.05; ┼Analysis of variance: ANOVA test.
BCVA, best-corrected visual acuity.
Impact of BCVA on QoL
Participants with BCVA ≤6/36 had a significant decrease in ocular pain and near activities compared to those with better vision (p < 0.05), indicating that those with worse visual acuity were more likely to experience higher levels of discomfort and difficulty in performing near tasks such as reading or fine manual work.
A notable difference in ‘ocular pain’ was observed when comparing participants with no perception of light (PL negative) to those who had undergone enucleation or exenteration (p = 0.00); most likely due to ongoing inflammation or complications associated.
Participants with PL negative when compared to those with enucleated or exenterated eyes were found to have similar subscale scores for ‘general vision’, ‘social functioning’ and ‘mental health’ (p > 0.05) (Table 3), suggesting that the emotional and social impacts of vision loss may not differ significantly between these two groups of severe injury.
25-Item Visual-Function Questionnaire composite and subscale scores of the participants having no vision.
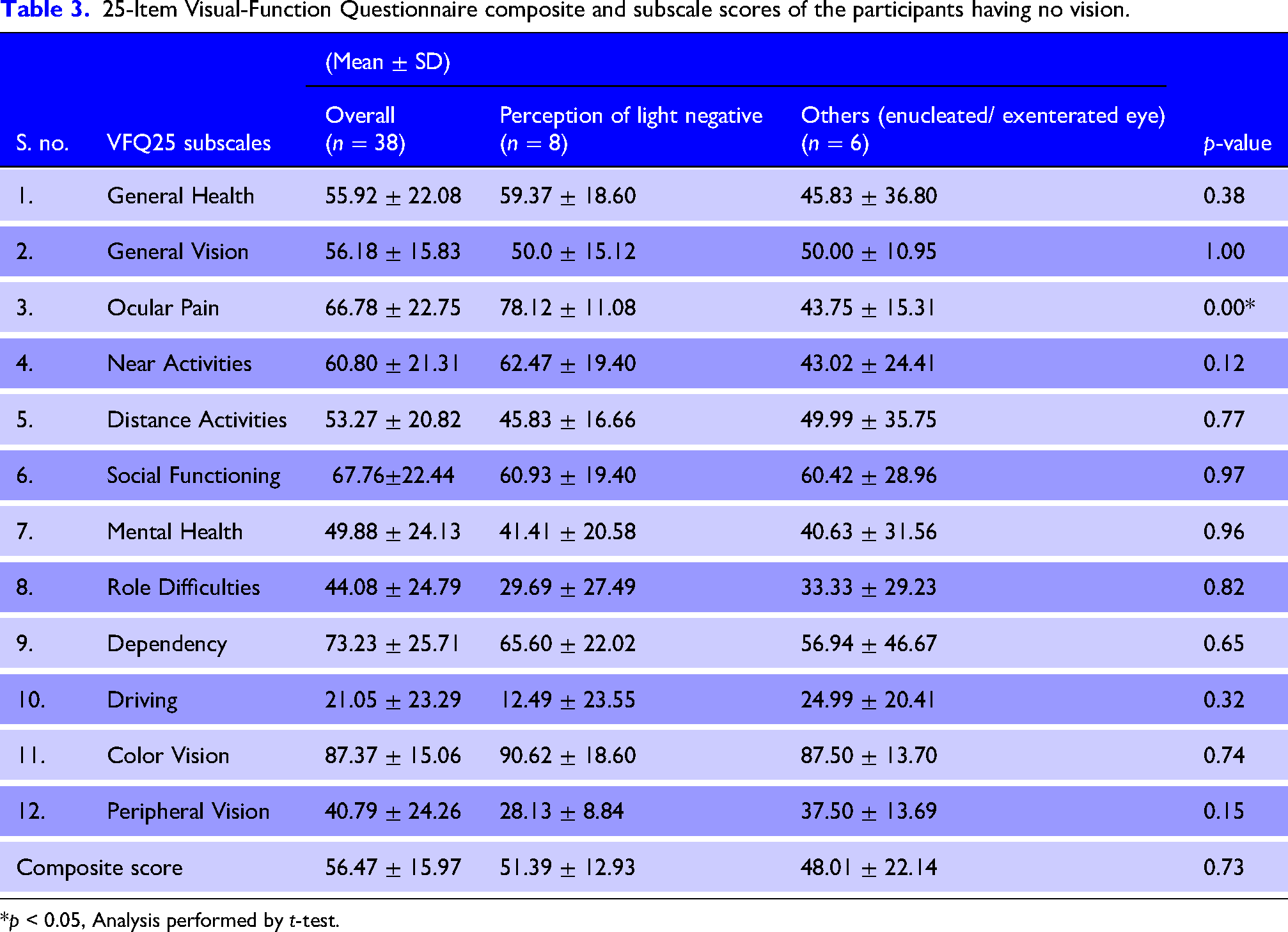
*p < 0.05, Analysis performed by t-test.
Discussion
Vision-related QoL is an unrecognized public health problem, largely due to the scarcity of epidemiological data on injury-related visual impairments. An intact binocular single vision plays an imperative role in development of QoL of an individual. While there have been several studies concerning ocular injuries, many have focused on the causes and characteristics in military personnel.13,14
This is a novel study to comprehensively assess VrQoL in individuals who sustained ocular trauma using VFQ25 questionnaire, providing valuable insights into this underexplored area. This study does not limit itself to BCVA but also explores the multidimensional impacts of monocular vision loss, which are often overlooked. This study also calls for a multidisciplinary rehabilitation approach, unlike traditional approaches that focus mainly on physical rehabilitation.
This study has reported the highest incidence of ocular trauma in the age group of 21–55 years, aligning with findings in other studies. 9 Few reports also suggest a bimodal pattern, with peaks in the 25–30 years of age group (34%) and again after 70 years. 15
Road-traffic accidents was most commonly responsible for ocular injuries in our study, emphasizing the need for better education on safe driving and the use of protective wears while driving. This can be taken care of by educating them via training programs and counselling the individuals.
A noteworthy finding was low incidence of open globe injuries (34.2%), which was much lower than seen in other studies reporting as high as 80.4%.16,17 While previous research in military settings often cited weapon handling etc as major causes, our study participants primarily faced trauma from civilian causes like RTAs.13,14
None of the participants with monocular vision loss crossed 50% of VD, in view of good vision (6/6) in the fellow eye. Participants with bilateral ocular trauma might have been invalidated out or not encountered during the study period.
Participants with BCVA <6/36 reported poorer VrQoL across all the subscales. The composite score reflects the overall effect of VD on one's life. Thus, low vision had a severe consequence on everyday lives. The composite score reported in this study (56.47 ± 15.97) was much lower than that reported in military personnel earlier with common ocular conditions such as glaucoma or age-related macular degeneration (74.4 ± 20.7).18–30
Our results are consistent with earlier work examining VrQoL in traumatic monocular vision. McLaughlin et al. reported a higher VFQ-25 composite score (68.2 ± 18.4) in U.S. military personnel with combat-related ocular trauma, possibly due to better rehabilitation resources and assistive support systems. 18 In contrast, Vichare et al. observed a lower mean score (51.8 ± 17.2) among civilian patients with both traumatic and non-traumatic causes of VD. 20 The composite score in our cohort (56.47 ± 15.97) lies between these two populations, suggesting that although the fellow eye retains good vision, functional and psychosocial challenges remain substantial in soldiers adapting to monocular status.
The subscale scores revealed that ‘driving’ had the most significant negative impact on QoL. Driving has a particularly strong association with independence, especially in countries where public transportation is limited, and was nearly impossible for most of the participants. This underscores how vision loss affects not only physical tasks but also psychosocial aspects, as participants reported feelings of frustration, mental health issues and role difficulties. As already reported, people with low vision show a higher percentage of individuals feeling short-tempered, exhausted and disinterested in everyday experiences. Also, it could be likely attributable to restrictions on driving licenses for individuals with monocular vision, rather than subjective visual difficulty alone. This restriction impacts mobility and independence, reflecting a broader psychosocial burden of trauma-related visual impairment.
Higher ‘ocular pain’ scores observed among participants with severely damaged eyes may be explained by post-traumatic complications such as chronic inflammation, elevated intraocular pressure, residual foreign body fragments or neuropathic pain pathways known to persist after severe ocular injury. In contrast, individuals who underwent enucleation reported lower ocular pain scores, consistent with the resolution of pain once the injured globe is removed.
Surprisingly, the ‘color vision’ and ‘dependency’ subscales had higher scores, indicating that they were able to accomplish most of their day-to-day activities on their own without much help from others, possibly due to good vision in the unaffected eye.
Despite monocular status, the ‘Color Vision’ subscale remained relatively high, likely due to the preserved chromatic perception provided by the healthy fellow eye. Since color discrimination depends mainly on intact cone function in one retina and normal cortical processing, patients with unilateral visual loss generally do not experience significant color vision impairment.
Patients with enucleated or exenterated eyes are similar in general vision with those having BCVA of PL negative, yet still the VFQ25 composite score was lower for the participants who had undergone removal of one eye. This suggests that, however the vision was similar in both groups but other vision-related factors were depressed more in those who underwent surgical removal of an eye following ocular trauma.
Interestingly, subjects who had undergone enucleation/exenteration reported lower scores in several VrQoL subscales compared to those with PL-negative eyes. This finding is consistent with previous reports that highlight the psychosocial burden associated with the loss of the eyeball, including disturbed self-image, cosmetic concerns and prosthesis-related discomfort or maladaptation. In contrast, retained but non-functional eyes may still provide a more satisfactory cosmetic appearance, potentially contributing to better perceived social functioning despite equivalent levels of VD. This suggests that cosmesis, ongoing ocular comfort and psychological adaptation play important roles in post-traumatic QoL beyond functional visual outcome alone.
Thus, it underlines the fact that other vision-related factors should always be considered while considering QoL in an individual. Also, in view of good vision in the fellow eye, these participants were able to manage for themselves and had not to rely too much on others for their work. This might also be the reason for similar scores in both groups in terms of social functioning and mental health.
This study suggests that along with BCVA, the overall QoL in patients with ocular trauma is affected in many aspects. Though they are able to perform most of their daily chores without much help from others due to good vision in other eye, the other fields such as difficulty in driving, poor mental health and difficulty in near activities definitely limit their capabilities.
These findings highlight the need for a more multidisciplinary approach in managing individuals with monocular vision loss after ocular trauma. Incorporating low-vision rehabilitation, driving and vocational counseling and psychological support services into military trauma recovery programs may improve functional adaptation and overall well-being. Structured follow-up focusing not only on visual acuity but also on long-term psychosocial adjustment is essential to mitigate the broader impact of monocular vision disability.
Limitations
This study is limited by its small sample size, lack of documentation of the use of eye protection at the time of trauma and lack of participants with bilateral ocular trauma. The study cohort comprised only 38 male active-duty soldiers, which reflects the injury epidemiology in the military setting but limits the generalizability of the findings to females, civilians and individuals in other occupational groups.
Further studies with a larger sample size, more diverse population and longitudinal follow-up are warranted to explore multidimensional impacts of ocular trauma and tailored rehabilitation strategies.
Conclusion
Ocular trauma has an extensive impact on visual function outcomes and overall VrQoL, highlighting the crucial role of considering broader implications such as functional dependence, mental health and social participation, apart from BCVA alone. While participants with monocular vision loss may manage daily tasks with relative independence, challenges such as driving, near activities and mental health issues persist. This reinforces the need for a multidisciplinary approach to rehabilitation, involving both ophthalmologists and psychiatrists.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.